Definition/Introduction
Central and peripheral chemoreceptors govern the primary drive for respiration. Central chemoreceptors, located in the anterior medulla of the brainstem, predominantly respond to a decrease in pH caused by the accumulation of carbon dioxide in the cerebrospinal fluid. The blood-brain barrier protects the central nervous system from external stimuli. Still, the lipid-soluble nature of carbon dioxide allows it to diffuse across this barrier, rapidly influencing respiratory drive.
Peripheral chemoreceptors, in contrast, are more sensitive to changes in oxygen levels. These chemoreceptors consist of the carotid and aortic bodies at the bifurcation of the common carotid artery and the aortic arch. Hypoxia stimulates the carotid bodies, prompting cranial nerve IX to send signals to the nucleus tractus solitarius, thereby triggering ventilation. However, the central chemoreceptors dominate the respiratory drive under normal circumstances as they operate within the body's central control system.[1]
Pursed-lip breathing (PLB) is designed to improve control over oxygenation and ventilation. This breathing technique involves a deliberate inhalation through the nose, followed by a slow, controlled exhalation through puckered or pursed lips, which prolongs the expiratory phase compared to the normal inspiration-to-expiration ratio (see Image. Pursed-Lip Breathing). This process generates backpressure, creating a small amount of positive end-expiratory pressure (PEEP). In PLB, respiratory accessory muscles, such as those in the neck and shoulders, remain relaxed while air is inhaled slowly and deeply through the nose and exhaled gently through rounded lips. The positive pressure generated in the upper airway is effectively transferred to the lower airway, helping to prevent bronchial obstruction and the accumulation of secretions, thereby enhancing respiratory efficiency and reducing dyspnea.[2]
During exhalation, airway collapse in noncartilaginous areas increases airway resistance, leading to carbon dioxide trapping.[3] Elevated carbon dioxide levels stimulate the central chemoreceptors to increase the respiratory rate to restore pH balance to approximately 7.4.[4][5] While this compensatory mechanism clears carbon dioxide, it may exacerbate air trapping and respiratory muscle fatigue.[6] By creating an artificial splint, PEEP prevents airway collapse, supports alveolar patency, increases surface area for gas exchange, and recruits additional alveoli for effective ventilation.[7]
The positive pressure generated by PLB counteracts the inward forces during exhalation, reducing hypercapnia by facilitating the excretion of carbon dioxide as a volatile acid. PLB relieves shortness of breath, reduces the work of breathing, and improves overall gas exchange. Beyond its physiological benefits, PLB empowers individuals by providing a sense of control over their breathing, enhancing relaxation, and alleviating respiratory distress.
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
While PLB offers significant benefits for managing dyspnea and improving gas exchange in obstructive pulmonary diseases, several issues of concern should be noted. PLB relies on voluntary initiation and proper execution for effectiveness, requiring individuals to master the technique, which includes maintaining prolonged exhalation and coordinated breathing patterns. The method can exacerbate air trapping and carbon dioxide retention without accurate implementation, counteracting its intended therapeutic effects. Overuse or extended application of PLB can lead to fatigue of the respiratory muscles and, in normal individuals, potentially result in lower-than-normal carbon dioxide levels, reducing cerebral perfusion pressure and risking syncope.
The therapeutic effects of PLB are typically short-lived, and its use is often limited to 3 to 5 breaths due to the potential for muscle fatigue and metabolic strain. In conditions like interstitial lung disease (ILD), acute exposure to PLB during activities such as the 6-minute walk test has not shown significant improvement in symptoms, walking distance, muscle oxygenation, or oxygen saturation compared to normal breathing. Due to increased metabolic demand, PLB was found to reduce walking distance in patients with normoxemia and negatively affect exercise capacity or dyspnea in ILD.[2] These findings highlight the variability in PLB's effectiveness across different patient populations and underscore the importance of tailoring its use to specific clinical contexts.
Clinical Significance
PLB is a simple yet highly effective technique with extensive clinical applications, particularly for individuals experiencing dyspnea and air trapping. When performed correctly, PLB provides significant relief by allowing patients to regain control over their breathing, reduce the work of breathing, and alleviate respiratory distress. PLB can be easily learned and applied with proper teaching and guidance from trained professionals. In addition to its primary role in relieving carbon dioxide retention and improving oxygenation, PLB is an excellent relaxation tool, helping patients manage anxiety and enhance their overall well-being.
