Introduction
The ovary is the female gonad. It is a paired intraperitoneal endocrine organ typically found in the lower left and right quadrants of the abdomen, respectively. The ovaries play a fundamental role in reproduction as well as the production of hormones.[1] Granulosa cells and theca cells found in the ovary secrete multiple hormones, including estrogen and progesterone. It is here in the ovary the follicles will mature during the proliferation phase. Once the dominant follicle matures and Luteinizing hormone surges, the oocyte will be expelled and begin its journey through the fallopian tubes and into the uterus.[2] The corpus luteum, a temporary endocrine organ will take its place in the ovary and will secrete large amounts of progesterone along with smaller amounts of inhibin A and estradiol. This hormonal production protects the oocyte and allows time for the sperm and egg to meet and implant before menstruation. If fertilization occurs, the newly formed blastocyst will secrete human chorionic gonadotropin hormone, which signals the corpus luteum to continue secreting progesterone. This function will be taken over by the placenta once it has matured. If fertilization does not occur, then the corpus luteum will degenerate into the corpus albicans, and the withdrawal of progesterone will start the process of menstruation.[3] Problems within the complex feedback loops in the ovaries, such as those described above, can result in infertility, pain, or hormone imbalances.
On physical exam, healthy ovaries are palpable, but, depending on the anatomical variation and body habitus of the patient, it may not be easy to palpate them. Ovaries that contain cysts may be easier to feel. Ultrasound is one of the most common modes of evaluating ovaries.[4] Laparoscopic procedures also provide valuable information if other modalities fail to provide answers. Multiple pathologic processes can occur in the ovaries, including ovarian cancer, ovarian torsions, ectopic pregnancies, ovarian abscesses, hormonal imbalances, or cysts. These conditions can have detrimental effects on the health of those affected.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Typically ovaries are found close to the fallopian tubes within the ovarian fossa. The ovarian fossa is composed of the bifurcation of the external iliac artery and the internal iliac artery. Anterior to the ovary is the medial umbilical ligament. Posteriorly is the ureter and internal iliac artery. Superior to the ovary is the infundibulum of the uterine tube along with the suspensory or infundibulopelvic ligament, which is the posterior extension of the broad ligament of the uterus and is also called the mesovarium. The ovary is connected to the body wall by the suspensory ligament of the ovary. Inferior to the ovary is the angle of the body and the uterine tube via the proper ligament of the ovary. The ovary has two ligaments. The suspensory ligament carries both of the ovarian artery and vein as well as the sympathetic and parasympathetic plexuses. The proper ligament of the ovary is the remnant of the gubernaculum and does not contain any vessels.[5]
The normal ovary is 2.0 cm in width, 3.5 cm in length and 1.0 cm in thickness; this is comparable to the size of a golf ball. The volume of the ovary changes as females age. One study found that 69% of changes in ovarian volume may solely be due to age. At two years old, the volume of the ovary averages 0.7 ml. At 20 years of age, the volume will peak at 7.7 ml. After this, the volume will slowly decrease until menopause, where the average volume is 2.8 ml.[6]
The microanatomy of the ovary begins with the outer epithelium; this layer is made of simple cuboidal and is called the germinal epithelium. Underneath this layer is a connective tissue made of collagen and called the tunica albuginea. The next zone contains the ovarian follicles and is called the cortex. Here follicles of different sizes and maturity can be seen. The most central zone is the medulla. It is made of loose connective tissue and contains major blood vessels; this region is also called the hilus.[7]
There are two primary functions of ovaries.
The first function of the ovary is hormone production, which changes at puberty. The ovaries will begin to secrete increasing levels of hormones, including estrogen, testosterone, inhibin, and progesterone; in response to rising levels of gonadotropin-releasing hormone (GnRH). This activity creates the hypothalamus-pituitary-ovarian (HPO) axis.[8] The GnRH is secreted by the hypothalamus, which acts on cells in the anterior pituitary. The anterior pituitary will then produce follicle-stimulating hormone (FSH) and luteinizing hormone (LH). FSH has an affinity for granulosa cells; these cells promote follicle growth and maturation. LH will affect theca cells, which produce androgens and precursors for estradiol. This estradiol will become estrogen, and the increase of estrogen at puberty leads to the development of secondary sex characteristics.[9]
Secondly, the ovary houses the egg cells, or oocytes, which begin developing in utero and pause development until puberty. The ovum mature and are released when the surge of luteinizing hormone gets secreted by the pituitary gland, which is ovulation. The average antral follicle measures between 2 to 9 mm. The average number of follicles is below 25 follicles (when using optimal resolution). Antral follicles enlarge during the menstrual cycle until a dominant follicle forms, while the others degenerate.
