Introduction
Otosclerosis (oto, "of the ear," and sclerosis, "abnormal hardening") is a pathological bone remodeling process that affects the middle and inner ears. It was first reported by Antonio Maria Valsalva in 1735 and subsequently described pathologically by Adam Politzer in 1839.[1] In otosclerosis, the normal, dense endochondral bone of the otic capsule around the inner ear labyrinth is replaced by irregularly laid spongy bone, which subsequently hardens and leads to fixation of the stapes footplate.[2]
Otosclerosis causes conductive hearing loss that typically presents with a normal tympanic membrane. However, a reddish blush on the promontory of the cochlea may be seen in some cases (Schwartze sign) if the tympanic membrane is clear enough.[3] Additionally, depending upon the foci of involvement within the bony labyrinth, otosclerosis may involve the cochlea, resulting in sensorineural hearing loss. Because of the frequent lack of otoscopic findings and the potentially significant hearing loss, many otolaryngologists characterize the presentation of otosclerosis with the phrase, "The doctor sees nothing, and the patient hears nothing."
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiopathogenesis of otosclerosis remains unclear. Some of the multiple hypotheses that have been postulated include:
Genetic
Many loci on chromosomes 6p, 9p, 1q, 3q, 6q, 7q, 15q, and 16q have been associated with otosclerosis. In an open genome-wide analysis, a new locus on chromosome 7q22.1 has also been identified. Additionally, other bone metabolism abnormalities, such as osteogenesis imperfecta, and multiple genes associated with bone remodeling have been considered potential causes of otosclerosis, including type I collagen (COL1A1), TGF-beta 1 (BMP2 and BMP4), angiotensin II (AGT M235T and ACE I/D), autoimmune reactions, human leucocyte antigen, inflammatory and regulatory cytokines, parathyroid hormone and expression of parathyroid hormone–related peptide receptors, and oxidative stress.[4][5][6][7][8][9][10][11][12][13][14][15][16][17][18]
Hereditary
In more than half of patients presenting with otosclerosis, there is a family history of the condition. Additionally, patients with family histories of otosclerosis tend to demonstrate earlier symptom onset. Genetic studies show that an autosomal dominant mode of inheritance with reduced penetrance (40%) and variable expressivity is found in most cases.[19][20][21][22]
Sex
The prevalence of otosclerosis is twice as great in women compared to men, suggesting the role of sex hormones.[23] However, because of the elasticity that estrogens provide to ligaments, women seem to suffer less hearing loss than men with the same degree of otosclerosis.[24][23]
Ethnicity
Otosclerosis is more common in patients of European or Indian ancestry. The condition is seen less frequently in individuals of African descent.[25][26]
Pregnancy
Pregnancy appears to exacerbate hearing loss in osteosclerosis; however, the exact nature of the relationship between pregnancy and otosclerosis remains unclear.[27]
Viral Infections
A role for measles virus infection in the pathogenesis of otosclerosis has been postulated. Measles virus ribonucleic acid has been detected in the footplate of the stapes on electron microscopy and immunohistochemical studies in 59%-100% of patients.[16][28][29][30][31][32][33][34][35][36] Moreover, vaccination against the measles virus appears to be a protective factor against otosclerosis: in 2007, Arnold et al demonstrated a ~25% lower rate of treatment for otosclerosis in Germany for the population vaccinated against measles compared with patients who were not.[37]
Other Causes
In addition to the above factors, menopause, trauma, and major surgery have been reported as either causing or aggravating otosclerosis.[27][38]
Epidemiology
The prevalence of clinical otosclerosis is around 0.04%-1% in White individuals, although histological evidence of otosclerosis may be present in as much as 10% of this group.[19][39][40] In contrast, the prevalence of histological otosclerosis in Black individuals is 1%, and in the Asian population is around 5%.[19] Otosclerosis is an early adult-onset disease with an incidence greater in women compared with men in a ratio of 2:1.[20][19] The disease starts in the third and fourth decades of life but usually does not cause hearing loss until after the fourth decade.[41] Overall, otosclerosis accounts for 5%-9% of hearing loss and 18%-22% of conductive hearing loss.[42]
Pathophysiology
Multiple etiological factors, such as otosclerosis, likely contribute to the pathogenesis of bony dyscrasias. Bone remodeling occurs within the otic capsule with bone resorption followed by bone deposition, thus replacing normal bone with spongiotic bone.[43] Though similar remodeling occurs in other bones, it is not typically seen in the otic capsule.
Early in the disease process, osteoclasts appear in the lesion, and their activity results in connective tissue replacing normal bone. Later, dense sclerotic bone forms in the areas of bony resorption. The result is disorganized bone, increased osteocytes, and widened marrow spaces with vascular and connective tissue. These marrow spaces are later replaced by dense, disorganized, sclerotic bone.
The initial lesion often appears in the area of the fissula ante fenestram, located between the oval window and the cochleariform process of the middle ear, expanding from there via vascular channels.[44] It is unclear why this region appears to be the epicenter in most cases of otosclerosis, but it may be because embryonic cartilage remnants occasionally persist in that location.[45] In most cases, lesions are limited to the anterior oval window and affect its function by calcifying the annular ligament or involving the stapes footplate. Both processes result in conductive hearing loss due to the limitation of the stapes' ability to transmit sonic vibrations. See Images. External and Middle Ear, Inner Ear, and Stapes for anatomical illustrations.
Histopathology
Grossly, otosclerotic foci appear chalky white, greyish, or yellowish. If the osteosclerotic centers are active and progressing rapidly, they may appear red due to increased vascularity (this is the etiology of the Schwartze sign).
Microscopically, the dense enchondral layer of the otic capsule appears to contain spongy bone. In immature active lesions of otosclerosis, there are abundant marrow and vascular spaces with numerous osteoblasts and osteoclasts. Additionally, a large quantity of cement substance appears bluish-grey (blue mantles of Manasse) with hematoxylin and eosin staining.[46] Less vascularity and more bone and fibrillar substance than cementum are seen in mature foci, which stain red.
