Introduction
Thoracic empyema, defined by the presence of frank purulent exudate in the pleural space, is an infectious and life-threatening condition with a long history (see Image. Chronic Empyema, Computed Tomography Scan). First recognized by Hippocrates and historically associated with high mortality rates, empyema presents a complex clinical challenge.[1] Stemming from multifactorial etiologies, empyema progresses through distinct stages that clinicians must recognize for effective management.[2] Prompt diagnosis and intervention are crucial for improving patient outcomes, as treatment hinges on integrating medical and surgical strategies to eradicate the infection and facilitate lung reexpansion.
Pleural infections, including empyema and complicated parapneumonic effusion, pose a serious health risk, impacting approximately 80,000 patients annually in the United States (US) and the United Kingdom (UK).[3] Despite diagnostic and therapeutic advancements, these infections carry substantial mortality, with 30-day mortality rates reaching up to 10.5% and exceeding 19% at 1 year. Furthermore, more than half of patients with pneumonia will develop parapneumonic effusions, resulting in increased morbidity across all patient groups, from those with simple effusions to those with advanced empyema. Beyond mortality, these infections impose significant morbidity, as patients often experience prolonged hospital stays—averaging 19 days, according to recent reviews—and frequently present with multiple comorbid conditions.[4]
Economic costs associated with thoracic empyema are substantial, with annual expenditures in the US estimated at $500 million. This financial burden is fueled by the need for pharmacologic and procedural interventions, including pleural drainage, increasing utilization of intrapleural enzyme therapy with tissue plasminogen activator and deoxyribonuclease, and surgical procedures.[4] Recent data from Mummadi et al reveal a rise in empyema hospitalizations in the US from 2007 to 2016, with in-hospital mortality ranging from 5.2% to 6.2% and an average cost per hospitalization of $38,591.[5] Together, these factors underscore the need for refined diagnostic and treatment strategies to improve patient outcomes and alleviate the economic impact of thoracic empyema.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Empyema thoracis, meaning “pus in the chest” in Greek, occurs when infections from various parts of the body spread to the pleural space. The most common cause of empyema is bacterial pneumonia and its resulting parapneumonic effusion. Approximately 20% to 40% of patients admitted for pneumonia experience associated parapneumonic effusion. Among these, 5% to 10% will develop empyema; 30% of these patients require surgical drainage, and the mortality rate for these patients is 15%. Less frequently, empyema can arise from conditions such as bronchogenic carcinoma, esophageal rupture, blunt or penetrating chest trauma, infectious mediastinitis spreading to the pleurae, infection crossing the diaphragm from abdominal sources, spinal infections, or postsurgical complications.
The development of pleural space infections likely involves increased permeability of the mesothelial layer of the inflamed pleurae, allowing bacteria to invade the typically sterile space. Interestingly, up to 56% of community-acquired and 73% of hospital-acquired pleural space infections demonstrate no radiographic signs of pneumonia. This, along with differing microbial profiles between pneumonia and pleural infections, suggests that hematogenous spread might be a factor in some patients with empyema. Despite these varied mechanisms, the most common etiologic pathway involves the aspiration of organisms from the oropharynx, leading to pneumonia in the dependent lobes, which, if left untreated, can progress to parapneumonic effusion and, ultimately, empyema.[6]
Risk Factors
Many pleural space infections present as complications from community- or hospital-acquired pneumonia.[1] Other causes include penetrating chest trauma, thoracic surgery, esophageal rupture, pulmonary tuberculosis, lung abscess, bronchiectasis, subphrenic abscess, and osteomyelitis of ribs. Independent risk factors for empyema development include:
- Younger than 60
- Poor oral hygiene
- Disorders with a predisposition to aspiration (seizure, alcohol use disorder, central nervous system disease)
- Intravenous drug misuse
- Diabetes
- Cardiovascular disease
- Liver cirrhosis
- Other immunocompromised states (eg, human immunodeficiency virus infection or malignancy)[7][8][9]
The results of a prospective observational study found 6 associated risk factors in patients admitted with community-acquired pneumonia who subsequently developed empyema, including albumin less than 30 g/L, sodium below 130 mmol/L, platelet count greater than 400 x 109, C-reactive protein over 100 mg/L, and a history of alcohol use or intravenous drug use disorders.[10]
Bacteriology
Aerobic Staphylococcus and Streptococcus species and gram-negative bacteria, including Escherichia coli, Haemophilus influenzae, and Klebsiella pneumoniae, are the predominant microorganisms in community-acquired empyema.[11] However, recent literature suggests that anaerobes and staphylococcal species have replaced Streptococcus pneumoniae as the primary pathogen in surgically treated empyemas. Also, anaerobic isolates were found to have a higher incidence of community-acquired pneumonia than previously reported.[12][13] Methicillin-resistant Staphylococcus aureus and gram-negative organisms, including Pseudomonas and Enterobacteriaceae, are pathogens commonly seen in hospital-acquired empyema. Anaerobes are slow-growing organisms that notoriously yield negative culture media. Therefore, broad-spectrum antibiotic coverage with anaerobic coverage is warranted.