Embryology
Ovaries originate from the intermediate mesoderm. The ovary differentiates into the medulla, which is the central aspect and has a layer of germinal epithelium across the surface. The dorsal endoderm of the yolk sac produces cells that will become immature ova, these cells migrate to the hindgut and then on to the gonadal ridge, which forms by week 4 of development. These cells continue to mature and multiply by mitosis as they migrate. At the end of the migration at the gonadal ridge, they are considered to be oogonia. The oogonia will continue to mature within a layer of connective tissue, which will become the granulosa cells. Altogether these aspects form the basis of rudimentary ovarian follicles.[10]
The ovaries will descend as they mature, however unlike their male counterparts, the testicles, the descent will end in the abdomen. The ovaries are attached to the gubernaculum, a strip of mesoderm. The other aspect of the gubernaculum connects to the uterus, preventing the ovaries from descending lower. The proper ovarian ligament arises from the remnant of the gubernaculum.[11]
Blood Supply and Lymphatics
The ovary has dual blood supply from both the ovarian artery and the uterine artery. The ovarian artery is a paired structure that originates from the abdominal aorta below the renal artery or around L2. The artery runs through the suspensory ligament of the ovary, which then enters the mesovarium. The ovarian artery may make an anastomosis with the uterine artery within the broad ligament.[12]
The ovarian vein which travels to the ovary by the suspensory ligament provides drainage to the parametrium, cervix, mesosalpinx, and pampiniform plexus as well. It can be found to have anastomoses with the para-ovarian, uterine, vesical, rectal, and vulvar venous plexuses. The left ovarian vein voids its contents into the left renal vein, while the right ovarian vein empties directly into the inferior vena cava. The ovarian vein has a diameter of 5 mm on average.[13]
The ovaries drain the majority of their lymph into the paraaortic lymph nodes, which arise around the level of L2. The lymph travels along with the ovarian vessel to the paraaortic nodes near the bifurcation of the renal arteries and the aorta. However, researchers have noted two other pathways. The first is lymph that travels via lateral vessels to hypogastric nodes, which will then drain into the paraaortic nodes. The second is lymph that follows vessels close to the round ligament, leading to the external iliac and inguinal lymph nodes.[14] These pathways are clinically important since they provide a route of metastasis for ovarian cancer.
Nerves
There are two sources of sympathetic innervation of the ovary; one is through the ovarian plexus. The origin of the ovarian plexus is the renal plexus which also innervates parts of the fundus of the uterus. The suspensory ligament of the ovary carries this plexus to the ovaries. The second source of sympathetic innervation is through the superior ovarian nerve, carried within the ovarian ligament.[15]
The parasympathetic innervation is from the uterine (pelvic) plexus, which arise from the pelvic splanchnic nerves.
Muscles
No muscles play a significant role in the anatomy of the ovary.
Physiologic Variants
The most common variant from canonical anatomy are ovaries that contain cysts. Simple ovarian or function cysts occur naturally with the changing levels of hormones during the menstrual cycle. However, some patients have persistent or extremely large cysts, which leads to an increase in volume; this increases the rate of ovarian torsions. While cysts of any size may cause pelvic pain or cause abnormal bleeding.[16]
Another physiologic variant is the number of ovaries that developed. There have been cases of accessory and supernumerary ovaries as well as patients having a single ovary.
An accessory ovary, which is uncommon, is when there are more than two ovaries attached to the typical ligaments. These ligaments include the utero-ovarian ligament, broad ligament, or the infundibulopelvic ligament.[17]
Supernumerary ovaries, on the other hand, are extremely rare. Unlike accessory ovaries, supernumerary ovaries do not connect via the typical ligaments (utero-ovarian ligament, broad ligament, or the infundibulopelvic ligament) but develop connections to other structures, such as the large intestine, the bladder, or rectum.[18]
These extraneous ovaries are typically smaller and found incidentally during surgery. They may be asymptomatic, or if they do produce symptoms, they are commonly non-specific, including abdominal or pelvic pain. It is common for these ovaries to have cysts, which may play a role in the produced abdominal or pelvic pain. Removal is necessary as they have a higher risk of neoplastic transformation.
Single ovaries are not common, and the etiology is not fully understood, but some prevailing theories include genetic defects or mechanical errors which lead to degeneration of one of the ovaries.
