Introduction
Psoriasis is recognized as the most prevalent immune-mediated inflammatory disease, involving skin and joints and associated with abnormalities of other systems. Plaque psoriasis is the commonest clinical type of psoriasis. Even though the condition is not life-threatening, it is difficult to treat and response rates vary widely.[1][2]
Plaque psoriasis typically presents with large oval-circular plaques over the scalp, trunk and extensor body surface. The plaques have an extensive amount of scaling due to the hyperproliferation of the epidermal cells. Most patients have acute flares and relapses of plaque psoriasis, which may sometimes become severe and progress into the pustular subtype. At least 15% of patients with plaque psoriasis will develop psoriatic arthritis.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Psoriasis has a multifactorial etiology. Apart from genetic predisposition, risk factors that trigger psoriasis include trauma, infection, drugs, metabolic factors, stress, alcohol, smoking, and sunlight. Drugs that can exacerbate psoriasis include antimalarials, beta-blockers, bupropion, calcium channel blockers, captopril, fluoxetine, glyburide, granulocyte colony-stimulating factor, interferon, interleukins, lipid-lowering drugs, lithium, penicillin, and terbinafine.[3]
Genetic factors do play a role in plaque psoriasis; there is a much higher risk of developing plaque psoriasis if one individual already has the disorder. Patients with susceptible loci (PSOR1) on chromosome 6 are more likely to develop the disorder.
Almost all types of trauma are known to be associated with plaque psoriasis. In addition, excessive scratching can trigger or aggravate localized psoriasis. The development of psoriatic plaques at any site of trauma is known as the koebner reaction.
Sunlight is known to be beneficial for patients with plaque psoriasis; however, in a small number of patients, the disorder may be aggravated by light.
Both HIV and pharyngeal streptococcal infections have been associated with psoriasis. However, HIV patients managed with HAART tend to have less severe disease.
Epidemiology
Psoriasis is prevalent worldwide with a global prevalence of 1% to 8%. It begins in childhood in approximately one-third of cases. An increase in the prevalence of childhood psoriasis has been reported in recent years.[4][5]
Psoriasis affects both genders equally. The disorder first appears in individuals between ages 15-22 and then a second peak occurs in individuals aged between 55-70 years. Overall, the disorder appears a few years earlier in females compared to males. Psoriasis is much more common in Caucasians but low rates have been reported in Africans and the Japanese.
Pathophysiology
Psoriasis is caused by inappropriate activation of the immune system defined by a series of linked cellular changes in the skin that include keratinocyte hyperplasia; altered T-cell function and angiogenesis, the most important cell series being the helper T cells. The role of oxidative stress, reactive oxygen species [ROS] and an increased expression of insulin-like growth factor-1 (IGF-1) and epidermal growth factor (EGF) in the pathogenesis of psoriasis have been proved. Many psoriasis susceptibility loci have been detected by linkage studies (PSORS1-12). HLA-Cw6 allele has a strong association with early-onset psoriasis.
More research is ongoing in the area of biomarkers in psoriasis. Leptin and resistin are considered as candidate biomarkers for prediction of development of insulin resistance and atherosclerosis in obese patients with psoriasis. K16 expression in non-lesional psoriatic epidermis has been suggested as a marker of preclinical psoriasis. IL-18 is the candidate cytokine biomarker of disease severity. Lower levels of cell surface expression markers of T-cell subsets, such as CD8, CD45RO, CD2, CD94, and CD161 are features of inflammatory linear verrucous epidermal nevus (ILVEN) but not with Blaschko linear psoriasis.[6][7]
Histopathology
Histology of a well-developed plaque shows compact orthokeratosis, parakeratosis, spongiform pustules, microabscesses with the neutrophil collection in the upper epidermis, acanthosis, elongation of rete with widened bases, suprapapillary thinning, and tortuous dilated papillary capillaries. Dilated capillaries and keratinocyte proliferation are the consistent features in all stages of psoriasis.
