Introduction
Pyogenic granuloma (PG), sometimes known as granuloma pyogenicum, refers to a common, acquired, benign vascular tumor that arises in tissues such as the skin and mucous membranes (see Image. Pyogenic Granuloma).[1] The scientifically accurate term for this entity is lobular capillary hemangioma.[2] In the past, pyogenic granulomas were thought to be an exaggerated granulomatous reaction to an infectious or pyogenic insult, which led to the use of terms such as ‘pyogenic granuloma’ and ‘granuloma pyogenicum.’ However, the term pyogenic granuloma is a misnomer that may initially cause confusion.
The lesion grossly appears as a solitary, red, pedunculated papule that is very friable. Less commonly, it may present as a sessile plaque. It shows rapid exophytic growth, with a surface that often undergoes ulceration. This is often seen on cutaneous or mucosal surfaces. Among the latter, it is most commonly seen within the oral cavity. Rarely, it may occur at other sites within the gastrointestinal tract. When it occurs in the intraoral mucosa in the setting of pregnancy, notably on the gingiva, it is referred to as granuloma gravidarum, granuloma of pregnancy, or epulis gravidarum, usually in the second or third trimester.[3] There is a case reported in the literature where a patient developed multiple disseminated lesions while on therapy with oral contraceptive pills and one report of the development of lesions after a renal transplant.[4][5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Various factors are implicated in the etiopathogenesis of this entity, but the exact cause is unknown. Studies investigating specific angiogenic factors and signal transduction pathways have yet to implicate a single pathway for the pathogenesis of the lesion. Proposed mechanisms emphasize the importance of insults resulting in an imbalance of pro-angiogenic and anti-angiogenic factors, which lead to a rapid proliferation of capillaries of a neovascular, friable, and lobulated character. Reactive granulation tissue from minor trauma may be contributory; however, studies attribute only up to 7% of these lesions directly to a history of trauma.[3][6][7] Other possible predisposing factors may include infections and preexisting vascular malformations.
Hormonal factors appear to play a role in the pregnancy-associated phenotype of this lesion.[8] There is also a later peak incidence in women, typically during childbearing years.[9] Opponents of this theory emphasize the paucity of vaginal mucosal lesions, together with a slight predilection of cutaneous lesions in men.[9] It is hypothesized that estrogens and other sex hormones exaggerate inflammatory responses in gingival tissue, particularly in pregnancy.[10] Further studies must be undertaken to determine their true significance in the etiology of this entity. Certain variants of lobular capillary hemangioma have also shown an association with medication use. Of these variants, multiple periungual pyogenic granulomas occur most frequently in association with medications (reports suggest up to 30% of these are associated with medications) and are also associated with other chronic dermatoses such as atopic dermatitis and psoriasis.[11][12]
Drugs implicated most often include:
- Systemic and topical retinoids
- Antiretrovirals
- Indinavir (HIV protease inhibitor)[13]
- Antineoplastics
- Immunosuppressive agents
Disseminated pyogenic granulomas, a rare entity, have been documented to occur with isotretinoin use in patients with severe nodulocystic acne and the use of granulocyte colony-stimulating factor (G-CSF) in immunodeficient patients.[25][26][27][28] Intraoral pyogenic granulomas are seen in patients on cyclosporine and tacrolimus after a hematopoietic stem cell transplant.[29][30][31][32] Several case reports support this hypothesis, especially with patients treated for either acute or chronic graft versus host disease with cyclosporine or tacrolimus.[29] PG may arise spontaneously within or following laser treatment or cryotherapy to a preexisting vascular malformation, such as capillary (port-wine stain)or arteriovenous malformation.[33][34][35]
Epidemiology
Pyogenic granuloma may be seen in patients of all ages. Conflicting reports exist on the epidemiologic pattern of disease. In one review, the incidence peaked in the second decade of life, and the lesion showed a slight male preponderance in certain studies.[9] However, mucosal lesions were more common in females than males in this review and were seen predominantly in the fourth decade of life in this cohort. In another review, the ratio of men to women was 1 to 1.2.[36] In this review, when considering both cutaneous and mucosal variants, male patients appear to present at a younger age, typically from childhood to the late twenties, compared to women, who usually present later in life between the ages of thirty to forty.[36] When considered on its own, mucosal pyogenic granuloma appears to occur at any time in men. In comparison, most cases in women occur before age forty.[36] Results from a pediatric study showed the average age at diagnosis was 6 to 10 years, with a male sex preponderance.[37]
Histopathology
Histologically, a lobular capillary hemangioma consists of lobular aggregates of capillary-sized vessels, with each lobule containing a central feeder vessel. These develop within highly vascular granulation tissue, with the lobules or tufts of thin-walled capillaries embedded within a loose fibrous stroma, with scattered fibroblasts and a variegated inflammatory infiltrate (see Image. Granulation Tissue, H/E, 20x).
At low power, the architecture resembles a well-circumscribed, exophytic, polypoid mass (see Image. Pyogenic Granuloma, H/E 4x). The overlying epidermis is variably involved but often thinned or atrophic, progressing to erosion and ulceration with severity. Features of superadded infection may be seen. An epidermal collarette is often present, composed of either acanthotic elongated rete ridges or hyperplasia of adnexal structures that separate these lesions from the underlying dermis (see Image. Pyogenic Granuloma H/E 10x). Within the papillary and upper reticular dermis, collections of these capillary-sized vessels are arranged into lobules and separated by fibromyxoid stroma.[2]
Within the stroma, a scarce, mixed inflammatory infiltrate is noted, consisting of lymphocytes, neutrophils, plasma cells, or mast cells, resembling normal granulation tissue. A study noted a normal number of mast cells within these lesions compared to increased numbers in the proliferative phase of a typical hemangioma.[7] The capillary lobules in the lesion's superficial regions are more distinctive and lined by flattened to slightly plump endothelial cells, with a progressive change in the deeper parts of the lesion, where increased cellularity leads to overlapping, small, and indistinct lumens. Mitotic activity within the lesion is highly variable. Immunohistochemistry staining is often unnecessary, given the characteristic clinical history and histologic architecture. Atypical lesions may, however, necessitate the use of IHC stains. The lesion stains are positive for vascular markers like CD31, CD34, and factor VIII antigen, but unlike infantile hemangioma, they are negative for glucose transporter-1 (GLUT1).[38][39]
When seen, intravascular pyogenic granulomas typically occur within a vein and resemble cutaneous lesions with a lobular capillary proliferation set in a fibromyxoid stroma. The lesion hangs from a fibrovascular stalk that connects to the intima of the vein. On the other hand, a granuloma is represented by an aggregation of macrophages with or without surrounding inflammatory infiltrate.[40] These develop in response to an antigenic stimulus, often an infectious pathogen or a foreign body. The initial histologic misconception that pyogenic granulomas were granulomatous with an additional mixed inflammatory infiltrate consisting of neutrophils led early investigators to assume these lesions were most likely analogous to traditional granulomas. Extensive investigations have since failed to identify a definite infectious agent as a trigger for these lesions, and these lesions are neither pyogenic nor granulomatous. To correct the misleading terminology, Mills et al. suggested using the more accurately descriptive term lobular capillary hemangioma.[2] However, the older term continues to see routine use.
