Introduction
The ribs are the bony framework of the thoracic cavity. Generally, there are twelve pairs of ribs. Each rib articulates posteriorly with two thoracic vertebrae; by the costovertebral joint. An exception to this rule is that the first rib articulates with the first thoracic vertebra only. According to their attachment to the sternum, the ribs are classified into three groups: true, false, and floating ribs. The true ribs are the ribs that directly articulate with the sternum with their costal cartilages; they are the first seven ribs. The false ribs are the ribs that indirectly articulate with the sternum, as their costal cartilages connect with the seventh costal cartilage; by the costochondral joint; They are the eighth, ninth, and tenth ribs. However, the floating ribs are the ribs that do not articulate with the sternum at all; they are the distal two ribs. The true ribs articulate with the sternum by the sternocostal joints. The first rib is an exception to that rule; it is a synarthrosis. Another thing that is good to know is that the first rib could uniquely articulate with the clavicle by the costoclavicular joint.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Typically, the ribs have the following anatomical components:
- Head with two articular facets
- Tubercle
- Neck
- Shaft
- Costal groove
Most of the ribs are typical ribs; which means that they have all these features. The atypical ribs which do not have all these features are:
- First rib
- Second rib
- Tenth rib
- Eleventh rib
- Twelfth rib
The first rib is atypical because it is wide and short, has two costal grooves, and one articular facet.
The second rib is thin, long, and has a tuberosity on its superior surface for the attachment of the serratus anterior muscle.
The tenth rib has only one articular facet.
The eleventh and twelfth ribs have only one articular facet with no neck.
The functions of the ribs are critical, as they protect the contents of the thoracic cavity and mediastinum, move superiorly, inferiorly, anteriorly and posteriorly to facilitate breathing, provide a place where some muscles originate or attach, and play a role in erythropoiesis during development.[2]
The ribs are critical in breathing since their flexibility in their movement increases/decreases the size of the thoracic cavity; assisting the lungs in respiration. Control of these movements is via the diaphragm, external intercostals, and the intercartilaginous portion of the internal intercostals.[3] At birth, the erythropoiesis sites change, it recedes in long bones and persists in flat bones, like ribs.[2]
Embryology
The ribs form embryologically by the differentiation of somites. Somite formation starts when the paraxial mesoderm begins to spiral and form a somitomere. Subsequently, somitomeres aggregate and form somites.[4]
Blood Supply and Lymphatics
The ribs receive their blood supply anteriorly; by the anterior intercostal arteries. However, they are supplied posteriorly; by the posterior intercostal arteries. Good to know, that the anterior intercostal arteries of the first seven ribs are branches of the internal thoracic artery. By contrast, the anterior intercostal arteries of the eighth, ninth, and tenth ribs are branches from the musculophrenic artery. All ten of these ribs are supplied posteriorly by the posterior intercostal arteries. Good to mention, that the first two posterior intercostal arteries are branches of the superior intercostal artery, a subsidiary of the costocervical trunk that arises from the left subclavian artery. Anyhow, the lower nine arteries are branches of the descending thoracic aorta. The floating ribs receive vascular supply differently since they are short and have no sternal articulation, only receiving supply posteriorly by the posterior intercostal arteries. The eleventh rib receives vascular supply by the posterior intercostal artery and the twelfth rib by the subcostal artery.
The nomenclature of the costal veins is the same as the arteries; they differ as to where they drain blood. The anterior intercostal veins drain blood into the internal thoracic and musculophrenic veins. The posterior intercostal veins drain blood into the azygos and hemiazygos system. The subcostal vein drains the blood of the twelfth rib.
Note: all arteries and veins run in the costal groove of each rib.
Nerves
The intercostal nerves supply the ribs by sensory and motor branches. They run between the innermost and internal intercostal muscles; inferior to the blood vessels in the costal groove. They exit the groove when they branch. Their branches are:
- Lateral cutaneous branches: these innervate the skin of the lateral thoracic wall. They pierce the external intercostal muscle and divide into anterior and posterior branches.
