Introduction
Prurigo nodularis (PN) is a chronic disorder of the skin that is classically seen as multiple, firm, flesh-to-pink-colored nodules commonly located on the extensor surfaces of the extremities. The lesions are very pruritic, and the condition may occur in any age group. It is commonly associated with another disorder of cutaneous hypersensitivity, such as atopic dermatitis or chronic pruritus of diverse origins. The diagnosis is mainly clinical, although certain conditions may simulate it clinically, warranting differentiation. The condition is associated with significant physical and psychological morbidity and is often refractory to treatments. A wide range of general measures, pharmacological approaches, and psychological therapies may be needed in a patient with advanced PN.[1][2][3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The exact etiology of PN remains poorly understood. Although the role of the unimpeded itch-scratch cycle is uncontested, the exact sequence of events leading to the final clinical picture remains debated. PN is accompanied by long-standing pruritus and is thought to develop as a reaction to repeated scratching in patients with chronic prurigo of various etiologies, including dermatological, systemic, infectious, and neuropsychiatric.[5][6] Anecdotal data suggest a causative role or association of infectious agents such as hepatitis C, Helicobacter pylori, Strongyloides stercoralis, mycobacteria, and HIV.[7][8]
An increase in the number of sensory structures of the epidermis (Merkel cells) and dermis (papillary dermal nerves) is encountered in PN lesions.[9] This neural alteration is typical of PN and not seen in lichen simplex chronicus or neurodermatitis. The density of mast cells and neutrophils is also increased in PN, although there seems to be no increase in their degranulation products. In contrast, although the number of eosinophils remains maintained, their products, such as the major basic protein and eosinophil-derived neurotoxin, show higher than normal levels.
The pruritus in PN seems to be a result of cutaneous neurogenic inflammation mediated by various neuropeptides, especially substance P, calcitonin gene–related peptide (CGRP),[10] and vanilloid receptor subtype 1 (VR-1). The latter binds to capsaicin, rendering it a potential therapeutic topical agent. Individuals with PN also show elevated levels of interleukin 31 (IL-31), a T-cell–derived highly prurigogenic cytokine.[11]
Epidemiology
The exact incidence of PN is unknown. A majority of patients with PN present between the ages of 51 and 65 years, although several cases in other age groups have also been described.[5][12] The disease afflicts both genders; however, it seems to be more frequent and more intense in females.[13] Multiple studies have shown that individuals with an atopic predisposition have an earlier age of onset.[5][14][15] Ethnicity and genetic predisposition seem to play a role since African-Americans are 3 to 4 times more likely to have PN than white patients.[12] Other conditions that have been reported to induce PN include internal malignancy, renal failure, and psychiatric conditions. In HIV-positive patients, PN has been reported to be predictive of advanced immunosuppression.[16]
Pathophysiology
The pathophysiology of PN has been controversial. Chronic or recurrent mechanical trauma or vigorous frictional assault to the skin induces epidermal hyperplasia with resultant thickening of the skin. Repetitive mechanical rubbing and scratching of the skin result in the formation of plaques and nodules (often with lichenification) and also give rise to dyschromic changes (typically hyperpigmentation). The itching of PN is typically episodic, severe, and uncontrollable; it tends to occur at discrete points that eventually transform into hyperpigmented nodular plaques with excoriations, crusting, and sometimes secondary bacterial infection.
Immunohistochemical studies have shown increased dermal nerve fibers in the papillary dermis of patients with PN. It has been postulated that the thin, unmyelinated epidermal nerves are the transmitters of severe prurigo. Nerve growth factor (NGF) and its receptor, tyrosine receptor kinase A (TrkA), are overexpressed in PN lesions; both may also be associated with the increased release and accumulation of neuropeptides, such as substance P and calcitonin gene–related peptides.[17] Interestingly, skin biopsies taken from lesions of PN tend to show significantly decreased intraepidermal—not dermal—nerve fiber density. Although this finding has raised doubt about some subclinical small nerve fiber neuropathy contributing to the pathophysiology of PN, recent studies have suggested that the reduction may be secondary to chronic scratching. This suggestion was confirmed by observing restoration of the intraepidermal nerve fiber density on complete healing of lesions.[18]
The role of helper T cytokines (T helper 1 [Th1] and T helper 2 [Th2]) has also been studied in the pathogenesis of PN using the signal transducers and activators of transcription (STAT) 1, 3, and 6. In all but 3 cases, the entire epidermis was stained with anti–phosphorylated STAT (pSTAT) 6, a marker for the Th2 cytokines IL-4, IL-5, and IL-13. These findings suggest that Th2 cytokines play a principal role in the pathogenesis of PN.[19]
Histopathology
PN lesions under histopathology can show thick orthohyperkeratosis, irregular epidermal hyperplasia, and pseudoepitheliomatous hyperplasia. Focal parakeratosis with irregular acanthosis, diminished nerve fiber density, and a nonspecific dermal infiltrate containing lymphocytes, macrophages, eosinophils, and neutrophils may also be seen.
