Introduction
Malaria is a significant global health problem with a substantial disease burden worldwide. In 2019 there were approximately 229 million cases of malaria responsible for about 409000 deaths, the majority on the African continent (WHO World Malaria Report 2020). Malaria results from infection with single-celled parasites belonging to the Plasmodium genus. Five species of Plasmodium are known to cause disease in humans: P. falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi. Globally, Plasmodium falciparum and Plasmodium vivax account for the majority of cases of malaria. While Plasmodium falciparum is responsible for more deaths, Plasmodium vivax is the most widespread of all of the malaria species, can cause severe, even fatal infections and results in significant global morbidity and mortality.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Plasmodium vivax is a protozoal infection spread via the Anopheles mosquito.
Epidemiology
Global Epidemiology
P. vivax is the most widespread of the malaria species. More than one-third of the world’s population, nearly 2.5 billion people, is at risk of infection with P. vivax malaria.[1] Due to its dormant liver phase, P. vivax can survive in colder climates than other species of malaria giving it a wider geographical range, including tropics, subtropics and temperate climates. The highest prevalence is in Latin America and Southeast Asia. According to 2018 WHO World Malaria Report, 74.1% of malaria cases in the Region of the Americas in 2017 resulted from P. vivax. While P. vivax endemicity overlaps significantly with that of P. falciparum in many parts of the world, there are several places in Southeast Asia such as South Korea where P. vivax is the exclusive cause of malaria infections.[1] A unique characteristic of the P. vivax parasite is that it requires the Duffy antigen on the surface of cells to invade red blood cells, which results in its prevalence being much lower than P. falciparum in Africa where the population has low expression of the Duffy antigen.[2] Classic teaching that the lack of Duffy antigen results in resistance to vivax malaria infection has been called into question by more recent studies have shown rare cases of P. vivax infection in Duffy-null Africans.[2][3] Acquisition of immunity to P. vivax occurs more rapidly than immunity to P. falciparum. Thus in endemic regions, morbidity tends to peak at an earlier age in P. vivax, and adults are more often asymptomatic when infected. Alternatively in low transmission settings risk of severe disease is not dependent on age.[4]
In the United States
According to the CDC, approximately 1,700 cases of malaria are diagnosed in the United States each year. In a 2004 study by Newman et al. that reviewed 185 deaths between 1963 and 2001, 92.7 % were due to P. falciparum with only 3.3% attributed to P. vivax. The study found that failure to take chemoprophylaxis, taking inappropriate or incomplete prophylaxis, and missed diagnosis were common, leading to the finding that 85% of the malaria deaths were preventable.[5]
Pathophysiology
Malaria parasites are micro-organisms belonging to the genus Plasmodium. The primary host of the parasite is the Anopheles mosquito and vertebrates (primarily humans). Malaria parasites are transmitted from the mosquito to its human host in the form of sporozoites during a blood meal. These immediately migrate to the liver where they invade hepatocytes and form schizonts. When these schizonts rupture, Plasmodium merozoites are released into the blood. This blood stage coincides with malaria symptoms in the host. Plasmodium vivax and ovale have a dormant hypnozoite liver stage. Hypnozoites may remain dormant for months or even years, causing relapsing infection when they finally re-enter the bloodstream.[4] Merozoites of P. vivax only infect reticulocytes unlike other species of malaria which will infect all stages of the red blood cell. This exclusive preference for reticulocytes results in significantly lower parasitemia levels in patients infected with P. vivax as compared to P. falciparum. While parasitemia rarely exceeds 2-3%, P. vivax can still result in significant disease due to increased host immune response[6]. Parasites undergo sexual and asexual multiplication in the human host. The infection spreads when a mosquito takes a blood meal from an infected human continuing the life cycle of the malaria parasite and eventually inoculates its next human host.