- Anterior cutaneous branches: provide innervation to the skin of the anterior thorax. It reaches the skin near the midline.
- Pleural sensory branches: innervate the parietal pleura.
- Peritoneal sensory branches: run in the parietal peritoneum on the seventh, eighth, ninth, tenth, and eleventh intercostal nerves.
- The collateral branch: runs on the upper border of the rib below its corresponding number.
- Muscular branches: innervate the intercostal muscles.
- Rami communicantes: connect the intercostal nerves to a sympathetic ganglion.
Muscles
Many muscles act on or affect the movement of the ribs. These muscles are:
- Pectoralis major: its clavicular head originates on the anterior surface of the medial half of the clavicle, but its sternocostal head originates on the anterior surface of the sternum, the proximal six costal cartilages, and the external abdominal oblique aponeurosis. It inserts on the bicipital groove's lateral lip of the humerus. Its sternal head is innervated by the medial pectoral nerve, and its clavicular head is innervated by the lateral pectoral nerve. It is considered to be an auxiliary inspiratory muscle.
- Pectoralis minor: originates on the third, fourth, and fifth ribs, and inserts on the coracoid process of the scapula. It lies posteriorly to the pectoralis major and is innervated by the medial pectoral nerve. It lifts the ribs when the scapula is in a fixed position. It is considered to be an auxiliary inspiration muscle and is one of the rotator cuff muscles.
- External abdominal oblique: it originates on the fifth to twelfth ribs, and inserts on the xiphoid process, pubic crest, outer lip of the iliac crest, linea alba, pubic tubercle, anterior superior iliac spine, and inguinal ligament. It pulls the ribs inferiorly and compresses the abdominal cavity to increase the intraabdominal pressure. It is innervated by the anterior lower six thoracoabdominal branches and the subcostal nerve on each side.
- Rectus abdominis: originates on the pubic crest and inserts on the fifth, sixth, and seventh costal cartilages and the xiphoid process. It is innervated by the thoracoabdominal and subcostal nerves. It acts on the ribs by tilting the rib cage and pelvis inward towards the abdomen helping in active expiration.
- Subclavius: originates on the first rib and cartilage and inserts on the clavicle's subclavian groove. It is innervated by the subclavian nerve. It elevates the first rib.
- Serratus anterior: originates on the upper eight or nine ribs and inserts along the medial border, superior angle, and inferior angle of the scapula.[5] It is innervated by the long thoracic nerve; and assists in respiration by lifting the ribs.
- External intercostal: originates on the lower borders of the ribs and inserts on the upper border of the rib below. It is innervated by intercostal nerves. It assists in inspiration by driving the ribs in the cranial direction.[6]
- Internal intercostal: its origin, insertion, and innervation are similar to the external intercostal muscle. It assists in forced expiration by depressing the ribs and bending them inward.
- Innermost intercostal: its origin, insertion, and innervation are similar to the external intercostal muscle. It assists in forced expiration in the same manner as internal intercostal.
- Diaphragm: The sternal part originates on the inner surface of the xiphoid process. The costal part originates on the inner surfaces of the cartilages of the distal six ribs. The medial crus originates on the lumbar vertebrae. The lateral crus originates on the ligaments that jump over the quadratus and psoas muscles. All the portions of the diaphragm insert on the central tendon. It is innervated by the phrenic and lower intercostal nerves. It expands the lower rib cage and is considered to be the main inspiratory muscle.[7]
- Quadratus lumborum: arises from the posterior border of the iliac crest and inserts on the first to fourth lumbar vertebrae plus the twelfth rib. It is innervated by the first four lumbar nerves, plus the twelfth thoracic nerve. It depresses the lower rib cage.