History and Physical
The most frequent chief complaint of patients with clinical otosclerosis is hearing loss, although tinnitus and vertigo may also occur. Patients with otosclerosis usually present with bilateral hearing loss (~70% of patients) that has been gradually worsening over many years. Typically, the hearing loss starts in one ear and, over time, progresses to involve the other ear.
Initial symptoms of otosclerosis include decreased sensitivity to low-frequency sounds, such as whispers. Patients may also paradoxically deny difficulty hearing conversation in loud background noise, which is termed "paracusis Willisii" or "paracusis of Willis," after the 1672 description of the phenomenon by Dr. Thomas Willis of Great Britain's Royal Society.[47] Although the paracusis of Willis is not pathognomonic for otosclerosis, it is indicative of conductive hearing loss. Tinnitus may worsen as the disease progresses. Vertigo is usually mild, but as the disease progresses, balance may deteriorate, mimicking Ménière disease.[48]
On physical examination, patients with otosclerosis may speak in low volume and monotonous voices. Otoscopy may reveal no abnormalities at all. With active otosclerosis, however, increased vascularity of the cochlear promontory may be visible through the tympanic membrane (Schwartze sign).[49] However, this finding is uncommon and only apparent in around 10% of patients.[50][51]
Evaluation
Tuning Fork Testing
A Weber test performed with a 512 Hz fork will generally lateralize toward the ear with the conductive loss or toward the ear with the greater conductive loss in cases of bilateral otosclerosis. Rinne testing will reveal bone conduction to be better than air conduction with >90% sensitivity if the conductive hearing loss exceeds 30 dB in magnitude, with 30 dB being the usual threshold for meeting indications for surgical intervention.[52]
Audiometry and Tympanometry
In most cases of otosclerosis, pure tone audiometry shows low frequency decreases in air conduction thresholds. Bone conduction, however, typically remains normal. A "Carhart notch" is often seen, which is an artifactual dip in the bone conduction line by 20-30 dB at 2,000 Hz due to the resonance frequency of the ossicular chain (see Image. Audiogram for Otosclerosis).[53] After stapedectomy, the Carhart notch usually disappears. A Carhart notch may also be present in cases of incus or malleus fixation and incudostapedial joint detachment.[54] Additionally, mixed hearing loss can be seen in patients with otosclerosis, particularly with advanced disease, as the process involves the cochlear endosteum and causes sensorineural hearing loss, particularly in the higher frequencies.[55]
Speech discrimination scores and tympanometry remain normal in early otosclerosis (type A tympanogram). However, a flattening or a stiffness curve may be observed in severe cases, indicating low compliance of the ossicular chain and tympanic membrane (type As tympanogram). Tympanometry can further differentiate otosclerosis from other pathologies with low resonance, such as ossicular chain discontinuity. Stapedial reflexes may be normal in early otosclerosis as well. However, they tend to disappear in later stages along with transient evoked otoacoustic emissions, particularly in patients who have had the condition for ten years or longer.[56][57]
High-Resolution Computed Tomography
Noncontrast, high-resolution computed tomography (CT) of the temporal bones is the gold standard for diagnosing otosclerosis (see Image. Otosclerosis).[58] In more overt cases, foci of spongiotic or sclerotic bone can be identified in the area anterior to the oval window. Additionally, the extent of thickening of the stapes footplate and round window involvement will inform the preoperative planning process. In cases of cochlear otosclerosis, a "halo sign" may be seen, in which radiolucent foci extend from the fissula ante fenestram around the cochlea itself.[59] A grading system suggested by Symons and Fanning can be used to characterize the severity of otosclerosis based on CT findings:[60]
- Grade 1: Spongiotic or sclerotic lesions are limited to the vicinity of the oval and round windows, manifesting as stapes footplate thickening and/or decalcified, narrowed, or enlarged round or oval windows.
- Grade 2: There is cochlear disease, with or without oval/round window involvement, localized to either the basal turn (Grade 2A), the middle/apical turns (Grade 2B), or both the basal turn and the middle/apical turns of the cochlea (Grade 2C).
- Grade 3: Cochlear involvement is diffuse and confluent with or without involvement of the oval and/or round windows.
Treatment / Management
Medical Management
Medical treatment is primarily aimed to halt the progress of otosclerosis or to prevent disease progression. There is no medical therapy that is curative for otosclerosis. Though sodium fluoride is prescribed to slow the progression of otosclerosis, its efficacy is still controversial.[61][62] Bisphosphonates exert antiresorptive action by inducing osteoclastic apoptosis, but should not be prescribed during pregnancy.(A1)
Third-generation bisphosphonates, such as risendronate and zolendronate, as well as older medications, like etidronate, have been used to treat otosclerosis with promising results.[43][63] The newer agents appear to be most effective due to their higher potencies and lower side effect profiles.[64] Additionally, vitamin D and bioflavonoids have been reported to improve hearing in some cases, but are not consistently effective.[64](A1)
Bilateral hearing aids are also used in many patients, either alone or in combination with other treatments.
Surgical Management
The treatment of choice is stapedotomy or stapedectomy, along with the placement of a prosthesis. In these procedures, either a hole is drilled in the center of the stapes footplate with a high-speed microdrill or a laser (stapedotomy), and a prosthesis is placed between the long process of the incus and the oval window membrane via the hole in the stapes footplate, or the stapes footplate is removed partially or in its entirety and a prosthesis placed between the incus and the oval window, typically with a vein or fascia graft used to protect the oval window membrane (stapedectomy) (see Image. Incudostapedial Joint, Intraoperative view). In both procedures, the crura of the stapes are fractured, and the incudostapedial joint is divided in order to permit the removal of the stapes superstructure.[65]
Surgical treatment for otosclerosis generally produces good outcomes, irrespective of the approach employed, provided appropriate patient selection. For patients with bilateral otosclerosis, the ear with greater hearing loss is typically addressed first; both ears are not operated under the same anesthetic in order to avoid the very unlikely scenario in which total sensorineural hearing loss occurs bilaterally as a result of surgery. A 2018 review published by Cheng et al indicated comparable results between stapedotomy and stapedectomy, with a slight advantage in terms of high-frequency hearing and complication rate for stapedotomy.[66] Revision surgery, if indicated for otosclerosis, is met with mixed success and may be necessary if the first attempt fails to improve hearing. In some cases, hearing results may be insufficient, and hearing aid use may still be required.