History and Physical
A lobular capillary hemangioma typically starts as a small, red papule; then it undergoes a variable, sometimes rapid, exophytic growth phase over weeks to months, eventually stabilizing in size. The color may vary from red to reddish-brown or purple. The diameter varies from a few millimeters for small lesions to several centimeters for larger lesions. Lesions are typically solitary, but satellite lesions may develop in proximity, and sometimes disseminated lesions may be noted. Mature lesions are polypoid or pedunculated and have a "collarette" of scale at the base of the lesion. This epidermal collarette may help identify the lesion, but it is not unique to this entity and may be seen in other conditions that show lesions erupting rapidly through the epidermis. Sessile lesions are rare. The surface is often friable, and the lesion can show profuse bleeding with even minor trauma. Bleeding is recurrent due to unavoidable trauma and may become difficult to control. Patients present to the clinic with band-aids applied over the lesions, an attempt to prevent trauma and bleeding from the lesion – colloquially termed the "band-aid sign."
A lobular capillary hemangioma can occur on any normal cutaneous or mucosal site. Cutaneous lesions occur more frequently than mucosal lesions.[9] In some instances, the lesion may also occur over vascular malformations, such as a nevus flammeus (port-wine stain). There is conflicting data regarding the most common site of involvement for cutaneous and mucosal PG. In adults, cutaneous PG appears to occur more frequently on the trunk and extremities (where it is more common on the upper than the lower extremities), followed by head and neck lesions, as opposed to children, in whom the lesions have a predilection for the head and neck region, followed by the trunk and extremities (see Image. Pyogenic Granuloma).[7][9] A unique entity within cutaneous PG is subungual or periungual PG, which usually presents at the proximal or lateral nail fold and may even erupt on multiple digits.
For mucosal PG, common locations include lips and gingival mucosa. Some studies cite the tongue as the most common site, followed by the gingivae, nasal mucosa, conjunctiva, cervix, and vagina.[2][9] Other authors suggest that the gingiva is the most common site for mucosal PG.[41][42] In pregnancy, the lesion occurs most frequently over the buccal mucosa and gingivae. Multiple lesions can occur in one of two distinct clinical variations: satellite lesions around a primary lesion or a disseminated form. Satellite forms favor the trunk, involving perilesional skin near the initial lesion following treatment or trauma.[33] Disseminated lesions are extremely rare but have been reported in the literature, occurring in an eruptive fashion with no predilection for any particular site. Occasionally, lobular capillary hemangiomas are found in subcutaneous or intravascular locations. Subcutaneous pyogenic granulomas typically occur in females and present as a well-circumscribed subcutaneous nodule.[43] Intravenous pyogenic granulomas typically present as a slow-growing, well-circumscribed, soft, subcutaneous nodule typically on the neck or upper extremities.[44][45] Rarely lobular capillary hemangioma develops in the gastrointestinal tract, where it mimics polyps.[46] Gastrointestinal tract lesions may be asymptomatic or present with overt bleeding or obscure chronic bleeding, causing anemia.[46]
A summary of certain clinical variants of lobular capillary hemangioma is described below:
- Digital or periungual pyogenic granulomas, which may be solitary or multiple:
- A solitary periungual pyogenic granuloma may mimic other periungual lesions, such as acute paronychia, and occur secondary to acute or chronic local trauma or infection.
- Multiple periungual pyogenic granulomas occur most frequently in association with medications (reports suggest up to 30% of these are associated with medications) but are also seen in association with other chronic dermatoses such as atopic dermatitis and psoriasis.[11][12]
- Satellite pyogenic granulomas that arise in an eruptive fashion around the initial sessional area are extremely rare. Reported cases classically occur after trauma to the primary lesion, typically after treatment by excision.[47][48]
- Disseminated pyogenic granulomas, although rare, have been documented to occur either spontaneously or after trauma, such as burns.[49][50][51][52] Certain medications are also implicated, including isotretinoin use in patients with severe nodulocystic acne and the use of granulocyte colony-stimulating factor (G-CSF) in immunodeficient patients.[25][26][27][28]
- Intraoral pyogenic granuloma appears to have a predilection for immunosuppressed patients, most often after a hematopoietic stem cell transplant.[29][30][31][32]
Evaluation
Lobular capillary hemangioma is usually a clinical diagnosis based on history and classical clinical findings. The history should include inquiries into previous trauma, association with pregnancy, and a thorough review of medications. In some instances, a dermoscopic examination is valuable. Lesions show a pink or red homogenous papule with a scaly, white "collarette."[53] Occasionally, white lines that intersect may be seen and represent fibrous septa.[53] A histologic examination is warranted if a diagnosis cannot be achieved on clinical grounds. Some may choose to excise these lesions to alleviate patient anxiety rather than diagnostic uncertainty. Irrespective of the deciding factor for excision, it is strongly recommended that the tissue is sent for histopathologic confirmation to rule out any other sinister lesions.
Treatment / Management
Lobular capillary hemangiomas show frequent ulceration and bleeding, which is the usual cause that warrants treatment. Clinical trials are limited; hence, there is no accepted standard of care for treating these lesions. Different treatments have variable degrees of success and variable rates of recurrence. No matter the treatment, the patient should be counseled about the risk of recurrence. In non-visible areas, complete excision is the preferred method of lesion removal because of its lower rates of recurrence, and it provides an excellent specimen for histopathologic characterization. The excision is performed under local anesthesia. For sessile or recurrent lesions, surgical excision with suturing is preferred and results in less postoperative bleeding with a lower recurrence rate.[54] Shave excision or curettage followed by electrocautery may be used for cosmetic areas, but recurrence is more common with these modalities.[55] Other modalities include non-surgical avenues such as cryotherapy, electrocautery or chemical cautery with silver nitrate without excision, and laser therapy.[55][56][57] Lasers that have been used include pulsed dye laser (PDL) or CO2 lasers and long-pulsed 1,064 nm Nd:YAG laser either on their own or combined with surgical intervention.[58][59][60] For small lesions in cosmetically sensitive areas or lesions in children, practitioners may consider non-operative management with pulsed dye laser, CO2 laser ablation, or electrocautery if laser therapies are not available.[54](A1)
Medical management is generally not recommended. A variety of topical or intralesional treatments have been used with variable responses. These include topical imiquimod cream, alitretinoin gel, timolol, propranolol, and even phenols for periungual lesions.[61][62][63][64][65] Intralesional therapy with corticosteroids and sclerosants such as ethanolamine oleate, sodium tetradecyl sulfate, polidocanol, and bleomycin have shown sporadic patient benefits.[66][67][68][69][70] In cases of pregnancy or medication-induced lobular capillary hemangiomas, the recurrence rate after treatment is higher. Medication should be discontinued if possible. For patients on antineoplastic medications, where stopping the medication is not possible, management is symptomatic. For example, in the case of epidermal growth factor receptor inhibitor-related lesions, the Multinational Association for Supportive Care in Cancer (MASCC) Skin Toxicity Study Group has published guidelines preventing and treating lobular capillary hemangiomas, recommending weekly chemical cauterization, electrodesiccation, or nail avulsion.[71](A1)
Differential Diagnosis
While lobular capillary hemangioma is easily diagnosed based on a history and examination, it is important to consider certain red flag diagnoses that may prove harmful. These include lesions such as (this is by no means an exhaustive list):
- Amelanotic melanoma
- Squamous cell carcinoma
- Basal cell carcinoma
- Angiosarcoma
Bacillary angiomatosis or Kaposi sarcoma should also be included in the differential in immunosuppressed individuals.