As a versatile and clinically significant technique, PLB is a valuable strategy for managing respiratory conditions. The benefits of this technique extend from offering immediate relief from respiratory symptoms to improving lung function, exercise capacity, and quality of life. Whether employed as a standalone intervention or integrated with other therapies, PLB is an effective, low-cost approach that supports respiratory health across various conditions, including chronic obstructive pulmonary disease (COPD), asthma, and COVID-19. PLB's adaptability and proven efficacy make it an indispensable tool in managing and rehabilitating respiratory diseases.
Role of PLB in Chronic Obstructive Pulmonary Disease
PLB commonly helps patients with COPD. PLB may not be voluntary for these patients, but it is a compensatory mechanism to help splint open the airways.[8][9] Individuals with COPD may have chronic obstruction of their airways from mucus plugging, loss of integrity of the airways, or enlargement of the airways. These changes in the airways can prevent the appropriate driving pressure and airflow to maintain an adequate clearance of carbon dioxide due to increased airway resistance.[10] The increase in airway resistance also affects inhalation, preventing enough oxygen from reaching the alveoli to create a sufficient partial pressure of oxygen needed to drive the diffusion of oxygen across the alveoli-capillary interface adequately.
The defective driving pressure for oxygenation is further exacerbated due to the retention of carbon dioxide, causing less carbon dioxide to diffuse from the blood into the alveoli for excretion. Blunting the proper mechanism to excrete carbon dioxide and adequate oxygenation stimulates the central chemoreceptors to increase respiration until exhaustion. Chronic hypercapnia decreases the sensitivity of the central chemoreceptors, allowing peripheral receptors sensing oxygen levels to become the predominant drive for respiration.[11][12] Increased purse lip breathing in these patients may indicate impending respiratory failure.
Significant use of PLB in individuals with COPD may indicate respiratory distress or impending respiratory failure.[13] Recognizing this sign allows clinicians to escalate care, potentially including noninvasive or invasive ventilatory support. Even on mechanical ventilation, incorporating prolonged expiration and minimizing auto-PEEP is critical to prevent complications such as inefficient ventilation or oxygenation. Auto-PEEP can be misinterpreted as high peak pressures, delaying appropriate intervention.[14]
Benefits Beyond COPD
For older adults with stable COPD, PLB training has improved lung function and quality of life.[15] The technique is a valuable component of disease rehabilitation, promoting better symptom management and enhancing functional capacity. Evidence supports using PLB alongside other breathing exercises, such as diaphragmatic breathing (DB), in conditions like asthma and other chronic respiratory illnesses.[16] Combining PLB and DB forms a simple, low-cost therapeutic strategy that improves lung function and exercise capacity. These techniques are particularly beneficial for daily respiratory care and as part of comprehensive pulmonary rehabilitation programs.[17]
Applications in COVID-19
In COVID-19, PLB and DB can play a vital role in rehabilitation.[18] Early pulmonary rehabilitation, including breathing exercises, airway clearance, and physical activity training, can help those hospitalized to maintain functional status, relieve dyspnea, and improve health-related quality of life after discharge. For patients recovering from COVID-19, incorporating PLB into pulmonary rehabilitation can help address dyspnea and support their overall recovery process.[18]
Nursing, Allied Health, and Interprofessional Team Interventions
Implementing PLB as a therapeutic intervention requires coordinated and ethical collaboration among advanced clinicians, nurses, pharmacists, and other health professionals. Advanced clinicians assess the patient’s respiratory condition, prescribe PLB within a broader care plan, and provide evidence-based guidance to the team. Teaching PLB involves explaining its benefits, potential adverse events, and underlying physiology. A proper demonstration should follow, with the trainee performing or explaining the technique to confirm understanding, ensure proper execution, and allow for correction of any mistakes that may occur during the learning process.[19][20] This process minimizes errors and optimizes therapeutic efficacy.