Complications from surgery include facial paralysis (if the tympanic segment of the facial nerve is injured where it passes superior to the oval window, particularly if it is dehiscent in the middle ear and hangs over the oval window), dysgeusia (from injury to the chorda tympani nerve during removal of the scutum bone in the surgical approach to the stapes), prosthesis displacement, reparative granuloma (an inflammatory reaction that may result in sensorineural hearing loss), and vertigo (if the prosthesis is too long and stimulates the saccule).[2][67][68][69][70] In order to ensure the correct length of prosthesis and prevent vertigo, many surgeons prefer to operate under local anesthesia with the patient awake.(B2)
Differential Diagnosis
Other otologic pathologies that present with conductive hearing loss and from which otosclerosis should be differentiated include:
Prognosis
Roughly 90% of patients with otosclerosis experience considerable improvement in their hearing acuity after surgery.[79] Occasionally, there may be a few cases in which the surgery yields no particular benefits. Worsening of the hearing loss has also been reported, albeit rarely.
Additionally, there is a chance of recurrence of the conductive hearing loss, which may be due to displacement of the prosthesis out of its original position with or without fixation of the prosthesis to the surrounding bone of the oval window or stapes footplate. If revision surgery is required, hearing outcomes are likely to be worse than those obtained with primary surgery.[80][81]
Complications
Untreated otosclerosis can gradually progress to moderate-severe (50-60 dB) conductive hearing loss, but profound hearing loss is unusual; it is indicative of cochlear involvement. On the other hand, surgical management of otosclerosis can result in a total sensorineural loss in the operated ear due to technical errors or occurrence of a reparative granuloma postoperatively, but these are very infrequent occurrences. Other complications of surgery for otosclerosis include facial nerve injury, vertigo, dysgeusia, and tinnitus. The prosthesis itself may also contribute to adverse outcomes, including necrosis and erosion of the long process of the incus due to overly tight crimping of the prosthesis onto the incus, displacement of the prosthesis, and development of the aforementioned reparative granuloma.[80]
Deterrence and Patient Education