Histology can be important in differentiating PN from lichen simplex (LS) and hypertrophic lichen planus (HLP). LS lesions are less likely to have pseudoepitheliomatous hyperplasia or nerve fiber thickening; however, these findings do not rule out the histological diagnosis of PN. To reliably distinguish between PN and LS, it is necessary to correlate clinical and histological findings.[20]
HLP and PN both demonstrate epidermal hyperplasia, hypergranulosis, and compact hyperkeratosis. Vertically arranged collagen fibers and increased fibroblasts and capillaries in the dermis are found in both conditions. However, basal cell degeneration is limited to the tips of rete ridges, and no band-like inflammation will be seen in HLP versus PN[21]
History and Physical
Patients with PN present with characteristic firm, dome-shaped, pruritic nodules that vary from a few millimeters to a few centimeters. The nodules can be flesh-colored, erythematous, pink, and brown/black. The lesions can begin as normal skin or areas of xerosis; patients will scratch them due to pruritus until the dome-shaped nodule forms. Typically, the lesions are found symmetrically on the extensor surfaces of the arm and legs.[22] Lesions can also be found in the occipital region of the scalp. The upper back, abdomen, and sacrum also can be involved.
Areas of the body that are difficult to reach, such as the upper mid-back, are usually spared from PN lesions, a finding called the “butterfly sign.” The palms, soles, face, and flexural areas are also usually spared. PN lesions cause severe pruritus, which can be very distressing for patients. It can be sporadic or continuous and can increase with sweating, clothing irritation, or heat. In addition to pruritic sensations, patients can experience burning, stinging, and alterations in lesional temperature.[5] It has been reported that in some cases, atopic dermatitis and xerosis are found in conjunction with PN and may be the initiating factor.
Lesions can often appear excoriated due to the pruritus involved with PN. Excoriated lesions are at increased risk of secondary infection and can appear crusted, erythematous, or painful if infected. PN can also be localized in cases of underlying local dermatosis such as venous stasis, postherpetic neuralgia, or brachioradial pruritus.[23]
Evaluation
PN is a clinical diagnosis. Patients with PN will likely have a history of chronic severe pruritus with excoriations and flesh-colored, pink nodular lesions on extensor surfaces. Dermoscopy can be a helpful tool when diagnosing PN versus HLP. In one study, dermoscopy of HLP demonstrated pearly white areas and peripheral striations, gray-blue globules, comedo-like openings, red dots and globules, brownish-black globules, and yellowish structures. In PN, red dots and globules and pearly white areas with peripheral striations were observed under dermoscopy.[24] A skin biopsy may be warranted for lesions that are bleeding, have formed ulcers, or are resistant to first-line therapies.
In patients with PN and severe pruritus, underlying causes of severe pruritus should be evaluated, including renal disease, liver disease, thyroid disease, HIV infection, malignancy, or parasitic infection.[25] Evaluation of these causes includes a complete blood cell count, complete metabolic panel, thyroid studies including thyroid-stimulating hormone and free thyroxine (T4), urinalysis, stool exam, HIV antibodies, and chest X-ray. Serum immunoglobulin E levels can also be elevated in patients with PN and atopic dermatitis.[26]
Treatment / Management
Management of PN requires a multifaceted approach. Patients need to be educated on practices to reduce scratching of lesions. Further, any psychological disorder associated with scratching and picking at skin should be diagnosed and treated. Any underlying causes of pruritus should also be diagnosed. Treatments for PN, both topical and systemic, are targeted at disrupting the itch-scratch cycle.
General Care
Patients with PN should be advised to:
- Keep their nails short, wear protective clothing (ie, long sleeves and gloves), and keep the nodules covered with bandages.
- Bathe with gentle cleansers and apply emollients throughout day to keep skin moisturized.
- Use calamine lotions and lotions containing menthol and camphor to provide itch relief.
- Stay in a cool, comfortable environment.
- Reduce stress.
Specific Care
Topical and Intralesional Therapy
- Although none have been examined in randomized trials, topical treatments for PN include class I topical corticosteroids, intralesional corticosteroids, topical calcineurin inhibitors, topical capsaicin, and topical vitamin D analogs.
- The suggested first-line therapy consists of topical corticosteroids, such as clobetasol dipropionate 0.05% ointment, applied under occlusion with plastic wrap once at nighttime for at least 2 to 4 weeks.