Benign lesions that may need to be distinguished from lobular capillary hemangiomas include:
- Hemangiomas
- Irritated melanocytic nevi
- Spitz nevus
- Warts
- An acquired digital fibrokeratoma
- Granulation tissue from minor trauma or scratching
- Glomus tumor
- Angiolymphoid hyperplasia with eosinophilia
The list of differential diagnoses on histopathology includes other forms of capillary hemangiomas, including, but not limited to, acquired tufted angioma, glomeruloid hemangioma, and infectious angiomatoses such as bacillary epithelioid angiomatosis and verruga peruana.[72][73]
Prognosis
These lesions have no malignant potential. However, since they do not regress spontaneously and may bleed, ulcerate, or be cosmetically disfiguring, they may necessitate treatment on these grounds.[74] Oral pyogenic granulomas occurring in pregnant women usually regress once they deliver their child.[75] Partial resection by shave excision or curettage may lead to recurrence in the future; hence complete primary excision is preferred. For recurrence, a complete surgical excision is warranted.
Complications
Possible complications of lobular capillary hemangioma include:
- Ulceration
- Hemorrhage from trauma to the lesion
- Secondary infections
- Cosmetic disfigurement may cause psychological distress to the patient, particularly when the lesion is on the face [74]
Deterrence and Patient Education
Patients typically need reassurance for this condition since they may be worried about more sinister conditions. They should be discouraged from scratching or picking at the lesion and must take some precautions to avoid trauma or secondary infection. They should be advised about the risk of recurrence with partial excisions and the risk of scarring with a total surgical excision. The decision of which modality to use for the lesion must be arrived at jointly by the patient and their physician.
Enhancing Healthcare Team Outcomes
Lobular capillary hemangiomas are friable lesions that may lead to undue anxiety for patients, parents, and healthcare providers unfamiliar with the lesions and their prognosis. Given their somewhat abrupt onset, patients may present in various settings such as urgent care, primary care, pediatric clinics, dermatology clinics, and podiatry clinics or sometimes even seek an oncologist or surgeon. As these lesions are common in children, pregnant women, and patients on certain medications, a strong link with specialists such as a dermatologist is needed for the appropriate treatment of these lesions by a suitable modality. When these lesions are excised, partially or wholly, specimens must always be sent for histopathologic assessment to rule out red-flag diagnoses.
Media
(Click Image to Enlarge)

Pyogenic Granuloma. This condition refers to a common, acquired, benign vascular tumor that arises in tissues such as the skin and mucous membranes.
(Click Image to Enlarge)

Pyogenic Granuloma, Scalp. In adults, cutaneous pyogenic granuloma occurs more frequently on the trunk and extremities, followed by head and neck lesions; the reverse is true in children.
Contributed by S Verma, MD, MBBS, DVD, FRCP, FAAD
(Click Image to Enlarge)
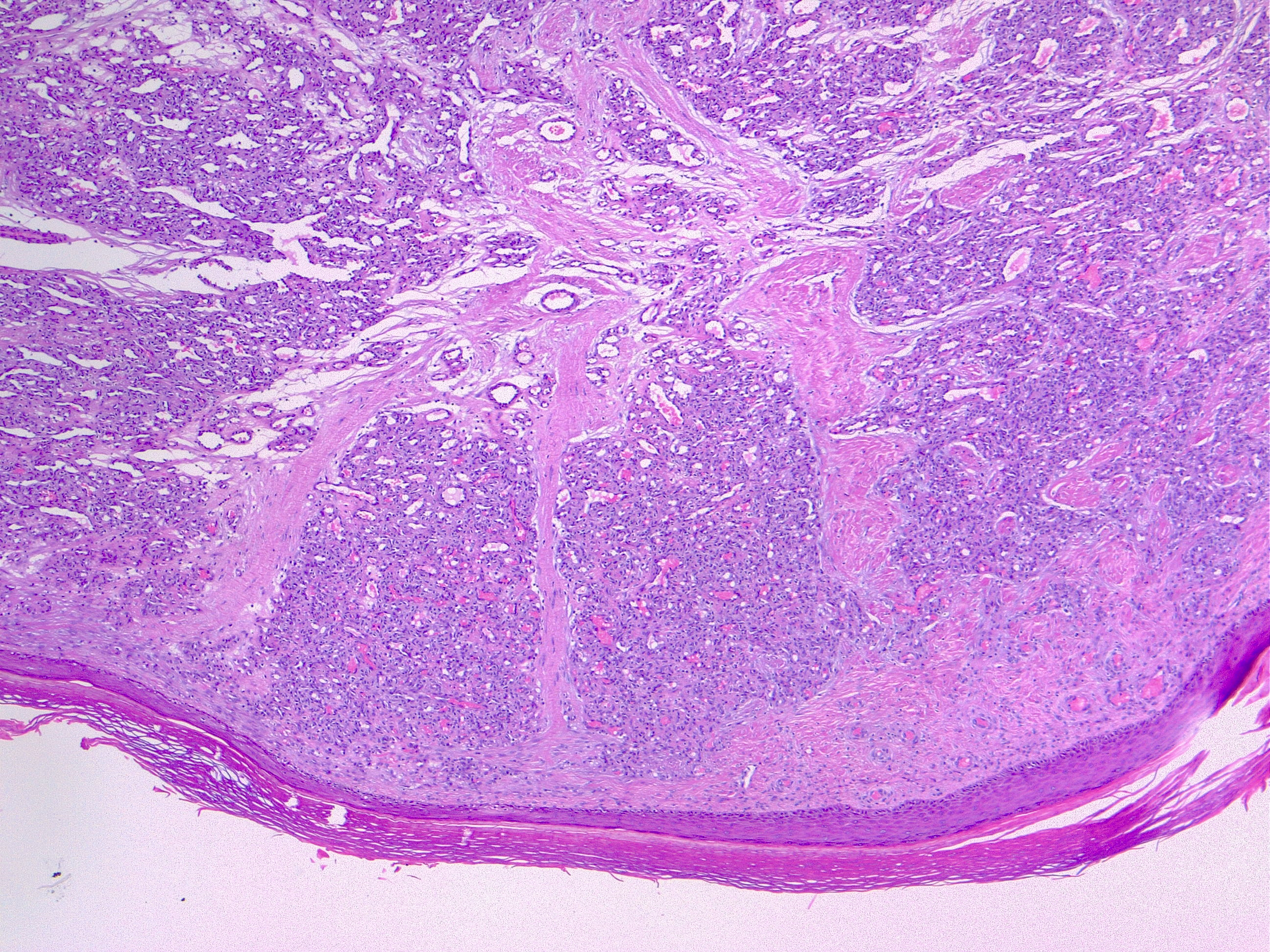
Pyogenic Granuloma, H/E 4×. The lobular arrangement of the capillary vessels is a common feature.