Histopathology
On Giemsa-stained blood smears, P. vivax parasites may be present. Because P. vivax invades erythrocytes, infected RBCs will appear larger than uninfected cells. Trophozoite may appear as thick, large ameboid rings, about one half the diameter of the RBC and Schuffner’s dots are present. P. vivax schizonts contain 12 to 24 merozoites, almost fill the entire cell, and also contain Schuffner’s dots.
History and Physical
The typical incubation period for vivax malaria is 12 to 17 days, but relapse may occur up to 2 years later from dormant hypnozoites.[7] Classic clinical signs and symptoms of malaria include fever, headache, nausea, vomiting, body aches, anemia, and jaundice. Making a clinical diagnosis of malaria is sometimes challenging because of the nonspecific symptoms and overlap of signs and symptoms with other febrile illnesses. Due to the parasite life cycle, patients with P. vivax malaria tend to have paroxysmal fevers every approximately 42 to 56 hours.[8] Thus P. vivax is sometimes referred to as “tertian fever.” Anemia is the most common presenting symptom in adults and children living in P. vivax endemic areas. Unlike falciparum malaria, vivax malaria does not tend to cause sequestration; thus multi-system organ failure is less common. However, there are reports of cases of severe vivax malaria.[7][8][9][10] ARDS can occur secondary to host inflammatory immune response to parasitemia.[6][8]
Evaluation
In 2010 the World Health Organization adjusted their guidelines, creating an edict that all cases concerning malaria undergo testing before initiating treatment. Two main diagnostic modalities exist to test for malaria in the clinical setting: Light microscopy and rapid diagnostic tests (RDTs). Polymerase chain reaction (PCR) testing is also available, with more utility in the research setting, it can be used to confirm malaria species after establishing a diagnosis.
Blood Smear
Direct visualization of P. vivax parasites on Giemsa-stained blood smears by light microscopy is considered the diagnostic gold standard for the diagnosis of vivax malaria. Three sets of both thick and thin smears should be obtained. Thick smears are more sensitive and are used to detect parasitemia. Thin smears allow for more clear visualization of parasites which helps with speciation. Thin smears can also be used to calculate parasite density. Light microscopy has good sensitivity and is low cost. Limitations to microscopy include the necessity for trained and experienced laboratory technicians, access to a microscope and electricity.[11]
Compared to P. falciparum, the number of parasites circulating in the blood of a person infected with P. vivax malaria is typically lower, making it more challenging to diagnose. Also, the dormant liver hypnozoite form is undetectable by current diagnostic tools.
Rapid Diagnostic Test (RDT)
Since the 1990s rapid diagnostic tests (RDTs) have become increasingly popular diagnostic tools, especially in the resource-limited setting.[11] RDTs detect one or more Plasmodium antigens in the blood. They offer the benefit of being fast, resulting in about 15 to 20 minutes and do not require a laboratory technician skilled at making and reading blood smears. RDTs are more sensitive at higher parasite loads and may be falsely negative at lower levels of parasitemia.[12]
Most RDTs test for the histidine-rich protein 2 (HRP2) found on Plasmodium falciparum. The sensitivity of these tests is as high as 93-99 percent.[13]
RDTs that can test for P. vivax may detect either the P. vivax-pLDH antigen specific to P. vivax or pan-pLDH or aldolase antigens common to all Plasmodium species.[14] Studies evaluating the utility of RDTs in detecting P. vivax have shown significantly lower sensitivities.[15][16][17]
In a 2014 Cochran Systematic Review of 47 studies enrolling 22,862 participants, looking at the use of rapid diagnostic tests for diagnosing uncomplicated non-falciparum or Plasmodium vivax malaria in endemic countries the authors found that RDTs that detect either pan-pLDH or aldolase had sensitivities for non-falciparum malaria that had a range in pooled analyses from 78% (Type 2) to 89%. They found better results for studies compared RDTs that detected a P. vivax specific antibody line to identify P. vivax. Compared with microscopy, the RDTs had pooled sensitivity of 95% (95% CI 86% to 99%) and showed pooled specificity of 99% (95% CI 99% to 100%).[12]
RDTs can remain positive one month after successful treatment of malaria.[18] In the United States standard practice is to confirm all RDTs with light microscopy.