- Triamcinolone acetonide, in concentrations of 10 mg/mL to 20 mg/mL injected intralesionally, has been shown to flatten lesions and provide relief from pruritus.[27][28][29][30][31]
- Pimecrolimus 1% is as effective as hydrocortisone and can be implemented in a long-term regimen.[32]
- Calcipotriol ointment shows greater efficacy than betamethasone valerate 0.1%.[33]
- Low concentrations of menthol (<5%) alleviate pruritus by heightening the threshold for pruritic stimuli.[34] (A1)
Antihistamines and Leukotriene Inhibitors
- High-dose nonsedating antihistamines can be used during the day, followed by first-generation sedating antihistamines at bedtime; a combination of fexofenadine and montelukast gives good results.[35]
- Common adverse reactions to antihistamines are drowsiness, dizziness, and weakness.
Phototherapy and Excimer Laser
- Phototherapy with psoralen–ultraviolet-A (PUVA), including bath and topical PUVA, long-wavelength UVA, narrowband UVB, and monochromatic excimer light of 308 nm, have been used and shown improvement of PN nodules.
- Narrow band UVB phototherapy significantly improves PN at an average dose of 23.88-26.00 j/cm2.[36]
- An excimer laser is more beneficial than topical clobetasol.[37] (A1)
Oral Immunosuppressants
- As with topical therapies, no randomized trials have been reported involving these systemic therapies, and the benefits versus risks of the drugs must be considered before beginning treatment.[13]
- Oral immunosuppressive therapy should be considered for patients with severe, recalcitrant PN.
- A single-institution retrospective study demonstrated clinical improvement and decreased pruritus with cyclosporine at a mean dose of 3.1 mg/kg.[38]
- Methotrexate dosed at 5 to 20 mg/kg weekly demonstrated complete or partial remission of 2.4 months. These patients showed a mean duration of response of 19 months.[39]
- Treatment with azathioprine and cyclophosphamide has also been reported to be successful.[40][41]
- Oral tacrolimus therapy dramatically reduced pruritus in a patient previously treated with cyclosporine.[42]
- Combination therapy of 3 cycles of intravenous immunoglobulin followed by methotrexate and topical steroids was effective in treating PN associated with atopic dermatitis.[43] (B2)
Novel Treatments
- Thalidomide is an immunomodulatory agent which also acts as a central and peripheral depressant and inhibits tumor necrosis factor-alpha.[43] The therapeutic effect against PN is thought to derive from its neurotoxic effects.[44]
- Lenalidomide, a more potent molecular form of thalidomide, is effective in PN and has a lower frequency of peripheral neuropathy.[45]
- Both selective serotonin reuptake inhibitors and tricyclic antidepressants can also be considered for chronic pruritus. It is also important for patients alsbe seen in conjunction with mental health professionals.
- Naloxone and naltrexone exert antipruritic effects by inhibiting Mu-opioid receptors on nociceptive neurons and interneurons, resulting in suppression of itch.[46]
- Neurokinin-1 receptor (NK1r) antagonists, aprepitant and serlopitant, could prevent substance P–mediated signaling in the pathogenesis of PN.[47] Significant relief of itch was achieved in PN patients on aprepitant monotherapy.
- IL 31 receptor antibody, nemolizumab, significantly improved pruritus scores in patients with moderate to severe atopic dermatitis; however, its role in PN remains unclear. (B3)
Differential Diagnosis
Due to similar morphologies, PN is often confused with and must be clinically separated from:
- LS chronicus
- HLP
- Pemphigoid nodularis
- Nodular scabies
- Keloids
- Dermatofibroma
- Foreign body reactions
Treatment Planning
Treatment of PN should be tailored to a patient's age, comorbidities, severity of prurigo, quality of life, and expected side effects.
First-line Therapy
- Class I topical steroids: Clobetasol propionate 0.05% and halobetasol propionate 0.05%); long-term applications can lead to adverse effects like skin atrophy, folliculitis, miliaria, delayed wound healing, and tachyphylaxis.
- Intralesional injections: Using triamcinolone acetonide (40 mg/ml); may be accompanied by cryotherapy[48][49]
- Topical menthol solution: In a concentration of less than 5%.
- Systemic antihistamines: Fexofenadine 180 mg, levocetirizine 5 mg, or desloratadine 5 mg during the day, and sedating antihistamines like hydroxyzine 25 mg at night time; first-generation antihistamines cause side effects like sedation, hyperexcitability, impaired cognitive function, dry mouth, constipation, dysuria, tachycardia, and arrhythmias.
Second-line Therapy
- Phototherapy: PUVA, long-wavelength UVA, Narrowband UVB, monochromatic excimer light of 308nm
- Systemic immunosuppressives: Cyclosporine 3 mg/kg daily; adverse effects include nephrotoxicity, hypertension, hyperlipidemia, hyperkalemia, and hyperuricemia. Methotrexate 5-20 mg/week; common adverse effects are nausea, gastrointestinal symptoms, and transaminitis.
- Thalidomide: Dosed at 300-400 mg daily yields a good response within 3 months, followed by tapering the dose to 50 mg daily; however, complete cessation of the drug leads to recurrences. Adverse effects are teratogenicity and peripheral neuropathy.