Patients with family histories of otosclerosis should consider undergoing screening audiometry to identify conductive hearing loss early and consider initiating prophylactic medical therapy, such as oral sodium fluoride supplementation. Similarly, patients who notice the appearance or worsening of hearing loss during pregnancy should undergo audiometry and consider starting sodium fluoride to delay or prevent progression of the disease.
Enhancing Healthcare Team Outcomes
Otosclerosis is an early adult-onset disease that progresses with time, ultimately leading to moderate to severe conductive hearing loss and potentially even profound sensorineural hearing loss if left untreated for long enough. Interprofessional communication and care coordination among the otolaryngologist or otologist, primary care provider, audiologist, and nursing staff will enhance overall outcomes for patients and minimize complications, particularly from surgery. Similarly, educating healthcare providers who lack experience with otosclerosis will permit prompt diagnosis and referral for specialist management, thus leading to better outcomes for patients.
Media
(Click Image to Enlarge)
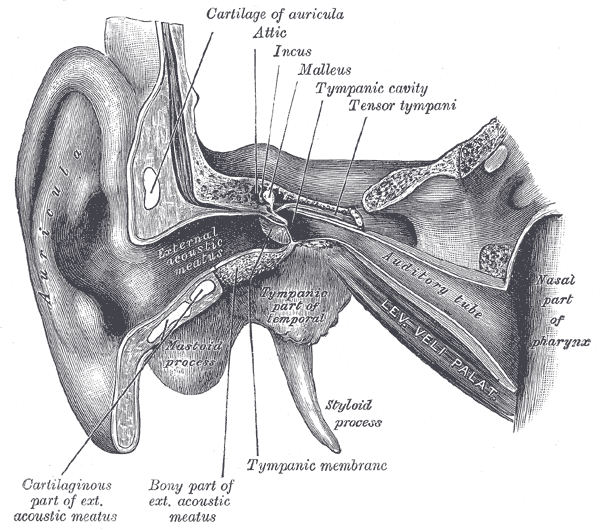
External and Middle Ear. Illustrated anatomy includes the attic, incus, malleus, tympanic cavity, tensor tympani, and auditory tube.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
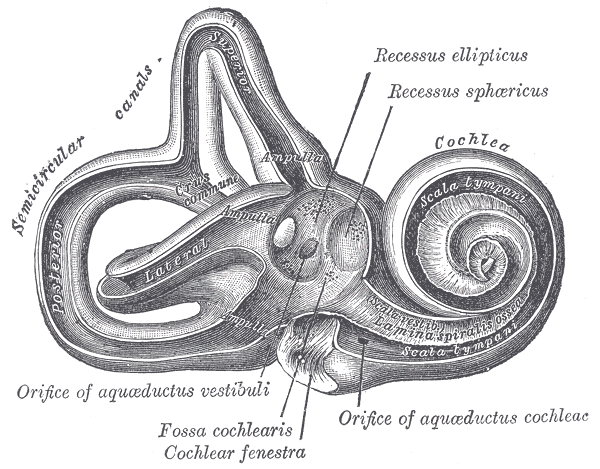
Internal Ear. Illustrated anatomy includes the labyrinth, interior of right osseous labyrinth, orifice of vestibular aqueduct, fossa cochlearis, cochlear fenestra, orifice of aquaeductus cochleae, and scala tympani.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
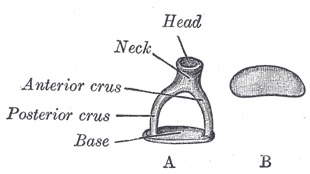
Left Stapes. Image A shows the left stapes' superior view. Image B shows the medial view of the left stapes' base. Structures included in these images include the head, neck, anterior and posterior crura, and base.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
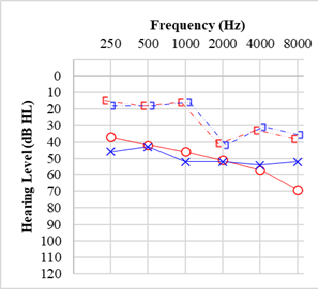
Audiogram for Otosclerosis
Contributed by Mandy Salmon
(Click Image to Enlarge)
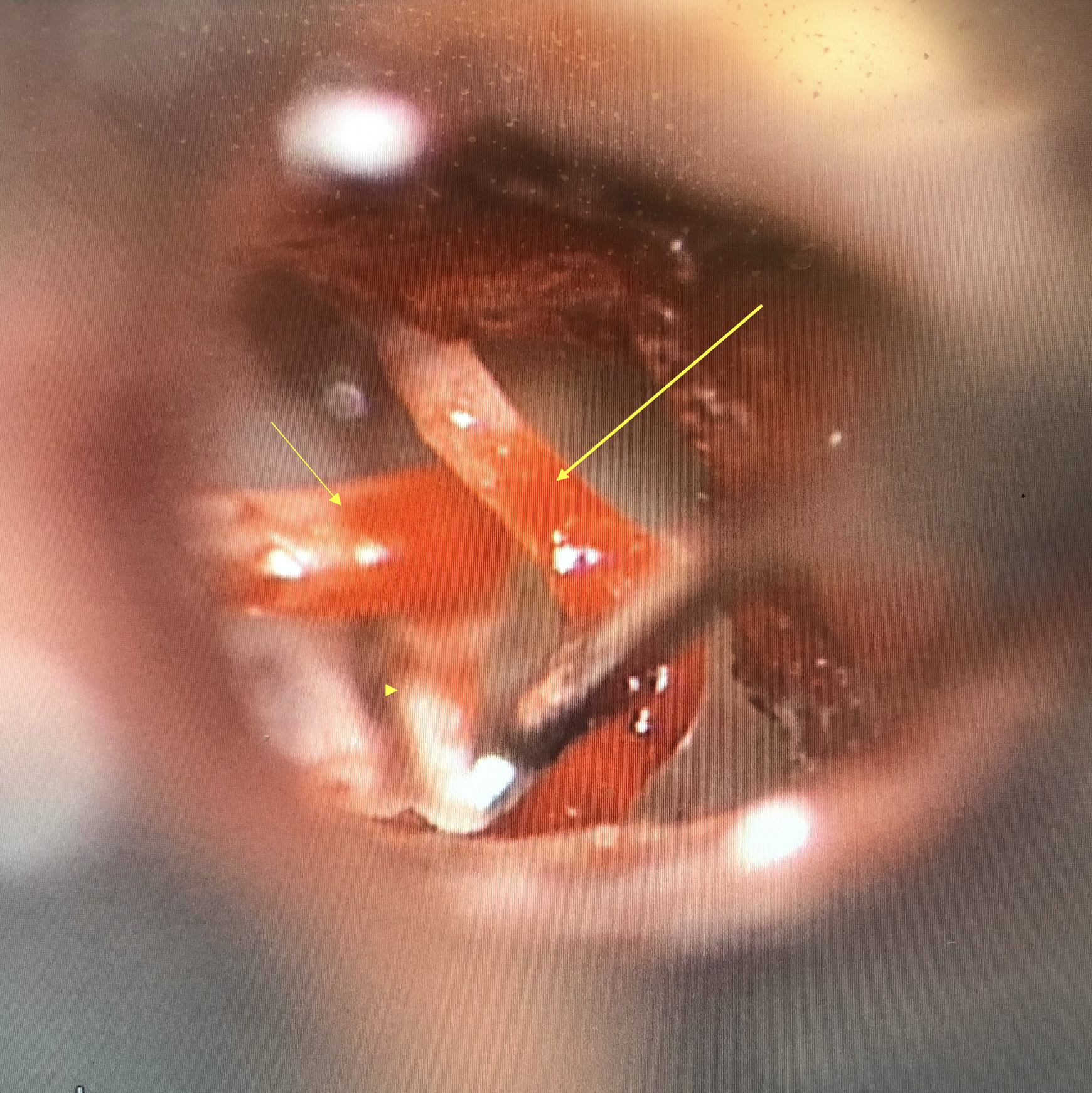
Incudostapedial Joint, Intraoperative View. Intraoperative view of the dehiscent tympanic segment of the facial nerve (long arrow) being gently retracted to visualize the joint between the incus (short arrow) and stapes (arrowhead).