Treatment / Management
Chloroquine remains the mainstay of treatment for uncomplicated vivax malaria. Exceptions to this include infection acquired in areas of chloroquine resistance, primarily Papua New Guinea and Indonesia[8]. According to the CDC appropriate treatment of chloroquine-sensitive uncomplicated vivax malaria includes Chloroquine phosphate or hydroxychloroquine plus primaquine. Dosing is listed below.(B3)
- Chloroquine phosphate: 600 mg base (=1,000 mg salt) orally immediately, followed by 300 mg base (=500 mg salt) orally at 6, 24, and 48 hours Total dose: 1,500 mg base (=2,500 mg salt) OR Hydroxychloroquine: 620 mg base (=800 mg salt) orally immediately, followed by 310 mg base (=400 mg salt) orally at 6, 24, and 48 hours
- Primaquine phosphate: 30 mg base orally once daily for 14 days
In regions where P. vivax is chloroquine resistant the CDC offers three possible treatment options: atovaquone-proguanil, quinine plus either tetracycline or doxycycline or mefloquine. Providers should select one of these three options to combine with primaquine.
Because of the dormant liver phase of P. vivax, primaquine must also be added to treatment regimens to treat the hypnozoite phase. Two scenarios in which primaquine is contraindicated include patient with G6PD deficiency and pregnant women. In patients with G6PD deficiency, primaquine may cause severe hemolytic anemia. Decisions for its use in this patient population must occur on a case-by-case basis.[19] In pregnant women, primaquine is contraindicated because of the risk for fetal hemolysis.[20] Delay primaquine treatment until after delivery.[21](B3)
For the treatment of severe malaria worldwide, the WHO recommends the use of intravenous artesunate (2.4mg/kg IV or IM at 0, 12, and 24h then daily). Multiple studies have shown improved efficacy and safety of artesunate in the treatment of severe malaria as compared to previously used intravenous quinidine.[22][23][24] Artesunate currently has no approval from the FDA. Current CDC recommendations for the treatment of severe malaria in the United States include intravenous quinidine plus tetracycline, or doxycycline, or clindamycin. When quinidine is administered patient require continuous cardiac monitoring because of the potential risk of arrhythmia. Intravenous artesunate is available in the United States as an investigational new drug (IND) protocol #76,725 via the CDC (https://www.cdc.gov/malaria/diagnosis_treatment/artesunate.html) for cases of severe malaria refractory to alternative treatment or when IV quinidine is unavailable.(A1)
Differential Diagnosis
- Dengue fever
- Chikungunya
- Typhoid Fever
- Sepsis from bacteremia
- Viral hemorrhagic fever
- Leptospirosis
