Introduction
Tuberculosis (TB), as a disease has been known since ancient times. It was described as early as 1000 to 600 BCE as "Yakshama" in ancient Indian medical literature as well as the Sushruta Samhita and Charaka Samhita.[1] In 1779, Sir Percival Pott described the tubercular disease of the spinal column presenting clinically with kyphotic deformity and neurological deficit in European patients.[2] Later, during the 19th and 20th centuries, the discovery of the underlying pathogenic microorganism (Mycobacterium tuberculosis), development of Bacillus Calmette-Guerin (BCG) vaccine, advancements made in the diagnostic modalities, chemotherapeutic agents, and surgical procedures had vastly revolutionized the management of spinal tuberculosis and provided the humanity with much better protection against this debilitating illness.[3]
Recently the disease has shown a significant resurgence in developed nations, particularly among the immunosuppressed population secondary to a "global migration phenomenon." This has posed a stiff challenge to the global community. There has been an ominous, increasing trend in the occurrence of multidrug-resistant bacterial strains of tuberculosis in the developing nations over the past decades. For these reasons, the disease continues to exist as a major, global public health menace to date.[4][5][6][7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The pathogen underlying tuberculosis is Mycobacterium genus complex. There are around 60 species, among which M. tuberculosis is the most common type. These organisms are fastidious, slow-growing and aerobic bacilli. Other non-tubercular mycobacterial species affecting humans include Mycobacterium avium, Mycobacterium bovis, Mycobacterium microti, and Mycobacterium africanum.[8] The TB bacilli are capable of remaining dormant for a long time; however, when the favorable conditions return, they tend to multiply once every 15 to 20 hours.[9]
The infection results in a granulomatous inflammatory reaction, which is typically characterized by caseating necrosis, lymphocytes, epithelioid cells, and Langhans-type giant cells.[10]
Some known risk factors for TB include prolonged exposure to infected patients, immunodeficiencies (HIV, alcohol, drug abuse), overcrowding, malnutrition, poverty, and lower socio-economic situation.
Epidemiology
The incidence of extrapulmonary TB (EPTB) is 3%, among which 10% of cases are skeletal TB. Spinal TB cases constitute 50% of skeletal tubercular infections.[6][11] The World Health Organisation (WHO) reported an incidence of 10.4 million new cases of tuberculosis in 2016, among which 46.5% of cases were reported from the South East Asian Region alone. India contributed to 23% of the global TB burden. WHO also reported a global increase in international migrants from 173 to 244 million between 2000 and 2015. This global increase in the phenomenon of migration has contributed to the recent resurgence of tuberculosis even in the developed world.[12][5][6]
Pathophysiology
Spinal TB is usually secondary to hematogenous spread from a primary site of infection (most commonly the lungs). The paradiscal vessels typically supply the subchondral bone on either side of the disc space and therefore, the most common site of vertebral involvement is paradiscal. The other patterns of involvement include central (with predominant vertebral body involvement), posterior (involving the posterior structures primarily) and non-osseous involvement (presenting with the abscess).[13][14] Progressive vertebral destruction leads to spinal kyphotic deformity and instability.
History and Physical
The clinical presentation of spinal tuberculosis is variable. The manifestations depend upon the duration of illness, severity of the disease, site of the lesion, and presence of associated complications including deformity and neurological deficit.[15] In uncomplicated disease, the patient typically presents with back pain; while the presentation associated with complicated tubercular spine disease involves deformity, instability, and neuro deficit. Back pain in tuberculosis can be related to the active disease itself (secondary to inflammation), bone destruction and instability. Rest pain is pathognomonic, and rarely, radicular pain can be the main presenting symptom. Constitutional symptoms including weight or appetite loss, fever, and malaise/ fatigue are less commonly associated with extrapulmonary tuberculosis than pulmonary disease.[16][17]
Cold Abscess
These abscesses typically lack all the inflammatory signs obvious in abscesses; and hence the name. In the cervical spine, they can present in the retropharyngeal space, anterior or posterior triangles of the neck or axilla. In the thoracic spine, they may present as pre- or paravertebral abscesses; or over the chest wall. In the lumbar spine, they may track down along the psoas muscle, Petit's triangle, Scarpa's triangle, or the gluteal region.[18]
Deformity
The clinical appearance of kyphotic deformity has been classified as knuckle (one vertebral involvement), gibbus (two vertebrae) and rounded kyphus (more than three vertebrae). Owing to the greater involvement of the anterior spinal column in TB, the spinal column progressively develops a kyphotic orientation; especially in the thoracic and thoracolumbar spine. Rajasekaran et al. purported a formula to predict the final kyphosis in adult population afflicted with spinal TB: y = a + bx, where y is the final kyphosis, a and b are constants equal to 5.5 and 30.5, respectively, and x is the initial loss of vertebral body height.[19] Jain et al. observed that kyphotic deformity greater than 60 degrees leads to significant disability and can potentially inflict neurological deficits.[20]
Neurological Deficit
A neurological deficit can occur either at the active stage of the disease (secondary to compression from an abscess, inflammatory tissue, sequestrum or spinal instability) or during the healed stage (usually secondary to mechanical traction over the internal gibbus or spinal instability).[21][22]
The initial compression in TB is secondary to vertebral body collapse, leading to anterior spinal tract involvement (exaggerated deep tendon reflexes and Babinski sign, further progression on to UMN-type motor deficit). Further on, the lateral spinal tracts are progressively involved (with loss of crude touch, pain, and temperature); followed by posterior column deficit (sphincter disturbances and complete sensory loss). The Frankel and ASIA scores, which were initially developed to classify neurological deficits in acute spinal injury may also be employed to classify the neuro deficiency in spinal tuberculosis.[23] Modified Tuli classification[24][25] is the most useful classification of Pott paraplegia with spinal cord involvement. There were five stages of Pott paraplegia:
- Stage 1: Deficit only evident, based on the clinical examination by the clinician (ankle clonus, exaggerated deep tendon reflexes and Babinski or plantar extensor)
- Stage 2: Patient has UMN-type of a motor deficit with spasticity, however, is still ambulatory. The anticipated motor score in tetraparesis is 60 to 100 and in paraparesis is between 80 and 100; sensory deficit involves the lateral column
- Stage 3: The patient is bedridden and spastic. The anticipated motor score in tetraparesis is 0 to 30, and in paraparesis is between 50 and 80; sensory deficit involves the lateral column
- Stage 4: The patient is bedridden with severe sensory loss/ pressure sores. The Anticipated motor score in tetraplegia is 0, and in paraplegia is between 50; sensory deficit involves posterior and lateral columns
- Stage 5: Similar to stage 4 +/- bladder/bowel involvement +/- flexor spasms/ flaccid tetraplegia/ paraplegia
Although most of the neuro deficit would fit into this classification, neuro deficits in intraspinal granulomas, cauda equina, or conus medullaris syndromes or TB of other atypical locations may not correspond to any of the stages mentioned above.