One of the most common pathophysiological variants is in patients with Turner syndrome who have “streaked” or atrophied ovaries. The ovaries start developing and functioning normally, but the ovarian tissue will soon begin to degenerate before birth. Instead of having over two million oocytes, patients with Turner syndrome will have markedly less, thus leading to infertility in the majority of patients. However, cases of spontaneous pregnancy have occurred in a small sub-set that carries the mosaic karyotype. The ovaries are described as “streak ovaries” due to the degenerate tissue forming waves of connective tissue with intermittent groups of granulosa cells.[19]
Surgical Considerations
Care is necessary when operating on or around the ovaries, especially if the patient would like to maintain fertility. Multiple possible emergent surgeries are possible, which include the ovaries, and thus, it is essential to understand the anatomy. Ruptured ectopic pregnancies, ovarian torsions, or emergent cesarean sections are just a few surgeries where ovaries are at higher risk for injury. Ovaries have an abundant blood supply, and thus it is important to control bleeding, or in the case of torsion, that there is the restoration of blood flow before definitive damage occurs to the ovaries.
One of the biggest concerns is the close approximation of different structures to the ovaries. Damage to the bladder, intestines, arterial, or venous system can all have life-altering consequences. For example, an important anatomical structure to be aware of is the bilateral ureters, which typically lay in close approximation to the ovary and its ligaments. Clamping a ureter accidentally during a procedure can lead to dysfunction in the ureter and possible ipsilateral renal failure.
Clinical Significance
Functional ovaries are necessary to maintain fertility as well as hormonal balance during the reproductive years. Problems with the ovaries can lead to systematic issues including anemia, increased risk for cardiac disease, and pain.
Premature ovarian failure, or premature menopause, brings a multitude of problems other than infertility. It will bring symptoms of menopause and will reduce the benefits of estrogen. The premature weakening of the bones and cardiac protective factors are two of the most commonly discussed side effects.[20]
There are over three million new cases of polycystic ovarian syndrome (PCOS) in the United States alone. PCOS has a wide range of symptoms but typically presents with oligomenorrhea, acne, hirsutism, and infertility. The ovaries can be view by ultrasound and will usually have over 25 active follicles (when using optimal resolution).[21]
Ovarian cancers are typically insidious and are the third leading cause of cancer-related death in women. Due to its slow, benign-appearing onset, ovarian cancer has a high morbidity and mortality rate as it may not get diagnosed until it has metastasized.[22]
Media
(Click Image to Enlarge)
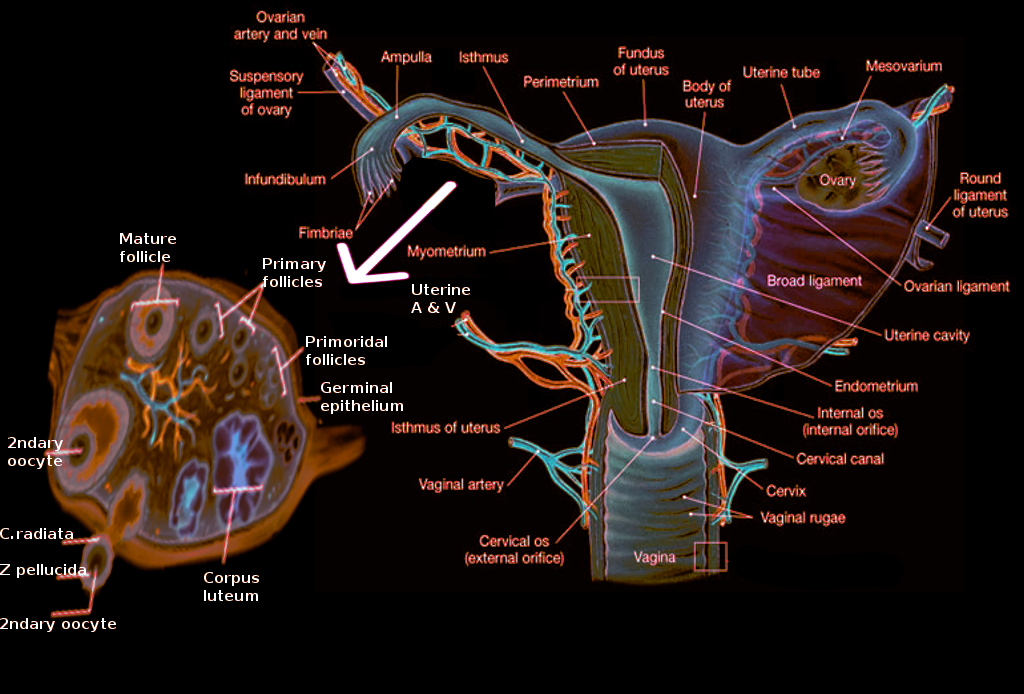
Ovary Anatomy. The ovaries are paired with female gonads, producing the female gametes (oocytes) and sex hormones, estrogen, and progesterone.