- Rickettsial infections
- Brucellosis
- Influenza
- Viral hepatitis
Prognosis
If appropriately recognized and treated, Plasmodium vivax malaria has a good prognosis and causes significantly fewer complications than falciparum malaria. However, it is recognized that more severe disease can occur. (See below under complications)
Complications
While classically P. vivax causes lower parasitemia and less severe disease than P. falciparum, more recent publications suggest that P. vivax is responsible for more severe disease than it was initially attributed. Case reports have demonstrated P. vivax causing cerebral malaria, renal failure, acute respiratory distress, and shock.[7][8]
Another rare complication is splenic rupture which carries a very high mortality rate of up to 80%.[25]
Pregnant women are at increased risk of adverse outcomes from all forms of malaria and P. vivax is no exception. Malaria in pregnancy is associated with higher levels of parasitemia and increases the risk of prematurity, miscarriage, low birth weight, neonatal or maternal death.[8][21]
Deterrence and Patient Education
Malaria prevention takes a multifaceted approach. For travelers, adherence to appropriate malaria prophylaxis medications is key. Also, appropriate clothing (long sleeves and pants) and use of DEET and/or permethrin has been shown to reduce the risk of malaria transmission greatly.[26] Additionally, recognizing that the Anopheles mosquitos general bite around dawn and dusk, appropriate behavioral modification may avoid infection as well. For patients living or staying in endemic regions the use of treated mosquito nets correlates with decreased infection.[27]
Pearls and Other Issues
- Plasmodium vivax is the most widespread malaria species with predominance in Latin America and Southeast Asia
- The blood smear is the gold standard diagnostic tool for malaria, but in resource-limited clinical settings, rapid diagnostic tests (RDTs) are a reasonable alternative
- Treatment decisions need to account for the severity of disease and local patterns of drug resistance
- The uncomplicated disease is treatable with chloroquine or hydroxychloroquine in combination with primaquine
- In the setting of severe disease outside of the United States, IV artesunate is the treatment of choice
- In the United States severe vivax malaria can be treated with intravenous quinidine plus tetracycline, or doxycycline, or clindamycin (artesunate is available in the United States as an investigational new drug (IND) protocol # 76,725 via the CDC)
Enhancing Healthcare Team Outcomes