History and Physical
Plaque psoriasis is asymptomatic in many individuals but can cause considerable itching, especially when there is an involvement of the scalp. Some people complain of soreness or pain due to fissuring, particularly affecting the palms and soles.
Psoriatic plaques are well-defined and erythematous with a predilection for the extensor aspect distributed over elbows, knees, and lower back. The plaques are invariably symmetrical, but the number of plaques may vary. They are covered by silvery-white scales which on removal show pinpoint bleeding spots (Auspitz sign). This is an important clinical sign although not pathognomonic in the diagnosis of plaque psoriasis. The depth of color of the plaques differs according to skin type; the full, rich red or salmon pink color is lost in dark-skinned individuals. In some patients, erythema and scaling may be less pronounced.
The presence of isomorphic (similar) lesions along the line of trauma indicates active disease and is known as the Koebner phenomenon. Fissuring is a common feature on palms, soles, and thick plaques of the limbs and lower back. The scalp, the most common initial spot, the retro-auricular area, and umbilical region are sites that should be examined in all suspected cases as these can give a signal to the evolving disease. The involvement of scalp and face may take any one or more of the following presentations: hairline psoriasis, sebopsoriasis, and true facial psoriasis.
Guttate plaques, which are commonly seen in children, may eventually evolve into psoriasis vulgaris with larger plaques in typical sites. Nail psoriasis is seen in up to 40% of cases, with pitting being the most common finding. Rupioid, elephantine and ostraceous psoriasis are special types characterized by gross hyperkeratosis. Psoriasis area and severity index [PASI] scoring is used at initial assessment and follow-up to monitor the effectiveness of therapy. Based on the PASI score, plaque psoriasis can be graded mild, moderate and severe.
About 15% of patients will present with arthritis of the small joints with features like dactylitis, joint deformity, and sausage-shaped digits.
Almost 80% of patients with psoriasis present with mild to moderate severity. Metabolic comorbidities are seen in association with psoriasis, leading to significant morbidity including type-2 diabetes mellitus, cardiovascular disease, hypertension, and metabolic syndrome. Erythrodermic, generalized pustular and arthropathic variants of psoriasis represent severe forms of psoriasis.
Evaluation
Essentially, the diagnosis of plaque psoriasis is clinical, and it is recognized by well-demarcated erythematous scaly plaques with a symmetrical distribution. Dermoscopy of typical plaques shows dotted vessels in a regular arrangement over a light red background and with uniformly distributed white scales. A biopsy may be performed to differentiate psoriasis from other inflammatory skin diseases. Patients with moderate to severe psoriasis should be screened for metabolic comorbidities like inflammatory arthritis, obesity, hypertension, diabetes, and dyslipidemia. A history of smoking and alcohol intake should be included.[8][9]
Treatment / Management
Treatments must be tailored to suit the age of the patient, quality of life (QOL) issues, and PASI score. Broadly, treatment can be categorized as topical applications, phototherapy, systemic drugs and other modalities. Topical therapy includes the use of emollients and moisturizers, corticosteroids, keratolytics, tar, anthralin, vitamin D3 analogs and calcineurin inhibitors. A combination of topical agents is sometimes more effective than when the drugs are used alone. [3][10][11]
Common sources of light therapy used in the management of plaque psoriasis include whole-body or targeted ultraviolet (UV) B (broad and narrow band), photochemotherapy (psoralen with UVA (PUVA)), home phototherapy and LASER.
Systemic drugs used include acitretin, methotrexate, cyclosporine, tacrolimus, hydroxyurea, 6-thioguanine, mycophenolate, fumaric acid esters, apremilast and biologic agents. Of the available biologic agents, etanercept, adalimumab, infliximab, secukinumab, ustekinumab, tildrakizumab and ixekizumab are indicated for plaque psoriasis. Etanercept can be safely used in children with proper monitoring. Other treatment modalities like fish oil rich in omega-3 fatty acids may be of benefit.[12]
Neuropeptide-modulating agents, newer NSAIDs like WBI-1001, LAS41002, and LAS41004, Janus-associated kinase inhibitors, MEK1/MEKK1 inhibitor, phosphodiesterase inhibitors, pan-selectin antagonists, and fibroblast growth factor 23 (FGF 23), are under research. The role of alefacept in HIV-associated psoriasis is being considered.