Pediatric Spinal TB
Owing to the immaturity and increased flexibility of the spine in children, they are particularly prone to developing severe deformity progression. Such worsening of deformity in children can also occur after the disease has completely healed, and therefore the need to follow-up this patient population until skeletal maturity cannot be understated. Rajasekaran et al. described 4 signs of "spine at risk" in children, which include:
- Retropulsion of the posterior aspect of the involved vertebra
- Facetal subluxation (separation of facets on lateral radiographs)
- Lateral translation of vertebrae (as observed on anteroposterior radiographs)
- The toppling of one vertebra over the other (defined by a line along the anterior surface of caudal normal vertebra crossing the mid-point of the anterior surface of the cranial normal vertebral bone)
He proposed that children with two or more of these signs had posterior facet disruption and required surgical intervention. He also proposed a classification system for the progression of the deformity in children:
- Type 1 curves where curvature increases until growth cessation or skeletal maturity and surgical intervention was required
- Type 2 curves where the deformity decreased with growth progression
- Type 3 curves where there was minimal change in the deformity either during the active or healed phases of the disease[26][27]
Atypical Presentations
Some of the atypical clinical presentations may include intervertebral disc prolapse, isolated abscess without skeletal involvement, and pure intraspinal granulomas. Similarly, atypical radiological presentations may include skip lesions, concentric vertebral collapse, circumferential vertebral involvement, isolated posterior arch involvement, ivory vertebra, isolated meningeal, neural or perineural involvement without any vertebral destruction and multifocal osseous lesions.[28]
Evaluation
The gold standard in the diagnosis of tuberculosis is the culture of Mycobacterium; however, the TB bacillus is fastidious; and the sole reliance on positive cultures for diagnosis can be associated with poor sensitivity.
Alternate laboratory reference standards for diagnosis include a histopathological demonstration of classic caseating granulomas, staining of smears to identify acid-fast bacilli (AFB), serological inflammatory markers, immunological tests, and molecular diagnostic modalities. A typical clinical presentation with additional indirect evidence from radiological and laboratory tests are usually necessary to clinch the diagnosis in a significant proportion of patients.
Imaging Modalities
Plain radiographs (15% sensitivity): Early stages (less than 30% vertebral destruction) – not much role; later stages (beyond 30% vertebral destruction) – can present with disc space reduction, endplate rarefaction, vertebral body destruction, instability, and spinal deformity. The chest x-ray is also an important investigation, as up to thirds of these patients with spinal TB can also have a concomitant pulmonary disease.[29]
Computed tomography (CT) (100% sensitivity): Can help in the diagnosis at a much earlier stage than plain x-rays. The types of vertebral destructive lesions by CT in spinal TB include fragmentary, osteolytic, subperiosteal, and localized sclerosis. CT scans can also aid in image-guided biopsy for establishing the diagnosis.[30][31][32]
Magnetic resonance imaging (MRI) (100% sensitivity and 80% specificity): MRI is the most useful modality in the diagnosis of spinal TB. MRI best detects the extent of soft tissue enhancement, the location of the abscess and spinal canal compromise. Gadolinium-enhanced MRI may provide additional information regarding the diagnosis. Screening sequences involving the whole spine can also help us in identifying non-contiguous vertebral involvement. MRI can also assess response to treatment.[33][34] The typical MRI findings including multi-segment sub-ligamentous collection, the occurrence of well-defined para/pre-vertebral mass or abscess with relatively thickened abscess walls, relatively spared disc space until the later stages of the disease and heterogeneous enhancement of vertebral body can help in distinguishing tubercular spondylodiscitis from other pyogenic infections.[35]
Nuclear imaging: 18 F-fluorodeoxyglucose (18F-FDG) labeled positron emission tomography (PET) scan provides evidence of functional activity in the involved tissues, based on the rationale that 18F-FDG is known to accumulate in macrophages at the inflammation site.[36] These modalities cannot help in distinguishing tubercular infections from malignancy or other pyogenic infections.
Laboratory Tests
Erythrocyte sedimentation rate (ESR) (60% to 90% sensitivity) is usually more than 20 mm/hour in TB and decreases with treatment response. Nevertheless, it is not a very sensitive test. C-reactive protein (CRP) (71% sensitivity) is more specific than ESR.[37]
Serological examination of IgG and IgM antibody levels against TB antigen cannot effectively distinguish between active or healed disease; natural TB infection or vaccinated persons; and is raised in both active and chronic stages of infection.[38][39]
Acid-fast bacilli (AFB) staining (25% to 75% sensitivity and 99% specificity): Using the Ziehl-Neelsen technique, tubercle bacillus presents with a bright red stain. At least, a concentration of 1 to 10 bacteria/ ml is necessary for detection.
TB culture: BACTEC radiometric culture assay (56% sensitivity and 100% specificity) takes 2 weeks of incubation time; while traditional culture on Lowenstein-Jenson (LJ) medium takes up to 6 weeks (47% sensitivity and 100% specificity).[40] Growth on the LJ medium requires a concentration of at least 10 to 100 bacteria/ml.