Nurses play a vital role in teaching and reinforcing PLB. They monitor patients for respiratory distress signs such as increased PLB use, dyspnea, or accessory muscle engagement. Nurses’ ability to promptly recognize distress ensures rapid initiation of response teams and prevents further deterioration.[21][22] For conditions such as COPD, congestive heart failure, or panic attacks, PLB can calm the patient, alleviate dyspnea, and potentially reduce the need for noninvasive mechanical ventilation.[23][24] Further, pharmacists optimize medication regimens to alleviate respiratory symptoms, complementing PLB’s benefits. Rehabilitation Specialists integrate PLB into physical therapy sessions, while mental health professionals address anxiety that may exacerbate dyspnea and hinder technique adherence.
Ethical responsibilities include respecting patient autonomy and addressing barriers like literacy or cultural differences during education. Interprofessional communication and care coordination ensure continuity, with regular team huddles and clear documentation fostering collaboration. By actively teaching and reinforcing PLB, health professionals empower patients to manage their symptoms effectively, improving outcomes, safety, and team performance.
Nursing, Allied Health, and Interprofessional Team Monitoring
Effective patient monitoring using PLB requires coordinated efforts by nursing staff, allied health professionals, and the interprofessional care team to enhance patient outcomes and ensure safety.
Nursing Role
Nurses play a pivotal role in teaching PLB, explaining its benefits and potential adverse events, and ensuring proper technique through demonstration and patient practice. They should also educate trainees or patients about when PLB is useful, such as during episodes of dyspnea related to COPD, congestive heart failure, or panic attacks. With frequent patient contact, nurses are well-positioned to identify respiratory distress signs, including dyspnea, use of accessory muscles, and increased respiratory rate. Recognizing these signs allows nurses to alert the appropriate response team and physicians for timely intervention, potentially preventing deterioration and the need for mechanical ventilation. Nurses should also monitor for respiratory muscle fatigue in COPD patients, a common consequence of compensatory PLB, and promptly report concerns to the care team.
Allied Health Professionals
Respiratory therapists refine PLB techniques, ensuring patients perform them correctly and tailor interventions to individual needs. Physical and occupational therapists integrate PLB into rehabilitation programs, assessing its utility during functional tasks or exertion. Mental health professionals provide support to address anxiety or panic that may interfere with effective technique use.
Interprofessional Team Coordination
Collaboration among all team members is vital for effective monitoring and patient-centered care. Advanced clinicians, nurses, respiratory therapists, and other allied health professionals should communicate regularly to evaluate patient progress and adjust care plans as needed. Pharmacists can optimize medications that improve respiratory function, complementing PLB's efficacy. The team must also thoroughly address patient questions and concerns, ensuring comprehension of the risks and benefits of PLB. By fostering comprehensive education, vigilant monitoring, and seamless communication, the interprofessional team can maximize the effectiveness of PLB, improve patient outcomes, and enhance safety.
Media
(Click Image to Enlarge)
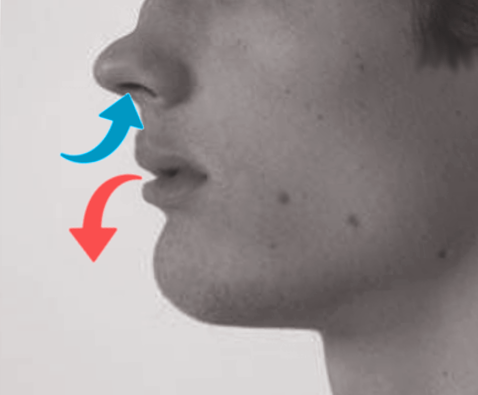
Pursed-Lip Breathing. This breathing technique involves a deliberate inhalation through the nose, followed by a slow, controlled exhalation through puckered or pursed lips, which prolongs the expiratory phase compared to the normal inspiration-to-expiration ratio.
