Introduction
Rib fractures occur when a significant enough force directed at the rib causes a break. There are a total of 12 pairs of ribs in the thoracic region. The first seven ribs attach anteriorly to the sternum and posteriorly to the spinal column. Rib numbers 8 through 10 attach similarly but connect to the costal cartilage of the sternum anteriorly. Ribs 11 and 12 have the name of “floating” ribs as they only attach posteriorly but do not attach anteriorly. Underneath each rib lies the intercostal nerve, artery, and veins which supply to blood supply and innervation. The ribs function to protect the underlying organs and structures of the thoracic cavity. Any rib fracture should warrant a thorough evaluation of any concomitant injury, including lungs, heart, kidney, spleen, liver, and neuro-vasculature.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Rib fractures can be traumatic or atraumatic. Most rib fractures are due to direct penetrating or blunt trauma to the chest. Ribs 1 through 3 are the hardest to break and signify a significant degree of trauma if fractured. Ribs 4 through 10 are typically the most vulnerable while ribs 11 through 12 are more mobile and therefore more difficult to break. In the elderly, falls are a common etiology of rib fractures and are associated with higher mortality and morbidity than younger patients.[2] Rib fractures may also be pathologic as a result of cancer metastasis from other organs. Through repetitive stress and microtrauma, athletes can develop rib fractures with chronic use. Spontaneous rib fractures can also occur due to severe cough and are more likely to occur in those with osteoporosis or underlying lung disease.[3] Because children tend to have more elastic ribs than adults do, children are less likely to sustain rib fractures. Therefore, children with rib fractures is a sign of significant trauma and should warrant an investigation of possible child abuse.[4][5]
Epidemiology
The incidence and prevalence of rib fractures depend on the injury and the severity of the trauma. Children are less likely to sustain rib fractures than adults due to their more elastic ribs. The elderly tend to be more prone to rib fractures than younger individuals, with higher mortality and morbidity.[6]
Pathophysiology
Rib fractures can occur from either direct penetrating or blunt trauma. Athletes can also develop specific patterns of stress fractures depending on their sport.[7] The most feared complication of rib fractures is the flail chest where three or more rib fractures at two points on the involved ribs, creating a floating rib segment and causes this segment to move paradoxically with the rest of the chest wall. The mortality rate of flail chest is between 10% to 15%.[8]
History and Physical
Most isolated rib fractures are diagnosable through a clinical exam. Typically, patients will provide a history of recent blunt or penetrating thoracic trauma and pain at that site. They may also exhibit decreased ability to perform full inspiration due to pain. The physical exam may reveal chest wall bruising, along with bony tenderness to palpitation or crepitus. Any vital sign abnormalities such as hypoxia, tachypnea, or significant respiratory distress should undergo further evaluation of other possible injuries such as pneumothorax, hemothorax, cardiac and pulmonary contusions. Lower rib segment injuries should undergo assessment for kidney, liver, and spleen. Any patient with paradoxical chest wall movement or suspicion for multiple rib fractures should be evaluated for flail chest and managed accordingly.
Evaluation
Rib fractures can be diagnosed clinically based upon history and physical exam without imaging. Dedicated rib x-ray series are typically not necessary due to the benign clinical course of isolated rib fractures. If there is suspicion for multiple rib fractures or significant trauma with underlying organ damage, imaging can be the next step. However, chest radiographs are limited and can only diagnose about 50% of isolated rib fractures.[9] Point-of-care ultrasonography can reliably detect rib fractures along with complications of rib fractures such as pneumothorax.[10] Chest computed tomography (CT) scan is the gold standard of detecting rib fractures, although the fractures detected may not be clinically significant. The utility of chest CT during evaluation has more importance in the general assessment of trauma for other injuries.