The microbiology of pleural infections plays a critical role in patient outcomes, with survival rates varying with the causative organisms. For instance, patients with streptococcal infections had an 83% survival rate, similar to the 87% in cases where no organism could be identified. This suggests that many culture-negative pleural infections may be streptococcal, with antibiotics quickly reducing bacterial load, leading to negative cultures. Anaerobic infections also had relatively favorable outcomes, with an 80% survival rate. In contrast, diseases caused by Staphylococcus, Enterobacteriaceae, and mixed aerobic organisms were associated with much higher mortality, with only 55% of patients surviving at 1 year.[13]
Fungal empyema is a clinical entity that is rare but carries a high mortality. One single-center retrospective analysis isolated Candida and Aspergillus species from 65 critically ill patients with variable comorbidities, including malignancy. Most of these cases were nosocomial infections or had concomitant fungemia.[14]
Epidemiology
In the US, the incidence of parapneumonic empyema is estimated to be 6 cases per 100,000. In-hospital mortality in patients older than 65 is approximately 16.1%.[15] Between 2005 and 2014, 150,469 patients aged 18 and older were admitted to US hospitals for pleural infections. The average age of these patients was 58.3 years; 68% of patients were men. White patients accounted for 79.3% of the admissions, and 4.4% of patients presented with either severe sepsis (a classification that has since been replaced by the Third International Consensus Definitions for Sepsis and Septic Shock) or septic shock.[16]
Pathophysiology
Approximately 60 years ago, the American Thoracic Society first described the evolution of empyema as a continuous process subdivided into 3 distinct but continuous stages or phases: exudative, fibrinopurulent and loculated, and chronic organizational. Specific pleural fluid characteristics, radiographic findings, and corresponding treatments distinguish these stages of parapneumonic effusion, pleural infection, and empyema.[6][17]
Exudative Stage
The initial phase of empyema formation is an exudative effusion, where fluid rapidly accumulates in the pleural space. During this phase, pleural fluid is typically culture and Gram stain negative, with glucose levels exceeding 60 mg/dL and lactate dehydrogenase (LDH) levels less than 3 times the upper limit of normal for serum. Proinflammatory mediators like tumor necrosis factor-alpha (TNF-α), interleukin 6 (IL-6), and IL-8 are believed to be vital in driving the inflammatory response at this stage.[6]
Fibrinopurulent and Loculated Stage
The second phase is the fibrinopurulent stage, which follows the initial exudative phase and typically results if antibiotic treatment is inadequate or delayed. This phase is characterized by bacterial invasion into the pleural space. In this stage, the pleural fluid will generally have a glucose level below 60 mg/mL with a pH below 7.20 and a pleural fluid LDH greater than 3 times the upper limit of normal for serum. Increased plasminogen-activator inhibitors and TNF-α lead to fibrin deposition, which forms septations and loculations. Within these loculations, walled-off bacteria increase neutrophil phagocytic activity, a corresponding increase in LDH, and increased production of lactic acid and glucose consumption; this explains the changes observed in pleural fluid analysis.[6]
Chronic Organizational Stage
The final stage, known as the organizing phase, is marked by the growth of fibroblasts into the visceral and parietal pleurae. This is accompanied by the deposition of a collagen-rich fibrin matrix within the pleural space, resulting in pleural thickening. This phase often leads to developing an inelastic visceral pleural peel, which can cause lung entrapment. The proliferation of fibroblasts is believed to be driven by the release of transforming growth factor-beta and platelet-derived growth factor.
History and Physical
Thoracic empyema has a complex presentation that varies based on the stage of the disease. Obtaining a thorough medical history and performing a comprehensive physical examination is vital for prompt diagnosis and management, especially given the condition’s high morbidity and mortality rates.
History
Patients with thoracic empyema often present with symptoms that mimic other respiratory or infectious conditions, particularly pneumonia. A typical history may include preceding or concurrent pulmonary infections, with pleural infection occurring as a complication of bacterial pneumonia in about 60% of cases. Other risk factors include recent thoracic surgery, trauma, esophageal perforation, or immunocompromise. Symptoms tend to evolve as the empyema progresses through its stages:
- Exudative stage: Early symptoms are similar to pneumonia, with common complaints of fever, cough, and pleuritic chest pain. Dyspnea may be mild at this stage, and chest discomfort is often described as a deep, dull pain.
- Fibrinopurulent stage: As the infection progresses, patients often report worsening chest pain, increased dyspnea, and a productive cough with purulent sputum. Fever may become more pronounced, and constitutional symptoms like malaise, fatigue, and night sweats are often present. This stage is marked by the accumulation of fibrin and pus, leading to loculated fluid pockets within the pleural space.
- Organizing stage: In chronic or untreated empyema, fibrous septa form within the pleural cavity, encasing the lung and restricting its expansion. At this stage, symptoms are more persistent and may include marked weight loss, cachexia, and chronic pain. Chronic empyema may lead to further respiratory compromise, with severe dyspnea and decreased exercise tolerance.
Physical Examination
The physical examination findings in thoracic empyema are variable and depend on the amount of pleural fluid, the degree of lung compression, and the stage of the disease.
- Vital signs: Fever is common, although its severity varies. Tachycardia and tachypnea may indicate a more severe infection or systemic inflammatory response. Hypoxemia may present in patients with underlying respiratory compromise, particularly in advanced empyema.
- Inspection: Patients may appear acutely ill, especially in the fibrinopurulent or organizing stages. Signs of respiratory distress or accessory muscle use may indicate severe disease. In chronic cases, weight loss and cachexia may be evident.
- Palpation and percussion: Dullness to percussion over the affected hemithorax is a hallmark of pleural effusion, and in empyema, the dullness is often more pronounced and localized. Tactile fremitus is typically decreased or absent over areas with large fluid collections.
- Auscultation: Breath sounds are diminished or absent over fluid accumulation, especially in the fibrinopurulent and organizing stages. In some cases, crackles or bronchial breath sounds may be heard at the periphery of the empyema cavity, suggesting surrounding lung consolidation. Friction rubs, though uncommon, may be audible, especially in the earlier stages.