- Transversus thoracis: originates from the posterior aspects of the xiphoid process, the body of the sternum, and the lower three or four true rib's costal cartilages. It inserts on the lower surfaces of the second through sixth ribs with their costal cartilages. It is innervated by the intercostal nerves; and assists in forced expiration by depressing the ribs.[8]
- Latissimus dorsi: originates on the inferior three or four ribs, thoracolumbar fascia, inferior angle of the scapula, iliac crest, and the spinous processes of the seventh thoracic to the fifth lumbar vertebrae. It inserts on the floor of the intertubercular sulcus of the humerus. It is innervated by the thoracodorsal nerve. Its role in the ribcage's movement is not yet clear but is considered to be a respiratory accessory muscle.[9]
- Serratus posterior superior: originates on the nuchal ligament and the seventh cervical to the third thoracic vertebrae. It inserts on the upper borders of the second to fifth ribs. It is innervated by the second to fifth intercostal nerves; its function is to elevate the second to fifth ribs. Note that there is no evidence supporting its role in respiration.[10]
- Serratus posterior inferior: originates on the spinous process of the eleventh thoracic to the second lumbar vertebrae and inserts on the inferior borders of the ninth to twelfth ribs. It is innervated by the distal four intercostal nerves; it depresses the distal four ribs. Note that there is no evidence supporting its role in respiration.[10]
Physiologic Variants
The rib cage’s volume is 10% smaller in females than males. Nevertheless, the cranio-caudal inclination of the ribs is greater in females. A general rule is that the females’ ribs grow longer relative to the axial skeleton than in males.[11]
Other variants in the ribs between individuals are developmental deformities and cervical/short rib that mimics true rib diseases.[12]
Surgical Considerations
The ribs are very important, and healthcare workers should know of the anatomical structures that lie deep to the ribs. The ribs can be counted by palpation to determine the site of thoracentesis or a thoracostomy tube. The rib count is also done before surgery to ensure that one opens the thoracic cavity in the proper location.
Clinical Significance
Ribs fractures are prevalent, as they comprise 12% of total fractures in patients. (The risk notably increases with age).[13]Other common abnormalities are[14][15]:
- Rib dislocation
- Costochondritis
- Osteoporosis
Tumors may also develop in the ribs. These tumors may be primary or secondary lesions. According to one study, the cure rate of benign and malignant cancers in the ribs through resection was 100% successful without recurrence.[16]
Other Issues
Pectus excavatum and pectus carinatum are the most common chest deformities in young patients. These lesions affect the patient psychosocially and physiologically; chiefly because the deformity is cosmetic. Besides, some of these patients may also experience difficulty with respiration. Surgical correction is done when necessary; to avoid complications affecting the heart and lungs.[4]
Media
(Click Image to Enlarge)
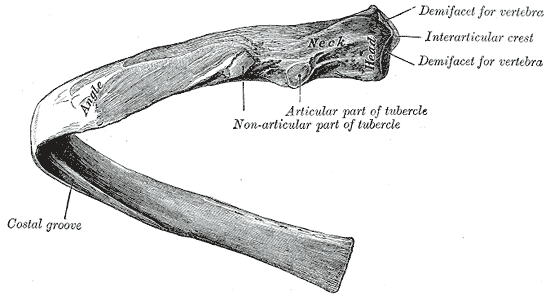
The Ribs, A central rib of the left side; viewed from behind
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
