Introduction
Popliteal artery aneurysms occur when the diameter of the popliteal artery undergoes focal dilation and exceeds 50% of its normal range. The normal diameter of the popliteal artery ranges from 0.7 to 1.1 cm. Popliteal artery aneurysms manifest as either fusiform (diffuse dilation) or saccular (asymmetrical) dilations and constitute a significant majority, comprising 85% of all peripheral aneurysms. Notably, popliteal artery aneurysms are frequently associated with abdominal aortic aneurysms, with a prevalence of 40% to 50%.[1][2][3]
The popliteal artery is considered a continuation of the superficial femoral artery after it passes through the adductor magnus hiatus. The vessel traverses the popliteal fossa alongside the vein and terminates by bifurcating into the anterior tibial artery and tibioperoneal trunk, situated at the lower border of the popliteus muscle, aligned with the tibial tuberosity level.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Modifiable risk factors include smoking, atherosclerosis, and connective tissue disorders such as Marfan syndrome and Ehlers-Danlos syndrome. Non-modifiable risk factors include advanced age, male gender, White race, and family history of aneurysmal disease.[4][2]
Epidemiology
The exact incidence of popliteal artery aneurysms is unknown, as no population-based study has been published. However, a few studies issued by different institutions suggest that popliteal artery aneurysm prevalence increases with age and peaks in the sixth or seventh decades of life. The incidence of femoral and popliteal aneurysms in persons with abdominal aortic aneurysms appears higher than in the general population. In one study of 225 patients, 28% (n=63) had a popliteal artery aneurysm greater than or equal to 10.5 mm, 19% (n=43) had a popliteal artery aneurysm greater than or equal to 12 mm, and 11% (n=25) had a popliteal artery aneurysm greater than or equal to 15 mm.
Pathophysiology
The etiology of popliteal artery aneurysms and general aneurysms is unknown. Molecular studies suggest that a combination of genetic defects and inflammatory processes are responsible. Atherosclerosis tends to increase flow turbulence distal to a stenosis, leading to a pathological dilation of the artery. According to current research, decreased wall strength associated with inflammatory cell infiltration results in aneurysm formation.[5]
History and Physical
Most commonly, popliteal artery aneurysms are asymptomatic. If patients exhibit chronic symptoms, these are usually secondary to mass effect and compression of adjacent structures, such as the tibial nerve, which causes leg pain or paresthesias. The popliteal vein also may be compressed, which causes calf swelling. Progressive luminal narrowing of the popliteal artery from thrombus formation may cause an insidious onset of claudication—approximately 50% of the patients present with bilateral aneurysms.
When an aneurysm acutely thromboses, the most common symptoms are acute lower extremity ischemia resulting in the acute onset of pain, paresthesias, paresis, pallor, and poikilothermia due to either aneurysmal intraluminal thrombosis or distal embolization of thrombus. Distal embolization can manifest as blue toe syndrome and/or acral cyanosis. Approximately 30% of untreated patients experience acute thrombosis and distal embolization with the risk of possible limb loss. Patients who develop acute thrombosis or embolism have a relatively poor prognosis, with a 15% amputation rate due to the occlusion of runoff vessels. The popliteal fossa should be examined bilaterally with the knee in a semi-flexed position. About 60% of patients with popliteal aneurysms have a palpable pulsatile mass at the knee joint level.
Evaluation
Duplex ultrasonography is the ideal screening and diagnostic imaging modality to detect a popliteal artery aneurysm and estimate the diameter. The duplex ultrasonography also provides detailed information regarding vessel patency, the development of mural thrombus, and the status of outflow vessels (see Image. Ultrasound of Left Popliteal Artery Aneurysm). Computed tomography (CT) or magnetic resonance angiography are other alternatives to duplex ultrasonography. They can accurately measure true lumen diameters or assist in planning surgical repair (see Image. Popliteal Artery Aneurysm Visualized on Magnetic Resonance Angiography). Conventional angiography is reserved for either elective endovascular repair of an aneurysm or in cases of threatening acute limb ischemia for thrombolytic therapy.[6][7][8]
Treatment / Management
All symptomatic popliteal artery aneurysms require repair because of an increased incidence of thrombosis or limb loss. Asymptomatic aneurysms with a diameter greater than 2 cm are considered an indication for elective operation to avoid complications such as limb-threatening ischemia. Greater than 45 angulation in asymptomatic aneurysms warrants surgical intervention because of the risk of acute limb ischemia secondary to kinking of the vessel.[9][10][6]
Conservative Management
Asymptomatic aneurysms less than 2 cm are safely manageable via duplex surveillance.