Contributed by C Orawan
References
Tetkova A, Susor A, Kubelka M, Nemcova L, Jansova D, Dvoran M, Del Llano E, Holubcova Z, Kalous J. Follicle-stimulating hormone administration affects amino acid metabolism in mammalian oocytes†. Biology of reproduction. 2019 Oct 25:101(4):719-732. doi: 10.1093/biolre/ioz117. Epub [PubMed PMID: 31290535]
Li YY, Guo L, Li H, Li J, Dong F, Yi ZY, Ouyang YC, Hou Y, Wang ZB, Sun QY, Lu SS, Han Z. NEK5 regulates cell cycle progression during mouse oocyte maturation and preimplantation embryonic development. Molecular reproduction and development. 2019 Sep:86(9):1189-1198. doi: 10.1002/mrd.23234. Epub 2019 Jul 15 [PubMed PMID: 31304658]
Oliver R, Pillarisetty LS. Anatomy, Abdomen and Pelvis, Ovary Corpus Luteum. StatPearls. 2023 Jan:(): [PubMed PMID: 30969526]
Witchel SF, Burghard AC, Tao RH, Oberfield SE. The diagnosis and treatment of PCOS in adolescents: an update. Current opinion in pediatrics. 2019 Aug:31(4):562-569. doi: 10.1097/MOP.0000000000000778. Epub [PubMed PMID: 31299022]
Level 3 (low-level) evidenceOżegowska K, Brązert M, Ciesiółka S, Nawrocki MJ, Kranc W, Celichowski P, Jankowski M, Bryja A, Jeseta M, Antosik P, Bukowska D, Skowroński MT, Bruska M, Pawelczyk L, Zabel M, Nowicki M, Kempisty B. Genes Involved in the Processes of Cell Proliferation, Migration, Adhesion, and Tissue Development as New Potential Markers of Porcine Granulosa Cellular Processes In Vitro: A Microarray Approach. DNA and cell biology. 2019 Jun:38(6):549-560. doi: 10.1089/dna.2018.4467. Epub 2019 May 22 [PubMed PMID: 31120353]
Zhu RY, Wong YC, Yong EL. Sonographic evaluation of polycystic ovaries. Best practice & research. Clinical obstetrics & gynaecology. 2016 Nov:37():25-37. doi: 10.1016/j.bpobgyn.2016.02.005. Epub 2016 Apr 1 [PubMed PMID: 27118252]
Zık B, Kurnaz H, Güler S, Asmaz ED. Effect of tamoxifen on the Notch signaling pathway in ovarian follicles of mice. Biotechnic & histochemistry : official publication of the Biological Stain Commission. 2019 Aug:94(6):410-419. doi: 10.1080/10520295.2019.1580387. Epub 2019 Jul 15 [PubMed PMID: 31305178]
Petraglia F, Musacchio C, Luisi S, De Leo V. Hormone-dependent gynaecological disorders: a pathophysiological perspective for appropriate treatment. Best practice & research. Clinical obstetrics & gynaecology. 2008 Apr:22(2):235-49 [PubMed PMID: 17804298]
Level 2 (mid-level) evidenceOwens LA, Kristensen SG, Lerner A, Christopoulos G, Lavery S, Hanyaloglu AC, Hardy K, Yding Andersen C, Franks S. Gene Expression in Granulosa Cells From Small Antral Follicles From Women With or Without Polycystic Ovaries. The Journal of clinical endocrinology and metabolism. 2019 Dec 1:104(12):6182-6192. doi: 10.1210/jc.2019-00780. Epub [PubMed PMID: 31276164]
Yoshino T, Saito D. Epithelial-to-mesenchymal transition-based morphogenesis of dorsal mesentery and gonad. Seminars in cell & developmental biology. 2019 Aug:92():105-112. doi: 10.1016/j.semcdb.2018.09.002. Epub 2018 Sep 6 [PubMed PMID: 30193994]
Kuyama H, Uemura S, Yoshida A, Yamamoto M. Close relationship between the short round ligament and the ovarian prolapsed inguinal hernia in female infants. Pediatric surgery international. 2019 May:35(5):625-629. doi: 10.1007/s00383-019-04465-6. Epub 2019 Mar 12 [PubMed PMID: 30863916]
Ying J, Feng J, Hu J, Wang S, Han P, Huang Y, Zhao W, Qian J. Can ovaries be preserved after an ovarian arteriovenous disconnection? One case report and a review of surgical treatment using Da Vinci robots for aggressive ovarian fibromatosis. Journal of ovarian research. 2019 Jun 7:12(1):52. doi: 10.1186/s13048-019-0528-y. Epub 2019 Jun 7 [PubMed PMID: 31174571]
