Introduction
The red nucleus (RN) is a primitive brainstem structure located in the ventral midbrain. Histologically, the RN consists of two distinct structures: a rostral parvocellular red nucleus (RNp) and a caudal magnocellular red nucleus (RNm).[1][2] Although the origin of the RN is not completely understood, studies suggest it can be attributed to the evolutionary development of limbs and locomotion among vertebrates.[3] Specifically, when comparing different species, there is wide variability in both the structure and function of the RN. Generally, the RNm predominates in lower vertebrates, while the RNp is more prominent in higher species.[2] Regarding quadrupedal mammals (i.e., cats and rats), the RNm is highly developed. However, when progressing upward the evolutionary pyramid, the RNm decreases in size and ultimately bares minimal significant volume or neurological function within the human brain (conversely, the RNp occupies most of the RN total volume in humans).[1][4][5][6] Furthermore, although the two subsections of the RN are virtually undifferentiated in lower mammals, the human RNm and RNp are so distinct that they are more so considered two completely independent structures altogether.[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
As mentioned, the RN is subdivided into the RNp and the RNm. These neurons are arranged in a somatotopic distribution, with the upper limb corresponding with the dorsomedial region and the lower limb correlating with the ventrolateral portion.[7][1] Regarding the RNm, the contralateral interposed nuclei of the deep cerebellum project neurons that travel directly to the RNm, which thereby gives rise to the rubrospinal tract and subsequently relays into the spinal cord.[1] Conversely, the RNp receives input from the dentate nucleus within the cerebral cortex as well as the deep white matter of the cerebellum and redirects input into the ipsilateral inferior olivary nucleus (commonly referred to as the myoclonic triangle, the triangle of Guillain-Mollaret, or the dentato-rubro-olivary pathway).[1]
It is important to distinguish the subsections of the red nuclei because each possesses a unique neuronal pathway and, therefore, dictates a separate neurologic function. For example, among quadrupedal animals, the RNm closely mirrors the pyramidal tract when animals navigate through obstacles and perform various coordinated extremity movements.[8] In upper mammals (such as primates) rubrospinal activity (and therefore RNm activity) influences more primitive motor activity such as grasping, most prominently among infants.[9] As mentioned previously, the RNm is largely rudimentary in adult humans (and therefore bears a lesser neurologic role), most likely due to the development (and functional redundancy) of the corticospinal tract and the pyramidal system.[9][10] One interesting correlation to note is that among fetuses and newborns, who possess a particularly notable magnocellular red neurons, also demonstrate particularly prominent limb flexor tone.[9] Additionally, anencephalic infants deprived of the cerebral cortex (but still have intact midbrain and, therefore, an RN) can exhibit synergistic stepping patterns, therefore reinforcing the notion that the rubrospinal tract bears functional responsibility in primitive movements.[11]
In contrast, the RNp provides an important connection between the motor and premotor cortices as well as the cerebellum and inputs directly into the inferior olivary nucleus.[9] Therefore, this subsection of the RN represents an important link in the motor circuit. Although the exact role of the RNp remains unknown, it is suggested to potentially play a role in complex cognitive-motor functions by regulating the olivocerebellar tract system.[12][13]
In summary, the parvocellular division of the RN is particularly prominent in the adult human brain and may play a role in cognitive-motor function, while the magnocellular RN only demonstrates functional relevance in early development through primitive movements and becomes less functionally significant with aging.[9]
Embryology
To date, very few studies have explored the embryonic development of the red neuron.[6][2] However, studies that have examined such development noted several consistent findings. First, initial development commences with cell migration concurrently with the mid-brain from the cerebellum at around week 7. Around week 8, cells accumulate along the cerebellar outgrowth, which eventually develops into the dentate nucleus in series with the RN. After that, RN differentiation commences with RNm formation beginning around 12 weeks.[2] By week 14, large and small neurons are recognizable within the RN and continue to develop into the RNm and the RNp. Between weeks 18-23, the oculomotor nerve localizes and clusters around the RN[2] and eventually distributes along the ventrolateral superior cerebellar peduncle from 28 weeks onward. Finally, from weeks 28 to 33, there is a near-linear increase in neuronal size with regards to gestational age, leading to ultimately a consistent detection of neuro-histology by 33 weeks.[2]
Blood Supply and Lymphatics
The RN receives blood supply from the posterior cerebral artery (PCA).[14][15][14]
Nerves
There is an increasing number of studies exploring the relationship between the magnocellular RN and pain modulation and allodynia,[16][17] most likely via inflammatory cytokine expression through the JAK/STAT, JNK, and ERK signaling cascade.[18][19] As such, previous studies have demonstrated that spared nerve injury in animal models up-regulates pro-inflammatory cytokines (such as interleukin-6 and tumor necrosis factor-alpha) within the red nucleus. Furthermore, the administration of recombinant pro-inflammatory cytokines directly within the RN can evoke tactile allodynia.[19][20] Conversely, inhibition of such cytokines can mitigate neuropathic pain[21][22] and relieve subsequent spared nerve injury tactile allodynia.[23][24][25] The combination of these findings suggests a causal relationship between the red nucleus and pain modulation.