Open surgical approach: Traditional open surgery involves ligation of the popliteal artery proximal (above the knee) and distal (below the knee) below the aneurysmal sac and bypassing the excluded segment using either a reversed autologous vein graft (saphenous vein) or prosthetic graft (see Image. Intraoperative Popliteal Artery Aneurysm Repair). An alternative surgical approach is aneurysmectomy, followed by an interposition bypass with a prosthetic graft between the proximal and distal normal segments of the popliteal artery. However, the former method is more common.
Endovascular approach: Recently, endovascular techniques have gained popularity in popliteal artery aneurysm repair as an alternative to the open surgical approach. This technique excludes the aneurysmal sac with stent-graft implantation. Recent studies show that popliteal artery stenting is a safe alternative technique for the treatment of popliteal artery aneurysms, especially in high-risk patients. The advantages of the endovascular technique include a shorter hospital stay and an abbreviated surgical time compared to open surgical intervention. Disadvantages include higher 30-day graft thrombosis rates (9% in the endovascular treatment group versus 2% in the open surgical treatment group) and higher 30-day re-intervention rates (9% in the endovascular treatment group versus 4% in the open surgical treatment group). The 2 repair groups have no significant difference in mortality or limb loss rates. Other reviews have also concurred that endovascular and open repair of popliteal artery aneurysms is safe.[11] Open repair is associated with greater limb salvage, fewer reintervention rates, and decreased short-term thrombosis.[12](A1)
Management of Acutely Thrombosed Aneurysms
Management varies according to the presentation. Asymptomatic patients with completely thrombosed popliteal artery aneurysms and those who are non-ambulatory patients or have acutely thrombosed aneurysms with a poor runoff despite thrombolysis are not candidates for surgical intervention. Only patients with disabling symptoms or critical limb ischemia are treated with surgical bypass as the first line of therapy. Patients presenting with acute limb-threatening ischemia should undergo urgent bypass. Acute thrombosis should be treated with intravenous heparin and continuous heparin infusion to limit the extension of the thrombus. However, some surgeons advise that threatening ischemia is better treated with thrombectomy, followed by bypass surgery.
Intra-Arterial Thrombolytic Therapy
This method is indicated when angiography demonstrates no target vessel or multiple distal thrombi are noted. The decision analysis suggested that open repair with great saphenous vein (GSV) bypass might be considered the preferred treatment for older, asymptomatic patients with popliteal artery aneurysms. The incidence of popliteal artery aneurysms in the general population is low, ranging from 0.1% to 2.8%. According to the rarity, screening unselected patients or patients undergoing abdominal aorta aneurysm is not cost-effective. However, patients with a known popliteal artery aneurysm have a significantly higher risk of having a contralateral popliteal artery aneurysm or an abdominal aortic aneurysm. The literature review suggests that younger age, the availability of a single-segment GSV, complicated runoff vessels, and lower surgical risk favor the option of open surgical repair. However, with advancing age and insufficient GSV, satisfactory landing zones, tibial runoff, and higher surgical risk might favor the endovascular options.