Contributed by Ryan Winters, MD
(Click Image to Enlarge)
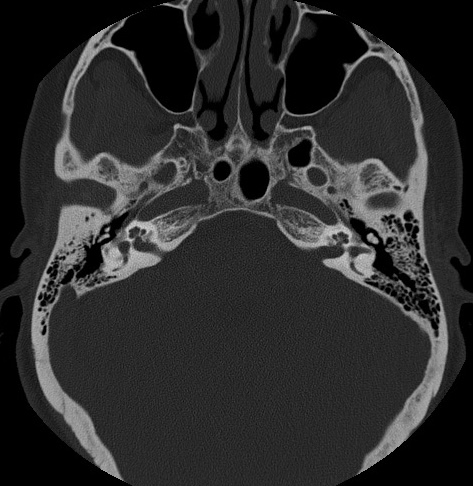
Otosclerosis Contributed by Steve Lange, MD
References
Makarem AO, Hoang TA, Lo WW, Linthicum FH Jr, Fayad JN. Cavitating otosclerosis: clinical, radiologic, and histopathologic correlations. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2010 Apr:31(3):381-4. doi: 10.1097/MAO.0b013e3181d275e8. Epub [PubMed PMID: 20195188]
Level 3 (low-level) evidenceRudic M, Keogh I, Wagner R, Wilkinson E, Kiros N, Ferrary E, Sterkers O, Bozorg Grayeli A, Zarkovic K, Zarkovic N. The pathophysiology of otosclerosis: Review of current research. Hearing research. 2015 Dec:330(Pt A):51-6. doi: 10.1016/j.heares.2015.07.014. Epub 2015 Aug 12 [PubMed PMID: 26276418]
Koenen L, Gupta G. Schwartze Sign. StatPearls. 2024 Jan:(): [PubMed PMID: 30422516]
Bittermann AJ, Wegner I, Noordman BJ, Vincent R, van der Heijden GJ, Grolman W. An introduction of genetics in otosclerosis: a systematic review. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2014 Jan:150(1):34-9. doi: 10.1177/0194599813509951. Epub 2013 Oct 29 [PubMed PMID: 24170657]
Level 1 (high-level) evidenceVan Den Bogaert K, Govaerts PJ, Schatteman I, Brown MR, Caethoven G, Offeciers FE, Somers T, Declau F, Coucke P, Van de Heyning P, Smith RJ, Van Camp G. A second gene for otosclerosis, OTSC2, maps to chromosome 7q34-36. American journal of human genetics. 2001 Feb:68(2):495-500 [PubMed PMID: 11170898]
Chen W, Campbell CA, Green GE, Van Den Bogaert K, Komodikis C, Manolidis LS, Aconomou E, Kyamides Y, Christodoulou K, Faghel C, Giguére CM, Alford RL, Manolidis S, Van Camp G, Smith RJ. Linkage of otosclerosis to a third locus (OTSC3) on human chromosome 6p21.3-22.3. Journal of medical genetics. 2002 Jul:39(7):473-7 [PubMed PMID: 12114476]
Brownstein Z, Goldfarb A, Levi H, Frydman M, Avraham KB. Chromosomal mapping and phenotypic characterization of hereditary otosclerosis linked to the OTSC4 locus. Archives of otolaryngology--head & neck surgery. 2006 Apr:132(4):416-24 [PubMed PMID: 16618911]
Thys M, Van Den Bogaert K, Iliadou V, Vanderstraeten K, Dieltjens N, Schrauwen I, Chen W, Eleftheriades N, Grigoriadou M, Pauw RJ, Cremers CR, Smith RJ, Petersen MB, Van Camp G. A seventh locus for otosclerosis, OTSC7, maps to chromosome 6q13-16.1. European journal of human genetics : EJHG. 2007 Mar:15(3):362-8 [PubMed PMID: 17213839]
Bel Hadj Ali I, Thys M, Beltaief N, Schrauwen I, Hilgert N, Vanderstraeten K, Dieltjens N, Mnif E, Hachicha S, Besbes G, Ben Arab S, Van Camp G. A new locus for otosclerosis, OTSC8, maps to the pericentromeric region of chromosome 9. Human genetics. 2008 Apr:123(3):267-72. doi: 10.1007/s00439-008-0470-3. Epub 2008 Jan 26 [PubMed PMID: 18224337]
Schrauwen I, Weegerink NJ, Fransen E, Claes C, Pennings RJ, Cremers CW, Huygen PL, Kunst HP, Van Camp G. A new locus for otosclerosis, OTSC10, maps to chromosome 1q41-44. Clinical genetics. 2011 May:79(5):495-7. doi: 10.1111/j.1399-0004.2010.01576.x. Epub [PubMed PMID: 21470211]
Level 3 (low-level) evidenceChen W, Meyer NC, McKenna MJ, Pfister M, McBride DJ Jr, Fukushima K, Thys M, Camp GV, Smith RJ. Single-nucleotide polymorphisms in the COL1A1 regulatory regions are associated with otosclerosis. Clinical genetics. 2007 May:71(5):406-14 [PubMed PMID: 17489845]
Level 3 (low-level) evidenceThys M, Schrauwen I, Vanderstraeten K, Dieltjens N, Fransen E, Ealy M, Cremers CW, van de Heyning P, Vincent R, Offeciers E, Smith RH, van Camp G. Detection of rare nonsynonymous variants in TGFB1 in otosclerosis patients. Annals of human genetics. 2009 Mar:73(2):171-5. doi: 10.1111/j.1469-1809.2009.00505.x. Epub 2009 Jan 30 [PubMed PMID: 19207109]
Level 2 (mid-level) evidenceImauchi Y, Jeunemaître X, Boussion M, Ferrary E, Sterkers O, Grayeli AB. Relation between renin-angiotensin-aldosterone system and otosclerosis: a genetic association and in vitro study. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2008 Apr:29(3):295-301 [PubMed PMID: 18491423]
Level 2 (mid-level) evidenceYoo TJ. Etiopathogenesis of otosclerosis: a hypothesis. The Annals of otology, rhinology, and laryngology. 1984 Jan-Feb:93(1 Pt 1):28-33 [PubMed PMID: 6367600]
Level 3 (low-level) evidenceMiyazawa T, Tago C, Ueda H, Niwa H, Yanagita N. HLA associations in otosclerosis in Japanese patients. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 1996:253(8):501-3 [PubMed PMID: 8950552]
Karosi T, Jókay I, Kónya J, Szabó LZ, Pytel J, Jóri J, Szalmás A, Sziklai I. Detection of osteoprotegerin and TNF-alpha mRNA in ankylotic Stapes footplates in connection with measles virus positivity. The Laryngoscope. 2006 Aug:116(8):1427-33 [PubMed PMID: 16885748]
Level 2 (mid-level) evidenceMenger DJ, Tange RA. The aetiology of otosclerosis: a review of the literature. Clinical otolaryngology and allied sciences. 2003 Apr:28(2):112-20 [PubMed PMID: 12680829]