Molecular testing and polymerase chain reaction (PCR) (75% sensitivity and 97% specificity)[6]: This technique requires only a concentration of 1 to 10 bacilli/ ml. This is a very useful technique in paucibacillary, extrapulmonary TB infections.
Gene Xpert MTB/RIF: This is a fully automated test, which yields results within 90 minutes (82.9% sensitivity and 98% specificity). This test also helps in diagnosing resistance to rifampicin. WHO, in March 2017 recommended Xpert MTB/RIF Ultra (87.8% sensitivity and 94.8% specificity) as an investigation with good yield in pediatric and extrapulmonary patients.[6][41]
Histopathological evaluation: Characteristic findings including caseating necrosis, epithelioid cell granuloma, and Langhans giant cells can be found in 72% to 97% of patients.[42][43]
Tests to Detect Latent Tuberculosis
Mantoux test (40% to 55% sensitivity and 75% specificity): Skin hypersensitivity test (purified protein derivative [PPD]) has been recommended as a low-cost test in developing nations; nevertheless it is not an accurate test in endemic countries or immunodeficient patients.
Interferon-gamma release assay (50% to 65% sensitivity and 85% specificity): Measuring interferons produced in response to tubercular antigens; not useful in endemic regions.[44]
Whole blood-based enzyme-linked immunosorbent assay (ELISA)[45]
Treatment / Management
It is essential to classify spinal TB disease into a complicated and uncomplicated disease, based on their presentation. While uncomplicated spinal TB is essentially a medical disease; complicated TB spine patients need surgical intervention in addition to chemotherapy.[46][47]
Chemotherapy
The mainstay of treatment in spinal TB is chemotherapy (antitubercular treatment [ATT]). Tubercle bacilli may exist as intracellular or extracellular forms or as dormant or rapidly multiplying forms.[48] Therefore, multi-drug treatment is essential to attack the bacilli in various stages or forms and reduce the instance of drug resistance. The duration (6, 9, 12, or 18 months) and frequency (daily versus alternate-day regimen) of administration of ATT have been controversial.[49] WHO recommends 6 months of multidrug anti-tubercular therapy, including 2 months of four- or five-drug treatment (isoniazid, rifampicin, pyrazinamide, ethambutol, and/ or streptomycin) constituting the initiation" phase, followed by 4 months of "continuation" phase therapy with a two-drug regimen including isoniazid and rifampicin. The American Thoracic Spine Society recommends a regimen involving 9 months of treatment with the same drugs ("continuation" phase extending for a period of 7 months). The Canadian Thoracic Society recommends treatment for 9 to 12 months duration.[9] Other second-line anti-tubercular drugs including kanamycin, capreomycin, pyrazinamide, amikacin, among others are typically indicated when there is resistance or poor tolerance to first-line medications. A recent meta-analysis has not demonstrated any difference between self-administered and directly observed treatment (directly observed therapy, short course [DOTS]); nevertheless WHO has continued to recommend DOTS therapy for optimum results.[50][51][52](A1)
Multidrug Resistance
MDR-TB is defined as TB infection resistant to INH and rifampicin. Extensively drug-resistant TB (XDR-TB) is defined as infection resistant to INH and rifampicin, along with resistance to a fluoroquinolone and at least one injectable second-line medication. Velayati et al. described the term "totally drug-resistant" TB, where the tubercular strain is resistant to all first- and second-line drugs.[53][54][55](B2)
Surgical Management
Principles
Traditionally, TB was treated by radical debridement through an anterior approach.[56][57] However, following successful outcomes with multidrug chemotherapy and Medical Research Council observations,[57] Tuli et al. introduced the concept of "middle path regimen" in the treatment of tuberculosis.[58] This regimen recommended medical management in all patients, along with surgical management necessitated in the following situations: (A1)
- Lack of response to chemotherapy
- Recurrent disease
- Severe neurological weakness
- Static or progressive neuro deficit despite a course of ATT
- Deformity
- Debilitating pain
- Instability
The objectives of surgical intervention include drainage of an abscess, debridement of infected tissues, stabilization of vertebrae and deformity correction. Tubercle bacilli do not produce any biofilm and therefore, tubercular infections are amenable to stabilization with implants. The surgical procedure typically involves debridement and fusion (instrumented or non-instrumented) through anterior, posterior or combined approaches.[6] Abscesses can be drained through minimally invasive or open approaches.
Anterior Approach
As TB spine involves the anterior vertebral structures predominantly, debridement through anterior approach and fusion has been traditionally used to manage the diseased tissues directly. Nevertheless, the anterior approach has been reported to be associated with serious complications including graft-related complications (subsidence, slippage, fracture, absorption among others), approach-related complications (respiratory compromise) and even mortality. An ideal indication for anterior surgery includes patients without any posterior vertebral structure involvement, in other words, no panvertebral disease.[59][60][61](B2)
Posterior Approach
In modern spine surgery, posterior approaches are more preferred in TB spondylitis in view of the following reasons[62][63][64][65][66]:(B2)
- Ease and familiarity of the approach
- Availability of more robust pedicle screw system
- Less approach-related morbidity
- Ability to perform circumferential decompression through a transpedicular approach
- Ability to perform global reconstruction through transpedicular, transfacetal, costotransversectomy or extracavitary-extrapleural approaches
Combined (Anterior and Posterior) Approach
Typically, this approach should be reserved for severe destructive lesions with severe deformities or inherently unstable spines only, as it is associated with significant morbidities and complications. The approaches can be performed in single or more than one stage.[67][68](B2)
Minimally Invasive Surgery
Recently, minimally invasive approaches including thoracoscopic debridement, minimally invasive fusion procedures and posterolateral endoscopic debridement have been demonstrated to provide an excellent outcome in TB spondylitis.[69][70][71](B2)
Surgery in Healed Tuberculosis
Surgery may be indicated in healed disease with instability or kyphotic deformity more than 60 degrees.[72][73] The decision to perform surgery in such cases should be made after taking into consideration multiple factors including age, associated comorbidities, the severity of the deformity, the location of the spine involved, number of involved levels, and the surgeon's preference. Anterior approach can be particularly difficult in thoracic and thoracolumbar levels at the apex of kyphosis. Posterior approaches are the most popular and include transpedicular decancellation, Ponte's osteotomy, pedicle subtraction osteotomy/ closing wedge osteotomy, posterior vertebral column resection, and closing opening wedge osteotomy.[74][75] Combined anterior and posterior approaches may be required in more severe deformities, the disease involving two or three vertebrae or complex revision surgeries.[76](B3)
Differential Diagnosis
Radiological Differentials
- Pyogenic and fungal infections
- Neoplastic – Lytic benign, benign aggressive and malignant (primary tumors and spinal metastases): In general, spinal metastasis and primary spinal malignancies present with primary vertebral body involvement and disc space preservation as compared to TB and other infections. Tuberculosis also presents with soft tissue and perivertebral abscess, in comparison with malignant tumors.