Therefore, in patients with poor tibial or pedal runoff, open surgical repair (OPAR) with GSV is considered preferential for moderate-risk patients. High-risk patients, defined as those with high cardiovascular risk or adverse anatomic criteria such as severe venous stasis or lymphedema, pose a challenge. For patients with a poor life expectancy and an asymptomatic popliteal artery aneurysm, conservative management is preferred. If treatment of a popliteal artery aneurysm is indicated for such patients because endovascular treatment is less taxing with limited postsurgical complications, endovascular popliteal artery aneurysm repair (EPAR) is preferred. The option is offered regardless of the GSV's availability or the runoff vessels' quality. Recent literature review suggests that younger age, the availability of single-segment GSV, challenged runoff vessels, and lower surgical risk favor the choice of OPAR.[13](A1)
Special Considerations
In patients with connective tissue disorders, a lack of consensus is apparent on whether an open or endovascular approach is better for repairing a popliteal aneurysm. Endovascular interventions are relatively contraindicated because of the risk of damaging an inherently weak artery [14] and subsequent aneurysmal degeneration.[15] However, most reports using the endovascular approach have suggested caution with promising results.[16] The best conduit for open reconstruction is unknown; synthetic grafts have inferior long-term patency rates with concerns that vein grafts may lead to aneurysms.[14](B2)
Differential Diagnosis
The entities that should be considered in the differential diagnosis include Baker cyst, lymph node, varicosity, and cystic adventitial disease.
Complications
Limb loss is considered a major complication.
Pearls and Other Issues
The differential diagnosis of popliteal fossa masses includes arterial and non-arterial pathologies and popliteal artery aneurysms. Rare popliteal artery pathology, most commonly located behind the knee, consists of cystic adventitial disease and popliteal entrapment syndrome. Both conditions usually present with chronic symptoms of claudication. However, the most common cause of a popliteal fossa mass is the Baker cyst, which is a benign swelling of the semimembranosus or, more rarely, some other synovial bursa found behind the knee joint. Orthopedic causes include prepatellar bursitis and meniscal cysts.
Enhancing Healthcare Team Outcomes
Popliteal artery aneurysm is usually managed by an interprofessional team of healthcare professionals, including a vascular surgeon, an interventional radiologist, an endocrinologist, an internist, and a critical care specialist. When elective management of these aneurysms yields positive results, patients who present with a rupture have a greater risk of losing their limbs. Given the high risk of losing a limb following the rupture of a popliteal artery aneurysm, patient education is vital.
The nurse plays a vital role in monitoring and educating patients with a popliteal artery aneurysm. The patient must understand that when they receive a diagnosis of an aneurysm, they should follow up with a vascular surgeon and undergo elective surgery or have an endovascular procedure. More importantly, the patient must stop smoking, manage high blood pressure, and control blood sugars; these are areas where the clinician can enlist the assistance of pharmacists. Finally, examining the patient for a popliteal artery aneurysm in the contralateral leg and abdomen is important. All patients with a pulsatile mass behind the knee should be referred to a radiologist for an ultrasound.[17][18][19] An interprofessional approach to diagnosis and management yields superior outcomes and reduces morbidity.
The prognosis is good for patients with the popliteal artery aneurysm repaired electively—surgery and endovascular procedure outcomes are similar in the short term. However, the long-term outcome of an endovascular procedure on the popliteal artery aneurysm remains unknown. In patients who present with a rupture of a popliteal artery aneurysm, the outcome is usually poor. Limb loss is common. The amputations may be above or below the knee. The only way to reduce these poor outcomes is by examining pulses in all patients on the initial exam.[20][21][22]
Media
(Click Image to Enlarge)
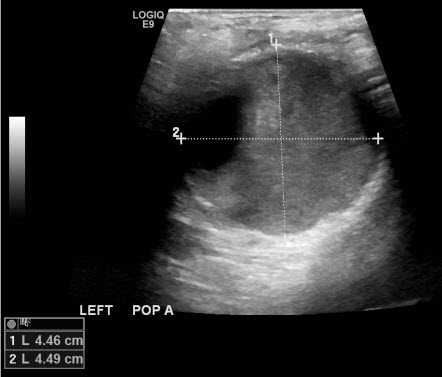
Ultrasound of Left Popliteal Artery Aneurysm. Ultrasound imaging visualizes a left popliteal artery aneurysm.