Fanó G, Venti-Donti G, Belia S, Paludetti G, Antonica A, Donti E, Maurizi M. PTH induces modification of transductive events in otosclerotic bone cell cultures. Cell biochemistry and function. 1993 Dec:11(4):257-61 [PubMed PMID: 8275550]
Markou K, Goudakos J. An overview of the etiology of otosclerosis. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2009 Jan:266(1):25-35. doi: 10.1007/s00405-008-0790-x. Epub 2008 Aug 13 [PubMed PMID: 18704474]
Level 3 (low-level) evidenceCrompton M, Cadge BA, Ziff JL, Mowat AJ, Nash R, Lavy JA, Powell HRF, Aldren CP, Saeed SR, Dawson SJ. The Epidemiology of Otosclerosis in a British Cohort. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2019 Jan:40(1):22-30. doi: 10.1097/MAO.0000000000002047. Epub [PubMed PMID: 30540696]
Moumoulidis I, Axon P, Baguley D, Reid E. A review on the genetics of otosclerosis. Clinical otolaryngology : official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery. 2007 Aug:32(4):239-47 [PubMed PMID: 17651264]
Morrison AW, Bundey SE. The inheritance of otosclerosis. The Journal of laryngology and otology. 1970 Sep:84(9):921-32 [PubMed PMID: 5471896]
Ben Arab S, Besbes G, Hachicha S. [Otosclerosis in populations living in northern Tunisia: epidemiology and etiology]. Annales d'oto-laryngologie et de chirurgie cervico faciale : bulletin de la Societe d'oto-laryngologie des hopitaux de Paris. 2001 Feb:118(1):19-25 [PubMed PMID: 11240433]
Ricci G, Gambacorta V, Lapenna R, Della Volpe A, La Mantia I, Ralli M, Di Stadio A. The effect of female hormone in otosclerosis. A comparative study and speculation about their effect on the ossicular chain based on the clinical results. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2022 Oct:279(10):4831-4838. doi: 10.1007/s00405-022-07295-w. Epub 2022 Feb 21 [PubMed PMID: 35187596]
Level 2 (mid-level) evidenceJOSEPH RB, FRAZER JP. OTOSCLEROSIS INCIDENCE IN CAUCASIANS AND JAPANESE. Archives of otolaryngology (Chicago, Ill. : 1960). 1964 Sep:80():256-62 [PubMed PMID: 14172803]
Arli C, Gulmez I, Saraç ET, Okuyucu Ş. Assessment of inflammatory markers in otosclerosis patients. Brazilian journal of otorhinolaryngology. 2020 Jul-Aug:86(4):456-460. doi: 10.1016/j.bjorl.2018.12.014. Epub 2019 Mar 8 [PubMed PMID: 30926454]
Gristwood RE, Venables WN. Pregnancy and otosclerosis. Clinical otolaryngology and allied sciences. 1983 Jun:8(3):205-10 [PubMed PMID: 6883784]
Level 2 (mid-level) evidenceKarosi T, Kónya J, Szabó LZ, Sziklai I. Measles virus prevalence in otosclerotic foci. Advances in oto-rhino-laryngology. 2007:65():93-106. doi: 10.1159/000098677. Epub [PubMed PMID: 17245029]
Level 2 (mid-level) evidenceKarosi T, Jókay I, Kónya J, Petkó M, Szabó LZ, Pytel J, Jóri J, Sziklai I. Activated osteoclasts with CD51/61 expression in otosclerosis. The Laryngoscope. 2006 Aug:116(8):1478-84 [PubMed PMID: 16885757]
Niedermeyer HP, Arnold W, Schuster M, Baumann C, Kramer J, Neubert WJ, Sedlmeier R. Persistent measles virus infection and otosclerosis. The Annals of otology, rhinology, and laryngology. 2001 Oct:110(10):897-903 [PubMed PMID: 11642419]
Niedermeyer HP, Arnold W, Neubert WJ, Sedlmeier R. Persistent measles virus infection as a possible cause of otosclerosis: state of the art. Ear, nose, & throat journal. 2000 Aug:79(8):552-4, 556, 558 passim [PubMed PMID: 10969462]
Level 2 (mid-level) evidenceNiedermeyer HP, Arnold W. Otosclerosis: a measles virus associated inflammatory disease. Acta oto-laryngologica. 1995 Mar:115(2):300-3 [PubMed PMID: 7610826]
McKenna MJ, Kristiansen AG, Haines J. Polymerase chain reaction amplification of a measles virus sequence from human temporal bone sections with active otosclerosis. The American journal of otology. 1996 Nov:17(6):827-30 [PubMed PMID: 8915408]
McKenna MJ, Mills BG. Immunohistochemical evidence of measles virus antigens in active otosclerosis. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1989 Oct:101(4):415-21 [PubMed PMID: 2508016]
Arnold W, Friedmann I. [Detection of measles and rubella-specific antigens in the endochondral ossification zone in otosclerosis]. Laryngologie, Rhinologie, Otologie. 1987 Apr:66(4):167-71 [PubMed PMID: 2439859]
Arnold W, Niedermeyer HP, Lehn N, Neubert W, Höfler H. Measles virus in otosclerosis and the specific immune response of the inner ear. Acta oto-laryngologica. 1996 Sep:116(5):705-9 [PubMed PMID: 8908246]
Arnold W, Busch R, Arnold A, Ritscher B, Neiss A, Niedermeyer HP. The influence of measles vaccination on the incidence of otosclerosis in Germany. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2007 Jul:264(7):741-8 [PubMed PMID: 17297608]
Level 2 (mid-level) evidenceHorner KC. The effect of sex hormones on bone metabolism of the otic capsule--an overview. Hearing research. 2009 Jun:252(1-2):56-60. doi: 10.1016/j.heares.2008.12.004. Epub 2008 Dec 24 [PubMed PMID: 19121641]