Differentials Based on Pathological Appearance
- Other pathologies involving granulomatous infections and clinically mimic TB include:
- Atypical bacteria: Actinomyces israelii, Nocardia asteroids, Brucella
- Fungi: Coccidioides immitis, Blastomyces dermatitidis, Cryptococcus neoformans, Aspergillosis
- Spirochetes: Treponema pallidum
- Other pathologies presenting with non-caseating granulomas include Sarcoidosis, Wegener's granulomatosis, Crohn disease, and leprosy.
Prognosis
Clinico-Radiological Staging of Pott Spine (Prognostic Staging)[77]
- I: Predestructive stage; straightening of curvature, perivertebral muscle spasm, hyperemia on scintiscan (Duration fewer than 3 months)
- II: Early destructive stage; disc space reduction and paradiscal erosion, knuckle less than 10 degrees, MRI demonstrates marrow edema, and CT shows erosions or cavitations (Duration 2 to 4 months)
- III: Mild angular kyphosis; 2 to 3 vertebrae involved and kyphosis 10 - 30 degrees (Duration 3 to 9 months)
- IV: Moderate angular kyphosis; 2 to 3 vertebrae involved and kyphosis 30 to 60 degrees (Duration 6 to 24 months)
- V: Severe angular kyphosis; more than 3 vertebrae involved and kyphosis greater than 60 degrees (Duration more than 24 months)
Early diagnosis and treatment are of utmost importance in ensuring a good outcome in Pott spine.
In general, complicated tubercular spine disease (with associated deformity, instability or neuro deficit) has a poorer prognosis as compared to an uncomplicated disease. Other important prognostic factors include age (poorer outcome in extremes of ages),[7] immunodeficiencies (HIV, alcohol, drug abuse), overcrowding, malnutrition, poverty, and lower socio-economic situation. Poor compliance and poor tolerance to ATT (including deranged liver functions) is a major factor for drug failure in TB.
Poor Prognostic Factors in Pott Paraplegia
Level of disease (junctional vertebral levels), pan-vertebral involvement, long duration of neuro deficit, rapidity of progression of neuro deficit, the severity of deficit, nature of compression (abscess versus granuloma) and presence of spinal cord changes
Poor Prognosis for Deformity Progression
Age less than 10 years, Kyphosis angle greater than 30 degrees, three or more vertebrae involved, greater than or equal to 1.5 vertebral body loss, pan-vertebral disease, and evidence of instability
Complications
- Failure of treatment: Depends on the presentation (complicated versus uncomplicated), clinical and radiological prognostic factors, patient compliance to chemotherapy, stage of the disease, drug resistance and other patient-related factors (socio-economic factors, general health, nourishment among others)
- Abscess
- Neuro deficit
- Spinal instability
- Spinal deformity (kyphosis)
- Systemic TB disease
Deterrence and Patient Education
Patient education is of utmost importance in the management of TB at the level of an individual, as well as the whole community. The need for isolation of patients who can potentially transmit the disease to others cannot be understated. Although extrapulmonary (including spinal TB) disease is not communicable, there can be an associated pulmonary involvement in a proportion of these patients. The role of strict compliance to long term chemotherapy in ensuring complete cure from the infection needs to be well understood by the patients. Directly observed therapy can ameliorate the compliance rates in TB patients. Appropriate bracing can also reduce the occurrence of kyphosis in non-operatively treated patients. In pediatric disease, the chances of progression of deformity even years after healing of the infection and the need for regular follow-up until skeletal maturity need to be clearly communicated to the parents.
Enhancing Healthcare Team Outcomes
The management of spinal TB disease is challenging and complex. While the major role in patient management is primarily played by the treating surgeon (spine/ orthopedic/neurosurgeon), the importance of contributions from the entire team including pediatrician, geriatrician, physician, hepatologist (for hepatic function monitoring), infectious disease specialist, radiologist, pathologist, occupational therapist, orthotist, physiotherapist, nurse practitioner, and social workers cannot be understated. The major initial challenge in the management of the disease lies in early diagnosis and timely treatment. Later, identification of the disease-related complications and appropriate decision-making regarding the need for surgical intervention in addition to long-term chemotherapy constitute the next major task. The challenges associated with the administration of long-term chemotherapy (including adverse effects and complications of the drug, compliance issues, socio-economic factors among others) are also greatly significant; and need to be addressed. At each of these stages of disease management, major contributions from each member of the health care team are required. During the perioperative period, important issues including adequate maintenance of nutrition, availability of proper financial, and social support system (to discuss ambulatory restrictions, poor general medical conditions, need for long term medications, as well as complications encountered during the course of treatment), patient education, and challenges faced by the family or caregivers have to be addressed as well.