- Lenalidomide: Dosed at 5-10 mg daily; less neurotoxic than thalidomide.
- Opioid receptor antagonists: Naltrexone 50 mg daily; adverse effects are restricted to the first 2 weeks of treatment and include nausea, fatigue, dizziness, heartburn, and diarrhea.
Prognosis
PN is a benign condition with a generally good prognosis. It is a chronic condition, typically preceded by an underlying cause of pruritus. However, PN is a distinct entity from the underlying causes and can persist despite the resolution of the predisposing condition.
Complications
PN lesions can become secondarily infected due to scratching of the lesions, leading to ulceration, abscess formation, and cellulitis. It is important to monitor for clinical signs of infection, such as erythema, pain, warmth, and fever. If secondary infection is suspected, it is important to begin appropriate topical or systemic antibiotic therapy to cover for skin flora.
Deterrence and Patient Education
The deterrents in PN treatment are the severe intensity of the itch, which can lead to psychological distress, the chronic nature of the condition, the long duration of the therapy, and the potential side effects of the medication.
Discussion with the patient should include the advantages and disadvantages of the therapy, side effects, and possible use of off-label medications. Patient education can thus promote treatment adherence. The potential length of therapy should also be discussed as PN is difficult to treat, and the patient may become frustrated with the lack of improvement.
Pearls and Other Issues
PN is a chronic skin disease that can significantly impact a patient's quality of life. Breaking the itch-scratch cycle requires a multifaceted approach, and patients should be encouraged to continue with therapy to reduce scratching and picking at the lesions. It may be necessary to involve behavioral therapy. It is important to explain to patients that PN lesions may be chronic and difficult to completely improve.
Enhancing Healthcare Team Outcomes
Management of PN requires an interprofessional team that includes the primary caregiver, nurse practitioner, dermatologist, and mental health nurse. Patients need to be educated on practices to reduce scratching of lesions, assurance and diagnosing of underlying causes of pruritus, and diagnosis and treatment of any psychological disorder associated with scratching and picking at skin.
Topical and systemic treatments are targeted at disrupting the itch-scratch cycle. Patients are encouraged to keep their nails short, wear protective clothing such as long sleeves and gloves, and keep the nodules covered with bandages. Using gentle cleansers to bathe and applying emollients multiple times a day to keep skin moisturized should be encouraged.
Calamine lotions and lotions containing menthol and camphor-like sarna can relieve pruritus. First-generation sedating antihistamines such as hydroxyzine administered at bedtime may be useful in controlling nocturnal pruritus. Both selective serotonin reuptake inhibitors and tricyclic antidepressants can also be considered for chronic pruritus.[12]
Finally, the pharmacist should educate the patient on potential adverse reactions to the medications and report to the clinical team if there are complications.
Media
(Click Image to Enlarge)

(Click Image to Enlarge)
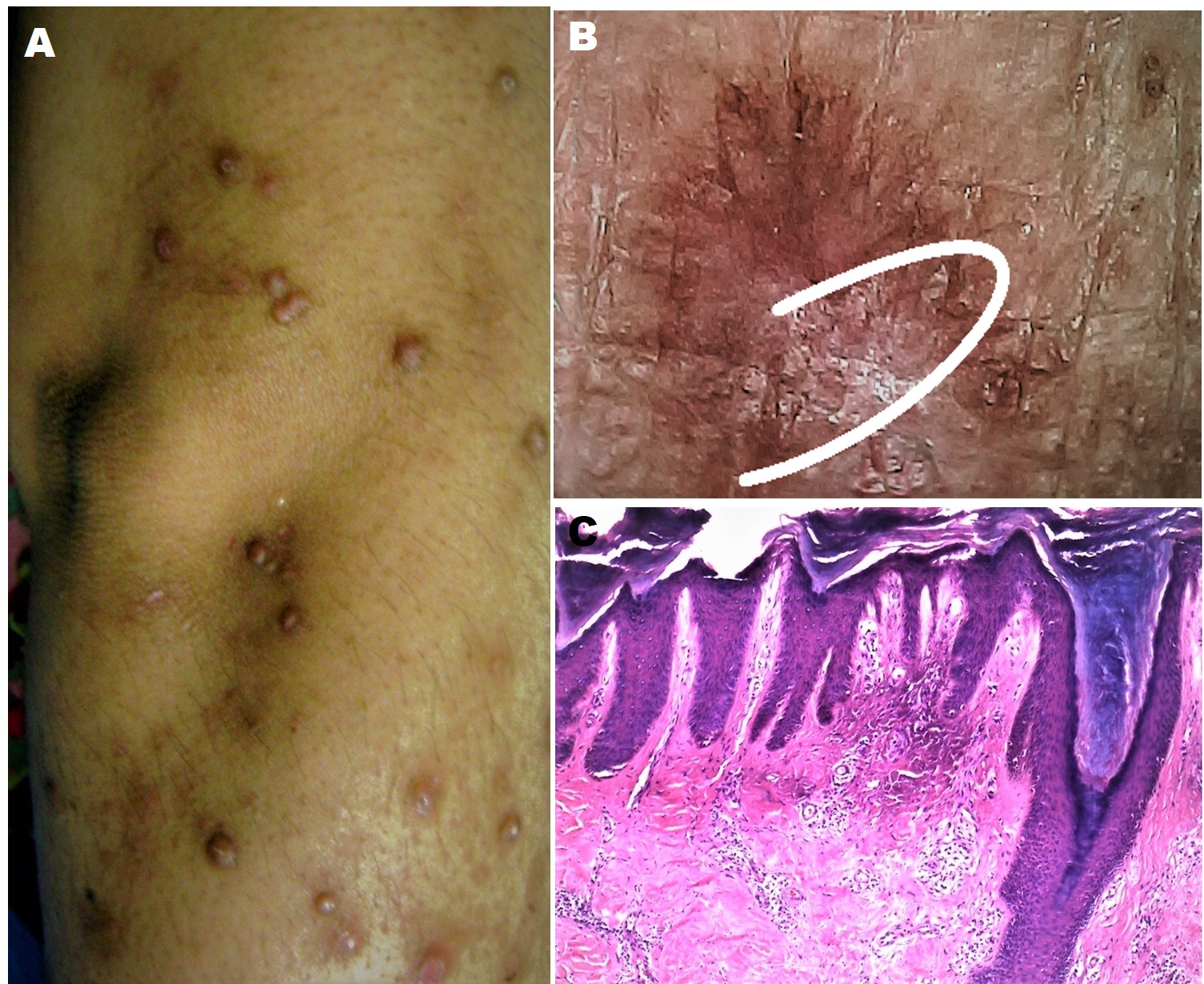