Level 3 (low-level) evidenceBrowning GG, Gatehouse S. Sensorineural hearing loss in stapedial otosclerosis. The Annals of otology, rhinology, and laryngology. 1984 Jan-Feb:93(1 Pt 1):13-16 [PubMed PMID: 6703592]
Declau F, Spaendonck MV, Timmermans JP, Michaels L, Liang J, Qiu JP, Van de Heyning P. Prevalence of histologic otosclerosis: an unbiased temporal bone study in Caucasians. Advances in oto-rhino-laryngology. 2007:65():6-16. doi: 10.1159/000098663. Epub [PubMed PMID: 17245017]
Level 2 (mid-level) evidenceFitzgerald DC. The aging ear. American family physician. 1985 Feb:31(2):225-32 [PubMed PMID: 3883726]
Sagar PR, Shah P, Bollampally VC, Alhumaidi N, Malik BH. Otosclerosis and Measles: Do Measles Have a Role in Otosclerosis? A Review Article. Cureus. 2020 Aug 21:12(8):e9908. doi: 10.7759/cureus.9908. Epub 2020 Aug 21 [PubMed PMID: 32968571]
Chole RA, McKenna M. Pathophysiology of otosclerosis. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2001 Mar:22(2):249-57 [PubMed PMID: 11300278]
Wiatr A, Składzień J, Świeży K, Wiatr M. A Biochemical Analysis of the Stapes. Medical science monitor : international medical journal of experimental and clinical research. 2019 Apr 12:25():2679-2686. doi: 10.12659/MSM.913635. Epub 2019 Apr 12 [PubMed PMID: 30975972]
Viza Puiggrós I, Granell Moreno E, Calvo Navarro C, Bohé Rovira M, Orús Dotu C, Quer I Agustí M. Diagnostic utility of labyrinth capsule bone density in the diagnosis of otosclerosis with high resolution tomography. Acta otorrinolaringologica espanola. 2020 Jul-Aug:71(4):242-248. doi: 10.1016/j.otorri.2019.09.004. Epub 2020 Mar 8 [PubMed PMID: 32156439]
Lindsay JR. Blue mantles in otosclerosis. The Annals of otology, rhinology, and laryngology. 1974 Jan-Feb:83(1):33-41 [PubMed PMID: 4130014]
Quinn KJ, Coelho DH. The Curious Rise and Incomplete Fall of "Paracusis Willisii". Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2022 Jan 1:43(1):137-143. doi: 10.1097/MAO.0000000000003368. Epub [PubMed PMID: 34619730]
Eza-Nuñez P, Manrique-Rodriguez M, Perez-Fernandez N. Otosclerosis among patients with dizziness. Revue de laryngologie - otologie - rhinologie. 2010:131(3):199-206 [PubMed PMID: 21488576]
Uppal S, Bajaj Y, Rustom I, Coatesworth AP. Otosclerosis 1: the aetiopathogenesis of otosclerosis. International journal of clinical practice. 2009 Oct:63(10):1526-30. doi: 10.1111/j.1742-1241.2009.02045.x. Epub [PubMed PMID: 19769709]
Nourollahian M, Irani S. Bilateral schwartze sign, decision-making for surgery. Iranian journal of otorhinolaryngology. 2013 Sep:25(73):263 [PubMed PMID: 24303451]
Salomone R, Riskalla PE, Vicente Ade O, Boccalini MC, Chaves AG, Lopes R, Felin Filho GB. Pediatric otosclerosis: case report and literature review. Brazilian journal of otorhinolaryngology. 2008 Mar-Apr:74(2):303-6 [PubMed PMID: 18568213]
Level 3 (low-level) evidenceKelly EA, Li B, Adams ME. Diagnostic Accuracy of Tuning Fork Tests for Hearing Loss: A Systematic Review. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2018 Aug:159(2):220-230. doi: 10.1177/0194599818770405. Epub 2018 Apr 17 [PubMed PMID: 29661046]
Level 1 (high-level) evidenceStenfelt S. Inner ear contribution to bone conduction hearing in the human. Hearing research. 2015 Nov:329():41-51. doi: 10.1016/j.heares.2014.12.003. Epub 2014 Dec 18 [PubMed PMID: 25528492]
Kashio A, Ito K, Kakigi A, Karino S, Iwasaki S, Sakamoto T, Yasui T, Suzuki M, Yamasoba T. Carhart notch 2-kHz bone conduction threshold dip: a nondefinitive predictor of stapes fixation in conductive hearing loss with normal tympanic membrane. Archives of otolaryngology--head & neck surgery. 2011 Mar:137(3):236-40. doi: 10.1001/archoto.2011.14. Epub [PubMed PMID: 21422306]
Level 2 (mid-level) evidenceCureoglu S, Baylan MY, Paparella MM. Cochlear otosclerosis. Current opinion in otolaryngology & head and neck surgery. 2010 Oct:18(5):357-62. doi: 10.1097/MOO.0b013e32833d11d9. Epub [PubMed PMID: 20693902]
Level 3 (low-level) evidenceKeefe DH, Archer KL, Schmid KK, Fitzpatrick DF, Feeney MP, Hunter LL. Identifying Otosclerosis with Aural Acoustical Tests of Absorbance, Group Delay, Acoustic Reflex Threshold, and Otoacoustic Emissions. Journal of the American Academy of Audiology. 2017 Oct:28(9):838-860. doi: 10.3766/jaaa.16172. Epub [PubMed PMID: 28972472]
Terkildsen K, Osterhammel P, Bretlau P. Acoustic middle ear muscle reflexes in patients with otosclerosis. Archives of otolaryngology (Chicago, Ill. : 1960). 1973 Sep:98(3):152-5 [PubMed PMID: 4742419]
Virk JS, Singh A, Lingam RK. The role of imaging in the diagnosis and management of otosclerosis. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2013 Sep:34(7):e55-60. doi: 10.1097/MAO.0b013e318298ac96. Epub [PubMed PMID: 23921926]
Level 1 (high-level) evidencede Oliveira Penido N, de Oliveira Vicente A. Medical Management of Otosclerosis. Otolaryngologic clinics of North America. 2018 Apr:51(2):441-452. doi: 10.1016/j.otc.2017.11.006. Epub [PubMed PMID: 29502728]