Based on the available literature, evidence on the role and efficiency of chemotherapy in tubercular spine disease is very strong. (Level I) However, evidence and recommendations regarding the ideal duration of treatment, indications for surgery and appropriate surgical intervention are largely based on level IV and V studies.
Media
(Click Image to Enlarge)
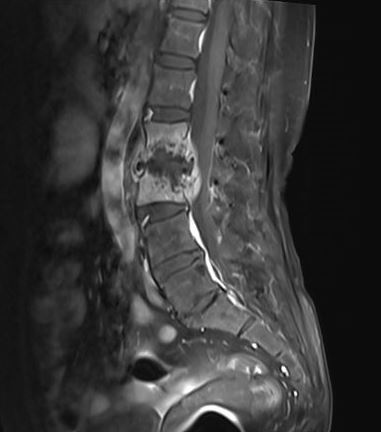
Pott spine Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
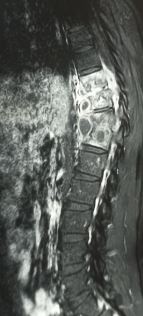
Pott spine Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)

Sacral TB with abscess Contributed by Sunil Munakomi, MD
References
Tuli SM. Historical aspects of Pott's disease (spinal tuberculosis) management. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013 Jun:22 Suppl 4(Suppl 4):529-38. doi: 10.1007/s00586-012-2388-7. Epub 2012 Jul 17 [PubMed PMID: 22802129]
Dobson J. Percivall Pott. Annals of the Royal College of Surgeons of England. 1972 Jan:50(1):54-65 [PubMed PMID: 4550865]
Oettinger T, Jørgensen M, Ladefoged A, Hasløv K, Andersen P. Development of the Mycobacterium bovis BCG vaccine: review of the historical and biochemical evidence for a genealogical tree. Tubercle and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease. 1999:79(4):243-50 [PubMed PMID: 10692993]
McLain RF, Isada C. Spinal tuberculosis deserves a place on the radar screen. Cleveland Clinic journal of medicine. 2004 Jul:71(7):537-9, 543-9 [PubMed PMID: 15320363]
Level 3 (low-level) evidenceArockiaraj J, Karthik R, Michael JS, Amritanand R, David KS, Krishnan V, Sundararaj GD. 'Need of the Hour': Early Diagnosis and Management of Multidrug Resistant Tuberculosis of the Spine: An Analysis of 30 Patients from a "High Multidrug Resistant Tuberculosis Burden" Country. Asian spine journal. 2019 Apr:13(2):265-271. doi: 10.31616/asj.2018.0073. Epub 2019 Jan 24 [PubMed PMID: 30669824]
Rajasekaran S, Soundararajan DCR, Shetty AP, Kanna RM. Spinal Tuberculosis: Current Concepts. Global spine journal. 2018 Dec:8(4 Suppl):96S-108S. doi: 10.1177/2192568218769053. Epub 2018 Dec 13 [PubMed PMID: 30574444]
Shetty AP, Viswanathan VK, Kanna RM, Shanmuganathan R. Tubercular spondylodiscitis in elderly is a more severe disease: a report of 66 consecutive patients. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2017 Dec:26(12):3178-3186. doi: 10.1007/s00586-017-5157-9. Epub 2017 Jun 7 [PubMed PMID: 28593383]
Jain AK, Dhammi IK. Tuberculosis of the spine: a review. Clinical orthopaedics and related research. 2007 Jul:460():39-49 [PubMed PMID: 17438468]
Rasouli MR, Mirkoohi M, Vaccaro AR, Yarandi KK, Rahimi-Movaghar V. Spinal tuberculosis: diagnosis and management. Asian spine journal. 2012 Dec:6(4):294-308. doi: 10.4184/asj.2012.6.4.294. Epub 2012 Dec 14 [PubMed PMID: 23275816]
Jain AK. Tuberculosis of spine: Research evidence to treatment guidelines. Indian journal of orthopaedics. 2016 Jan-Feb:50(1):3-9. doi: 10.4103/0019-5413.173518. Epub [PubMed PMID: 26955172]
Kulchavenya E. Extrapulmonary tuberculosis: are statistical reports accurate? Therapeutic advances in infectious disease. 2014 Apr:2(2):61-70. doi: 10.1177/2049936114528173. Epub [PubMed PMID: 25165556]
Level 3 (low-level) evidenceGlaziou P, Floyd K, Raviglione MC. Global Epidemiology of Tuberculosis. Seminars in respiratory and critical care medicine. 2018 Jun:39(3):271-285. doi: 10.1055/s-0038-1651492. Epub 2018 Aug 2 [PubMed PMID: 30071543]
Goni V, Thapa BR, Vyas S, Gopinathan NR, Rajan Manoharan S, Krishnan V. Bilateral psoas abscess: atypical presentation of spinal tuberculosis. Archives of Iranian medicine. 2012 Apr:15(4):253-6 [PubMed PMID: 22424047]
Level 3 (low-level) evidenceRajasekaran S, Kanna RM, Shetty AP. Pathophysiology and Treatment of Spinal Tuberculosis. JBJS reviews. 2014 Sep 23:2(9):. pii: e4. doi: 10.2106/JBJS.RVW.M.00130. Epub [PubMed PMID: 27490153]
Ansari S, Amanullah MF, Ahmad K, Rauniyar RK. Pott's Spine: Diagnostic Imaging Modalities and Technology Advancements. North American journal of medical sciences. 2013 Jul:5(7):404-11. doi: 10.4103/1947-2714.115775. Epub [PubMed PMID: 24020048]
Su SH, Tsai WC, Lin CY, Lin WR, Chen TC, Lu PL, Huang PM, Tsai JR, Wang YL, Feng MC, Wang TP, Chen YH. Clinical features and outcomes of spinal tuberculosis in southern Taiwan. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi. 2010 Aug:43(4):291-300. doi: 10.1016/S1684-1182(10)60046-1. Epub [PubMed PMID: 20688289]
Level 2 (mid-level) evidenceHayes AJ, Choksey M, Barnes N, Sparrow OC. Spinal tuberculosis in developed countries: difficulties in diagnosis. Journal of the Royal College of Surgeons of Edinburgh. 1996 Jun:41(3):192-6 [PubMed PMID: 8763187]