Figure 1 PRURIGO NODULARIS involving the limbs of a 65-year old lady: A, Clinical Image showing the typical hyperpigmented papules and nodules over the right upper extremity with excoriations; B, Polarized dermoscopic image from a papule showing an irregularly-shaped large reddish-brown clod with localized white structureless area (white arc), with interspersed red and brown colored dots and pigmented granules [Escope, USB Videodermoscope, 30X; Timpac Healthcare Pvt. Ltd., New Delhi]; and C, On histopathology from a nodule the epidermis is showing marked compact orthokeratosis, thickened granular layer, and irregular epidermal hyperplasia. The papillary dermis is thickened with papillomatosis and thickened bundles of collagen in vertical array, with increased number of thick walled capillaries and sparse superficial perivascular lymphocytic infiltrate [Hematoxylin & eosin, 400X] Contributed by Dr Sidharth Sonthalia, MD, DNB, MNAMS
(Click Image to Enlarge)

Prurigo Nodularis Contributed by Dr. Shyam Verma, MBBS, DVD, FRCP, FAAD, Vadodara, India
References
Harbaoui S, Litaiem N. Acquired Perforating Dermatosis. StatPearls. 2024 Jan:(): [PubMed PMID: 30969537]
Larson VA, Tang O, Stander S, Miller LS, Kang S, Kwatra SG. Association between prurigo nodularis and malignancy in middle-aged adults. Journal of the American Academy of Dermatology. 2019 Nov:81(5):1198-1201. doi: 10.1016/j.jaad.2019.03.083. Epub 2019 Apr 5 [PubMed PMID: 30954580]
Ständer S, Kwon P, Hirman J, Perlman AJ, Weisshaar E, Metz M, Luger TA, TCP-102 Study Group. Serlopitant reduced pruritus in patients with prurigo nodularis in a phase 2, randomized, placebo-controlled trial. Journal of the American Academy of Dermatology. 2019 May:80(5):1395-1402. doi: 10.1016/j.jaad.2019.01.052. Epub 2019 Mar 17 [PubMed PMID: 30894279]
Level 1 (high-level) evidenceKowalski EH, Kneiber D, Valdebran M, Patel U, Amber KT. Treatment-resistant prurigo nodularis: challenges and solutions. Clinical, cosmetic and investigational dermatology. 2019:12():163-172. doi: 10.2147/CCID.S188070. Epub 2019 Feb 28 [PubMed PMID: 30881076]
Iking A, Grundmann S, Chatzigeorgakidis E, Phan NQ, Klein D, Ständer S. Prurigo as a symptom of atopic and non-atopic diseases: aetiological survey in a consecutive cohort of 108 patients. Journal of the European Academy of Dermatology and Venereology : JEADV. 2013 May:27(5):550-7. doi: 10.1111/j.1468-3083.2012.04481.x. Epub 2012 Feb 25 [PubMed PMID: 22364653]
Level 3 (low-level) evidenceRowland Payne CM, Wilkinson JD, McKee PH, Jurecka W, Black MM. Nodular prurigo--a clinicopathological study of 46 patients. The British journal of dermatology. 1985 Oct:113(4):431-9 [PubMed PMID: 4063179]
Mattila JO, Vornanen M, Vaara J, Katila ML. Mycobacteria in prurigo nodularis: the cause or a consequence? Journal of the American Academy of Dermatology. 1996 Feb:34(2 Pt 1):224-8 [PubMed PMID: 8642086]
Level 3 (low-level) evidenceJacob CI, Patten SF. Strongyloides stercoralis infection presenting as generalized prurigo nodularis and lichen simplex chronicus. Journal of the American Academy of Dermatology. 1999 Aug:41(2 Pt 2):357-61 [PubMed PMID: 10426933]
Level 3 (low-level) evidenceNahass GT, Penneys NS. Merkel cells and prurigo nodularis. Journal of the American Academy of Dermatology. 1994 Jul:31(1):86-8 [PubMed PMID: 7517411]
Vaalasti A, Suomalainen H, Rechardt L. Calcitonin gene-related peptide immunoreactivity in prurigo nodularis: a comparative study with neurodermatitis circumscripta. The British journal of dermatology. 1989 May:120(5):619-23 [PubMed PMID: 2474315]