Surgical Considerations
Among the most common surgical interventions for Parkinson disease involves targeted deep brain stimulation of the subthalamic nucleus. This procedure, however, is subject to a high rate of error.[26][27] One important consideration with regards to this procedure is the close resemblance, both anatomically and physiologically between the subthalamic nucleus and the RN, especially among Parkinson disease patients.[27] This close resemblance commonly causes incorrect lead placement[27][28] and is the reason why over 50% of deep brain stimulation procedures result in failure.[29]
Clinical Significance
There are a number of clinical situations that bear relation to the RN and its function. First, as mentioned previously, there is considerable functional redundancy between the corticospinal tract and the rubrospinal tract. Therefore, in the case of corticospinal tract injury (such as stroke or spinal cord injury), neurologic compensation and response occur in the acute setting, by which the red nuclei undergo remodeling and increase activity.[30] This upregulation may provide a small degree of compensation in motor function.[30][31][32][33][34]
Another clinically relevant manifestation with regard to the RN can be seen in patients with substantial brain damage. Specifically, the involuntary posture that a patient demonstrates can help localize the lesion of interest. In decorticate rigidity, flexion of the upper extremities illustrates an intact RN (and rubrospinal tract). If the lesion reaches the RN (and, therefore, the midbrain), the upper extremities demonstrate extended posture, which is referred to as decerebrate posturing.[35]
The third (and much less common) clinical manifestation regarding direct damage to red nuclei involves hypertrophic olivary degeneration and, ultimately, palatal myoclonus (and dysphagia), [36] by which patients’ diaphragm, laryngeal muscles, as well as the soft palate and pharyngopalatine arch move in a rhythmic and involuntary jerking motion.[37]
Fourth, lesions of the RN may lead to various third nerve palsies due to the intimate anatomical relationship between it and the oculomotor nerve. Specifically, fibers of cranial nerve III travel alongside the RN as they leave the oculomotor nerve nucleus and pass ventrally through the midbrain.[38] It is also worth noting that given the close proximity between the dentate nucleus of the cerebral cortex, the cerebellum, and the inferior olivary nucleus, there are a number of rare yet academically notable syndromes that manifest secondary to lesions within this network. There are two specific associated syndromes worth noting, and the first is colloquially referred to as Benedikt Syndrome (paramedian midbrain syndrome), which presents as ipsilateral cranial nerve III palsy, contralateral hemiataxia with intention tremor, and contralateral hemiparesis.[39][40] The second is Claude Syndrome, which encompasses all the features of Benedikt syndrome as well as an associated asynergy and dysdiadochokinesia due to a lesion of the adjacent superior cerebellar peduncle.[41]
Fifth, there is a rare autosomal recessive disorder known as Woodhouse-Sakati Syndrome, characterized by hypogonadism, adolescent-onset diabetes mellitus, hypothyroidism, and alopecia.[42] Additional neurologic findings include bilateral sensorineural hearing loss in childhood, mild intellectual disability, and various extrapyramidal findings.[42] These changes are caused by mutations in the DCAF17 gene. As a result of these changes, there is excess iron deposition among several structures within the brain, including the substantia nigra, red nucleus, and dentate nucleus.[43]