Contributed by F Farci, MD
(Click Image to Enlarge)
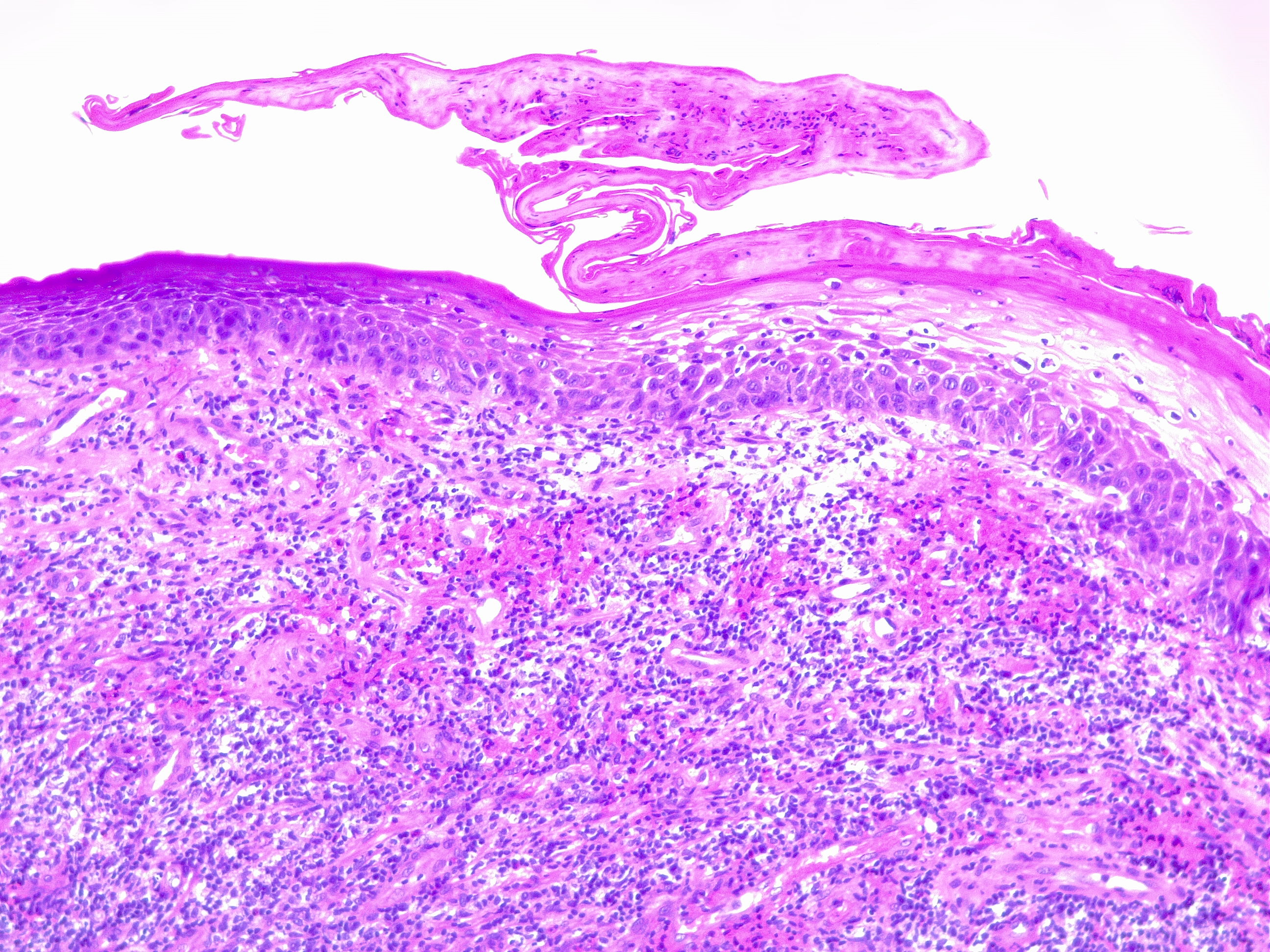
Pyogenic Granuloma H/E 10×. Secondary ulceration and inflammatory changes change the lobular morphology. In this picture, the epidermis is ulcerated, and neutrophils are widely occupying the lesion. An epidermal collarette is present over true granulation tissue of the dermis.