Level 2 (mid-level) evidenceSonkoly E, Muller A, Lauerma AI, Pivarcsi A, Soto H, Kemeny L, Alenius H, Dieu-Nosjean MC, Meller S, Rieker J, Steinhoff M, Hoffmann TK, Ruzicka T, Zlotnik A, Homey B. IL-31: a new link between T cells and pruritus in atopic skin inflammation. The Journal of allergy and clinical immunology. 2006 Feb:117(2):411-7 [PubMed PMID: 16461142]
Boozalis E, Tang O, Patel S, Semenov YR, Pereira MP, Stander S, Kang S, Kwatra SG. Ethnic differences and comorbidities of 909 prurigo nodularis patients. Journal of the American Academy of Dermatology. 2018 Oct:79(4):714-719.e3. doi: 10.1016/j.jaad.2018.04.047. Epub 2018 May 4 [PubMed PMID: 29733939]
Fostini AC, Girolomoni G, Tessari G. Prurigo nodularis: an update on etiopathogenesis and therapy. The Journal of dermatological treatment. 2013 Dec:24(6):458-62. doi: 10.3109/09546634.2013.814759. Epub 2013 Jul 3 [PubMed PMID: 23767411]
Tanaka M, Aiba S, Matsumura N, Aoyama H, Tagami H. Prurigo nodularis consists of two distinct forms: early-onset atopic and late-onset non-atopic. Dermatology (Basel, Switzerland). 1995:190(4):269-76 [PubMed PMID: 7655104]
Tan WS, Tey HL. Extensive prurigo nodularis: characterization and etiology. Dermatology (Basel, Switzerland). 2014:228(3):276-80. doi: 10.1159/000358250. Epub 2014 Mar 22 [PubMed PMID: 24662043]
Level 2 (mid-level) evidenceMagand F, Nacher M, Cazorla C, Cambazard F, Marie DS, Couppié P. Predictive values of prurigo nodularis and herpes zoster for HIV infection and immunosuppression requiring HAART in French Guiana. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2011 Jul:105(7):401-4. doi: 10.1016/j.trstmh.2011.04.001. Epub 2011 May 28 [PubMed PMID: 21621233]
Level 2 (mid-level) evidenceLee MR, Shumack S. Prurigo nodularis: a review. The Australasian journal of dermatology. 2005 Nov:46(4):211-18; quiz 219-20 [PubMed PMID: 16197418]
Pereira MP, Mühl S, Pogatzki-Zahn EM, Agelopoulos K, Ständer S. Intraepidermal Nerve Fiber Density: Diagnostic and Therapeutic Relevance in the Management of Chronic Pruritus: a Review. Dermatology and therapy. 2016 Dec:6(4):509-517 [PubMed PMID: 27730494]
Fukushi S, Yamasaki K, Aiba S. Nuclear localization of activated STAT6 and STAT3 in epidermis of prurigo nodularis. The British journal of dermatology. 2011 Nov:165(5):990-6. doi: 10.1111/j.1365-2133.2011.10498.x. Epub 2011 Sep 29 [PubMed PMID: 21711341]
Weigelt N, Metze D, Ständer S. Prurigo nodularis: systematic analysis of 58 histological criteria in 136 patients. Journal of cutaneous pathology. 2010 May:37(5):578-86. doi: 10.1111/j.1600-0560.2009.01484.x. Epub 2009 Nov 30 [PubMed PMID: 20002240]
Level 2 (mid-level) evidenceAnkad BS, Beergouder SL. Hypertrophic lichen planus versus prurigo nodularis: a dermoscopic perspective. Dermatology practical & conceptual. 2016 Apr:6(2):9-15. doi: 10.5826/dpc.0602a03. Epub 2016 Apr 30 [PubMed PMID: 27222766]
Level 3 (low-level) evidenceVaidya DC, Schwartz RA. Prurigo nodularis: a benign dermatosis derived from a persistent pruritus. Acta dermatovenerologica Croatica : ADC. 2008:16(1):38-44 [PubMed PMID: 18358109]
Pereira MP, Lüling H, Dieckhöfer A, Steinke S, Zeidler C, Ständer S. Brachioradial Pruritus and Notalgia Paraesthetica: A Comparative Observational Study of Clinical Presentation and Morphological Pathologies. Acta dermato-venereologica. 2018 Jan 12:98(1):82-88. doi: 10.2340/00015555-2789. Epub [PubMed PMID: 28902951]