Recognizing and diagnosing malaria can be challenging as the symptoms are nonspecific and the diagnosis is uncommon in non-endemic areas. Thus, it is vital that all members of the healthcare team including nurses, midlevel providers, and physicians receive education and training in malaria diagnosis and management. Additionally, skilled laboratory technicians, trained in malaria parasite recognition is key to diagnostic accuracy. If uncertainty exists, a pathologist review may be required. Consultation with infectious disease specialists is often warranted especially in the setting of severe disease. Communication and coordination between healthcare providers (primary care provider, nurse practitioner, pharmacist) are critical to patient care.
Media
(Click Image to Enlarge)

Life Cycle of the Malaria Parasite Contributed by Wikimedia Commons, National Institutes of Health (NIH) (Public Domain)
(Click Image to Enlarge)
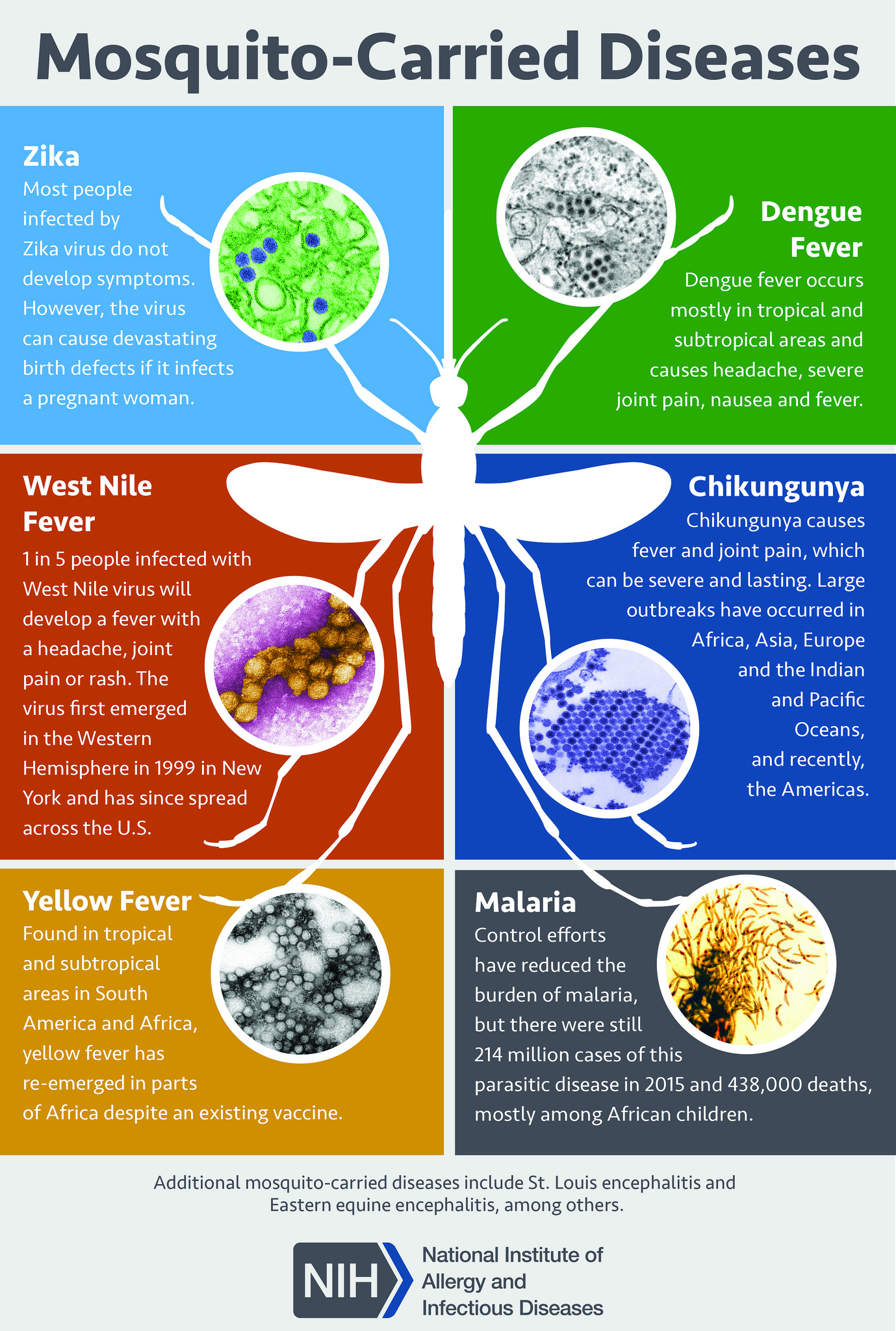
Mosquito-Borne Diseases. Mosquitoes are carriers of various diseases, including Zika, dengue fever, West Nile fever, chikungunya, yellow fever, and malaria.
National Institute of Allergy and Infectious Diseases, National Institutes of Health
(Click Image to Enlarge)
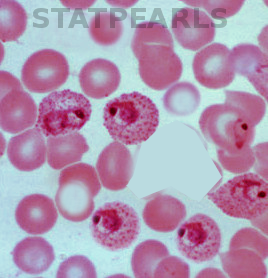
Blood smear malaria Image courtesy S Bhimji MD
References
Howes RE, Battle KE, Mendis KN, Smith DL, Cibulskis RE, Baird JK, Hay SI. Global Epidemiology of Plasmodium vivax. The American journal of tropical medicine and hygiene. 2016 Dec 28:95(6 Suppl):15-34. doi: 10.4269/ajtmh.16-0141. Epub 2016 Jul 11 [PubMed PMID: 27402513]
Gunalan K, Lo E, Hostetler JB, Yewhalaw D, Mu J, Neafsey DE, Yan G, Miller LH. Role of Plasmodium vivax Duffy-binding protein 1 in invasion of Duffy-null Africans. Proceedings of the National Academy of Sciences of the United States of America. 2016 May 31:113(22):6271-6. doi: 10.1073/pnas.1606113113. Epub 2016 May 17 [PubMed PMID: 27190089]
Gunalan K, Niangaly A, Thera MA, Doumbo OK, Miller LH. Plasmodium vivax Infections of Duffy-Negative Erythrocytes: Historically Undetected or a Recent Adaptation? Trends in parasitology. 2018 May:34(5):420-429. doi: 10.1016/j.pt.2018.02.006. Epub 2018 Mar 9 [PubMed PMID: 29530446]
Dayananda KK, Achur RN, Gowda DC. Epidemiology, drug resistance, and pathophysiology of Plasmodium vivax malaria. Journal of vector borne diseases. 2018 Jan-Mar:55(1):1-8. doi: 10.4103/0972-9062.234620. Epub [PubMed PMID: 29916441]
Newman RD, Parise ME, Barber AM, Steketee RW. Malaria-related deaths among U.S. travelers, 1963-2001. Annals of internal medicine. 2004 Oct 5:141(7):547-55 [PubMed PMID: 15466772]
Hemmer CJ, Holst FG, Kern P, Chiwakata CB, Dietrich M, Reisinger EC. Stronger host response per parasitized erythrocyte in Plasmodium vivax or ovale than in Plasmodium falciparum malaria. Tropical medicine & international health : TM & IH. 2006 Jun:11(6):817-23 [PubMed PMID: 16772003]