Extra care must be taken while treating a pregnant woman with psoriasis. UVB can be safely used, and the risk of topical PUVA is considered low in pregnancy. Adalimumab, etanercept, and infliximab come under FDA category B; anthralin, betamethasone dipropionate, calcineurin inhibitors, cyclosporine, psoralen, methylprednisolone aceponate are category C drugs; whereas, acitretin, methotrexate, and tazarotene belong to category X.
Psoriasis is a chronic inflammatory disease with remissions and exacerbations that are often requiring prolonged therapy. The choice of therapy should take into consideration the long-term side effects of therapy with particular reference to topical steroids and other immune-suppressive agents. High-potency topical steroids like clobetasol propionate are contraindicated in young children for fear of side effects like atrophy, depigmentation, and precipitation of pustular psoriasis on sudden withdrawal (which may also occur in adults using excessive quantities over a long period). While using phototherapy and systemic drugs, a similar caution should be exercised. In children, immature hepatic andrenal systems, and the active hematopoietic system should be carefully considered when prescribing systemic drugs. Since the long-term side effects of newer drugs are not yet available, it is prudent to use them only when indicated and other treatments have failed or are contraindicated.
In summary, topical therapy and phototherapy are used in mild-to-moderate psoriasis, and systemic therapy is indicated for more severe disease. Biologics should be instituted by qualified experts only when indicated.[13]
Differential Diagnosis
Psoriasis has to be differentiated from tinea corporis (dermatophyte fungal infection) and eczema. In some patients, they can coexist. ILVEN should be differentiated from Blaschko linear psoriasis. In chronic plaques that resist treatment, squamous cell carcinoma in situ and cutaneous T-cell lymphoma may require exclusion by histological examination.
Staging
Practice Guidelines
- Psoriasis is considered extensive if more than 10% of the body surface area involved
- Even localized disease can lead to severe impairment and mental stress (eg nail or joint disease, face, palms, genitals)
- Always start with topical therapy first for localized disease
- If the disease is extensive, consider methotrexate or cyclosporine.
- Consider biological therapy early and assess response promptly
- Women of childbearing age started on biological therapy should use effective contraception
- Live vaccinations should not be given to mothers who receive biological therapy
- TNF antagonists should not be used in patients with demyelination disorders, heart failure
- Phototherapy can be used as monotherapy. Short term psoralen plus UV light is more effective than light therapy alone.
- Genitals should be protected when using ultraviolet therapy
- Folate supplementation is recommended for women of childbearing age receiving light therapy
Prognosis
Plaque psoriasis is an unpredictable disorder. Not only is there no cure, but it is difficult to know who will relapse, how long the active disease will last or how frequently the patient will have remissions. The disorder is not life-threatening but with constant relapses, it can significantly affect the quality of life. Poor prognostic factors include stress, family history and early onset of symptoms. Both warm weather and sunlight have benefits and improve the symptoms. If the disorder becomes pustular, then mortality rates are high. In addition, all treatments have major adverse effects including skin cancers, liver damage and susceptibility to infections. The biggest morbidity is from poor aesthetics which can cause depression, isolation, and withdrawal from society.
Finally, psoriasis is associated with obesity and adverse cardiac events.
Complications
Complications of psoriasis include:
- Disfigurement
- Constant itching
- Poor quality of life
- Side effects of treatment.
Consultations
Patients with moderate to severe psoriasis should consult a dermatologist to determine the most suitable treatment and for monitoring phototherapy and systemic therapy.
They should consult rheumatologist if they have evidence of inflammatory joint disease.
Enhancing Healthcare Team Outcomes
Plaque psoriasis is a complex life long disorder with enormous morbidity. Thus, it is best managed by an interprofessional team.