Faure E, Souilamas R, Riquet M, Chehab A, Le Pimpec-Barthes F, Manac'h D, Debesse B. Cold abscess of the chest wall: a surgical entity? The Annals of thoracic surgery. 1998 Oct:66(4):1174-8 [PubMed PMID: 9800802]
Level 2 (mid-level) evidenceRajasekaran S, Shanmugasundaram TK. Prediction of the angle of gibbus deformity in tuberculosis of the spine. The Journal of bone and joint surgery. American volume. 1987 Apr:69(4):503-9 [PubMed PMID: 3571308]
Level 3 (low-level) evidenceJain AK, Aggarwal PK, Arora A, Singh S. Behaviour of the kyphotic angle in spinal tuberculosis. International orthopaedics. 2004 Apr:28(2):110-4 [PubMed PMID: 15224169]
Hodgson AR, Skinsnes OK, Leong CY. The pathogenesis of Pott's paraplegia. The Journal of bone and joint surgery. American volume. 1967 Sep:49(6):1147-56 [PubMed PMID: 6038860]
Subramani S, Shetty AP, Kanna RM, Shanmuganathan R. Ossified ligamentum flavum causing neurological deficit above the level of post-tuberculous kyphotic deformity. Journal of clinical orthopaedics and trauma. 2017 Apr-Jun:8(2):174-177. doi: 10.1016/j.jcot.2016.09.012. Epub 2016 Oct 19 [PubMed PMID: 28720997]
Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH, Vernon JD, Walsh JJ. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia. 1969 Nov:7(3):179-92 [PubMed PMID: 5360915]
Jain AK, Sinha S. Evaluation of systems of grading of neurological deficit in tuberculosis of spine. Spinal cord. 2005 Jun:43(6):375-80 [PubMed PMID: 15685259]
Level 1 (high-level) evidenceJain AK, Kumar J. Tuberculosis of spine: neurological deficit. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013 Jun:22 Suppl 4(Suppl 4):624-33. doi: 10.1007/s00586-012-2335-7. Epub 2012 May 8 [PubMed PMID: 22565802]
Rajasekaran S. The natural history of post-tubercular kyphosis in children. Radiological signs which predict late increase in deformity. The Journal of bone and joint surgery. British volume. 2001 Sep:83(7):954-62 [PubMed PMID: 11603534]
Rajasekaran S. Buckling collapse of the spine in childhood spinal tuberculosis. Clinical orthopaedics and related research. 2007 Jul:460():86-92 [PubMed PMID: 17471103]
Pande KC, Babhulkar SS. Atypical spinal tuberculosis. Clinical orthopaedics and related research. 2002 May:(398):67-74 [PubMed PMID: 11964633]
Dharmalingam M. Tuberculosis of the spine-the Sabah experience. Epidemiology, treatment and results. Tuberculosis (Edinburgh, Scotland). 2004:84(1-2):24-8 [PubMed PMID: 14670343]
Level 2 (mid-level) evidenceSinan T, Al-Khawari H, Ismail M, Ben-Nakhi A, Sheikh M. Spinal tuberculosis: CT and MRI feature. Annals of Saudi medicine. 2004 Nov-Dec:24(6):437-41 [PubMed PMID: 15646161]
Desai SS. Early diagnosis of spinal tuberculosis by MRI. The Journal of bone and joint surgery. British volume. 1994 Nov:76(6):863-9 [PubMed PMID: 7983108]
Adapon BD, Legada BD Jr, Lim EV, Silao JV Jr, Dalmacio-Cruz A. CT-guided closed biopsy of the spine. Journal of computer assisted tomography. 1981 Feb:5(1):73-8 [PubMed PMID: 7240501]
Level 3 (low-level) evidenceKim NH, Lee HM, Suh JS. Magnetic resonance imaging for the diagnosis of tuberculous spondylitis. Spine. 1994 Nov 1:19(21):2451-5 [PubMed PMID: 7846600]
Level 3 (low-level) evidenceKaila R, Malhi AM, Mahmood B, Saifuddin A. The incidence of multiple level noncontiguous vertebral tuberculosis detected using whole spine MRI. Journal of spinal disorders & techniques. 2007 Feb:20(1):78-81 [PubMed PMID: 17285057]
Level 2 (mid-level) evidenceGouliamos AD, Kehagias DT, Lahanis S, Athanassopoulou AA, Moulopoulou ES, Kalovidouris AA, Trakadas SJ, Vlahos LJ. MR imaging of tuberculous vertebral osteomyelitis: pictorial review. European radiology. 2001:11(4):575-9 [PubMed PMID: 11354749]
Vorster M, Sathekge MM, Bomanji J. Advances in imaging of tuberculosis: the role of ¹⁸F-FDG PET and PET/CT. Current opinion in pulmonary medicine. 2014 May:20(3):287-93. doi: 10.1097/MCP.0000000000000043. Epub [PubMed PMID: 24614238]
Level 3 (low-level) evidenceGuo LX, Ma YZ, Li HW, Xue HB, Peng W, Luo XB. [Variety of ESR and C-reactive protein levels during perioperative period in spinal tuberculosis]. Zhongguo gu shang = China journal of orthopaedics and traumatology. 2010 Mar:23(3):200-2 [PubMed PMID: 20415078]
Jain AK, Jena SK, Singh MP, Dhammi IK, Ramachadran VG, Dev G. Evaluation of clinico-radiological, bacteriological, serological, molecular and histological diagnosis of osteoarticular tuberculosis. Indian journal of orthopaedics. 2008 Apr:42(2):173-7. doi: 10.4103/0019-5413.40253. Epub [PubMed PMID: 19826523]
Chen CH, Chen YM, Lee CW, Chang YJ, Cheng CY, Hung JK. Early diagnosis of spinal tuberculosis. Journal of the Formosan Medical Association = Taiwan yi zhi. 2016 Oct:115(10):825-836. doi: 10.1016/j.jfma.2016.07.001. Epub 2016 Aug 10 [PubMed PMID: 27522334]