Level 3 (low-level) evidenceBaird JK. Evidence and implications of mortality associated with acute Plasmodium vivax malaria. Clinical microbiology reviews. 2013 Jan:26(1):36-57. doi: 10.1128/CMR.00074-12. Epub [PubMed PMID: 23297258]
Price RN, Tjitra E, Guerra CA, Yeung S, White NJ, Anstey NM. Vivax malaria: neglected and not benign. The American journal of tropical medicine and hygiene. 2007 Dec:77(6 Suppl):79-87 [PubMed PMID: 18165478]
Level 3 (low-level) evidenceKochar DK, Saxena V, Singh N, Kochar SK, Kumar SV, Das A. Plasmodium vivax malaria. Emerging infectious diseases. 2005 Jan:11(1):132-4 [PubMed PMID: 15705338]
Level 3 (low-level) evidenceVal F, Machado K, Barbosa L, Salinas JL, Siqueira AM, Costa Alecrim MG, Portillo HD, Bassat Q, Monteiro WM, Guimarães Lacerda MV. Respiratory Complications of Plasmodium vivax Malaria: Systematic Review and Meta-Analysis. The American journal of tropical medicine and hygiene. 2017 Sep:97(3):733-743. doi: 10.4269/ajtmh.17-0131. Epub 2017 Jul 19 [PubMed PMID: 28722625]
Level 1 (high-level) evidenceBoyce MR, O'Meara WP. Use of malaria RDTs in various health contexts across sub-Saharan Africa: a systematic review. BMC public health. 2017 May 18:17(1):470. doi: 10.1186/s12889-017-4398-1. Epub 2017 May 18 [PubMed PMID: 28521798]
Level 1 (high-level) evidenceAbba K, Kirkham AJ, Olliaro PL, Deeks JJ, Donegan S, Garner P, Takwoingi Y. Rapid diagnostic tests for diagnosing uncomplicated non-falciparum or Plasmodium vivax malaria in endemic countries. The Cochrane database of systematic reviews. 2014 Dec 18:2014(12):CD011431. doi: 10.1002/14651858.CD011431. Epub 2014 Dec 18 [PubMed PMID: 25519857]
Level 2 (mid-level) evidenceHaditsch M. Quality and reliability of current malaria diagnostic methods. Travel medicine and infectious disease. 2004 Aug-Nov:2(3-4):149-60 [PubMed PMID: 17291976]
Level 2 (mid-level) evidenceMaltha J, Gillet P, Jacobs J. Malaria rapid diagnostic tests in endemic settings. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2013 May:19(5):399-407. doi: 10.1111/1469-0691.12151. Epub 2013 Feb 25 [PubMed PMID: 23438048]
Pattanasin S, Proux S, Chompasuk D, Luwiradaj K, Jacquier P, Looareesuwan S, Nosten F. Evaluation of a new Plasmodium lactate dehydrogenase assay (OptiMAL-IT) for the detection of malaria. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2003 Nov-Dec:97(6):672-4 [PubMed PMID: 16117960]
Level 3 (low-level) evidenceTjitra E, Suprianto S, Dyer M, Currie BJ, Anstey NM. Field evaluation of the ICT malaria P.f/P.v immunochromatographic test for detection of Plasmodium falciparum and Plasmodium vivax in patients with a presumptive clinical diagnosis of malaria in eastern Indonesia. Journal of clinical microbiology. 1999 Aug:37(8):2412-7 [PubMed PMID: 10405377]