Evaluation
Imaging
Chest imaging is a cornerstone of empyema diagnosis and management as it provides critical information about pleural infections' presence, extent, and nature. While advancements in imaging modalities have enhanced diagnostic accuracy, plain radiography remains a valuable initial screening tool, particularly in patients with pneumonia. A unilateral, markedly asymmetric pleural effusion with costophrenic angle blunting is typically seen, and smaller effusions may be better visualized using a lateral view. Decubitus radiographs can further assess for layering and quantify fluid volume. However, the specificity of chest radiography is limited, particularly in the early stages of empyema, necessitating further imaging. However, ultrasonography and computed tomography (CT) have greater sensitivity for fluid detection and provide additional information for determining the extent and nature of the pleural infection.[18]
Thoracic ultrasonography can differentiate simple effusions from complex ones, detect septations and loculations characteristic of empyema, and guide safe thoracentesis for fluid sampling. In a case series, ultrasonography demonstrated superior sensitivity to plain radiography for diagnosing pleural effusions, reinforcing its role as a preferred modality in suspected empyema cases.[19]
CT with intravenous contrast remains the most definitive imaging study for empyema and provides detailed visualization of pleural thickening, loculations, and enhancement of the pleurae, hallmark features of empyema. The “split pleura” sign, characterized by thickened visceral and parietal pleurae separated by fluid greater than 30 mm, is a highly specific finding suggesting complicated parapneumonic effusion requiring drainage.[20] CT is particularly useful for distinguishing empyema from lung abscess, which can present with overlapping clinical and radiographic findings but requires distinct management approaches. Additionally, CT helps evaluate the extent of disease, the involvement of adjacent structures, and the appropriateness of drainage procedures.
Thoracentesis
Diagnostic fluid sampling via thoracentesis is essential in evaluating pleural effusions associated with pneumonia, recent chest trauma, surgery, or ongoing sepsis, particularly when effusion depth exceeds 2 cm on lateral decubitus films or CT.[18][19] Frank pus in the pleural space necessitates surgical drainage. However, in cases where the fluid is turbid but not purulent, a pleural fluid pH of less than 7.2, measured using a blood gas analyzer, indicates the need for invasive drainage.[20] Additional biochemical and microbiological analyses provide critical diagnostic information.
Pleural fluid analysis begins with assessing appearance, as grossly purulent fluid strongly suggests empyema. Biochemical markers are also crucial, with empyema typically characterized by low pH (<7.2), low glucose (<60 mg/dL), and elevated LDH (>1000 IU/L), reflecting the acidic, metabolically active environment of infection. A leukocytosis with neutrophilic predominance indicates acute inflammation, further supporting the diagnosis.
Microbiological evaluation includes Gram staining for immediate organism identification and pleural fluid cultures for definitive diagnosis. Pathogens frequently associated with empyema include Streptococcus species, Staphylococcus aureus, and anaerobes. Pleural fluid culture yield can be significantly improved by injecting pleural fluid into blood culture bottles immediately after aspiration.[21] These cultures are vital for guiding targeted antimicrobial therapy and determining the need for additional interventions, such as mechanical drainage or surgery.
In certain cases, additional testing may be necessary. For example, pleural fluid should be analyzed in patients with suspected tuberculosis using acid-fast bacilli stain, culture, and polymerase chain reaction testing, especially in high-risk populations or regions with a high tuberculosis prevalence. This comprehensive diagnostic approach ensures accurate identification of the underlying cause and informs the optimal therapeutic strategy.
Blood Cultures
Blood cultures are necessary for any patient with empyema. Although generally nondiagnostic, they can help identify causative pathogens and bacteremia if the results are positive.
Advanced Diagnostic Techniques
Advanced diagnostic techniques may be necessary when initial fluid analysis and imaging fail to provide a definitive diagnosis. Pleural biopsy is particularly valuable in suspected tuberculosis or malignancy cases when pleural fluid studies are nondiagnostic. Thoracoscopic biopsy offers the advantage of direct visualization of the pleurae, allowing for targeted tissue sampling for histopathology and culture. Although not routinely used to evaluate empyema, bronchoscopy can be helpful in specific scenarios and is particularly useful in identifying bronchopleural fistulas, endobronchial obstructions, or other intrathoracic pathologies that may contribute to the infection.
Treatment / Management
The treatment and management of thoracic empyema involve a combination of medical and surgical interventions aimed at eradicating infection, achieving adequate drainage of the pleural space, and restoring lung function. Early and aggressive management is critical to improving outcomes and minimizing complications. In 2000, the American College of Chest Clinicians published clinical practice guidelines emphasizing the importance of pleural space anatomy, fluid bacteriology, and fluid chemistry in determining the risk of poor outcomes in empyema.
Categories 1 and 2 represent free-flowing exudative-stage effusions with the lowest risk for adverse outcomes. Category 3 refers to complicated effusions in the fibrinopurulent stage, which may be larger, loculated, or free-flowing, with a moderate risk of poor outcomes.[22] Empyema, categorized as stage 4, carries the highest risk of adverse outcomes. Management aims to eradicate infection through antimicrobials and achieve adequate pleural drainage using tube thoracostomy, with or without intrapleural therapies, video-assisted thoracoscopic surgery (VATS), or open thoracotomy with decortication.(A1)
Data from 2005 to 2014 reveal trends in empyema management, revealing that 76.3% of patients underwent interventions such as tube thoracostomy, VATS, or thoracotomy. Tube thoracostomy as a first-line treatment increased from 21.7% to 29.6%, while VATS rose from 11.2% to 14.9%, reflecting its growing acceptance. Thoracotomy decreased from 22.6% to 18.9%, likely due to the less invasive nature of VATS. Notably, 64.9% of patients treated with initial tube thoracostomy did not require further surgical intervention, underscoring its effectiveness in many cases.[16]
Medical Management
Antimicrobials
Empiric broad-spectrum antibiotics are necessary for most patients with suspected or confirmed empyema. Initiation of therapy should not delay diagnostic procedures. Antimicrobials should be tailored to target pathogens based on geographic epidemiology, antibiotic resistance patterns, mode of acquisition (aspiration, trauma), and whether the affected patient presents from a community versus a healthcare setting.