Contributed by P Shaw, MD
(Click Image to Enlarge)
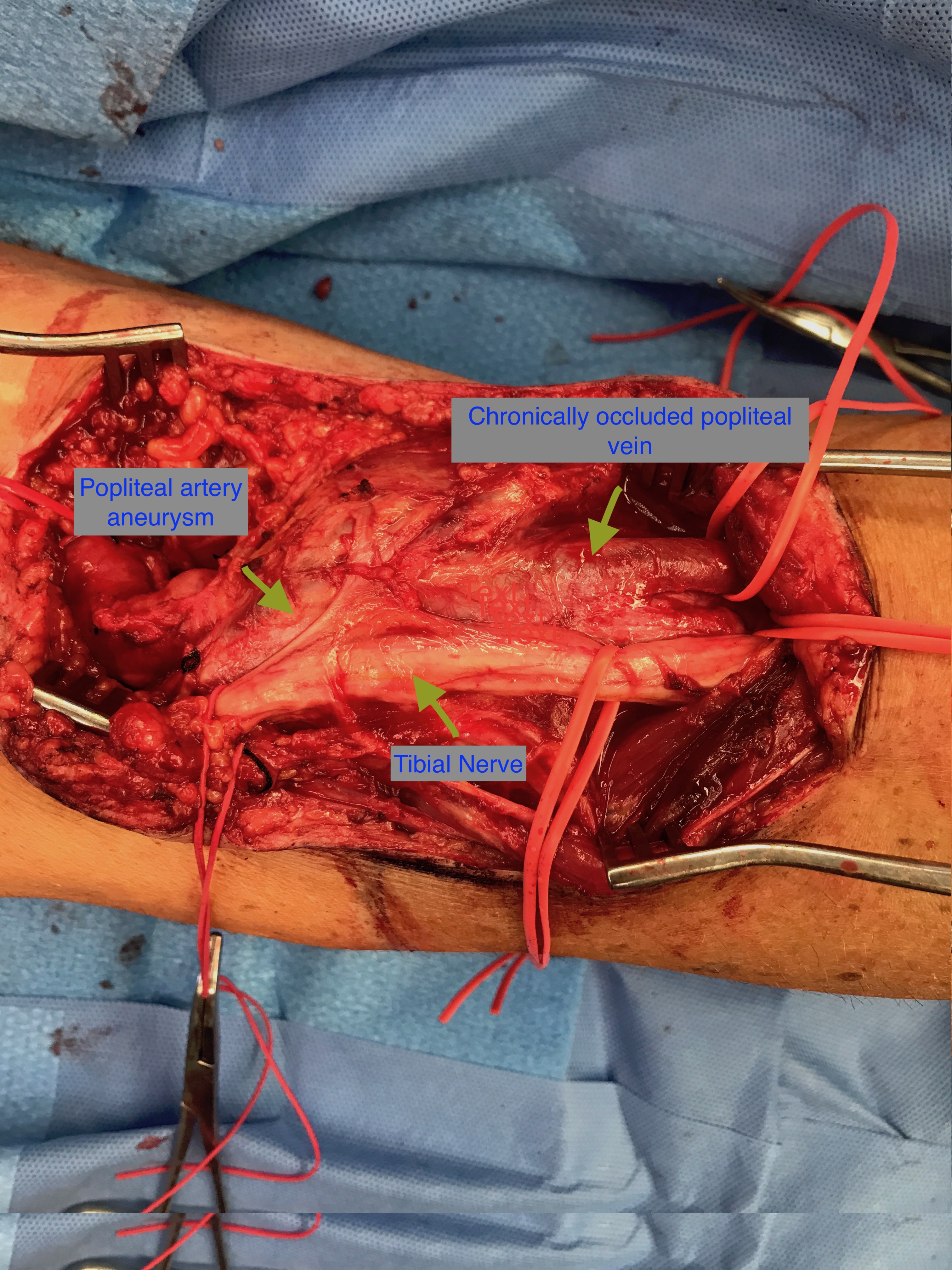
Intraoperative Popliteal Artery Aneurysm Repair. Posterior approach to popliteal artery aneurysm repair visualized intraoperatively.
Contributed by P Shaw, MD
(Click Image to Enlarge)

Popliteal Artery Aneurysm Visualized on Magnetic Resonance Angiography. Magnetic resonance angiography visualizes a popliteal artery aneurysm.