Level 2 (mid-level) evidenceNair PA, Patel T. Dermatoscopic Features of Prurigo Nodularis. Indian dermatology online journal. 2019 Mar-Apr:10(2):187-189. doi: 10.4103/idoj.IDOJ_224_18. Epub [PubMed PMID: 30984602]
Nowak DA, Yeung J. Diagnosis and treatment of pruritus. Canadian family physician Medecin de famille canadien. 2017 Dec:63(12):918-924 [PubMed PMID: 29237630]
Przybilla B, Ring J, Völk M. [Total IgE levels in the serum in dermatologic diseases]. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete. 1986 Feb:37(2):77-82 [PubMed PMID: 3957665]
Katayama C, Hayashida Y, Sugiyama S, Shiohara T, Aoyama Y. Corticosteroid-resistant prurigo nodularis: a rare syringotropic variant associated with hypohidrosis. European journal of dermatology : EJD. 2019 Apr 1:29(2):212-213. doi: 10.1684/ejd.2019.3498. Epub [PubMed PMID: 30827950]
Legat FJ. The Antipruritic Effect of Phototherapy. Frontiers in medicine. 2018:5():333. doi: 10.3389/fmed.2018.00333. Epub 2018 Nov 30 [PubMed PMID: 30560129]
Gupta MA, Pur DR, Vujcic B, Gupta AK. Use of antiepileptic mood stabilizers in dermatology. Clinics in dermatology. 2018 Nov-Dec:36(6):756-764. doi: 10.1016/j.clindermatol.2018.08.005. Epub 2018 Aug 16 [PubMed PMID: 30446200]
Beck KM, Yang EJ, Sekhon S, Bhutani T, Liao W. Dupilumab Treatment for Generalized Prurigo Nodularis. JAMA dermatology. 2019 Jan 1:155(1):118-120. doi: 10.1001/jamadermatol.2018.3912. Epub [PubMed PMID: 30427994]
Qureshi AA, Abate LE, Yosipovitch G, Friedman AJ. A systematic review of evidence-based treatments for prurigo nodularis. Journal of the American Academy of Dermatology. 2019 Mar:80(3):756-764. doi: 10.1016/j.jaad.2018.09.020. Epub 2018 Sep 25 [PubMed PMID: 30261199]
Level 1 (high-level) evidenceSiepmann D, Lotts T, Blome C, Braeutigam M, Phan NQ, Butterfass-Bahloul T, Augustin M, Luger TA, Ständer S. Evaluation of the antipruritic effects of topical pimecrolimus in non-atopic prurigo nodularis: results of a randomized, hydrocortisone-controlled, double-blind phase II trial. Dermatology (Basel, Switzerland). 2013:227(4):353-60. doi: 10.1159/000355671. Epub 2013 Nov 23 [PubMed PMID: 24281309]
Level 1 (high-level) evidenceWong SS, Goh CL. Double-blind, right/left comparison of calcipotriol ointment and betamethasone ointment in the treatment of Prurigo nodularis. Archives of dermatology. 2000 Jun:136(6):807-8 [PubMed PMID: 10871962]
Level 3 (low-level) evidencePatel T, Ishiuji Y, Yosipovitch G. Menthol: a refreshing look at this ancient compound. Journal of the American Academy of Dermatology. 2007 Nov:57(5):873-8 [PubMed PMID: 17498839]
Level 3 (low-level) evidenceShintani T, Ohata C, Koga H, Ohyama B, Hamada T, Nakama T, Furumura M, Tsuruta D, Ishii N, Hashimoto T. Combination therapy of fexofenadine and montelukast is effective in prurigo nodularis and pemphigoid nodularis. Dermatologic therapy. 2014 May-Jun:27(3):135-9. doi: 10.1111/dth.12094. Epub 2013 Sep 17 [PubMed PMID: 24102897]
Hammes S, Hermann J, Roos S, Ockenfels HM. UVB 308-nm excimer light and bath PUVA: combination therapy is very effective in the treatment of prurigo nodularis. Journal of the European Academy of Dermatology and Venereology : JEADV. 2011 Jul:25(7):799-803. doi: 10.1111/j.1468-3083.2010.03865.x. Epub 2010 Oct 15 [PubMed PMID: 20946583]