- Community-acquired empyema: The antibiotic regimen should target common pathogens of the oropharynx, including aerobic Staphylococcus and Streptococcus species and anaerobes. Appropriate antibiotics include third-generation cephalosporins, metronidazole, or a beta-lactam/beta-lactamase inhibitor combination.[23]
- Hospital-acquired empyema: Antimicrobial therapy should cover methicillin-resistant S aureus, Pseudomonas, and typical organisms and anaerobes. Reasonable options include vancomycin plus metronidazole and an antipseudomonal cephalosporin. Vancomycin plus piperacillin/tazobactam, a broad-spectrum beta-lactam/beta-lactamase inhibitor, provides both anaerobic and antipseudomonal activity. (B3)
Caution should be taken with aminoglycosides due to poor pleural penetration; this antimicrobial class is not recommended for treating empyema.[24] The duration of antibiotics is generally recommended to be 2 to 6 weeks (intravenous followed by oral), depending on the degree of infection and clinical response to therapy.[25][26]
Surgical and Procedural Interventions
Tube thoracostomy and intrapleural therapies
Chest tube placement under radiologic guidance remains the cornerstone nonsurgical intervention for empyema. Optimal thoracostomy tube size has been a controversial topic amongst chest physicians. Traditionally, large-bore (>22F) tubes were preferred for draining viscous purulent fluid; recent evidence suggests no significant advantage over small-bore (<20F) tubes regarding mortality or surgical delays.[27][28] Clinical success depends more on accurate placement, as malpositioning is a common cause of treatment failure. Radiographic confirmation of tube location within 24 hours is essential. Typically, chest tubes are removed when drainage falls below 50 mL in 24 hours or when imaging confirms lung reexpansion.(A1)
The use of adjunctive intrapleural therapies has varied outcomes. Isolated fibrinolytic agents such as streptokinase, urokinase, or tissue-type plasminogen activator (tPA) have demonstrated limited benefit. However, combination therapy with tPA and deoxyribonuclease (DNase) significantly improves fluid drainage, reduces surgical referrals, and shortens hospital stays without impacting mortality. Emerging approaches, such as saline lavage, have shown promise. The Pleural Irrigation Trial's results showed a radiographic improvement after 3 days in empyema patients receiving saline irrigation via tube thoracostomy vs standard of care.[29] Results from a smaller retrospective study comparing saline flushes plus urokinase versus saline alone found decreased chest tube duration and use of fibrinolytic. Although researchers noted no mortality benefit, more extensive randomized studies are needed to confirm the benefits of this inexpensive, well-tolerated therapy.[28] (A1)
Intrapleural enzyme therapy (IET) is an adjunctive approach, particularly for complicated parapneumonic effusions and empyema. This therapy involves administering fibrinolytic agents, such as tPA, and enzymatic agents, like DNase, directly into the pleural space. tPA dissolves fibrin clots, reducing septations, while DNase targets extracellular deoxyribonucleic acid in pus, lowering fluid viscosity. The combination enhances fluid drainage, improves pleural clearance, and minimizes the need for surgical intervention.[29](A1)
Since the publication of the results from the Multicenter Intrapleural Sepsis Trial study, IET has significantly transformed the medical management of pleural infections. Although the MIST-2 trial had a limited number of patients in the IET group (n= 52) and primarily measured radiographic clearance, subsequent reports involving over 600 patients have demonstrated reduced surgical intervention rates and shorter hospital stays. Additionally, a multicenter retrospective study of 1850 patients treated with IET reported a low incidence of bleeding complications (4.2%) and no significant adverse events.[30](A1)
IET is particularly indicated for patients with loculated effusions unresponsive to tube thoracostomy, those at high surgical risk, or as a bridge to surgery for preoperative optimization. The standard regimen includes 10 mg of tPA and 5 mg of DNase in sterile saline, instilled via a chest tube every 12 hours for 3 days, with a 1-hour dwell time per dose. While generally safe, IET can cause fever, pain, and rarely systemic bleeding, requiring careful patient selection, especially in those with coagulopathies. Though not universally effective in advanced cases with dense fibrous organization, IET offers a minimally invasive option that enhances drainage, reduces surgical interventions, and optimizes patient outcomes when integrated into a multidisciplinary care strategy.
VATS
Surgical consultation should be a consideration when drainage via tube thoracostomy fails or for patients with multiloculated empyema. VATS is a minimally invasive surgical technique that allows for direct visualization and evacuation of the infected pleural space. Although the appropriate timing of VATS is unclear, it has been documented to have superior outcomes when compared to tube thoracostomy for the treatment of advanced-stage empyema in terms of postoperative morbidity, complications, and length of hospital stay.[31](A1)
Open thoracostomy and decortication
Persistent empyema refractory to standard therapies, including VATS, should be considered for open window thoracostomy with prolonged chest tube drainage or decortication. Acute empyema can have long-term consequences despite adequate therapeutic interventions. Pleural scarring and fibrosis can lead to adhesions, decreased lung compliance, and a restrictive lung disease pattern. Decortication is an option for lung reexpansion if symptoms persist 6 months after empyema resolution.
Supportive care
Supportive care is crucial in managing thoracic empyema and promoting patient recovery. Nutritional support is essential for enhancing immune function and overall recovery, as patients with empyema often experience significant systemic inflammation and metabolic demands. Pulmonary rehabilitation, including breathing exercises and physiotherapy, is equally important to encourage lung expansion, prevent atelectasis, and restore respiratory function. Additionally, regular imaging and clinical evaluations are necessary to monitor the resolution of the infection and ensure proper lung re-expansion, enabling early detection and management of any complications or recurrence.
Collaborative approach
Effective management requires an interdisciplinary team of healthcare professionals involving pulmonologists, thoracic surgeons, infectious disease specialists, radiologists, and nursing staff. Coordination ensures timely diagnosis, proper drainage procedures, and individualized treatment plans. This collaborative effort minimizes morbidity, improves patient outcomes, and reduces healthcare costs.