Lastly, there is consideration given towards the interplay between the RN and Parkinson disease.[27] Although the exact mechanism remains unknown, a number of studies have explored the potential relationships, including the overall RN firing rate in relation to Parkinson disease,[27] the relationship between the iron content of RN and the likelihood of levodopa-induced dyskinesia development,[44] and the relationship between RN volume and Parkinson disease-associated motor symptoms.[45][46] Similarly, and as mentioned previously, the functional and expressive similarities between the RN and the subthalamic nuclei also present difficulties with regard to treating Parkinson disease via deep brain stimulation, and also provide obstacles in better understanding this disease.[27][26] Of related note, the red nucleus (as well as the inferior olivary nucleus) has been theorized to play a role in essential tremor but remains in question.[47]
Media
(Click Image to Enlarge)
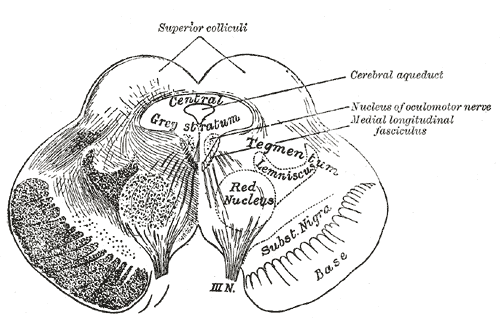
The Midbrain or Mesencephalon. Transverse section of the mid-brain at the level of superior colliculi, optic nerve, cerebral aqueduct, nucleus of oculomotor nerve, medial longitudinal fasciculus, red nucleus, tegmentum, and lemniscus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
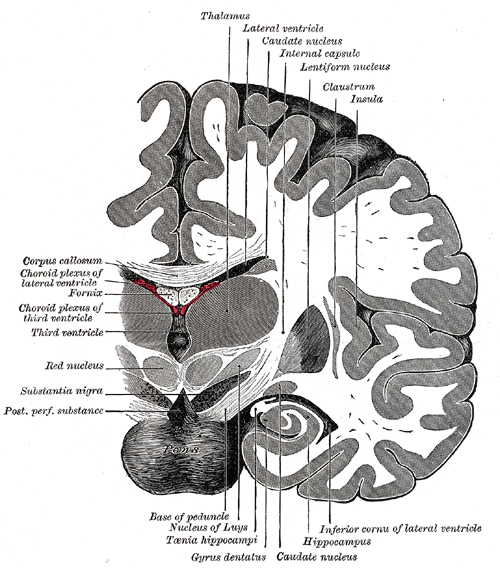
The Fore-brain or Prosencephalon, Coronal section of brain immediately in front of pons, Thalamus, Lateral ventricle, Caudate nucleus, Internal capsule, Lentiform nucleus, Claustrum, Insula, Hippocampus, Gyrus dentatus, Red Nucleus, Fornix, Corpus callosum
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Red nucleus Image courtesy S Bhimji MD
References
Cacciola A, Milardi D, Basile GA, Bertino S, Calamuneri A, Chillemi G, Paladina G, Impellizzeri F, Trimarchi F, Anastasi G, Bramanti A, Rizzo G. The cortico-rubral and cerebello-rubral pathways are topographically organized within the human red nucleus. Scientific reports. 2019 Aug 20:9(1):12117. doi: 10.1038/s41598-019-48164-7. Epub 2019 Aug 20 [PubMed PMID: 31431648]
Yamaguchi K, Goto N. Development of the human magnocellular red nucleus: a morphological study. Brain & development. 2006 Aug:28(7):431-5 [PubMed PMID: 16516425]
Massion J. Red nucleus: past and future. Behavioural brain research. 1988 Apr-May:28(1-2):1-8 [PubMed PMID: 3289561]
Level 3 (low-level) evidenceten Donkelaar HJ. Evolution of the red nucleus and rubrospinal tract. Behavioural brain research. 1988 Apr-May:28(1-2):9-20 [PubMed PMID: 3289562]
Level 3 (low-level) evidenceOnodera S, Hicks TP. A comparative neuroanatomical study of the red nucleus of the cat, macaque and human. PloS one. 2009 Aug 13:4(8):e6623. doi: 10.1371/journal.pone.0006623. Epub 2009 Aug 13 [PubMed PMID: 19675676]
Level 3 (low-level) evidencePatt S, Gerhard L, Zill E. A Golgi study on the red nucleus in man. Histology and histopathology. 1994 Jan:9(1):7-10 [PubMed PMID: 8003824]
Miller LE, van Kan PL, Sinkjaer T, Andersen T, Harris GD, Houk JC. Correlation of primate red nucleus discharge with muscle activity during free-form arm movements. The Journal of physiology. 1993 Sep:469():213-43 [PubMed PMID: 8271199]