Lee TC, Aviv RI, Chen JM, Nedzelski JM, Fox AJ, Symons SP. CT grading of otosclerosis. AJNR. American journal of neuroradiology. 2009 Aug:30(7):1435-9. doi: 10.3174/ajnr.A1558. Epub 2009 Mar 25 [PubMed PMID: 19321627]
Uppal S, Bajaj Y, Coatesworth AP. Otosclerosis 2: the medical management of otosclerosis. International journal of clinical practice. 2010 Jan:64(2):256-65. doi: 10.1111/j.1742-1241.2009.02046.x. Epub [PubMed PMID: 20089010]
Hentschel MA, Huizinga P, van der Velden DL, Wegner I, Bittermann AJ, van der Heijden GJ, Grolman W. Limited evidence for the effect of sodium fluoride on deterioration of hearing loss in patients with otosclerosis: a systematic review of the literature. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2014 Jul:35(6):1052-7. doi: 10.1097/MAO.0000000000000310. Epub [PubMed PMID: 24751746]
Level 1 (high-level) evidenceQuesnel AM, Seton M, Merchant SN, Halpin C, McKenna MJ. Third-generation bisphosphonates for treatment of sensorineural hearing loss in otosclerosis. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2012 Oct:33(8):1308-14. doi: 10.1097/MAO.0b013e318268d1b3. Epub [PubMed PMID: 22935809]
Level 2 (mid-level) evidenceGogoulos PP, Sideris G, Nikolopoulos T, Sevastatou EK, Korres G, Delides A. Conservative Otosclerosis Treatment With Sodium Fluoride and Other Modern Formulations: A Systematic Review. Cureus. 2023 Feb:15(2):e34850. doi: 10.7759/cureus.34850. Epub 2023 Feb 10 [PubMed PMID: 36923175]
Level 1 (high-level) evidenceToscano ML, Shermetaro C. Stapedectomy. StatPearls. 2024 Jan:(): [PubMed PMID: 32965876]
Cheng HCS,Agrawal SK,Parnes LS, Stapedectomy Versus Stapedotomy. Otolaryngologic clinics of North America. 2018 Apr; [PubMed PMID: 29397948]
Bajaj Y, Uppal S, Bhatti I, Coatesworth AP. Otosclerosis 3: the surgical management of otosclerosis. International journal of clinical practice. 2010 Mar:64(4):505-10. doi: 10.1111/j.1742-1241.2009.02047.x. Epub [PubMed PMID: 20456195]
McElveen JT Jr, Kutz JW Jr. Controversies in the Evaluation and Management of Otosclerosis. Otolaryngologic clinics of North America. 2018 Apr:51(2):487-499. doi: 10.1016/j.otc.2017.11.017. Epub [PubMed PMID: 29502731]
Redfors YD, Hellgren J, Möller C. Hearing-aid use and benefit: a long-term follow-up in patients undergoing surgery for otosclerosis. International journal of audiology. 2013 Mar:52(3):194-9. doi: 10.3109/14992027.2012.754957. Epub 2013 Jan 22 [PubMed PMID: 23336672]
Level 2 (mid-level) evidenceMahadevaiah A, Parikh B, Kumaraswamy K. Reparative granuloma following stapes surgery. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2007 Dec:59(4):346-8. doi: 10.1007/s12070-007-0098-y. Epub 2007 Dec 11 [PubMed PMID: 23120470]
Searight FT, Singh R, Peterson DC. Otitis Media With Effusion. StatPearls. 2024 Jan:(): [PubMed PMID: 30855877]
Rosario DC, Mendez MD. Chronic Suppurative Otitis. StatPearls. 2024 Jan:(): [PubMed PMID: 32119479]
Park HY, Han DH, Lee JB, Han NS, Choung YH, Park K. Congenital stapes anomalies with normal eardrum. Clinical and experimental otorhinolaryngology. 2009 Mar:2(1):33-8. doi: 10.3342/ceo.2009.2.1.33. Epub 2009 Mar 26 [PubMed PMID: 19434289]
Koenen L, Andaloro C. Meniere Disease. StatPearls. 2025 Jan:(): [PubMed PMID: 30725640]
Gibb AG, Pang YT. Current considerations in the etiology and diagnosis of tympanosclerosis. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 1994:251(8):439-51 [PubMed PMID: 7718216]
Harris JP, Mehta RP, Nadol JB. Malleus fixation: clinical and histopathologic findings. The Annals of otology, rhinology, and laryngology. 2002 Mar:111(3 Pt 1):246-54 [PubMed PMID: 11913685]
Level 2 (mid-level) evidenceCampbell E, Tan NC. Ossicular-Chain Dislocation. StatPearls. 2024 Jan:(): [PubMed PMID: 32809456]
Palma Diaz M, Cisneros Lesser JC, Vega Alarcón A. Superior Semicircular Canal Dehiscence Syndrome - Diagnosis and Surgical Management. International archives of otorhinolaryngology. 2017 Apr:21(2):195-198. doi: 10.1055/s-0037-1599785. Epub [PubMed PMID: 28382131]
Odat H, Kanaan Y, Alali M, Al-Qudah M. Hearing results after stapedotomy for otosclerosis: comparison of prosthesis variables. The Journal of laryngology and otology. 2021 Jan:135(1):28-32. doi: 10.1017/S0022215120002595. Epub 2021 Jan 22 [PubMed PMID: 33478597]
Ramaswamy AT, Lustig LR. Revision Surgery for Otosclerosis. Otolaryngologic clinics of North America. 2018 Apr:51(2):463-474. doi: 10.1016/j.otc.2017.11.014. Epub [PubMed PMID: 29502729]
Vincent R, Sperling NM, Oates J, Jindal M. Surgical findings and long-term hearing results in 3,050 stapedotomies for primary otosclerosis: a prospective study with the otology-neurotology database. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2006 Dec:27(8 Suppl 2):S25-47 [PubMed PMID: 16985478]