Differential Diagnosis
The differential diagnosis of thoracic empyema includes several other causes of pleural effusion and thoracic infections and conditions that mimic empyema clinically and radiographically. Differentiating empyema from these conditions is essential to ensure appropriate treatment. Key considerations include:
- Uncomplicated parapneumonic effusion
- Complicated parapneumonic effusion
- Lung abscess
- Tuberculosis pleuritis
- Malignant pleural effusion
- Chylothorax
- Hemothorax
- Fungal pleural infection
- Autoimmune pleuritis (eg, rheumatoid arthritis, lupus)
- Heart failure-related effusion
- Pulmonary infarct
Prognosis
Empyema has a generally poor prognosis if not treated promptly and aggressively, as untreated or inadequately managed cases can lead to high morbidity and mortality. Although most patients recover, outcomes remain challenging, with approximately 20% requiring surgery and a 1-year mortality rate nearing 20%. Frail, older adults, and immunocompromised individuals have a 1.5-fold increase in adverse outcomes, highlighting the importance of early, individualized intervention for these vulnerable groups. The in-hospital mortality rate for empyema ranges from 5% to 15%, influenced by factors such as age, delayed diagnosis, advanced disease stage, and underlying health conditions.
Empyema risks recurrence and long-term complications, including chronic fibrothorax and restrictive lung disease, especially in cases of insufficient drainage or persistent infection. These chronic changes can impair lung function, reduce exercise tolerance, cause chronic cough, and decrease quality of life. The average hospital stay for empyema is approximately 19 days due to the need for prolonged drainage, antibiotics, and sometimes surgical intervention, with prolonged recovery impacting functional outcomes, especially in older individuals.
Results from a retrospective cohort analysis by Wilshire et al found no significant mortality advantage between initial surgery and fibrinolytic therapy but highlighted that initial surgical intervention was linked to shorter hospital stays, reduced duration of chest tube placement, and fewer subsequent treatments or readmissions.[32] These findings align with other studies' results, indicating that early surgical intervention may optimize outcomes by reducing treatment failure rates and minimizing healthcare resource utilization.
The economic impact of empyema is considerable, with an estimated treatment cost of $38,000 per case and annual US healthcare costs nearing $500 million. Costs are driven by extended hospitalizations, advanced pharmacologic interventions, and procedural requirements, emphasizing the need for timely diagnosis and management to reduce financial and healthcare burdens.
Complications
If untreated or inadequately managed, empyema can lead to serious complications affecting the respiratory system and overall patient health. These complications contribute to prolonged hospital stays, increased healthcare costs, and significant morbidity and mortality. Key complications associated with empyema include:
Pleural fibrosis and fibrothorax: Chronic empyema can lead to fibrosis of the pleural membranes, resulting in a condition known as fibrothorax, where the pleural space becomes thickened and scarred. This restricts lung expansion, causes restrictive lung disease, and results in persistent dyspnea, reduced exercise tolerance, and diminished quality of life. Fibrothorax may require surgical decortication to release the lung from the fibrous encasement.
Bronchopleural fistulae: A bronchopleural fistula, an abnormal connection between the bronchial tree and pleural space, can occur due to lung necrosis or after surgical intervention, particularly lobectomy or pneumonectomy. Bronchopleural fistulae can lead to persistent air leaks, pneumothorax, and impaired lung function, complicating the treatment and drainage of empyema. Bronchopleural fistulae increase the risk of severe, recurrent infection and are challenging to manage, often requiring surgical repair or prolonged chest tube placement.
Sepsis and septic shock: If empyema is not adequately contained, the infection can spread into the bloodstream, leading to sepsis, a life-threatening systemic response to infection. This complication significantly increases mortality and is particularly common in those who are immunocompromised, older, or frail. Sepsis due to empyema requires intensive care and aggressive antibiotic therapy, often alongside respiratory support and hemodynamic monitoring.
Respiratory failure: Empyema compromises lung function by compressing the underlying lung, impairing ventilation, and causing hypoxemia. If left untreated, this compression can progress to respiratory failure, particularly in patients with underlying pulmonary diseases like chronic obstructive pulmonary disease or asthma. In severe cases, patients may require mechanical ventilation, and the prognosis is generally poorer when empyema leads to respiratory decompensation.
Recurrent empyema: Inadequate drainage or incomplete resolution of infection may lead to recurrent empyema, which can occur weeks or even months after the initial episode. Recurrent empyema increases the risk of pleural thickening, longer hospital stays, and the need for more aggressive surgical interventions. This condition is often seen in cases where conservative management alone was insufficient or in patients with a history of pleural disease.
Empyema necessitans: In rare cases, empyema can erode through the chest wall, leading to an external draining sinus—a condition known as empyema necessitans.[33] This unusual complication typically occurs in patients with tuberculosis or chronic infections and can lead to chest wall deformity and severe scarring. Empyema necessitans often require surgical debridement and may necessitate prolonged antibiotic therapy.
Reduced quality of life and functional impairment: Chronic empyema is associated with long-term functional limitations and reduced quality of life, especially in patients who develop fibrothorax. Persistent dyspnea, chest pain, and fatigue are common, especially in patients who are older or those with preexisting lung disease. Patients may experience limited physical activity, dependence on supplemental oxygen, and chronic respiratory symptoms, which impact their daily lives.
Cardiovascular complications: The inflammation and infection associated with empyema can strain the cardiovascular system, especially in large effusions that compress the heart and great vessels. Patients may experience hemodynamic instability, including hypotension and tachycardia, which can be exacerbated by sepsis or a systemic inflammatory response. This strain is particularly dangerous for patients with preexisting cardiac conditions.
Deterrence and Patient Education
Deterrence and patient education are crucial in preventing thoracic empyema, which often results from untreated or poorly managed pneumonia and other pleural infections. Empowering patients and their families with knowledge about risk factors, early symptoms, and the importance of medical follow-up can significantly reduce the likelihood of empyema and its associated complications. Preventing underlying infections is a foundational step in empyema deterrence. Vaccination against common pathogens like S pneumoniae and influenza is essential, particularly for high-risk groups, including older adults, individuals with chronic lung disease, and those who are immunocompromised.
Patients should be educated to seek prompt treatment for respiratory infections, as untreated or inadequately treated infections increase the risk of complications, including empyema. Proper adherence to prescribed antibiotics is essential to prevent resistant or recurrent infections. Smoking cessation is also a vital preventive measure since smoking impairs lung function and increases the risk of respiratory infections, further raising the likelihood of empyema. Clinicians should offer resources and support to encourage smoking cessation and promote respiratory health.