Treatment / Management
For simple, isolated rib fractures, conservative therapy is usually adequate which includes appropriate analgesia, rest, and ice. The use of an incentive spirometer should be encouraged to prevent pulmonary atelectasis and splinting. Intercostal nerve blocks can also be applied to aid in pain control.[11] Rib taping is no longer the recommended treatment as it can impede inspiratory effort. When conservative management fails or for more severe rib fractures, surgical stabilization can be an option. Typical indications for surgical management include rib fracture nonunion, chest wall deformity or defect, refractory rib fracture pain causing respiratory failure, and flail chest.[12] If surgery is necessary, earlier operative intervention leads to better outcomes and also reduction or avoidance for mechanical ventilation.[13] Additionally, any other underlying injuries such as pneumothorax or hemothorax should be appropriately managed with insertion of a chest tube if indicated.
Differential Diagnosis
- Rib and chest wall contusion
- Diaphragmatic injury
- Hemothorax
- Pneumothorax
- Sternal fracture
- Pulmonary contusion
- Cardiac contusion
- Clavicular fracture
- Flail chest
- Scapular fracture
- Pneumomediastinum
Prognosis
Depending on the severity of the trauma sustained and degree of pain, rib fractures may be managed either outpatient or inpatient. Isolated rib fractures tend to heal well and do not need any further interventions beyond pain control, rest, and ice. Multiple rib fractures, displaced rib fractures, or those with underlying concomitant injuries may require inpatient monitoring for respiratory failure or surgical correction. Elderly individuals with rib fractures tend to have a higher mortality rate than younger individuals and may require closer monitoring.
Complications
The most severe complications related to rib fractures are the flail chest and damage to the underlying structures. Solid organ injuries associated with rib fractures include liver injuries and splenic injuries. Typically, the higher the rib fracture is within the thoracic cage, the more likely it is to cause a liver or splenic injury.[14] Particular attention needs to be paid for the patient's respiratory status, as rib fractures may cause the patients to go on and develop acute respiratory failure due to poor respiratory efforts and may need mechanical ventilation and surgical stabilization.
Deterrence and Patient Education
Given that rib fractures in the elderly are associated with higher mortality and morbidity, particular attention and resources need to be directed towards fall prevention to reduce the incidence of rib fractures. Studies show that an interdisciplinary team can significantly reduce the risk of falls in the elderly and therefore, clinicians and hospital staff should receive training on how to provide the necessary tools and resources needed to prevent falls.[15]
Enhancing Healthcare Team Outcomes
As with all significant trauma, a team of trained and dedicated professionals including emergency physicians, trauma surgeons, emergency and ICU nurses is requisite for initial evaluation, management, and stabilization. Early identification of potential patient decompensation should receive attention as a team, and possible interventions such as intubation, chest tubes, thoracotomies should be a team discussion to achieve optimal patient care and clinical results. [Level V] For insignificant trauma and simple rib fractures, patients can be safely discharged after evaluation.
Media
(Click Image to Enlarge)
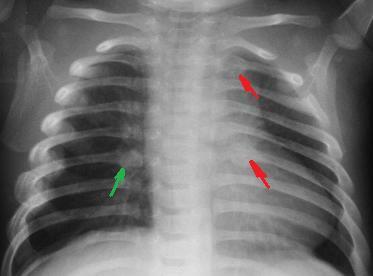
Rib fractures in an infant secondary to child abuse Contributed By National Institute of Health (NIH)
(Click Image to Enlarge)

