Introduction
The rhomboids are a collective group of muscles formed by the rhomboid major and minor. The rhomboids are important in upper limb movement and stability of both the shoulder girdle and scapula. Both rhomboids receive innervation from the dorsal scapular nerve, and their vascular supply the dorsal scapular artery. Variants in rhomboid musculature have been found but are very rare. While surgeries of the rhomboid musculature are infrequent, winged scapula and rhomboid palsy are clinical pathologies associated with the rhomboids.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The rhomboids consist of two separate muscles; the major and minor muscles, which are found immediately deep to the trapezius. The rhomboid minor is a cylindrical muscle that originates at the ligamentum nuchae and C7 and T1 vertebra. It inserts at the scapula's medial border near the base of the spine of the scapula. The rhomboid major is a quadrangular muscle located inferior to the rhomboid minor. The origin of the rhomboid muscles is from the spinous processes of the T2-T5 vertebra and inserts on the medial border of the scapula, just inferior to the rhomboid minor.[2][3][4]
With the assistance of many other muscles, the rhomboids help form the shoulder girdle. This group of muscles is important for the movement of the upper extremity and stabilization of the shoulder through articulation with the trunk. Functionally, the rhomboid muscles retract, elevate and rotate the scapula. They also protract the medial border of the scapula, keeping it in position at the posterior thoracic wall. Dysfunction, weakness, or loss of nerve function to the rhomboids causes winging of the medial border of the scapula and inferior scapular angle rotation.[2][5]
The rhomboids are also vital to actions such as pulling and have been shown to play a large role in throwing and overhead arm movement.[4]
Embryology
The deep shoulder girdle muscles (i.e., rhomboid major, rhomboid minor, and serratus anterior) are derived from thoracic somitic cells, unlike other muscles of the shoulder and upper limb, which develop from the lateral plate mesoderm and limb bud.[5] Compared to the rest of the skeletal limb muscles, which receive innervation from the brachial plexus, the deep shoulder girdle muscles have been innervated by branches of cervical spinal nerves.[6]
Despite these differences, the embryonic origin of the rhomboids correlates to their respective nerve supply, as is the case with other muscles of the shoulder and upper limb.[5] Ultimately, it may be concluded that the rhomboid muscles, like other deep shoulder girdle muscles, have a distinct developmental program different from that of the limb and superficial shoulder muscles.[6]
Blood Supply and Lymphatics
The rhomboid muscles primarily receive their vascular supply via the dorsal scapular artery (DSA), which generally arises from either the second or the third portion of the subclavian artery. Some studies have also shown variations where the DSA stems from the thyrocervical trunk. Regardless of its site of origin, the DSA passes through the brachial plexus, where it joins and runs parallel to the dorsal scapular nerve. Together both the nerve and artery course inferiorly to supply the rhomboid muscles.[7][8]
Nerves
The motor function of the rhomboid muscles is controlled by the dorsal scapular nerve (DSN). The dorsal scapular nerve originates from the ventral ramus of the spinal nerve root C5 and courses posterior inferiorly through the middle scalene muscles and between the posterior scalene, levator scapulae (to which it also provides innervation), and the serratus posterior superior. It continues deep to the brachial plexus to innervate both the rhomboid minor and major muscles at their anterior border.[9]
Muscles