Level 3 (low-level) evidenceLavoie S, Drew T. Discharge characteristics of neurons in the red nucleus during voluntary gait modifications: a comparison with the motor cortex. Journal of neurophysiology. 2002 Oct:88(4):1791-814 [PubMed PMID: 12364507]
Level 3 (low-level) evidenceUlfig N, Chan WY. Differential expression of calcium-binding proteins in the red nucleus of the developing and adult human brain. Anatomy and embryology. 2001 Feb:203(2):95-108 [PubMed PMID: 11218063]
Hicks TP, Onodera S. The mammalian red nucleus and its role in motor systems, including the emergence of bipedalism and language. Progress in neurobiology. 2012 Feb:96(2):165-75. doi: 10.1016/j.pneurobio.2011.12.002. Epub 2012 Jan 2 [PubMed PMID: 22230734]
Level 3 (low-level) evidenceYang JF, Stephens MJ, Vishram R. Infant stepping: a method to study the sensory control of human walking. The Journal of physiology. 1998 Mar 15:507 ( Pt 3)(Pt 3):927-37 [PubMed PMID: 9508851]
Level 3 (low-level) evidenceReid EK, Norris SA, Taylor JA, Hathaway EN, Smith AJ, Yttri EA, Thach WT. Is the parvocellular red nucleus involved in cerebellar motor learning? Current trends in neurology. 2009 Jan 1:3():15-22 [PubMed PMID: 21743781]
Lang EJ, Apps R, Bengtsson F, Cerminara NL, De Zeeuw CI, Ebner TJ, Heck DH, Jaeger D, Jörntell H, Kawato M, Otis TS, Ozyildirim O, Popa LS, Reeves AM, Schweighofer N, Sugihara I, Xiao J. The Roles of the Olivocerebellar Pathway in Motor Learning and Motor Control. A Consensus Paper. Cerebellum (London, England). 2017 Feb:16(1):230-252. doi: 10.1007/s12311-016-0787-8. Epub [PubMed PMID: 27193702]
Level 3 (low-level) evidenceFisher CM. The posterior cerebral artery syndrome. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 1986 Aug:13(3):232-9 [PubMed PMID: 3742339]
Level 3 (low-level) evidenceJaved K, Reddy V, M Das J. Neuroanatomy, Posterior Cerebral Arteries. StatPearls. 2024 Jan:(): [PubMed PMID: 30860709]
Huang M, Liu M, Li X. [The analgesic effect of red nucleus and preliminary research on its mechanism]. Zhen ci yan jiu = Acupuncture research. 1992:17(3):166-70 [PubMed PMID: 1339625]
Level 3 (low-level) evidenceSteffens H, Rathelot JA, Padel Y. Effects of noxious skin heating on spontaneous cell activity in the magnocellular red nucleus of the cat. Experimental brain research. 2000 Mar:131(2):215-24 [PubMed PMID: 10766273]
Level 3 (low-level) evidenceGuo YJ, Li HN, Ding CP, Han SP, Wang JY. Red nucleus interleukin-1β evokes tactile allodynia through activation of JAK/STAT3 and JNK signaling pathways. Journal of neuroscience research. 2018 Dec:96(12):1847-1861. doi: 10.1002/jnr.24324. Epub 2018 Sep 14 [PubMed PMID: 30216497]
Ding CP, Guo YJ, Li HN, Wang JY, Zeng XY. Red nucleus interleukin-6 participates in the maintenance of neuropathic pain through JAK/STAT3 and ERK signaling pathways. Experimental neurology. 2018 Feb:300():212-221. doi: 10.1016/j.expneurol.2017.11.012. Epub 2017 Nov 26 [PubMed PMID: 29183675]
Zhang Q, Wang J, Duan MT, Han SP, Zeng XY, Wang JY. NF-κB, ERK, p38 MAPK and JNK contribute to the initiation and/or maintenance of mechanical allodynia induced by tumor necrosis factor-alpha in the red nucleus. Brain research bulletin. 2013 Oct:99():132-9. doi: 10.1016/j.brainresbull.2013.10.008. Epub 2013 Oct 23 [PubMed PMID: 24161765]
Level 3 (low-level) evidenceWang J, Yu J, Ding CP, Han SP, Zeng XY, Wang JY. Transforming growth factor-beta in the red nucleus plays antinociceptive effect under physiological and pathological pain conditions. Neuroscience. 2015 Apr 16:291():37-45. doi: 10.1016/j.neuroscience.2015.01.059. Epub 2015 Feb 4 [PubMed PMID: 25662509]