Insulin resistance and cardiovascular diseases are more common in psoriatic patients as are metabolic comorbidities. Obesity is the most common comorbidity observed in children with psoriasis. Many patients present with reduced quality of life and psychological manifestations and need special attention and counseling. Thus, primary care clinicians should advocate lifestyle modification such as reducing weight, reducing alcohol intake and smoking cessation may help control psoriasis, improve the results of treatment and prevent future complications.
Sudden onset, palmoplantar keratoderma, severe nail dystrophy, the involvement of skin folds should arouse suspicion of associated HIV infection in whom pustular forms are also more common with a higher frequency of arthritis. [14]
Teaching Points
- Patients with psoriasis should be counseled and screened for metabolic comorbidity and arthritis.
- Treatment with systemic drugs and phototherapy should be used when indicated with proper monitoring.
- Early detection of plaque psoriasis, appropriate treatment and follow-up may prevent complications.
- In the future, biomarkers may be used to help predict the progression of disease and response to treatment.
- Alcohol is considered a trigger factor, especially in young people, and should be avoided.
- The pharmacist should educate the patient about the importance of medication compliance, adverse effects of the drugs and the need to follow up with the clinical team
- A mental health nurse should be consulted as many patients develop depression because of the poor aesthetics
- Screening for skin cancer is vital for patients who have been treated with biological agents and light therapy
Outcomes
Psoriasis is an unpredictable disorder with varying response rates to treatment. Relapses are common and what works in one person may not work in another person. Poor prognostic signs include a family history of psoriasis, early onset of disease. In many patients, psychosocial stress seems to affect the outcomes adversely. Non-photosensitive patients with plaque psoriasis are encouraged to seek sunlight and may have less severe disease in a warm weather climate. The use of potent drugs is often required in recalcitrant cases, but in some patients, the adverse effects of these drugs are not well tolerated.[15][16][17] (Level V)
Media
(Click Image to Enlarge)

(Click Image to Enlarge)

Erythematous Scaly Plaques of Psoriasis. Plaques across lower back note the silvery white scales and fissures.
Contributed by Scott Jones, MD
(Click Image to Enlarge)
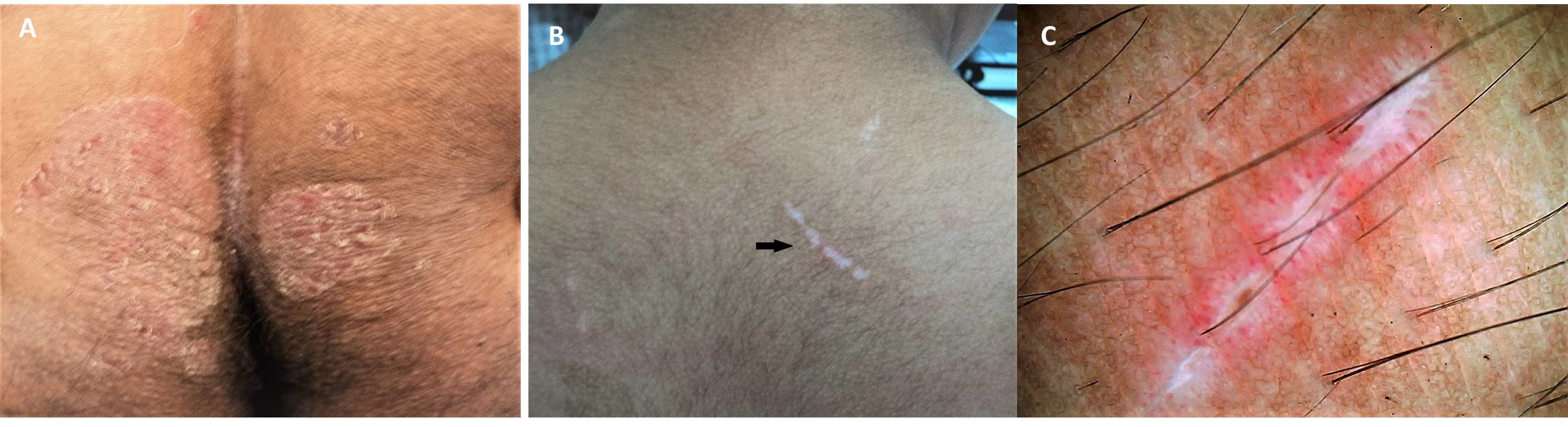
True Koebner Phenomenon. (A) In a patient with chronic plaque psoriasis. Appreciate the 'kissing' lesions of psoriasis developing along the natal cleft stemming from trivial friction-induced trauma; (B) In a patient with vitiligo vulgaris. Appreciate the linear depigmented macule over the back of patient (black arrow) with active vitiligo, which developed within a week of the patient having sustained a mild abrasion along that line; and (C) In lichen planus involving the neck fold of an adult man - Dermoscopic image highlighting the linearly arranged Wickham's striae (white structureless areas) for better clarity [Escope Videodermatoscope; 70X, polarized; Timpac Healthcare Pvt. Ltd.].