Recognizing early symptoms of empyema is equally important. Patients should be aware of symptoms such as persistent fever, chest pain, and worsening cough after starting antibiotics for pneumonia. Unexplained dyspnea, pleuritic chest pain, and malaise may indicate a complication like a parapneumonic effusion or empyema. Those with chronic respiratory diseases or a history of pneumonia should be particularly vigilant in reporting new or worsening symptoms. Another critical patient education component is the importance of follow-up after pneumonia treatment. Regular follow-up visits help assess response to treatment and detect any signs of complications, even if symptoms seem to improve. Imaging, such as chest radiographs or ultrasounds, should be completed as recommended to ensure the resolution of infection.
Patient adherence to antibiotic therapy is essential to prevent empyema, as incomplete use of antibiotics can lead to recurrent or unresolved infection. Patients should be advised to complete their antibiotic course even if they start to feel better. Lifestyle modifications and comorbidity management are also key to reducing empyema risk, especially for those with conditions like diabetes or chronic obstructive pulmonary disease (COPD). Those with COPD, for example, may benefit from pulmonary rehabilitation and optimal inhaler use to reduce infection risk. General health measures such as maintaining good hydration, nutrition, and regular physical activity can bolster immune function and lower infection susceptibility.
Education on the potential complications of empyema, including chronic lung disease, respiratory failure, and high mortality, is vital to emphasize the importance of early intervention and adherence to treatment. Patients and caregivers who understand the serious nature of empyema are more likely to comply with medical advice and seek early hospital care if symptoms recur or worsen. In summary, comprehensive education on prevention, symptom recognition, treatment adherence, and follow-up care empowers patients to take an active role in their health, reducing the incidence and severity of empyema and improving overall outcomes.
Enhancing Healthcare Team Outcomes
Managing thoracic empyema is complex, requiring coordinated, multidisciplinary care to optimize patient outcomes. Physicians, advanced practitioners, nurses, pharmacists, and other healthcare professionals must work collaboratively to address empyema's medical and surgical challenges. The American Association for Thoracic Surgery, British Thoracic Society, and American College of Chest Physicians have developed evidence-based guidelines for diagnosis, antibiotic use, thoracentesis, tube thoracostomy, and surgical referral. These guidelines emphasize the early involvement of chest clinicians and thoracic surgeons in identifying surgical candidates, assessing risks, and managing complications.[34] They also support the involvement of infectious disease specialists in guiding antibiotic stewardship.[35]
Interprofessional collaboration further enhances care by leveraging the expertise of each team member. Clinicians oversee diagnosis, imaging, and procedural decisions, while nurses provide critical postsurgical care, monitor for complications, and educate patients on respiratory health and infection prevention. Pharmacists ensure appropriate antimicrobial therapy, manage drug interactions, and verify dosing. Regular communication through team meetings and comprehensive care plans facilitates smooth transitions between diagnostic, therapeutic, and surgical teams. Case managers coordinate postdischarge care to prevent readmissions. This cohesive approach, grounded in interprofessional teamwork, ensures patient-centered care, improved safety, reduced complications, and better overall outcomes for patients with thoracic empyema.
Media
(Click Image to Enlarge)
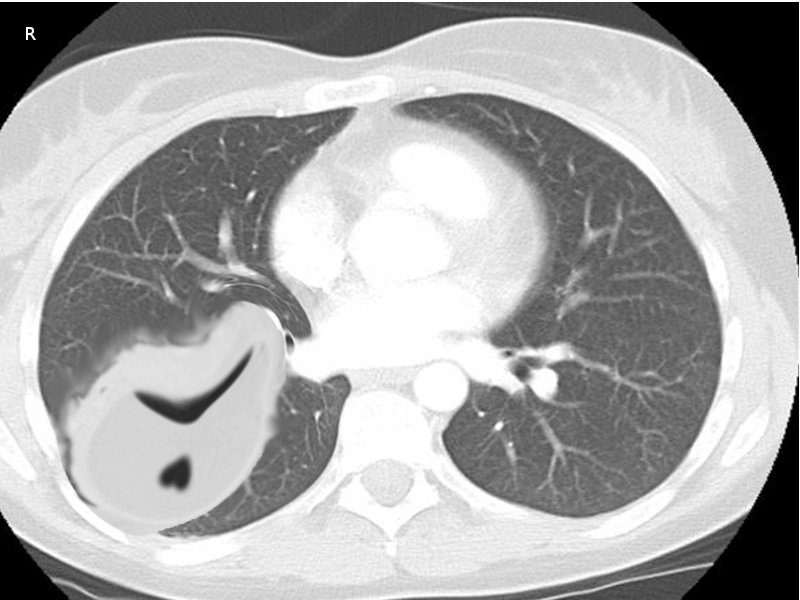
Chronic Empyema, Computed Tomography Scan. This image shows the characteristic frank purulent exudate in the pleural space seen in empyema, an infectious and life-threatening condition with a long history.