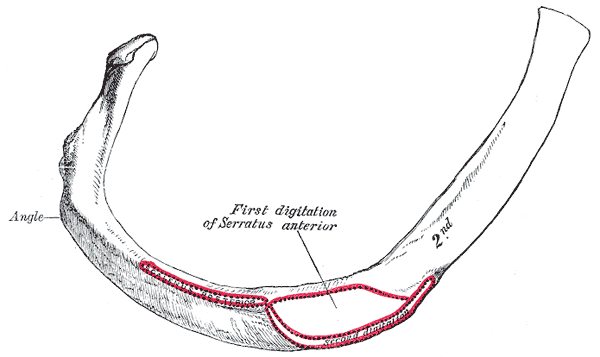
The Ribs, Second Peculiar rib
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

The image shows the ribcage and the different ribs. Contributed by Bruno Bordoni, PhD
References
Redlund-Johnell I. The costoclavicular joint. Skeletal radiology. 1986:15(1):25-6 [PubMed PMID: 3941919]
Level 3 (low-level) evidenceHom J, Dulmovits BM, Mohandas N, Blanc L. The erythroblastic island as an emerging paradigm in the anemia of inflammation. Immunologic research. 2015 Dec:63(1-3):75-89. doi: 10.1007/s12026-015-8697-2. Epub [PubMed PMID: 26376896]
De Troyer A, Boriek AM. Mechanics of the respiratory muscles. Comprehensive Physiology. 2011 Jul:1(3):1273-300. doi: 10.1002/cphy.c100009. Epub [PubMed PMID: 23733642]
Level 3 (low-level) evidenceHussain A, Burns B. Anatomy, Thorax, Wall. StatPearls. 2024 Jan:(): [PubMed PMID: 30571035]
Lung K, St Lucia K, Lui F. Anatomy, Thorax, Serratus Anterior Muscles. StatPearls. 2024 Jan:(): [PubMed PMID: 30285352]
De Troyer A, Wilson TA. The canine parasternal and external intercostal muscles drive the ribs differently. The Journal of physiology. 2000 Mar 15:523 Pt 3(Pt 3):799-806 [PubMed PMID: 10718756]
Level 3 (low-level) evidencePickering M, Jones JF. The diaphragm: two physiological muscles in one. Journal of anatomy. 2002 Oct:201(4):305-12 [PubMed PMID: 12430954]
Level 3 (low-level) evidenceJelev L, Hristov S, Ovtscharoff W. Variety of transversus thoracis muscle in relation to the internal thoracic artery: an autopsy study of 120 subjects. Journal of cardiothoracic surgery. 2011 Jan 27:6():11. doi: 10.1186/1749-8090-6-11. Epub 2011 Jan 27 [PubMed PMID: 21272314]
Level 2 (mid-level) evidenceJeno SH, Varacallo M. Anatomy, Back, Latissimus Dorsi. StatPearls. 2024 Jan:(): [PubMed PMID: 28846224]
Vilensky JA, Baltes M, Weikel L, Fortin JD, Fourie LJ. Serratus posterior muscles: anatomy, clinical relevance, and function. Clinical anatomy (New York, N.Y.). 2001 Jul:14(4):237-41 [PubMed PMID: 11424195]
Bellemare F, Fuamba T, Bourgeault A. Sexual dimorphism of human ribs. Respiratory physiology & neurobiology. 2006 Feb 28:150(2-3):233-9 [PubMed PMID: 16476656]
Kurihara Y, Yakushiji YK, Matsumoto J, Ishikawa T, Hirata K. The ribs: anatomic and radiologic considerations. Radiographics : a review publication of the Radiological Society of North America, Inc. 1999 Jan-Feb:19(1):105-19; quiz 151-2 [PubMed PMID: 9925395]
Barnea Y, Kashtan H, Skornick Y, Werbin N. Isolated rib fractures in elderly patients: mortality and morbidity. Canadian journal of surgery. Journal canadien de chirurgie. 2002 Feb:45(1):43-6 [PubMed PMID: 11837920]
Proulx AM, Zryd TW. Costochondritis: diagnosis and treatment. American family physician. 2009 Sep 15:80(6):617-20 [PubMed PMID: 19817327]
Agnew AM, Stout SD. Brief communication: Reevaluating osteoporosis in human ribs: the role of intracortical porosity. American journal of physical anthropology. 2012 Jul:148(3):462-6. doi: 10.1002/ajpa.22048. Epub 2012 Mar 15 [PubMed PMID: 22419443]
Andrianopoulos EG, Lautidis G, Kormas P, Karameris A, Lahanis S, Papachristos I, Kaselouris C, Argyropoulos A. Tumors of the ribs: experience with 47 cases. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 1999 May:15(5):615-20 [PubMed PMID: 10386406]
Level 2 (mid-level) evidence