Level 3 (low-level) evidenceWang ZH, Zeng XY, Han SP, Fan GX, Wang JY. Interleukin-10 of red nucleus plays anti-allodynia effect in neuropathic pain rats with spared nerve injury. Neurochemical research. 2012 Aug:37(8):1811-9. doi: 10.1007/s11064-012-0795-0. Epub 2012 May 15 [PubMed PMID: 22584848]
Level 3 (low-level) evidenceDing CP, Xue YS, Yu J, Guo YJ, Zeng XY, Wang JY. The Red Nucleus Interleukin-6 Participates in the Maintenance of Neuropathic Pain Induced by Spared Nerve Injury. Neurochemical research. 2016 Nov:41(11):3042-3051 [PubMed PMID: 27485712]
Li X, Wang J, Wang Z, Dong C, Dong X, Jing Y, Yuan Y, Fan G. Tumor necrosis factor-α of Red nucleus involved in the development of neuropathic allodynia. Brain research bulletin. 2008 Nov 25:77(5):233-6. doi: 10.1016/j.brainresbull.2008.08.025. Epub 2008 Sep 25 [PubMed PMID: 18824078]
Level 3 (low-level) evidenceZhang Q, Yu J, Wang J, Ding CP, Han SP, Zeng XY, Wang JY. The Red Nucleus TNF-α Participates in the Initiation and Maintenance of Neuropathic Pain Through Different Signaling Pathways. Neurochemical research. 2015 Jul:40(7):1360-71. doi: 10.1007/s11064-015-1599-9. Epub 2015 May 8 [PubMed PMID: 25952358]
Okun MS, Tagliati M, Pourfar M, Fernandez HH, Rodriguez RL, Alterman RL, Foote KD. Management of referred deep brain stimulation failures: a retrospective analysis from 2 movement disorders centers. Archives of neurology. 2005 Aug:62(8):1250-5 [PubMed PMID: 15956104]
Level 2 (mid-level) evidenceRodriguez-Oroz MC, Rodriguez M, Leiva C, Rodriguez-Palmero M, Nieto J, Garcia-Garcia D, Luis Zubieta J, Cardiel C, Obeso JA. Neuronal activity of the red nucleus in Parkinson's disease. Movement disorders : official journal of the Movement Disorder Society. 2008 Apr 30:23(6):908-11. doi: 10.1002/mds.22000. Epub [PubMed PMID: 18383534]
Level 3 (low-level) evidenceMerola A, Mandybur G, Biddell K, Tareen TK, Wilson-Perez H, Espay AJ, Duker AP. Subthalamic or red nucleus? A puzzling question arising during intraoperative recording for DBS. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2017 Apr:128(4):558-560. doi: 10.1016/j.clinph.2017.01.011. Epub 2017 Jan 28 [PubMed PMID: 28231473]
Ellis TM, Foote KD, Fernandez HH, Sudhyadhom A, Rodriguez RL, Zeilman P, Jacobson CE 4th, Okun MS. Reoperation for suboptimal outcomes after deep brain stimulation surgery. Neurosurgery. 2008 Oct:63(4):754-60; discussion 760-1. doi: 10.1227/01.NEU.0000325492.58799.35. Epub [PubMed PMID: 18981887]
Level 2 (mid-level) evidenceKim H, Lee H, Jung KI, Ohn SH, Yoo WK. Changes in Diffusion Metrics of the Red Nucleus in Chronic Stroke Patients With Severe Corticospinal Tract Injury: A Preliminary Study. Annals of rehabilitation medicine. 2018 Jun 27:42(3):396-405. doi: 10.5535/arm.2018.42.3.396. Epub 2018 Jun 27 [PubMed PMID: 29961737]
Yang HS, Kwon HG, Hong JH, Hong CP, Jang SH. The rubrospinal tract in the human brain: diffusion tensor imaging study. Neuroscience letters. 2011 Oct 17:504(1):45-8. doi: 10.1016/j.neulet.2011.08.054. Epub 2011 Sep 3 [PubMed PMID: 21911039]
Level 3 (low-level) evidenceYeo SS, Jang SH. Changes in red nucleus after pyramidal tract injury in patients with cerebral infarct. NeuroRehabilitation. 2010:27(4):373-7. doi: 10.3233/NRE-2010-0622. Epub [PubMed PMID: 21160128]
Level 2 (mid-level) evidenceBelhaj-Saïf A, Cheney PD. Plasticity in the distribution of the red nucleus output to forearm muscles after unilateral lesions of the pyramidal tract. Journal of neurophysiology. 2000 May:83(5):3147-53 [PubMed PMID: 10805709]