Contributed by O Chaigasame, MD
References
Ahmed AE, Yacoub TE. Empyema thoracis. Clinical medicine insights. Circulatory, respiratory and pulmonary medicine. 2010 Jun 17:4():1-8 [PubMed PMID: 21157522]
Reichert M, Hecker M, Witte B, Bodner J, Padberg W, Weigand MA, Hecker A. Stage-directed therapy of pleural empyema. Langenbeck's archives of surgery. 2017 Feb:402(1):15-26. doi: 10.1007/s00423-016-1498-9. Epub 2016 Nov 4 [PubMed PMID: 27815709]
Søgaard M, Nielsen RB, Nørgaard M, Kornum JB, Schønheyder HC, Thomsen RW. Incidence, length of stay, and prognosis of hospitalized patients with pleural empyema: a 15-year Danish nationwide cohort study. Chest. 2014 Jan:145(1):189-192. doi: 10.1378/chest.13-1912. Epub [PubMed PMID: 24394842]
Addala DN, Bedawi EO, Rahman NM. Parapneumonic Effusion and Empyema. Clinics in chest medicine. 2021 Dec:42(4):637-647. doi: 10.1016/j.ccm.2021.08.001. Epub [PubMed PMID: 34774171]
Foley SPF, Parrish JS. Pleural Space Infections. Life (Basel, Switzerland). 2023 Jan 29:13(2):. doi: 10.3390/life13020376. Epub 2023 Jan 29 [PubMed PMID: 36836732]
Hassan M, Patel S, Sadaka AS, Bedawi EO, Corcoran JP, Porcel JM. Recent Insights into the Management of Pleural Infection. International journal of general medicine. 2021:14():3415-3429. doi: 10.2147/IJGM.S292705. Epub 2021 Jul 14 [PubMed PMID: 34290522]
Petrusevska-Marinkovic S, Kondova-Topuzovska I, Milenkovic Z, Kondov G, Anastasovska A. Clinical, Laboratory and Radiographic Features of Patients with Pneumonia and Parapneumonic Effusions. Open access Macedonian journal of medical sciences. 2016 Sep 15:4(3):428-434 [PubMed PMID: 27703568]
Zablockis R, Petruskeviciene R, Nargela RV. [Causes and risk factors of pleural empyema and complicated parapneumonic pleural effusion]. Medicina (Kaunas, Lithuania). 2010:46(2):113-9 [PubMed PMID: 20440084]
Maskell NA, Batt S, Hedley EL, Davies CW, Gillespie SH, Davies RJ. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. American journal of respiratory and critical care medicine. 2006 Oct 1:174(7):817-23 [PubMed PMID: 16840746]
Chalmers JD, Singanayagam A, Murray MP, Scally C, Fawzi A, Hill AT. Risk factors for complicated parapneumonic effusion and empyema on presentation to hospital with community-acquired pneumonia. Thorax. 2009 Jul:64(7):592-7. doi: 10.1136/thx.2008.105080. Epub 2009 Jan 8 [PubMed PMID: 19131449]
Level 2 (mid-level) evidenceBrook I, Frazier EH. Aerobic and anaerobic microbiology of empyema. A retrospective review in two military hospitals. Chest. 1993 May:103(5):1502-7 [PubMed PMID: 8486033]
Level 2 (mid-level) evidencePinnola A, Kuo YH, Sciarretta JD, McIntyre A, Messier R, Davis JM. Bacteriology and Comorbidities in Patients Requiring Surgical Management of Empyema. The American surgeon. 2018 Apr 1:84(4):599-603 [PubMed PMID: 29712613]
Hassan M, Cargill T, Harriss E, Asciak R, Mercer RM, Bedawi EO, McCracken DJ, Psallidas I, Corcoran JP, Rahman NM. The microbiology of pleural infection in adults: a systematic review. The European respiratory journal. 2019 Sep:54(3):. pii: 1900542. doi: 10.1183/13993003.00542-2019. Epub 2019 Oct 1 [PubMed PMID: 31248959]
Level 1 (high-level) evidenceKo SC, Chen KY, Hsueh PR, Luh KT, Yang PC. Fungal empyema thoracis: an emerging clinical entity. Chest. 2000 Jun:117(6):1672-8 [PubMed PMID: 10858401]
Level 2 (mid-level) evidenceGrijalva CG, Zhu Y, Nuorti JP, Griffin MR. Emergence of parapneumonic empyema in the USA. Thorax. 2011 Aug:66(8):663-8. doi: 10.1136/thx.2010.156406. Epub 2011 May 26 [PubMed PMID: 21617169]
Gupta I, Eid SM, Gillaspie EA, Broderick S, Shafiq M. Epidemiologic Trends in Pleural Infection. A Nationwide Analysis. Annals of the American Thoracic Society. 2021 Mar:18(3):452-459. doi: 10.1513/AnnalsATS.202001-075OC. Epub [PubMed PMID: 33001756]
McCauley L, Dean N. Pneumonia and empyema: causal, casual or unknown. Journal of thoracic disease. 2015 Jun:7(6):992-8. doi: 10.3978/j.issn.2072-1439.2015.04.36. Epub [PubMed PMID: 26150912]
Davies HE, Davies RJ, Davies CW, BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010 Aug:65 Suppl 2():ii41-53. doi: 10.1136/thx.2010.137000. Epub [PubMed PMID: 20696693]
Moffett BK, Panchabhai TS, Anaya E, Nakamatsu R, Arnold FW, Peyrani P, Wiemken T, Guardiola J, Ramirez JA. Computed tomography measurements of parapneumonic effusion indicative of thoracentesis. The European respiratory journal. 2011 Dec:38(6):1406-11. doi: 10.1183/09031936.00004511. Epub 2011 May 26 [PubMed PMID: 21622586]
Davies CW, Gleeson FV, Davies RJ, Pleural Diseases Group, Standards of Care Committee, British Thoracic Society. BTS guidelines for the management of pleural infection. Thorax. 2003 May:58 Suppl 2(Suppl 2):ii18-28 [PubMed PMID: 12728147]
Level 1 (high-level) evidenceMenzies SM, Rahman NM, Wrightson JM, Davies HE, Shorten R, Gillespie SH, Davies CW, Maskell NA, Jeffrey AA, Lee YC, Davies RJ. Blood culture bottle culture of pleural fluid in pleural infection. Thorax. 2011 Aug:66(8):658-62. doi: 10.1136/thx.2010.157842. Epub 2011 Apr 1 [PubMed PMID: 21459855]