Cruciani M, Scarparo C, Malena M, Bosco O, Serpelloni G, Mengoli C. Meta-analysis of BACTEC MGIT 960 and BACTEC 460 TB, with or without solid media, for detection of mycobacteria. Journal of clinical microbiology. 2004 May:42(5):2321-5 [PubMed PMID: 15131224]
Level 1 (high-level) evidenceMaynard-Smith L, Larke N, Peters JA, Lawn SD. Diagnostic accuracy of the Xpert MTB/RIF assay for extrapulmonary and pulmonary tuberculosis when testing non-respiratory samples: a systematic review. BMC infectious diseases. 2014 Dec 31:14():709. doi: 10.1186/s12879-014-0709-7. Epub 2014 Dec 31 [PubMed PMID: 25599808]
Level 1 (high-level) evidenceLifeso RM, Weaver P, Harder EH. Tuberculous spondylitis in adults. The Journal of bone and joint surgery. American volume. 1985 Dec:67(9):1405-13 [PubMed PMID: 4077912]
Alothman A, Memish ZA, Awada A, Al-Mahmood S, Al-Sadoon S, Rahman MM, Khan MY. Tuberculous spondylitis: analysis of 69 cases from Saudi Arabia. Spine. 2001 Dec 15:26(24):E565-70 [PubMed PMID: 11740373]
Level 2 (mid-level) evidenceKumar R, Das RK, Mahapatra AK. Role of interferon gamma release assay in the diagnosis of Pott disease. Journal of neurosurgery. Spine. 2010 May:12(5):462-6. doi: 10.3171/2009.10.SPINE093. Epub [PubMed PMID: 20433293]
Brodie D, Lederer DJ, Gallardo JS, Trivedi SH, Burzynski JN, Schluger NW. Use of an interferon-gamma release assay to diagnose latent tuberculosis infection in foreign-born patients. Chest. 2008 Apr:133(4):869-74. doi: 10.1378/chest.07-1815. Epub 2008 Jan 15 [PubMed PMID: 18198254]
Rajasekaran S, Khandelwal G. Drug therapy in spinal tuberculosis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013 Jun:22 Suppl 4(Suppl 4):587-93. doi: 10.1007/s00586-012-2337-5. Epub 2012 May 12 [PubMed PMID: 22581190]
Zhang Z, Luo F, Zhou Q, Dai F, Sun D, Xu J. The outcomes of chemotherapy only treatment on mild spinal tuberculosis. Journal of orthopaedic surgery and research. 2016 May 14:11(1):49. doi: 10.1186/s13018-016-0385-y. Epub 2016 May 14 [PubMed PMID: 27177692]
Bodapati PC, Vemula RCV, Mohammad AA, Mohan A. Outcome and management of spinal tuberculosis according to severity at a tertiary referral center. Asian journal of neurosurgery. 2017 Jul-Sep:12(3):441-446. doi: 10.4103/1793-5482.180924. Epub [PubMed PMID: 28761522]
Jawahar MS. Current trends in chemotherapy of tuberculosis. The Indian journal of medical research. 2004 Oct:120(4):398-417 [PubMed PMID: 15520489]
Ali A, Musbahi O, White VLC, Montgomery AS. Spinal Tuberculosis: A Literature Review. JBJS reviews. 2019 Jan:7(1):e9. doi: 10.2106/JBJS.RVW.18.00035. Epub [PubMed PMID: 30694877]
Cox HS, Morrow M, Deutschmann PW. Long term efficacy of DOTS regimens for tuberculosis: systematic review. BMJ (Clinical research ed.). 2008 Mar 1:336(7642):484-7. doi: 10.1136/bmj.39463.640787.BE. Epub 2008 Feb 4 [PubMed PMID: 18250104]
Level 1 (high-level) evidenceValsalan R, Purushothaman R, Raveendran M, Zacharia B, Surendran S. Efficacy of directly observed treatment short-course intermittent regimen in spinal tuberculosis. Indian journal of orthopaedics. 2012 Mar:46(2):138-44. doi: 10.4103/0019-5413.93673. Epub [PubMed PMID: 22448050]
Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, Zeller K, Andrews J, Friedland G. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet (London, England). 2006 Nov 4:368(9547):1575-80 [PubMed PMID: 17084757]
Pawar UM, Kundnani V, Agashe V, Nene A, Nene A. Multidrug-resistant tuberculosis of the spine--is it the beginning of the end? A study of twenty-five culture proven multidrug-resistant tuberculosis spine patients. Spine. 2009 Oct 15:34(22):E806-10. doi: 10.1097/BRS.0b013e3181af7797. Epub [PubMed PMID: 19829244]
Level 2 (mid-level) evidenceVelayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, ZiaZarifi AH, Hoffner SE. Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in iran. Chest. 2009 Aug:136(2):420-425. doi: 10.1378/chest.08-2427. Epub 2009 Apr 6 [PubMed PMID: 19349380]
Level 2 (mid-level) evidenceHODGSON AR, STOCK FE. Anterior spinal fusion a preliminary communication on the radical treatment of Pott's disease and Pott's paraplegia. The British journal of surgery. 1956 Nov:44(185):266-75 [PubMed PMID: 13383153]
. A controlled trial of six-month and nine-month regimens of chemotherapy in patients undergoing radical surgery for tuberculosis of the spine in Hong Kong. Tenth report of the Medical Research Council Working Party on Tuberculosis of the Spine. Tubercle. 1986 Dec:67(4):243-59 [PubMed PMID: 2889281]
Level 1 (high-level) evidenceTuli SM. Severe kyphotic deformity in tuberculosis of the spine. International orthopaedics. 1995:19(5):327-31 [PubMed PMID: 8567145]
Govender S, Kumar KP. Cortical allografts in spinal tuberculosis. International orthopaedics. 2003:27(4):244-8 [PubMed PMID: 12715238]