The rhomboid major and minor are a group of deep intrinsic shoulder muscles that, together with the sternocleidomastoid, trapezius, pectoralis muscles, latissimus dorsi, and serratus anterior, form the shoulder girdle. Furthermore, the serratus anterior, trapezius, and rhomboid major and minor work with the rhomboids to anchor the scapula and prevent winging. Additionally, the serratus anterior is the antagonist muscle group to the rhomboids.[2] The rhomboids also work in conjunction with the levator scapulae to elevate and retract the scapula.[10]
Physiologic Variants
Variants of the rhomboid muscles are rare but present interesting cases when discovered. There have been three reported cases of an additional rhomboid muscle discovered in humans. The first, known as “occipito-scapularis,” is attached at the level of the occipital bone and passes inferior and across the splenius capitis. It coursed deep to the trapezius and inserted into the insertions of the rhomboid major and minor muscles at the level of the spine of the scapula. A second variant, “rhomboideus-occipitalis or capitis,” originated at the superior nuchal line deep to the trapezius. It then inserts between the inferior rhomboid minor and superior levator scapulae and into the serratus posterior. The third variant, also referred to as “rhomboideus capitis,” originated from the superior nuchal line and moved inferiorly on the splenius capitis. It follows the medial levator scapulae before inserting on the medial scapula opposite the scapular spine.[11]
Surgical Considerations
Surgical intervention of the rhomboid muscles is rare. However, it may be required in some cases. Rhomboid muscle flaps can be used in the treatment of head and neck cancers, esophagus reconstruction, mandibular defects, and Sprengel disease (Sprengel deformity), which is the congenital elevation of the scapula.[3] Additionally, severe winging of the scapula due to weakened rhomboid muscles may be corrected by using fascia lata grafts. These grafts act to assist the weakened rhomboids and also connect the infra-medial border and the inferior angle of the scapula to the spinal muscles and latissimus dorsi, respectively. However, complications may arise as the grafts have been known to fail and weaken over time.[2][12]
Although not specifically surgical, ultrasound-guided injections into the rhomboids have also been shown to be more effective than superficial trapezius injections for pain, disability, and quality of life for patients with myofascial pain syndrome.[13]
Clinical Significance
A winged scapula due to rhomboid palsy is one of the more common pathologies specific to this muscle group. Rhomboid palsy most often occurs due to damage to the dorsal scapular nerve. Entrapment of the dorsal scapular nerve is the most frequent cause, but the exact location of entrapment has not been specified. Additionally, direct injury to the dorsal scapular nerve through trauma, anterior shoulder dislocation, or overuse of overhead athletics (i.e., baseball and volleyball) are other noted causes of rhomboid palsy.[2]
Patients often present with medial scapular pain, abnormal shoulder motion, and neck, back, and shoulder discomfort. Physical examination often yields subtle lateral winging of the scapula. As a result of the subtle exam finding and the deep anatomic position of the rhomboids, rhomboid palsy is often underdiagnosed. EMG is most specific for the diagnosis of rhomboid palsy and shows prolonged muscle latency of the muscle action potential.[14] Treatment is usually conservative and focused on cervical spine stabilization, muscle relaxants, physical therapy, NSAIDs, and possibly surgery in extreme cases.[2]
Media
(Click Image to Enlarge)
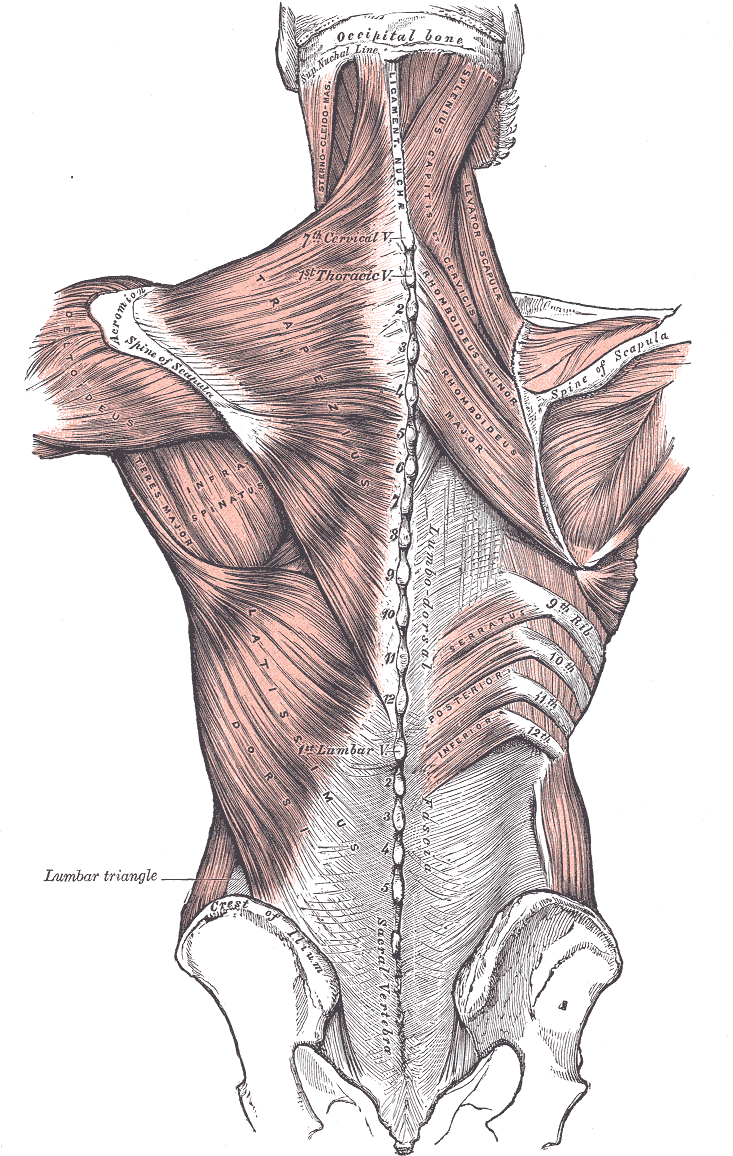