Contributed by S Bhimji, MD
References
Shiwani H, Baxter P, Taylor E, Bailey MA, Scott DJA. Modelling the growth of popliteal artery aneurysms. The British journal of surgery. 2018 Dec:105(13):1749-1752. doi: 10.1002/bjs.10955. Epub 2018 Aug 23 [PubMed PMID: 30136713]
Cecenarro RR, Allende JN, Barreras Molinelli L, Antueno FJ, Gramática L. [Popliteal Artery Aneurysms: Literature Review and presentation of case.]. Revista de la Facultad de Ciencias Medicas (Cordoba, Argentina). 2018 Mar 29:75(1):41-45. doi: 10.31053/1853.0605.v75.n1.16097. Epub 2018 Mar 29 [PubMed PMID: 30130484]
Level 3 (low-level) evidenceCervin A, Ravn H, Björck M. Ruptured popliteal artery aneurysm. The British journal of surgery. 2018 Dec:105(13):1753-1758. doi: 10.1002/bjs.10953. Epub 2018 Jul 24 [PubMed PMID: 30043540]
Mikhaylov IP, Lavrenov VN, Isaev GA, Kokov LS, Trofimova EY. [Ruptures of popliteal artery aneurysms]. Khirurgiia. 2018:(4):57-62. doi: 10.17116/hirurgia2018457-62. Epub [PubMed PMID: 29697685]
Fioranelli A, Carpentieri EA, Wolosker N, Castelli V Jr, Caffaro RA. Rupture of Thrombosed Popliteal Aneurysm: A Case Report. Annals of vascular surgery. 2018 Aug:51():324.e7-324.e10. doi: 10.1016/j.avsg.2017.12.024. Epub 2018 Mar 5 [PubMed PMID: 29518513]
Level 3 (low-level) evidenceGolchehr B, Zeebregts CJ, Reijnen MMPJ, Tielliu IFJ. Long-term outcome of endovascular popliteal artery aneurysm repair. Journal of vascular surgery. 2018 Jun:67(6):1797-1804. doi: 10.1016/j.jvs.2017.09.040. Epub 2017 Dec 29 [PubMed PMID: 29291906]
Cousins RS, Dexter DJ, Ahanchi SS, Cain BC, Powell OM, Ongstad SB, Parikh NM, Panneton JM. Determining patient risk factors associated with accelerated growth of popliteal artery aneurysms. Journal of vascular surgery. 2018 Mar:67(3):838-847. doi: 10.1016/j.jvs.2017.07.117. Epub 2017 Dec 22 [PubMed PMID: 29276109]
Ravn H, Pansell-Fawcett K, Björck M. Popliteal Artery Aneurysm in Women. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2017 Dec:54(6):738-743. doi: 10.1016/j.ejvs.2017.10.001. Epub 2017 Nov 7 [PubMed PMID: 29126647]
Kim SM, Jung IM. Successful Endovascular Treatment of a Ruptured Popliteal Artery Aneurysm in a Patient with Behcet Disease. Annals of vascular surgery. 2018 Nov:53():274.e1-274.e5. doi: 10.1016/j.avsg.2018.05.076. Epub 2018 Aug 6 [PubMed PMID: 30092437]
Ucci A, Curci R, Azzarone M, Bianchini Massoni C, Bozzani A, Marcato C, Marone EM, Perini P, Tecchio T, Freyrie A, Argenteri A. Early and mid-term results in the endovascular treatment of popliteal aneurysms with the multilayer flow modulator. Vascular. 2018 Oct:26(5):556-563. doi: 10.1177/1708538118771258. Epub 2018 Apr 17 [PubMed PMID: 29665749]
Sousa RS, Oliveira-Pinto J, Mansilha A. Endovascular versus open repair for popliteal aneurysm: a review on limb salvage and reintervention rates. International angiology : a journal of the International Union of Angiology. 2020 Oct:39(5):381-389. doi: 10.23736/S0392-9590.20.04387-4. Epub 2020 Apr 29 [PubMed PMID: 32348102]
Tian Y, Yuan B, Huang Z, Zhang N. A Comparison of Endovascular Versus Open Repair of Popliteal Artery Aneurysms: An Updated Meta-Analysis. Vascular and endovascular surgery. 2020 May:54(4):355-361. doi: 10.1177/1538574420908091. Epub 2020 Mar 3 [PubMed PMID: 32122277]