Level 1 (high-level) evidenceBrenninkmeijer EE, Spuls PI, Lindeboom R, van der Wal AC, Bos JD, Wolkerstorfer A. Excimer laser vs. clobetasol propionate 0·05% ointment in prurigo form of atopic dermatitis: a randomized controlled trial, a pilot. The British journal of dermatology. 2010 Oct:163(4):823-31. doi: 10.1111/j.1365-2133.2010.09858.x. Epub [PubMed PMID: 20491772]
Level 2 (mid-level) evidenceWiznia LE, Callahan SW, Cohen DE, Orlow SJ. Rapid improvement of prurigo nodularis with cyclosporine treatment. Journal of the American Academy of Dermatology. 2018 Jun:78(6):1209-1211. doi: 10.1016/j.jaad.2018.02.024. Epub 2018 Feb 10 [PubMed PMID: 29438756]
Klejtman T, Beylot-Barry M, Joly P, Richard MA, Debarbieux S, Misery L, Wolkenstein P, Chosidow O, Ingen-Housz-Oro S. Treatment of prurigo with methotrexate: a multicentre retrospective study of 39 cases. Journal of the European Academy of Dermatology and Venereology : JEADV. 2018 Mar:32(3):437-440. doi: 10.1111/jdv.14646. Epub 2017 Nov 7 [PubMed PMID: 29055135]
Level 2 (mid-level) evidenceLear JT, English JS, Smith AG. Nodular prurigo responsive to azathioprine. The British journal of dermatology. 1996 Jun:134(6):1151 [PubMed PMID: 8763446]
Level 3 (low-level) evidenceGupta R. Treatment of prurigo nodularis with dexamethasone-cyclophosphamide pulse therapy. Indian journal of dermatology, venereology and leprology. 2016 Mar-Apr:82(2):239. doi: 10.4103/0378-6323.174413. Epub [PubMed PMID: 26924412]
Halvorsen JA, Aasebø W. Oral tacrolimus treatment of pruritus in prurigo nodularis. Acta dermato-venereologica. 2015 Sep:95(7):866-7. doi: 10.2340/00015555-2107. Epub [PubMed PMID: 25804254]
Level 3 (low-level) evidenceFeldmeyer L, Werner S, Kamarashev J, French LE, Hofbauer GF. Atopic prurigo nodularis responds to intravenous immunoglobulins. The British journal of dermatology. 2012 Feb:166(2):461-2. doi: 10.1111/j.1365-2133.2011.10587.x. Epub 2011 Dec 5 [PubMed PMID: 21910702]
Level 3 (low-level) evidenceChen M, Doherty SD, Hsu S. Innovative uses of thalidomide. Dermatologic clinics. 2010 Jul:28(3):577-86. doi: 10.1016/j.det.2010.03.003. Epub [PubMed PMID: 20510766]
Kanavy H, Bahner J, Korman NJ. Treatment of refractory prurigo nodularis with lenalidomide. Archives of dermatology. 2012 Jul:148(7):794-6. doi: 10.1001/archdermatol.2011.2918. Epub [PubMed PMID: 22801610]
Level 3 (low-level) evidencePhan NQ, Lotts T, Antal A, Bernhard JD, Ständer S. Systemic kappa opioid receptor agonists in the treatment of chronic pruritus: a literature review. Acta dermato-venereologica. 2012 Sep:92(5):555-60. doi: 10.2340/00015555-1353. Epub [PubMed PMID: 22504709]
Level 3 (low-level) evidenceHaas S, Capellino S, Phan NQ, Böhm M, Luger TA, Straub RH, Ständer S. Low density of sympathetic nerve fibers relative to substance P-positive nerve fibers in lesional skin of chronic pruritus and prurigo nodularis. Journal of dermatological science. 2010 Jun:58(3):193-7. doi: 10.1016/j.jdermsci.2010.03.020. Epub 2010 Apr 4 [PubMed PMID: 20417061]
Waldinger TP, Wong RC, Taylor WB, Voorhees JJ. Cryotherapy improves prurigo nodularis. Archives of dermatology. 1984 Dec:120(12):1598-600 [PubMed PMID: 6508332]
Level 3 (low-level) evidenceStoll DM, Fields JP, King LE Jr. Treatment of prurigo nodularis: use of cryosurgery and intralesional steroids plus lidocaine. The Journal of dermatologic surgery and oncology. 1983 Nov:9(11):922-4 [PubMed PMID: 6630706]
Level 3 (low-level) evidence