Level 3 (low-level) evidenceRüber T, Schlaug G, Lindenberg R. Compensatory role of the cortico-rubro-spinal tract in motor recovery after stroke. Neurology. 2012 Aug 7:79(6):515-22. doi: 10.1212/WNL.0b013e31826356e8. Epub 2012 Jul 25 [PubMed PMID: 22843266]
WARD AA Jr. Decerebrate rigidity. Journal of neurophysiology. 1947 Mar:10(2):89-103 [PubMed PMID: 20291835]
Telford R, Vattoth S. MR anatomy of deep brain nuclei with special reference to specific diseases and deep brain stimulation localization. The neuroradiology journal. 2014 Feb:27(1):29-43 [PubMed PMID: 24571832]
Pearce JM. Palatal Myoclonus (syn. Palatal Tremor). European neurology. 2008:60(6):312-5. doi: 10.1159/000159929. Epub 2008 Oct 3 [PubMed PMID: 18832845]
Level 3 (low-level) evidenceBrazis PW. Localization of lesions of the oculomotor nerve: recent concepts. Mayo Clinic proceedings. 1991 Oct:66(10):1029-35 [PubMed PMID: 1921485]
Bandt SK, Anderson D, Biller J. Deep brain stimulation as an effective treatment option for post-midbrain infarction-related tremor as it presents with Benedikt syndrome. Journal of neurosurgery. 2008 Oct:109(4):635-9. doi: 10.3171/JNS/2008/109/10/0635. Epub [PubMed PMID: 18826349]
Level 3 (low-level) evidenceAkdal G, Kutluk K, Men S, Yaka E. Benedikt and "plus-minus lid" syndromes arising from posterior cerebral artery branch occlusion. Journal of the neurological sciences. 2005 Jan 15:228(1):105-7 [PubMed PMID: 15607218]
Level 3 (low-level) evidenceBroadley SA, Taylor J, Waddy HM, Thompson PD. The clinical and MRI correlate of ischaemia in the ventromedial midbrain: Claude's syndrome. Journal of neurology. 2001 Dec:248(12):1087-9 [PubMed PMID: 12013587]
Level 3 (low-level) evidenceLouro P, Durães J, Oliveira D, Paiva S, Ramos L, Macário MC. Woodhouse-Sakati Syndrome: First report of a Portuguese case. American journal of medical genetics. Part A. 2019 Nov:179(11):2237-2240. doi: 10.1002/ajmg.a.61303. Epub 2019 Jul 26 [PubMed PMID: 31347785]
Level 3 (low-level) evidenceAbusrair AH, Bohlega S, Al-Semari A, Al-Ajlan FS, Al-Ahmadi K, Mohamed B, AlDakheel A. Brain MR Imaging Findings in Woodhouse-Sakati Syndrome. AJNR. American journal of neuroradiology. 2018 Dec:39(12):2256-2262. doi: 10.3174/ajnr.A5879. Epub 2018 Nov 8 [PubMed PMID: 30409855]
Lewis MM, Du G, Kidacki M, Patel N, Shaffer ML, Mailman RB, Huang X. Higher iron in the red nucleus marks Parkinson's dyskinesia. Neurobiology of aging. 2013 May:34(5):1497-503. doi: 10.1016/j.neurobiolaging.2012.10.025. Epub 2012 Nov 21 [PubMed PMID: 23177595]
Philippens IHCHM, Wubben JA, Franke SK, Hofman S, Langermans JAM. Involvement of the Red Nucleus in the Compensation of Parkinsonism may Explain why Primates can develop Stable Parkinson's Disease. Scientific reports. 2019 Jan 29:9(1):880. doi: 10.1038/s41598-018-37381-1. Epub 2019 Jan 29 [PubMed PMID: 30696912]
Camlidag I, Kocabicak E, Sahin B, Jahanshahi A, Incesu L, Aygun D, Yildiz O, Temel Y, Belet U. Volumetric analysis of the subthalamic and red nuclei based on magnetic resonance imaging in patients with Parkinson's disease. The International journal of neuroscience. 2014 Apr:124(4):291-5. doi: 10.3109/00207454.2013.843091. Epub 2013 Sep 26 [PubMed PMID: 24020352]
Level 2 (mid-level) evidenceLouis ED, Lenka A. The Olivary Hypothesis of Essential Tremor: Time to Lay this Model to Rest? Tremor and other hyperkinetic movements (New York, N.Y.). 2017:7():473. doi: 10.7916/D8FF40RX. Epub 2017 Jul 13 [PubMed PMID: 28966877]