Contributed by F Farci, MD
(Click Image to Enlarge)
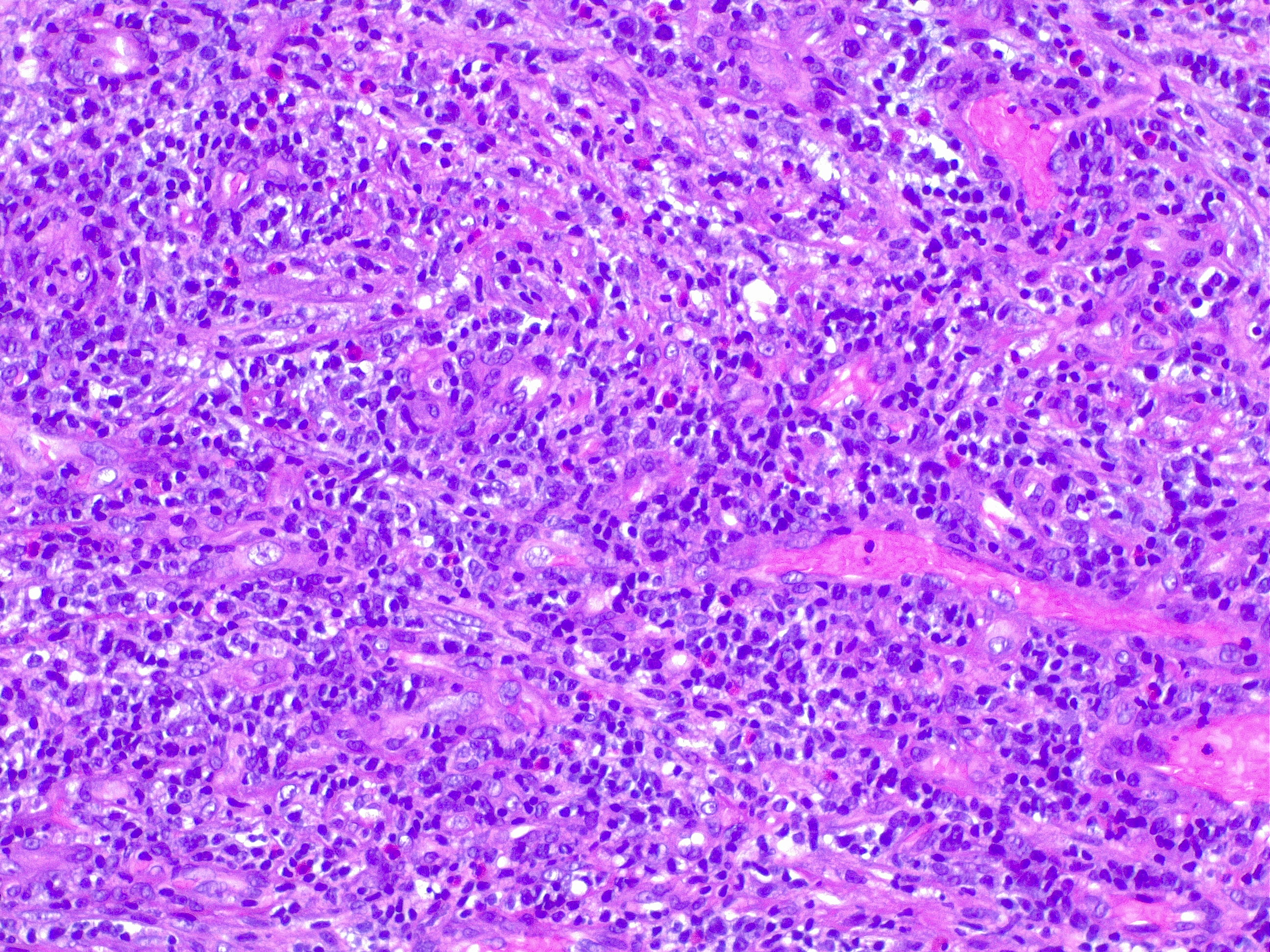
Granulation Tissue, H/E, 20×. In this image, true granulation tissue is formed in a preexisting pyogenic granuloma/angioma. The lobular morphology of pyogenic granuloma can be obscured by ulceration and inflammatory changes.
Contributed by F Farci, MD
References
Wollina U, Langner D, França K, Gianfaldoni S, Lotti T, Tchernev G. Pyogenic Granuloma - A Common Benign Vascular Tumor with Variable Clinical Presentation: New Findings and Treatment Options. Open access Macedonian journal of medical sciences. 2017 Jul 25:5(4):423-426. doi: 10.3889/oamjms.2017.111. Epub 2017 Jul 13 [PubMed PMID: 28785323]
Mills SE, Cooper PH, Fechner RE. Lobular capillary hemangioma: the underlying lesion of pyogenic granuloma. A study of 73 cases from the oral and nasal mucous membranes. The American journal of surgical pathology. 1980 Oct:4(5):470-9 [PubMed PMID: 7435775]
Level 3 (low-level) evidenceAndrikopoulou M, Chatzistamou I, Gkilas H, Vilaras G, Sklavounou A. Assessment of angiogenic markers and female sex hormone receptors in pregnancy tumor of the gingiva. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2013 Aug:71(8):1376-81. doi: 10.1016/j.joms.2013.03.009. Epub 2013 Apr 24 [PubMed PMID: 23623199]
Level 2 (mid-level) evidenceUsui S,Kogame T,Shibuya M,Okamoto N,Toichi E, Case of multiple disseminated cutaneous lobular capillary hemangioma that developed while taking oral contraceptive pills. The Journal of dermatology. 2019 Jun; [PubMed PMID: 30628110]
Level 3 (low-level) evidenceal-Zayer M, da Fonseca M, Ship JA. Pyogenic granuloma in a renal transplant patient: case report. Special care in dentistry : official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry. 2001 Sep-Oct:21(5):187-90 [PubMed PMID: 11803643]
Level 3 (low-level) evidenceArbiser JL, Weiss SW, Arbiser ZK, Bravo F, Govindajaran B, Caceres-Rios H, Cotsonis G, Recavarren S, Swerlick RA, Cohen C. Differential expression of active mitogen-activated protein kinase in cutaneous endothelial neoplasms: implications for biologic behavior and response to therapy. Journal of the American Academy of Dermatology. 2001 Feb:44(2):193-7 [PubMed PMID: 11174372]
Patrice SJ, Wiss K, Mulliken JB. Pyogenic granuloma (lobular capillary hemangioma): a clinicopathologic study of 178 cases. Pediatric dermatology. 1991 Dec:8(4):267-76 [PubMed PMID: 1792196]
Level 2 (mid-level) evidenceJafarzadeh H, Sanatkhani M, Mohtasham N. Oral pyogenic granuloma: a review. Journal of oral science. 2006 Dec:48(4):167-75 [PubMed PMID: 17220613]
Harris MN, Desai R, Chuang TY, Hood AF, Mirowski GW. Lobular capillary hemangiomas: An epidemiologic report, with emphasis on cutaneous lesions. Journal of the American Academy of Dermatology. 2000 Jun:42(6):1012-6 [PubMed PMID: 10827405]
Level 2 (mid-level) evidenceHugoson A. Gingival inflammation and female sex hormones. A clinical investigation of pregnant women and experimental studies in dogs. Journal of periodontal research. Supplement. 1970:5():1-18 [PubMed PMID: 4249979]
Level 3 (low-level) evidenceAlessandrini A, Bruni F, Starace M, Piraccini BM. Periungual Pyogenic Granuloma: The Importance of the Medical History. Skin appendage disorders. 2016 May:1(4):175-8. doi: 10.1159/000444302. Epub 2016 Feb 24 [PubMed PMID: 27386461]
Zaiac MN, Walker A. Nail abnormalities associated with systemic pathologies. Clinics in dermatology. 2013 Sep-Oct:31(5):627-49. doi: 10.1016/j.clindermatol.2013.06.018. Epub [PubMed PMID: 24079592]
Bouscarat F, Bouchard C, Bouhour D. Paronychia and pyogenic granuloma of the great toes in patients treated with indinavir. The New England journal of medicine. 1998 Jun 11:338(24):1776-7 [PubMed PMID: 9625645]
Level 3 (low-level) evidencePiguet V, Borradori L. Pyogenic granuloma-like lesions during capecitabine therapy. The British journal of dermatology. 2002 Dec:147(6):1270-2 [PubMed PMID: 12452889]
Level 3 (low-level) evidenceCurr N, Saunders H, Murugasu A, Cooray P, Schwarz M, Gin D. Multiple periungual pyogenic granulomas following systemic 5-fluorouracil. The Australasian journal of dermatology. 2006 May:47(2):130-3 [PubMed PMID: 16637811]
Level 3 (low-level) evidenceDevillers C, Vanhooteghem O, Henrijean A, Ramaut M, de la Brassinne M. Subungueal pyogenic granuloma secondary to docetaxel therapy. Clinical and experimental dermatology. 2009 Mar:34(2):251-2. doi: 10.1111/j.1365-2230.2008.02799.x. Epub 2008 Dec 22 [PubMed PMID: 19120399]
Level 3 (low-level) evidencePaul LJ, Cohen PR. Paclitaxel-associated subungual pyogenic granuloma: report in a patient with breast cancer receiving paclitaxel and review of drug-induced pyogenic granulomas adjacent to and beneath the nail. Journal of drugs in dermatology : JDD. 2012 Feb:11(2):262-8 [PubMed PMID: 22270214]
Level 3 (low-level) evidenceHigh WA. Gefitinib: a cause of pyogenic granulomalike lesions of the nail. Archives of dermatology. 2006 Jul:142(7):939 [PubMed PMID: 16847224]