Contributed by O Chaigasame, MD
References
Brinkman JE, Toro F, Sharma S. Physiology, Respiratory Drive. StatPearls. 2025 Jan:(): [PubMed PMID: 29494021]
Hun Kim S, Beom Shin Y, Shin MJ, Hui Hong C, Huh S, Yoo W, Lee K. Effects of walking with a portable oxygen concentrator on muscle oxygenation while performing normal or pursed-lip breathing in patients with interstitial lung disease: a randomized crossover trial. Therapeutic advances in respiratory disease. 2023 Jan-Dec:17():17534666231186732. doi: 10.1177/17534666231186732. Epub [PubMed PMID: 37462163]
Level 1 (high-level) evidenceSeadler BD, Toro F, Sharma S. Physiology, Alveolar Tension. StatPearls. 2025 Jan:(): [PubMed PMID: 30969647]
Hopkins E, Sanvictores T, Sharma S. Physiology, Acid Base Balance. StatPearls. 2024 Jan:(): [PubMed PMID: 29939584]
Keir DA, Duffin J, Millar PJ, Floras JS. Simultaneous assessment of central and peripheral chemoreflex regulation of muscle sympathetic nerve activity and ventilation in healthy young men. The Journal of physiology. 2019 Jul:597(13):3281-3296. doi: 10.1113/JP277691. Epub 2019 May 28 [PubMed PMID: 31087324]
Lomax M, Kapus J, Webb S, Ušaj A. The effect of inspiratory muscle fatigue on acid-base status and performance during race-paced middle-distance swimming. Journal of sports sciences. 2019 Jul:37(13):1499-1505. doi: 10.1080/02640414.2019.1574250. Epub 2019 Feb 6 [PubMed PMID: 30724711]
Gonçalves-Ferri WA, Jauregui A, Martins-Celini FP, Sansano I, Fabro AT, Sacramento EMF, Aragon DC, Ochoa JM. Analysis of different levels of positive end-expiratory pressure during lung retrieval for transplantation: an experimental study. Brazilian journal of medical and biological research = Revista brasileira de pesquisas medicas e biologicas. 2019:52(7):e8585. doi: 10.1590/1414-431X20198585. Epub 2019 Jul 15 [PubMed PMID: 31314854]
Vatwani A. Pursed Lip Breathing Exercise to Reduce Shortness of Breath. Archives of physical medicine and rehabilitation. 2019 Jan:100(1):189-190. doi: 10.1016/j.apmr.2018.05.005. Epub 2018 Jul 19 [PubMed PMID: 30033163]
Sakhaei S, Sadagheyani HE, Zinalpoor S, Markani AK, Motaarefi H. The Impact of Pursed-lips Breathing Maneuver on Cardiac, Respiratory, and Oxygenation Parameters in COPD Patients. Open access Macedonian journal of medical sciences. 2018 Oct 25:6(10):1851-1856. doi: 10.3889/oamjms.2018.407. Epub 2018 Oct 20 [PubMed PMID: 30455761]
Haghighi B, Choi S, Choi J, Hoffman EA, Comellas AP, Newell JD Jr, Lee CH, Barr RG, Bleecker E, Cooper CB, Couper D, Han ML, Hansel NN, Kanner RE, Kazerooni EA, Kleerup EAC, Martinez FJ, O'Neal W, Paine R 3rd, Rennard SI, Smith BM, Woodruff PG, Lin CL. Imaging-based clusters in former smokers of the COPD cohort associate with clinical characteristics: the SubPopulations and intermediate outcome measures in COPD study (SPIROMICS). Respiratory research. 2019 Jul 15:20(1):153. doi: 10.1186/s12931-019-1121-z. Epub 2019 Jul 15 [PubMed PMID: 31307479]
Docio I, Olea E, Prieto-LLoret J, Gallego-Martin T, Obeso A, Gomez-Niño A, Rocher A. Guinea Pig as a Model to Study the Carotid Body Mediated Chronic Intermittent Hypoxia Effects. Frontiers in physiology. 2018:9():694. doi: 10.3389/fphys.2018.00694. Epub 2018 Jun 5 [PubMed PMID: 29922183]
Benner A, Lewallen NF, Sharma S. Physiology, Carbon Dioxide Response Curve. StatPearls. 2025 Jan:(): [PubMed PMID: 30844173]