Level 3 (low-level) evidenceFransisca L, Kusnanto JH, Satoto TB, Sebayang B, Supriyanto, Andriyan E, Bangs MJ. Comparison of rapid diagnostic test Plasmotec Malaria-3, microscopy, and quantitative real-time PCR for diagnoses of Plasmodium falciparum and Plasmodium vivax infections in Mimika Regency, Papua, Indonesia. Malaria journal. 2015 Mar 5:14():103. doi: 10.1186/s12936-015-0615-5. Epub 2015 Mar 5 [PubMed PMID: 25890368]
Dalrymple U, Arambepola R, Gething PW, Cameron E. How long do rapid diagnostic tests remain positive after anti-malarial treatment? Malaria journal. 2018 Jun 8:17(1):228. doi: 10.1186/s12936-018-2371-9. Epub 2018 Jun 8 [PubMed PMID: 29884184]
Recht J, Ashley EA, White NJ. Use of primaquine and glucose-6-phosphate dehydrogenase deficiency testing: Divergent policies and practices in malaria endemic countries. PLoS neglected tropical diseases. 2018 Apr:12(4):e0006230. doi: 10.1371/journal.pntd.0006230. Epub 2018 Apr 19 [PubMed PMID: 29672516]
Baird JK, Hoffman SL. Primaquine therapy for malaria. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2004 Nov 1:39(9):1336-45 [PubMed PMID: 15494911]
Level 3 (low-level) evidenceKovacs SD, Rijken MJ, Stergachis A. Treating severe malaria in pregnancy: a review of the evidence. Drug safety. 2015 Feb:38(2):165-81. doi: 10.1007/s40264-014-0261-9. Epub [PubMed PMID: 25556421]
Dondorp A, Nosten F, Stepniewska K, Day N, White N, South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet (London, England). 2005 Aug 27-Sep 2:366(9487):717-25 [PubMed PMID: 16125588]
Level 1 (high-level) evidenceJones KL, Donegan S, Lalloo DG. Artesunate versus quinine for treating severe malaria. The Cochrane database of systematic reviews. 2007 Oct 17:(4):CD005967 [PubMed PMID: 17943870]
Level 1 (high-level) evidenceHess KM, Goad JA, Arguin PM. Intravenous artesunate for the treatment of severe malaria. The Annals of pharmacotherapy. 2010 Jul-Aug:44(7-8):1250-8. doi: 10.1345/aph.1M732. Epub 2010 Jun 15 [PubMed PMID: 20551300]
Hartley J. Oxford handbook of tropical medicine. BMJ (Clinical research ed.). 2000 Mar 11:320(7236):721A [PubMed PMID: 10710604]
Goodyer LI, Croft AM, Frances SP, Hill N, Moore SJ, Onyango SP, Debboun M. Expert review of the evidence base for arthropod bite avoidance. Journal of travel medicine. 2010 May-Jun:17(3):182-92. doi: 10.1111/j.1708-8305.2010.00402.x. Epub [PubMed PMID: 20536888]
Pryce J, Richardson M, Lengeler C. Insecticide-treated nets for preventing malaria. The Cochrane database of systematic reviews. 2018 Nov 6:11(11):CD000363. doi: 10.1002/14651858.CD000363.pub3. Epub 2018 Nov 6 [PubMed PMID: 30398672]
Level 1 (high-level) evidence