Level 3 (low-level) evidenceSegaert S, Van Cutsem E. Clinical signs, pathophysiology and management of skin toxicity during therapy with epidermal growth factor receptor inhibitors. Annals of oncology : official journal of the European Society for Medical Oncology. 2005 Sep:16(9):1425-33 [PubMed PMID: 16012181]
Dika E, Barisani A, Vaccari S, Fanti PA, Ismaili A, Patrizi A. Periungual pyogenic granuloma following imatinib therapy in a patient with chronic myelogenous leukemia. Journal of drugs in dermatology : JDD. 2013 May:12(5):512-3 [PubMed PMID: 23652942]
Level 3 (low-level) evidenceHenning B, Stieger P, Kamarachev J, Dummer R, Goldinger SM. Pyogenic granuloma in patients treated with selective BRAF inhibitors: another manifestation of paradoxical pathway activation. Melanoma research. 2016 Jun:26(3):304-7. doi: 10.1097/CMR.0000000000000248. Epub [PubMed PMID: 27116335]
Sammut SJ, Tomson N, Corrie P. Pyogenic granuloma as a cutaneous adverse effect of vemurafenib. The New England journal of medicine. 2014 Sep 25:371(13):1265-7. doi: 10.1056/NEJMc1407683. Epub [PubMed PMID: 25251629]
Level 3 (low-level) evidencePatruno C, Balato N, Cirillo T, Napolitano M, Ayala F. Periungual and subungual pyogenic granuloma following anti-TNF-α therapy: is it the first case? Dermatologic therapy. 2013 Nov-Dec:26(6):493-5. doi: 10.1111/dth.12022. Epub 2013 Apr 1 [PubMed PMID: 24552415]
Level 3 (low-level) evidenceSibaud V, Dalenc F, Mourey L, Chevreau C. Paronychia and pyogenic granuloma induced by new anticancer mTOR inhibitors. Acta dermato-venereologica. 2011 Sep:91(5):584-5. doi: 10.2340/00015555-1097. Epub [PubMed PMID: 21667012]
Level 3 (low-level) evidenceExner JH, Dahod S, Pochi PE. Pyogenic granuloma-like acne lesions during isotretinoin therapy. Archives of dermatology. 1983 Oct:119(10):808-11 [PubMed PMID: 6225396]
Level 3 (low-level) evidenceBenedetto C, Crasto D, Ettefagh L, Nami N. Development of Periungual Pyogenic Granuloma with Associated Paronychia Following Isotretinoin Therapy: A Case Report and a Review of the Literature. The Journal of clinical and aesthetic dermatology. 2019 Apr:12(4):32-36 [PubMed PMID: 31119008]
Level 3 (low-level) evidenceLenczowski JM, Cassarino DS, Jain A, Turner ML. Disseminated vascular papules in an immunodeficient patient being treated with granulocyte colony-stimulating factor. Journal of the American Academy of Dermatology. 2003 Jul:49(1):105-8 [PubMed PMID: 12833018]
Level 3 (low-level) evidencePalmero ML, Pope E. Eruptive pyogenic granulomas developing after drug hypersensitivity reaction. Journal of the American Academy of Dermatology. 2009 May:60(5):855-7. doi: 10.1016/j.jaad.2008.11.021. Epub 2009 Feb 10 [PubMed PMID: 19211171]
Level 3 (low-level) evidenceCheney-Peters D, Lund TC. Oral Pyogenic Granuloma After Bone Marrow Transplant in the Pediatric/Adolescent Population: Report of 5 Cases. Journal of pediatric hematology/oncology. 2016 Oct:38(7):570-3. doi: 10.1097/MPH.0000000000000593. Epub [PubMed PMID: 27271813]
Level 3 (low-level) evidenceKanda Y, Arai C, Chizuka A, Suguro M, Hamaki T, Yamamoto R, Yamauchi Y, Matsuyama T, Takezako N, Shirai Y, Miwa A, Iwasaki K, Nasu M, Togawa A. Pyogenic granuloma of the tongue early after allogeneic bone marrow transplantation for multiple myeloma. Leukemia & lymphoma. 2000 Apr:37(3-4):445-9 [PubMed PMID: 10752998]
Level 3 (low-level) evidenceBachmeyer C, Devergie A, Mansouri S, Dubertret L, Aractingi S. [Pyogenic granuloma of the tongue in chronic graft versus host disease]. Annales de dermatologie et de venereologie. 1996:123(9):552-4 [PubMed PMID: 9615106]
Level 3 (low-level) evidenceLee L, Miller PA, Maxymiw WG, Messner HA, Rotstein LE. Intraoral pyogenic granuloma after allogeneic bone marrow transplant. Report of three cases. Oral surgery, oral medicine, and oral pathology. 1994 Nov:78(5):607-10 [PubMed PMID: 7838468]
Level 3 (low-level) evidenceBacher J, Assaad D, Adam DN. Pyogenic granuloma of the foot with satellitosis: a role for conservative management. Journal of cutaneous medicine and surgery. 2011 Jan-Feb:15(1):58-60 [PubMed PMID: 21291657]
Level 3 (low-level) evidenceBeers BB, Rustad OJ, Vance JC. Pyogenic granuloma following laser treatment of a port-wine stain. Cutis. 1988 Apr:41(4):266-8 [PubMed PMID: 3284723]
Level 3 (low-level) evidenceAghaei S. Pyogenic granuloma arising in port-wine stain after cryotherapy. Dermatology online journal. 2003 Dec:9(5):16 [PubMed PMID: 14996389]
Level 3 (low-level) evidenceKoo MG, Lee SH, Han SE. Pyogenic Granuloma: A Retrospective Analysis of Cases Treated Over a 10-Year. Archives of craniofacial surgery. 2017 Mar:18(1):16-20. doi: 10.7181/acfs.2017.18.1.16. Epub 2017 Mar 25 [PubMed PMID: 28913297]
Level 2 (mid-level) evidencePagliai KA, Cohen BA. Pyogenic granuloma in children. Pediatric dermatology. 2004 Jan-Feb:21(1):10-3 [PubMed PMID: 14871318]