Posterior Axioappendicular Muscles. This image depicts the posterior axioappendicular muscles, including the trapezius, levator scapulae, latissimus dorsi, rhomboid major and minor, and serratus posterior inferior. Additional muscles shown in the image include the sternocleidomastoid, splenius capitis of services, deltoideus, teres major, and infraspinatus. Bony structures featured in the image include the vertebral column, occipital bone and superior nuchal line, scapular spine, iliac crest, and sacral vertebra. Furthermore, the ligamentum nuchae and lumbar triangle are also depicted in this image.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mitchell B, Imonugo O, Tripp JE. Anatomy, Back, Extrinsic Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30725901]
Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Current reviews in musculoskeletal medicine. 2008 Mar:1(1):1-11. doi: 10.1007/s12178-007-9000-5. Epub [PubMed PMID: 19468892]
Beger O, Dinç U, Beger B, Uzmansel D, Kurtoğlu Z. Morphometric properties of the levator scapulae, rhomboid major, and rhomboid minor in human fetuses. Surgical and radiologic anatomy : SRA. 2018 Apr:40(4):449-455. doi: 10.1007/s00276-018-2002-8. Epub 2018 Mar 15 [PubMed PMID: 29541801]
Paine R, Voight ML. The role of the scapula. International journal of sports physical therapy. 2013 Oct:8(5):617-29 [PubMed PMID: 24175141]
Marecki B, Wosicki J. Morphology of the rhomboid muscle in human fetuses. Folia morphologica. 1987:46(3-4):227-33 [PubMed PMID: 3508144]
Valasek P, Theis S, Krejci E, Grim M, Maina F, Shwartz Y, Otto A, Huang R, Patel K. Somitic origin of the medial border of the mammalian scapula and its homology to the avian scapula blade. Journal of anatomy. 2010 Apr:216(4):482-8. doi: 10.1111/j.1469-7580.2009.01200.x. Epub 2010 Jan 28 [PubMed PMID: 20136669]
Level 3 (low-level) evidenceHUELKE DF. The dorsal scapular artery--a proposed term for the artery to the rhomboid muscles. The Anatomical record. 1962 Jan:142():57-61 [PubMed PMID: 14449723]
Verenna AA, Alexandru D, Karimi A, Brown JM, Bove GM, Daly FJ, Pastore AM, Pearson HE, Barbe MF. Dorsal Scapular Artery Variations and Relationship to the Brachial Plexus, and a Related Thoracic Outlet Syndrome Case. Journal of brachial plexus and peripheral nerve injury. 2016:11(1):e21-e28. doi: 10.1055/s-0036-1583756. Epub 2016 May 10 [PubMed PMID: 28077957]
Level 3 (low-level) evidenceTubbs RS, Tyler-Kabara EC, Aikens AC, Martin JP, Weed LL, Salter EG, Oakes WJ. Surgical anatomy of the dorsal scapular nerve. Journal of neurosurgery. 2005 May:102(5):910-1 [PubMed PMID: 15926718]
Nguyen VH, Liu HH, Rosales A, Reeves R. A Cadaveric Investigation of the Dorsal Scapular Nerve. Anatomy research international. 2016:2016():4106981. doi: 10.1155/2016/4106981. Epub 2016 Aug 15 [PubMed PMID: 27597900]
Rogawski KM. The rhomboideus capitis in man--correctly named rare muscular variation. Okajimas folia anatomica Japonica. 1990 Aug:67(2-3):161-3 [PubMed PMID: 2216308]
Galano GJ, Bigliani LU, Ahmad CS, Levine WN. Surgical treatment of winged scapula. Clinical orthopaedics and related research. 2008 Mar:466(3):652-60. doi: 10.1007/s11999-007-0086-2. Epub 2008 Jan 8 [PubMed PMID: 18196359]
Level 2 (mid-level) evidenceMetin Ökmen B, Ökmen K, Altan L. Comparison of the Efficiency of Ultrasound-Guided Injections of the Rhomboid Major and Trapezius Muscles in Myofascial Pain Syndrome: A Prospective Randomized Controlled Double-blind Study. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2018 May:37(5):1151-1157. doi: 10.1002/jum.14456. Epub 2017 Oct 19 [PubMed PMID: 29048132]
Level 1 (high-level) evidenceSultan HE,Younis El-Tantawi GA, Role of dorsal scapular nerve entrapment in unilateral interscapular pain. Archives of physical medicine and rehabilitation. 2013 Jun [PubMed PMID: 23220342]
Level 2 (mid-level) evidence