Contributed by S Sonthalia, MD, DNB, MNAMS
References
Berekmeri A, Mahmood F, Wittmann M, Helliwell P. Tofacitinib for the treatment of psoriasis and psoriatic arthritis. Expert review of clinical immunology. 2018 Sep:14(9):719-730. doi: 10.1080/1744666X.2018.1512404. Epub [PubMed PMID: 30118353]
Staubach P, Zimmer S. [Plaque psoriasis – more than a skin disorder]. Medizinische Monatsschrift fur Pharmazeuten. 2017 Jun:40(6):231-3 [PubMed PMID: 29979560]
Plaque psoriasis – more than a skin disorder., Staubach P,Zimmer S,, Medizinische Monatsschrift fur Pharmazeuten, 2017 Jun [PubMed PMID: 29979560]
Schadler ED, Ortel B, Mehlis SL. Biologics for the primary care physician: Review and treatment of psoriasis. Disease-a-month : DM. 2019 Mar:65(3):51-90. doi: 10.1016/j.disamonth.2018.06.001. Epub 2018 Jul 20 [PubMed PMID: 30037762]
Mohd Affandi A, Khan I, Ngah Saaya N. Epidemiology and Clinical Features of Adult Patients with Psoriasis in Malaysia: 10-Year Review from the Malaysian Psoriasis Registry (2007-2016). Dermatology research and practice. 2018:2018():4371471. doi: 10.1155/2018/4371471. Epub 2018 Apr 23 [PubMed PMID: 29849578]
Romiti R, Fabrício LHZ, Souza CDS, Galvão LO, de Castro CCS, Terena AC, Carneiro FRO, Oyafuso LKM, Carneiro S, Gontijo B, Kobata CM, de Oliveira MFP, Cestari T, Antônio JR, Martins GA, Marques SA, Chaibub SCW, Arruda ACBB, Félix PAO, Magalhães RF, Abulafia LA, Ferreira KA, Medeiros da Silva A, Silva BL, Souza J. Assessment of psoriasis severity in Brazilian patients with chronic plaque psoriasis attending outpatient clinics: a multicenter, population-based cross-sectional study (APPISOT). The Journal of dermatological treatment. 2018 Dec:29(8):775-785. doi: 10.1080/09546634.2018.1466023. Epub 2018 Jun 17 [PubMed PMID: 29697004]
Level 2 (mid-level) evidenceCozzani E, Rosa GM, Burlando M, Parodi A. Psoriasis as a cardiovascular risk factor: updates and algorithmic approach. Giornale italiano di dermatologia e venereologia : organo ufficiale, Societa italiana di dermatologia e sifilografia. 2018 Oct:153(5):659-665. doi: 10.23736/S0392-0488.18.06040-6. Epub 2018 Apr 19 [PubMed PMID: 29683293]
Costa MC, Rocha BO, Paixão CS, Oliveira MFSP, Mota LMHD, Carvalho LP. Monocyte subpopulations study in patients with plaque psoriasis. Medical hypotheses. 2017 Jul:104():101-103. doi: 10.1016/j.mehy.2017.05.031. Epub 2017 May 29 [PubMed PMID: 28673565]
Trayes KP, Savage K, Studdiford JS. Annular Lesions: Diagnosis and Treatment. American family physician. 2018 Sep 1:98(5):283-291 [PubMed PMID: 30216021]