Seyedmajidi M, Shafaee S, Hashemipour G, Bijani A, Ehsani H. Immunohistochemical Evaluation of Angiogenesis Related Markers in Pyogenic Granuloma of Gingiva. Asian Pacific journal of cancer prevention : APJCP. 2015:16(17):7513-6 [PubMed PMID: 26625754]
Johnson EF, Davis DM, Tollefson MM, Fritchie K, Gibson LE. Vascular Tumors in Infants: Case Report and Review of Clinical, Histopathologic, and Immunohistochemical Characteristics of Infantile Hemangioma, Pyogenic Granuloma, Noninvoluting Congenital Hemangioma, Tufted Angioma, and Kaposiform Hemangioendothelioma. The American Journal of dermatopathology. 2018 Apr:40(4):231-239. doi: 10.1097/DAD.0000000000000983. Epub [PubMed PMID: 29561329]
Level 3 (low-level) evidenceAdams DO. The granulomatous inflammatory response. A review. The American journal of pathology. 1976 Jul:84(1):164-92 [PubMed PMID: 937513]
Lawoyin JO, Arotiba JT, Dosumu OO. Oral pyogenic granuloma: a review of 38 cases from Ibadan, Nigeria. The British journal of oral & maxillofacial surgery. 1997 Jun:35(3):185-9 [PubMed PMID: 9212296]
Level 3 (low-level) evidenceZain RB, Khoo SP, Yeo JF. Oral pyogenic granuloma (excluding pregnancy tumour)--a clinical analysis of 304 cases. Singapore dental journal. 1995 Jul:20(1):8-10 [PubMed PMID: 9582682]
Level 3 (low-level) evidencePutra J, Rymeski B, Merrow AC, Dasgupta R, Gupta A. Four cases of pediatric deep-seated/subcutaneous pyogenic granuloma: Review of literature and differential diagnosis. Journal of cutaneous pathology. 2017 Jun:44(6):516-522. doi: 10.1111/cup.12923. Epub 2017 Mar 23 [PubMed PMID: 28233342]
Level 3 (low-level) evidenceJohnson NA,Haeney J,Yii NW, Intravenous pyogenic granuloma of the finger. The Journal of hand surgery, European volume. 2011 Mar; [PubMed PMID: 21282218]
Level 3 (low-level) evidenceJoethy J, Al Jajeh I, Tay SC. Intravenous pyogenic granuloma of the hand - a case report. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand. 2011:16(1):87-9 [PubMed PMID: 21348038]
Level 3 (low-level) evidenceMeeks MW, Kamal UM, Hammami MB, Taylor JR, Omran ML, Chen Y, Lai JP. Gastrointestinal Pyogenic Granuloma (Lobular Capillary Hemangioma): An Underrecognized Entity Causing Iron Deficiency Anemia. Case reports in gastrointestinal medicine. 2016:2016():4398401. doi: 10.1155/2016/4398401. Epub 2016 Jun 15 [PubMed PMID: 27403353]
Level 3 (low-level) evidenceBlickenstaff RD, Roenigk RK, Peters MS, Goellner JR. Recurrent pyogenic granuloma with satellitosis. Journal of the American Academy of Dermatology. 1989 Dec:21(6):1241-4 [PubMed PMID: 2584462]
Level 3 (low-level) evidenceBenmously-Mlika R, Hammami H, Mokhtar I. Violaceous papules of the back: a quiz. Diagnosis: recurrent pyogenic granuloma or Warner and Wilson-Jones syndrome (1, 2). Acta dermato-venereologica. 2011 Jun:91(4):491-4. doi: 10.2340/00015555-1008. Epub [PubMed PMID: 21103841]
Level 3 (low-level) evidenceDillman AM, Miller RC, Hansen RC. Multiple pyogenic granulomata in childhood. Pediatric dermatology. 1991 Mar:8(1):28-31 [PubMed PMID: 1862021]
Level 3 (low-level) evidenceWilson BB, Greer KE, Cooper PH. Eruptive disseminated lobular capillary hemangioma (pyogenic granuloma). Journal of the American Academy of Dermatology. 1989 Aug:21(2 Pt 2):391-4 [PubMed PMID: 2754072]
Level 3 (low-level) evidenceShah M, Kingston TP, Cotterill JA. Eruptive pyogenic granulomas: a successfully treated patient and review of the literature. The British journal of dermatology. 1995 Nov:133(5):795-6 [PubMed PMID: 8555038]
Level 3 (low-level) evidenceCeyhan AM, Basak PY, Akkaya VB, Yildirim M, Kapucuoglu N. A case of multiple, eruptive pyogenic granuloma developed on a region of the burned skin: can erythromycin be a treatment option? Journal of burn care & research : official publication of the American Burn Association. 2007 Sep-Oct:28(5):754-7 [PubMed PMID: 17667838]
Level 3 (low-level) evidenceZaballos P, Carulla M, Ozdemir F, Zalaudek I, Bañuls J, Llambrich A, Puig S, Argenziano G, Malvehy J. Dermoscopy of pyogenic granuloma: a morphological study. The British journal of dermatology. 2010 Dec:163(6):1229-37. doi: 10.1111/j.1365-2133.2010.10040.x. Epub [PubMed PMID: 20846306]
Lee J, Sinno H, Tahiri Y, Gilardino MS. Treatment options for cutaneous pyogenic granulomas: a review. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2011 Sep:64(9):1216-20. doi: 10.1016/j.bjps.2010.12.021. Epub 2011 Feb 11 [PubMed PMID: 21316320]
Ghodsi SZ, Raziei M, Taheri A, Karami M, Mansoori P, Farnaghi F. Comparison of cryotherapy and curettage for the treatment of pyogenic granuloma: a randomized trial. The British journal of dermatology. 2006 Apr:154(4):671-5 [PubMed PMID: 16536810]
Level 1 (high-level) evidenceMirshams M, Daneshpazhooh M, Mirshekari A, Taheri A, Mansoori P, Hekmat S. Cryotherapy in the treatment of pyogenic granuloma. Journal of the European Academy of Dermatology and Venereology : JEADV. 2006 Aug:20(7):788-90 [PubMed PMID: 16898898]
Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silver nitrate cauterization for pyogenic granuloma of the hand. The Journal of hand surgery. 2003 May:28(3):435-8 [PubMed PMID: 12772100]
Sud AR, Tan ST. Pyogenic granuloma-treatment by shave-excision and/or pulsed-dye laser. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2010 Aug:63(8):1364-8. doi: 10.1016/j.bjps.2009.06.031. Epub 2009 Jul 21 [PubMed PMID: 19625228]
Level 2 (mid-level) evidenceRaulin C, Greve B, Hammes S. The combined continuous-wave/pulsed carbon dioxide laser for treatment of pyogenic granuloma. Archives of dermatology. 2002 Jan:138(1):33-7 [PubMed PMID: 11790165]
Hammes S, Kaiser K, Pohl L, Metelmann HR, Enk A, Raulin C. Pyogenic granuloma: treatment with the 1,064-nm long-pulsed neodymium-doped yttrium aluminum garnet laser in 20 patients. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2012 Jun:38(6):918-23. doi: 10.1111/j.1524-4725.2012.02344.x. Epub 2012 Jan 24 [PubMed PMID: 22272571]
Tritton SM, Smith S, Wong LC, Zagarella S, Fischer G. Pyogenic granuloma in ten children treated with topical imiquimod. Pediatric dermatology. 2009 May-Jun:26(3):269-72. doi: 10.1111/j.1525-1470.2008.00864.x. Epub [PubMed PMID: 19706086]
Maloney DM, Schmidt JD, Duvic M. Alitretinoin gel to treat pyogenic granuloma. Journal of the American Academy of Dermatology. 2002 Dec:47(6):969-70 [PubMed PMID: 12451394]
Level 3 (low-level) evidenceKnöpfel N, Escudero-Góngora MDM, Bauzà A, Martín-Santiago A. Timolol for the treatment of pyogenic granuloma (PG) in children. Journal of the American Academy of Dermatology. 2016 Sep:75(3):e105-e106. doi: 10.1016/j.jaad.2016.03.036. Epub [PubMed PMID: 27543231]
Neri I, Baraldi C, Balestri R, Piraccini BM, Patrizi A. Topical 1% propranolol ointment with occlusion in treatment of pyogenic granulomas: An open-label study in 22 children. Pediatric dermatology. 2018 Jan:35(1):117-120. doi: 10.1111/pde.13372. Epub 2017 Dec 20 [PubMed PMID: 29266656]
Losa Iglesias ME, Becerro de Bengoa Vallejo R. Topical phenol as a conservative treatment for periungual pyogenic granuloma. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2010 May:36(5):675-8. doi: 10.1111/j.1524-4725.2010.01528.x. Epub 2010 Apr 2 [PubMed PMID: 20384744]
Parisi E, Glick PH, Glick M. Recurrent intraoral pyogenic granuloma with satellitosis treated with corticosteroids. Oral diseases. 2006 Jan:12(1):70-2 [PubMed PMID: 16390473]
Level 3 (low-level) evidenceHong SK, Lee HJ, Seo JK, Lee D, Hwang SW, Sung HS. Reactive vascular lesions treated using ethanolamine oleate sclerotherapy. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2010 Jul:36(7):1148-52. doi: 10.1111/j.1524-4725.2010.01599.x. Epub 2010 Jun 1 [PubMed PMID: 20533938]
Level 2 (mid-level) evidenceMoon SE, Hwang EJ, Cho KH. Treatment of pyogenic granuloma by sodium tetradecyl sulfate sclerotherapy. Archives of dermatology. 2005 May:141(5):644-6 [PubMed PMID: 15897398]
Level 3 (low-level) evidenceCarvalho RA, Neto V. Letter: Polidocanol sclerotherapy for the treatment of pyogenic granuloma. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2010 Jun:36 Suppl 2():1068-70. doi: 10.1111/j.1524-4725.2009.01470.x. Epub [PubMed PMID: 20590716]
Level 3 (low-level) evidenceDaya M. Complete resolution of a recurrent giant pyogenic granuloma on the palm of the hand following single dose of intralesional bleomycin injection. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2010 Mar:63(3):e331-3. doi: 10.1016/j.bjps.2009.07.002. Epub 2009 Jul 26 [PubMed PMID: 19632910]
Level 3 (low-level) evidenceLacouture ME, Anadkat MJ, Bensadoun RJ, Bryce J, Chan A, Epstein JB, Eaby-Sandy B, Murphy BA, MASCC Skin Toxicity Study Group. Clinical practice guidelines for the prevention and treatment of EGFR inhibitor-associated dermatologic toxicities. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer. 2011 Aug:19(8):1079-95. doi: 10.1007/s00520-011-1197-6. Epub 2011 Jun 1 [PubMed PMID: 21630130]
Level 1 (high-level) evidenceAl-Thunayan A, Al-Rehaili M, Al-Meshal O, Al-Qattan MM. Bacillary angiomatosis presenting as a pyogenic granuloma of the hand in an otherwise apparently healthy patient. Annals of plastic surgery. 2013 Jun:70(6):652-3. doi: 10.1097/SAP.0b013e31823b6866. Epub [PubMed PMID: 23038144]
Level 3 (low-level) evidenceNthumba PM. Giant pyogenic granuloma of the thigh: a case report. Journal of medical case reports. 2008 Mar 31:2():95. doi: 10.1186/1752-1947-2-95. Epub 2008 Mar 31 [PubMed PMID: 18377654]
Level 3 (low-level) evidenceKapadia SB, Heffner DK. Pitfalls in the histopathologic diagnosis of pyogenic granuloma. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 1992:249(4):195-200 [PubMed PMID: 1642875]
Løes S, Tornes K. Misinterpretation of histopathological results as an important risk factor for unneeded surgery - case report of a "near miss" event in a pregnant woman. Patient safety in surgery. 2008 Jun 5:2():14. doi: 10.1186/1754-9493-2-14. Epub 2008 Jun 5 [PubMed PMID: 18534003]
Level 3 (low-level) evidence