Level 2 (mid-level) evidenceColice GL, Curtis A, Deslauriers J, Heffner J, Light R, Littenberg B, Sahn S, Weinstein RA, Yusen RD. Medical and surgical treatment of parapneumonic effusions : an evidence-based guideline. Chest. 2000 Oct:118(4):1158-71 [PubMed PMID: 11035692]
Level 1 (high-level) evidenceOdaka H, Asahi R, Shimada K, Kamei M, Kato T. Empyema Caused by Pasteurella multocida in a Patient With Chronic Obstructive Respiratory Disease Taking Inhaled Corticosteroids: A Case Report. Cureus. 2023 Feb:15(2):e35156. doi: 10.7759/cureus.35156. Epub 2023 Feb 18 [PubMed PMID: 36949977]
Level 3 (low-level) evidenceVaudaux P, Waldvogel FA. Gentamicin inactivation in purulent exudates: role of cell lysis. The Journal of infectious diseases. 1980 Oct:142(4):586-93 [PubMed PMID: 7441018]
Ampofo K, Byington C. Management of parapneumonic empyema. The Pediatric infectious disease journal. 2007 May:26(5):445-6 [PubMed PMID: 17468658]
Kanellakis NI, Wrightson JM, Gerry S, Ilott N, Corcoran JP, Bedawi EO, Asciak R, Nezhentsev A, Sundaralingam A, Hallifax RJ, Economides GM, Bland LR, Daly E, Yao X, Maskell NA, Miller RF, Crook DW, Hinks TSC, Dong T, Psallidas I, Rahman NM. The bacteriology of pleural infection (TORPIDS): an exploratory metagenomics analysis through next generation sequencing. The Lancet. Microbe. 2022 Apr:3(4):e294-e302. doi: 10.1016/S2666-5247(21)00327-X. Epub 2022 Mar 11 [PubMed PMID: 35544066]
Rahman NM, Maskell NA, West A, Teoh R, Arnold A, Mackinlay C, Peckham D, Davies CW, Ali N, Kinnear W, Bentley A, Kahan BC, Wrightson JM, Davies HE, Hooper CE, Lee YC, Hedley EL, Crosthwaite N, Choo L, Helm EJ, Gleeson FV, Nunn AJ, Davies RJ. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. The New England journal of medicine. 2011 Aug 11:365(6):518-26. doi: 10.1056/NEJMoa1012740. Epub [PubMed PMID: 21830966]
Level 1 (high-level) evidencePorcel JM. Minimally invasive treatment of complicated parapneumonic effusions and empyemas in adults. The clinical respiratory journal. 2018 Apr:12(4):1361-1366. doi: 10.1111/crj.12730. Epub 2017 Nov 23 [PubMed PMID: 29087029]
Altmann ES, Crossingham I, Wilson S, Davies HR. Intra-pleural fibrinolytic therapy versus placebo, or a different fibrinolytic agent, in the treatment of adult parapneumonic effusions and empyema. The Cochrane database of systematic reviews. 2019 Oct 30:2019(10):. doi: 10.1002/14651858.CD002312.pub4. Epub 2019 Oct 30 [PubMed PMID: 31684683]
Level 1 (high-level) evidenceBedawi EO, Stavroulias D, Hedley E, Blyth KG, Kirk A, De Fonseka D, Edwards JG, Internullo E, Corcoran JP, Marchbank A, Panchal R, Caruana E, Kadwani O, Okiror L, Saba T, Purohit M, Mercer RM, Taberham R, Kanellakis N, Condliffe AM, Lewis LG, Addala DN, Asciak R, Banka R, George V, Hassan M, McCracken D, Sundaralingam A, Wrightson JM, Dobson M, West A, Barnes G, Harvey J, Slade M, Chester-Jones M, Dutton S, Miller RF, Maskell NA, Belcher E, Rahman NM. Early Video-assisted Thoracoscopic Surgery or Intrapleural Enzyme Therapy in Pleural Infection: A Feasibility Randomized Controlled Trial. The Third Multicenter Intrapleural Sepsis Trial-MIST-3. American journal of respiratory and critical care medicine. 2023 Dec 15:208(12):1305-1315. doi: 10.1164/rccm.202305-0854OC. Epub [PubMed PMID: 37820359]
Level 1 (high-level) evidenceRedden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. The Cochrane database of systematic reviews. 2017 Mar 17:3(3):CD010651. doi: 10.1002/14651858.CD010651.pub2. Epub 2017 Mar 17 [PubMed PMID: 28304084]
Level 1 (high-level) evidenceWilshire CL, Jackson AS, Meggyesy AM, Buehler KE, Chang SC, Horslen LC, Rayburn JR, Fuller CC, Farivar AS, Bograd AJ, Louie BE, Vallières E, Aye RW, Gilbert CR, Gorden JA. Comparing Initial Surgery versus Fibrinolytics for Pleural Space Infections: A Retrospective Multicenter Cohort Study. Annals of the American Thoracic Society. 2022 Nov:19(11):1827-1833. doi: 10.1513/AnnalsATS.202108-964OC. Epub [PubMed PMID: 35830586]
Level 2 (mid-level) evidenceBandaru S, Manthri S, Sundareshan V, Prakash V. Empyema Necessitans in the Setting of Methicillin-Susceptible Staphylococcus aureus Causing Pneumonia and Bacteremia. Case reports in infectious diseases. 2018:2018():4906547. doi: 10.1155/2018/4906547. Epub 2018 Apr 5 [PubMed PMID: 29850305]
Level 3 (low-level) evidenceBalfour-Lynn IM, Abrahamson E, Cohen G, Hartley J, King S, Parikh D, Spencer D, Thomson AH, Urquhart D, Paediatric Pleural Diseases Subcommittee of the BTS Standards of Care Committee. BTS guidelines for the management of pleural infection in children. Thorax. 2005 Feb:60 Suppl 1(Suppl 1):i1-21 [PubMed PMID: 15681514]
Level 1 (high-level) evidenceShen KR, Bribriesco A, Crabtree T, Denlinger C, Eby J, Eiken P, Jones DR, Keshavjee S, Maldonado F, Paul S, Kozower B. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. The Journal of thoracic and cardiovascular surgery. 2017 Jun:153(6):e129-e146. doi: 10.1016/j.jtcvs.2017.01.030. Epub 2017 Feb 4 [PubMed PMID: 28274565]
Level 3 (low-level) evidence