Benli IT, Kaya A, Acaroğlu E. Anterior instrumentation in tuberculous spondylitis: is it effective and safe? Clinical orthopaedics and related research. 2007 Jul:460():108-16 [PubMed PMID: 17452918]
Christodoulou AG, Givissis P, Karataglis D, Symeonidis PD, Pournaras J. Treatment of tuberculous spondylitis with anterior stabilization and titanium cage. Clinical orthopaedics and related research. 2006 Mar:444():60-5 [PubMed PMID: 16523128]
Level 2 (mid-level) evidenceChen YC, Chang MC, Wang ST, Yu WK, Liu CL, Chen TH. One-stage posterior surgery for treatment of advanced spinal tuberculosis. Journal of the Chinese Medical Association : JCMA. 2003 Jul:66(7):411-7 [PubMed PMID: 14509403]
Lee SH, Sung JK, Park YM. Single-stage transpedicular decompression and posterior instrumentation in treatment of thoracic and thoracolumbar spinal tuberculosis: a retrospective case series. Journal of spinal disorders & techniques. 2006 Dec:19(8):595-602 [PubMed PMID: 17146304]
Level 2 (mid-level) evidenceZhong W, Xiong G, Wang B, Lu C, Dai Z, Lv G. Surgical management for thoracic spinal tuberculosis posterior only versus anterior video-assisted thoracoscopic surgery. PloS one. 2015:10(3):e0119759. doi: 10.1371/journal.pone.0119759. Epub 2015 Mar 17 [PubMed PMID: 25781165]
Level 2 (mid-level) evidenceJain AK, Dhammi IK, Prashad B, Sinha S, Mishra P. Simultaneous anterior decompression and posterior instrumentation of the tuberculous spine using an anterolateral extrapleural approach. The Journal of bone and joint surgery. British volume. 2008 Nov:90(11):1477-81. doi: 10.1302/0301-620X.90B11.20972. Epub [PubMed PMID: 18978269]
Moon MS. Tuberculosis of spine: current views in diagnosis and management. Asian spine journal. 2014 Feb:8(1):97-111. doi: 10.4184/asj.2014.8.1.97. Epub 2014 Feb 6 [PubMed PMID: 24596613]
Chen WJ, Wu CC, Jung CH, Chen LH, Niu CC, Lai PL. Combined anterior and posterior surgeries in the treatment of spinal tuberculous spondylitis. Clinical orthopaedics and related research. 2002 May:(398):50-9 [PubMed PMID: 11964631]
Talu U, Gogus A, Ozturk C, Hamzaoglu A, Domanic U. The role of posterior instrumentation and fusion after anterior radical debridement and fusion in the surgical treatment of spinal tuberculosis: experience of 127 cases. Journal of spinal disorders & techniques. 2006 Dec:19(8):554-9 [PubMed PMID: 17146297]
Level 2 (mid-level) evidenceJayaswal A, Upendra B, Ahmed A, Chowdhury B, Kumar A. Video-assisted thoracoscopic anterior surgery for tuberculous spondylitis. Clinical orthopaedics and related research. 2007 Jul:460():100-7 [PubMed PMID: 17471105]
Level 2 (mid-level) evidenceKandwal P, G V, Jayaswal A. Management of Tuberculous Infection of the Spine. Asian spine journal. 2016 Aug:10(4):792-800. doi: 10.4184/asj.2016.10.4.792. Epub 2016 Aug 16 [PubMed PMID: 27559464]
Ito M, Sudo H, Abumi K, Kotani Y, Takahata M, Fujita M, Minami A. Minimally invasive surgical treatment for tuberculous spondylodiscitis. Minimally invasive neurosurgery : MIN. 2009 Oct:52(5-6):250-3. doi: 10.1055/s-0029-1220685. Epub 2010 Jan 14 [PubMed PMID: 20077368]
Level 3 (low-level) evidenceRajasekaran S. Natural history of Pott's kyphosis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2013 Jun:22 Suppl 4(Suppl 4):634-40. doi: 10.1007/s00586-012-2336-6. Epub 2012 May 15 [PubMed PMID: 22584918]
Grevitt M, Kamath V, Avadhani A, Rajasekaran S. Correction of thoracic kyphosis with Ponte osteotomy. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2010 Feb:19(2):351-2. doi: 10.1007/s00586-010-1311-3. Epub [PubMed PMID: 20135330]
Level 3 (low-level) evidenceKalra KP, Dhar SB, Shetty G, Dhariwal Q. Pedicle subtraction osteotomy for rigid post-tuberculous kyphosis. The Journal of bone and joint surgery. British volume. 2006 Jul:88(7):925-7 [PubMed PMID: 16798997]
Rajasekaran S, Vijay K, Shetty AP. Single-stage closing-opening wedge osteotomy of spine to correct severe post-tubercular kyphotic deformities of the spine: a 3-year follow-up of 17 patients. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2010 Apr:19(4):583-92. doi: 10.1007/s00586-009-1234-z. Epub 2009 Dec 15 [PubMed PMID: 20013004]
Zheng B, Hao D, Guo H, He B. Anterior versus posterior surgical approach for lumbosacral tuberculosis. The Journal of international medical research. 2018 Jul:46(7):2569-2577. doi: 10.1177/0300060518764933. Epub 2018 Mar 27 [PubMed PMID: 29584540]
Kumar K. Spinal tuberculosis, natural history of disease, classifications and principles of management with historical perspective. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2016 Aug:26(6):551-8. doi: 10.1007/s00590-016-1811-x. Epub 2016 Jul 19 [PubMed PMID: 27435619]
Level 3 (low-level) evidence