Level 2 (mid-level) evidenceTanaka Y, Tsuboyama T, Yamamoto K, Terai Y, Ohmichi M, Narumi Y. A case of torsion of a normal ovary in the third trimester of pregnancy: MRI findings with emphasis on asymmetry in the diameter of the ovarian veins. Radiology case reports. 2019 Mar:14(3):324-327. doi: 10.1016/j.radcr.2018.11.021. Epub 2018 Dec 11 [PubMed PMID: 30581517]
Level 3 (low-level) evidenceHallas-Potts A, Dawson JC, Herrington CS. Ovarian cancer cell lines derived from non-serous carcinomas migrate and invade more aggressively than those derived from high-grade serous carcinomas. Scientific reports. 2019 Apr 2:9(1):5515. doi: 10.1038/s41598-019-41941-4. Epub 2019 Apr 2 [PubMed PMID: 30940866]
Del Campo M, Piquer B, Witherington J, Sridhar A, Lara HE. Effect of Superior Ovarian Nerve and Plexus Nerve Sympathetic Denervation on Ovarian-Derived Infertility Provoked by Estradiol Exposure to Rats. Frontiers in physiology. 2019:10():349. doi: 10.3389/fphys.2019.00349. Epub 2019 Apr 9 [PubMed PMID: 31024331]
Seo SK, Lee JB, Lee I, Yun J, Yun BH, Jung YS, Chon SJ. Clinical and pathological comparisons of adnexal torsion between pregnant and non-pregnant women. The journal of obstetrics and gynaecology research. 2019 Sep:45(9):1899-1905. doi: 10.1111/jog.14057. Epub 2019 Jul 10 [PubMed PMID: 31293029]
Gurumurthy RY, Shankar NS, Mohan Raj CS, Sriram N. Accessory ovary: A rare case report. Indian journal of pathology & microbiology. 2019 Jan-Mar:62(1):171-172. doi: 10.4103/IJPM.IJPM_648_17. Epub [PubMed PMID: 30706891]
Level 3 (low-level) evidenceOgishima D, Sakaguchi A, Kodama H, Ogura K, Miwa A, Sugimori Y, Matuoka S, Matsumoto T. Cystic Endometrioma with Coexisting Fibroma Originating in a Supernumerary Ovary in the Rectovaginal Pouch. Case reports in obstetrics and gynecology. 2017:2017():7239018. doi: 10.1155/2017/7239018. Epub 2017 Jan 22 [PubMed PMID: 28210515]
Level 3 (low-level) evidenceHankus M, Soltysik K, Szeliga K, Antosz A, Drosdzol-Cop A, Wilk K, Zachurzok A, Malecka-Tendera E, Gawlik AM. Prediction of Spontaneous Puberty in Turner Syndrome Based on Mid-Childhood Gonadotropin Concentrations, Karyotype, and Ovary Visualization: A Longitudinal Study. Hormone research in paediatrics. 2018:89(2):90-97. doi: 10.1159/000485321. Epub 2017 Dec 22 [PubMed PMID: 29275408]
Fraison E, Crawford G, Casper G, Harris V, Ledger W. Pregnancy following diagnosis of premature ovarian insufficiency: a systematic review. Reproductive biomedicine online. 2019 Sep:39(3):467-476. doi: 10.1016/j.rbmo.2019.04.019. Epub 2019 Apr 30 [PubMed PMID: 31279714]
Level 1 (high-level) evidenceSatyaraddi A, Cherian KE, Kapoor N, Kunjummen AT, Kamath MS, Thomas N, Paul TV. Body Composition, Metabolic Characteristics, and Insulin Resistance in Obese and Nonobese Women with Polycystic Ovary Syndrome. Journal of human reproductive sciences. 2019 Apr-Jun:12(2):78-84. doi: 10.4103/jhrs.JHRS_2_19. Epub [PubMed PMID: 31293320]
Chacón E, Dasí J, Caballero C, Alcázar JL. Risk of Ovarian Malignancy Algorithm versus Risk Malignancy Index-I for Preoperative Assessment of Adnexal Masses: A Systematic Review and Meta-Analysis. Gynecologic and obstetric investigation. 2019:84(6):591-598. doi: 10.1159/000501681. Epub 2019 Jul 16 [PubMed PMID: 31311023]
Level 1 (high-level) evidence