Rib Fracture. Computed tomography of a patient who sustained a rib fracture (A) complicated by a pneumothorax and collapsed lung.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
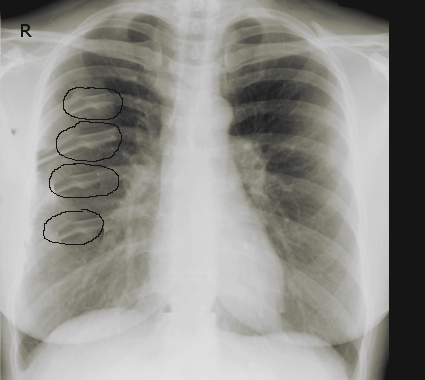
Consecutive rib fractures following blunt trauma Image courtesy S Bhimji MD
References
Graeber GM, Nazim M. The anatomy of the ribs and the sternum and their relationship to chest wall structure and function. Thoracic surgery clinics. 2007 Nov:17(4):473-89, vi. doi: 10.1016/j.thorsurg.2006.12.010. Epub [PubMed PMID: 18271162]
Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. The Journal of trauma. 2000 Jun:48(6):1040-6; discussion 1046-7 [PubMed PMID: 10866248]
Level 2 (mid-level) evidenceKatrancioglu O, Akkas Y, Arslan S, Sahin E. Spontaneous rib fractures. Asian cardiovascular & thoracic annals. 2015 Jul:23(6):701-3. doi: 10.1177/0218492315586485. Epub 2015 May 8 [PubMed PMID: 25957093]
Garcia VF, Gotschall CS, Eichelberger MR, Bowman LM. Rib fractures in children: a marker of severe trauma. The Journal of trauma. 1990 Jun:30(6):695-700 [PubMed PMID: 2352299]
Kemp AM, Dunstan F, Harrison S, Morris S, Mann M, Rolfe K, Datta S, Thomas DP, Sibert JR, Maguire S. Patterns of skeletal fractures in child abuse: systematic review. BMJ (Clinical research ed.). 2008 Oct 2:337():a1518. doi: 10.1136/bmj.a1518. Epub 2008 Oct 2 [PubMed PMID: 18832412]
Level 1 (high-level) evidenceBoele van Hensbroek P, Mulder S, Luitse JS, van Ooijen MR, Goslings JC. Staircase falls: high-risk groups and injury characteristics in 464 patients. Injury. 2009 Aug:40(8):884-9. doi: 10.1016/j.injury.2009.01.105. Epub 2009 May 31 [PubMed PMID: 19486973]
Level 2 (mid-level) evidenceIwamoto J, Takeda T. Stress fractures in athletes: review of 196 cases. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2003:8(3):273-8 [PubMed PMID: 12768465]
Level 3 (low-level) evidencePettiford BL, Luketich JD, Landreneau RJ. The management of flail chest. Thoracic surgery clinics. 2007 Feb:17(1):25-33 [PubMed PMID: 17650694]
Assi AA, Nazal Y. Rib fracture: Different radiographic projections. Polish journal of radiology. 2012 Oct:77(4):13-6 [PubMed PMID: 23269931]
Turk F, Kurt AB, Saglam S. Evaluation by ultrasound of traumatic rib fractures missed by radiography. Emergency radiology. 2010 Nov:17(6):473-7. doi: 10.1007/s10140-010-0892-9. Epub 2010 Jul 23 [PubMed PMID: 20652719]
Hwang EG, Lee Y. Effectiveness of intercostal nerve block for management of pain in rib fracture patients. Journal of exercise rehabilitation. 2014 Aug:10(4):241-4. doi: 10.12965/jer.140137. Epub 2014 Aug 31 [PubMed PMID: 25210700]
Doben AR, Eriksson EA, Denlinger CE, Leon SM, Couillard DJ, Fakhry SM, Minshall CT. Surgical rib fixation for flail chest deformity improves liberation from mechanical ventilation. Journal of critical care. 2014 Feb:29(1):139-43. doi: 10.1016/j.jcrc.2013.08.003. Epub 2013 Sep 24 [PubMed PMID: 24075300]
Pieracci FM, Coleman J, Ali-Osman F, Mangram A, Majercik S, White TW, Jeremitsky E, Doben AR. A multicenter evaluation of the optimal timing of surgical stabilization of rib fractures. The journal of trauma and acute care surgery. 2018 Jan:84(1):1-10. doi: 10.1097/TA.0000000000001729. Epub [PubMed PMID: 29077677]
Rostas JW, Lively TB, Brevard SB, Simmons JD, Frotan MA, Gonzalez RP. Rib fractures and their association With solid organ injury: higher rib fractures have greater significance for solid organ injury screening. American journal of surgery. 2017 Apr:213(4):791-797. doi: 10.1016/j.amjsurg.2016.08.002. Epub 2016 Aug 28 [PubMed PMID: 27663650]
Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C. Prevention of falls in the elderly trial (PROFET): a randomised controlled trial. Lancet (London, England). 1999 Jan 9:353(9147):93-7 [PubMed PMID: 10023893]
Level 1 (high-level) evidence