Level 1 (high-level) evidenceFarber A, Angle N, Avgerinos E, Dubois L, Eslami M, Geraghty P, Haurani M, Jim J, Ketteler E, Pulli R, Siracuse JJ, Murad MH. The Society for Vascular Surgery clinical practice guidelines on popliteal artery aneurysms. Journal of vascular surgery. 2022 Jan:75(1S):109S-120S. doi: 10.1016/j.jvs.2021.04.040. Epub 2021 May 20 [PubMed PMID: 34023430]
Level 1 (high-level) evidencePeng KX, Davila VJ, Fowl RJ. Successful repair of a popliteal aneurysm with saphenous vein graft in a patient with Marfan syndrome. Journal of vascular surgery cases and innovative techniques. 2019 Dec:5(4):393-395. doi: 10.1016/j.jvscit.2018.08.008. Epub 2019 Sep 17 [PubMed PMID: 31660457]
Level 3 (low-level) evidenceWang S, Kernodle A, Hicks CW, Black JH 3rd. Endovascular repair of tortuous recurrent femoral-popliteal aneurysm in a patient with Loeys-Dietz syndrome. Journal of vascular surgery cases and innovative techniques. 2018 Jun:4(2):156-159. doi: 10.1016/j.jvscit.2018.03.001. Epub 2018 Apr 30 [PubMed PMID: 29942909]
Level 3 (low-level) evidenceWaterman AL, Feezor RJ, Lee WA, Hess PJ, Beaver TM, Martin TD, Huber TS, Beck AW. Endovascular treatment of acute and chronic aortic pathology in patients with Marfan syndrome. Journal of vascular surgery. 2012 May:55(5):1234-40; disucssion 1240-1. doi: 10.1016/j.jvs.2011.11.089. Epub 2012 Apr 1 [PubMed PMID: 22465552]
Level 2 (mid-level) evidenceKaufman RL. Popliteal aneurysm as a cause of leg pain in a geriatric patient. Journal of manipulative and physiological therapeutics. 2004 Jul-Aug:27(6):e9 [PubMed PMID: 15319769]
Level 3 (low-level) evidenceFargion A, Masciello F, Pratesi G, Giacomelli E, Dorigo W, Pratesi C. Endovascular Treatment with Primary Stenting of Acutely Thrombosed Popliteal Artery Aneurysms. Annals of vascular surgery. 2017 Oct:44():421.e5-421.e8. doi: 10.1016/j.avsg.2017.04.027. Epub 2017 May 5 [PubMed PMID: 28483627]
Lee TL, Bokovoy J. Understanding discharge instructions after vascular surgery: an observational study. Journal of vascular nursing : official publication of the Society for Peripheral Vascular Nursing. 2005 Mar:23(1):25-9 [PubMed PMID: 15741962]
Level 2 (mid-level) evidenceSalzler GG, Long B, Avgerinos ED, Chaer RA, Leers S, Hager E, Makaroun MS, Eslami MH. Contemporary Results of Surgical Management of Peripheral Mycotic Aneurysms. Annals of vascular surgery. 2018 Nov:53():86-91. doi: 10.1016/j.avsg.2018.04.019. Epub 2018 Jun 8 [PubMed PMID: 29886217]
Wrede A, Wiberg F, Acosta S. Increasing the Elective Endovascular to Open Repair Ratio of Popliteal Artery Aneurysm. Vascular and endovascular surgery. 2018 Feb:52(2):115-123. doi: 10.1177/1538574417742762. Epub 2017 Dec 4 [PubMed PMID: 29202650]
Leake AE, Segal MA, Chaer RA, Eslami MH, Al-Khoury G, Makaroun MS, Avgerinos ED. Meta-analysis of open and endovascular repair of popliteal artery aneurysms. Journal of vascular surgery. 2017 Jan:65(1):246-256.e2. doi: 10.1016/j.jvs.2016.09.029. Epub [PubMed PMID: 28010863]
Level 1 (high-level) evidence