Alzaabi O, Guerot E, Planquette B, Diehl JL, Soumagne T. Predicting outcomes in patients with exacerbation of COPD requiring mechanical ventilation. Annals of intensive care. 2024 Oct 20:14(1):159. doi: 10.1186/s13613-024-01394-z. Epub 2024 Oct 20 [PubMed PMID: 39427276]
Goodfellow LT, Miller AG, Varekojis SM, LaVita CJ, Glogowski JT, Hess DR. AARC Clinical Practice Guideline: Patient-Ventilator Assessment. Respiratory care. 2024 Jul 24:69(8):1042-1054. doi: 10.4187/respcare.12007. Epub 2024 Jul 24 [PubMed PMID: 39048148]
Level 1 (high-level) evidenceKuanli H, Qinlong Z. Effects of Pursed Lip Breathing Training on Rehabilitation for Older Adults With Stable COPD. Alternative therapies in health and medicine. 2024 Jun 14:():. pii: AT9704. Epub 2024 Jun 14 [PubMed PMID: 38870497]
Level 2 (mid-level) evidenceBurge AT, Gadowski AM, Jones A, Romero L, Smallwood NE, Ekström M, Reinke LF, Saggu R, Wijsenbeek M, Holland AE. Breathing techniques to reduce symptoms in people with serious respiratory illness: a systematic review. European respiratory review : an official journal of the European Respiratory Society. 2024 Oct:33(174):. doi: 10.1183/16000617.0012-2024. Epub 2024 Oct 30 [PubMed PMID: 39477355]
Level 1 (high-level) evidenceYang Y, Wei L, Wang S, Ke L, Zhao H, Mao J, Li J, Mao Z. The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiotherapy theory and practice. 2022 Jul:38(7):847-857. doi: 10.1080/09593985.2020.1805834. Epub 2020 Aug 18 [PubMed PMID: 32808571]
Level 1 (high-level) evidenceLan CC, Hsieh PC, Yang MC, Su WL, Wu CW, Huang HY, Wu YK. Early pulmonary rehabilitation of COVID-19 patients in an isolation ward and intensive care unit. Tzu chi medical journal. 2023 Apr-Jun:35(2):137-142. doi: 10.4103/tcmj.tcmj_136_22. Epub 2022 Nov 2 [PubMed PMID: 37261306]
Feinberg I, Ogrodnick MM, Hendrick RC, Bates K, Johnson K, Wang B. Perception Versus Reality: The Use of Teach Back by Medical Residents. Health literacy research and practice. 2019 Apr:3(2):e117-e126. doi: 10.3928/24748307-20190501-01. Epub 2019 Jul 1 [PubMed PMID: 31294313]
Yen PH, Leasure AR. Use and Effectiveness of the Teach-Back Method in Patient Education and Health Outcomes. Federal practitioner : for the health care professionals of the VA, DoD, and PHS. 2019 Jun:36(6):284-289 [PubMed PMID: 31258322]
MIT Critical Data, Charlton PH, Pimentel M, Lokhandwala S. Data Fusion Techniques for Early Warning of Clinical Deterioration. Secondary Analysis of Electronic Health Records. 2016:(): [PubMed PMID: 31314272]
Cui L, Liu H, Sun L. Multidisciplinary respiratory rehabilitation in combination with non-invasive positive pressure ventilation in the treatment of elderly patients with severe chronic obstructive pulmonary disease. Pakistan journal of medical sciences. 2019 Mar-Apr:35(2):500-505. doi: 10.12669/pjms.35.2.459. Epub [PubMed PMID: 31086540]
Sha J, Worsnop CJ, Leaver BA, Vagias C, Kinsella P, Rahman MA, McDonald CF. Hospitalised exacerbations of chronic obstructive pulmonary disease: adherence to guideline recommendations in an Australian teaching hospital. Internal medicine journal. 2020 Apr:50(4):453-459. doi: 10.1111/imj.14378. Epub [PubMed PMID: 31157943]
Avdeev SN, Truschenko NV, Gaynitdinova VV, Soe AK, Nuralieva GS. Treatment of exacerbations of chronic obstructive pulmonary disease. Terapevticheskii arkhiv. 2018 Dec 30:90(12):68-75. doi: 10.26442/00403660.2018.12.000011. Epub [PubMed PMID: 30701836]