Agozzino M, Noal C, Lacarrubba F, Ardigò M. Monitoring treatment response in psoriasis: current perspectives on the clinical utility of reflectance confocal microscopy. Psoriasis (Auckland, N.Z.). 2017:7():27-34. doi: 10.2147/PTT.S107514. Epub 2017 Feb 20 [PubMed PMID: 29387605]
Level 3 (low-level) evidenceHu Y, Chen Z, Gong Y, Shi Y. A Review of Switching Biologic Agents in the Treatment of Moderate-to-Severe Plaque Psoriasis. Clinical drug investigation. 2018 Mar:38(3):191-199. doi: 10.1007/s40261-017-0603-3. Epub [PubMed PMID: 29249053]
Fortina AB, Bardazzi F, Berti S, Carnevale C, Di Lernia V, El Hachem M, Neri I, Gelmetti CM, Lora V, Mazzatenta C, Milioto M, Moretta G, Patrizi A, Peris K, Villani A. Treatment of severe psoriasis in children: recommendations of an Italian expert group. European journal of pediatrics. 2017 Oct:176(10):1339-1354. doi: 10.1007/s00431-017-2985-x. Epub 2017 Aug 23 [PubMed PMID: 28836064]
Bangert C, Kopp T. Tildrakizumab for the treatment of psoriasis. Immunotherapy. 2018 Sep:10(13):1105-1122. doi: 10.2217/imt-2018-0028. Epub 2018 Aug 7 [PubMed PMID: 30081696]
Torsekar R, Gautam MM. Topical Therapies in Psoriasis. Indian dermatology online journal. 2017 Jul-Aug:8(4):235-245. doi: 10.4103/2229-5178.209622. Epub [PubMed PMID: 28761838]
Staubach P, Zimmer S. [The psoriasis patient – an exemplification of interdisciplinarity]. Medizinische Monatsschrift fur Pharmazeuten. 2017 Jun:40(6):245-6 [PubMed PMID: 29979843]
The psoriasis patient – an exemplification of interdisciplinarity., Staubach P,Zimmer S,, Medizinische Monatsschrift fur Pharmazeuten, 2017 Jun [PubMed PMID: 29979843]
Cornelius V, Wilson R, Cro S, Barker J, Burden D, Griffiths CEM, Lachmann H, McAteer H, Reynolds N, Pink A, Warren RB, Capon F, Smith C. A small population, randomised, placebo-controlled trial to determine the efficacy of anakinra in the treatment of pustular psoriasis: study protocol for the APRICOT trial. Trials. 2018 Aug 29:19(1):465. doi: 10.1186/s13063-018-2841-y. Epub 2018 Aug 29 [PubMed PMID: 30157880]
Level 1 (high-level) evidenceMoots RJ, Curiale C, Petersel D, Rolland C, Jones H, Mysler E. Efficacy and Safety Outcomes for Originator TNF Inhibitors and Biosimilars in Rheumatoid Arthritis and Psoriasis Trials: A Systematic Literature Review. BioDrugs : clinical immunotherapeutics, biopharmaceuticals and gene therapy. 2018 Jun:32(3):193-199. doi: 10.1007/s40259-018-0283-4. Epub [PubMed PMID: 29790131]
Level 1 (high-level) evidenceImafuku S, Zheng M, Tada Y, Zhang X, Theng C, Thevarajah S, Zhao Y, Song HJ. Asian consensus on assessment and management of mild to moderate plaque psoriasis with topical therapy. The Journal of dermatology. 2018 Jul:45(7):805-811. doi: 10.1111/1346-8138.14338. Epub 2018 May 9 [PubMed PMID: 29740870]
Level 3 (low-level) evidence