Introduction
Os odontoideum is an anatomic anomaly of the upper cervical spine and was first described by Giacomini in 1886 (see Image. Os Odontoideum).[1] Radiologically, this condition is defined as an oval or round-shaped ossicle with smooth circumferential cortical margins, representing a hypoplastic odontoid process (dens) without continuity with the C2 vertebral body.[2][3][4] Typically, the ossicle migrates cranially to the expected position of the odontoid tip and can manifest in 2 anatomical types—an ossicle located in the normal odontoid (orthotopic) position and another near the occiput in the area of the foramen magnum (dystopic).[5][6][7]
Researchers have described radiological dimensions of os odontoideum, with most being approximately half the size of a normal odontoid process. Some are exceptionally small and cephalic, posing challenges for diagnosis via plain x-rays or computed tomography (CT).[4] The ossicle is located slightly posterior and superior to the anterior arch of C1.[8] The os odontoideum is often attached to the anterior arch of C1 through a transverse ligament.
One of the primary risks associated with this anatomical entity is anterior atlantoaxial subluxation, while posterior atlantoaxial subluxation is extremely rare.[9] This instability in the atlantoaxial joint can result in cervical spinal stenosis, leading to cervical myelopathy due to vascular compromise, bony compression, or stretching of the spinal cord.[10]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of this condition remains debated, with 2 prevailing theories—traumatic and congenital—regarding the origin of os odontoideum.
Most studies favor the traumatic theory, considering it an acquired pathology resulting from avascular necrosis caused by an odontoid fracture. This theory purports that the os odontoideum forms after a traumatic event, with the preservation of the blood supply to the fractured odontoid tip; this can occur in the prenatal or postnatal periods and may not be recalled by the patient.[11][12][13][14] There have been case reports documenting the formation of an os odontoideum after trauma in patients with previously documented normal odontoid processes.[15][16][17]
On the other hand, the congenital hypothesis considers it a segmental defect, representing a failed fusion of the odontoid and axis vertebral body,[18][19][20] an incomplete migration of the axis centrum, failure of segmentation, or nontraumatic avascular necrosis.[21] The congenital theory may explain os odontoideum in identical twins without a history of trauma or reports of familial expression.[22][23][11][24] This line of thought is reinforced by Straus et al, who demonstrated trends in gene expression profiles between os odontoideum patients and normal subjects.[25] Certain associations with upper cervical anomalies such as the hypoplastic posterior arch of C1, Klippel-Feil syndrome, trisomy 21 syndrome, Morquio syndrome, or neurofibromatosis also help support this theory.[11]
In pediatrics, awareness of normal embryology and ossification of the odontoid process is critical to reducing the rate of false-positive diagnoses. The apex of the odontoid arises from the fourth occipital sclerotome, the odontoid process and anterior arch of C1 arise from the first cervical sclerotome, and the body of the axis arises from the second sclerotome. Although the apex (ossiculum terminale, secondary ossification center) typically ossifies between the ages of 3 and 6, it does not fuse with the body of the odontoid until a child attains approximately ages 10 to 12. Similarly, the normal sub-dental synchondrosis, situated between the odontoid and the body of C2, typically fuses between the ages of 3 and 8.[22][21][7]
Epidemiology
Os odontoideum is a rare condition with an uncertain estimated prevalence due to the usual asymptomatic course and the absence of large-scale screening studies. This condition is usually found incidentally in the pediatric population or diagnosed in symptomatic patients during adulthood.[4][6] In a retrospective review conducted by Perdikakis et al, examining the magnetic resonance imaging (MRI) of odontoid process configuration in 133 patients aged between 19 and 81, os odontoideum was identified in only one case, representing a prevalence of 0.7%.[26]
Pathophysiology
The ossiculum terminale, or the apical odontoid epiphysis, originates from the fourth occipital sclerotome, while the odontoid and axis bodies develop from the first and second cervical sclerotomes, respectively. The neurocentral synchondrosis is an epiphyseal growth plate, delineating the first and second cervical sclerotomes. Additionally, the subdental synchondrosis, a cartilaginous band, typically exists between the odontoid process and the body of the axis in most children aged 4 and younger, disappearing by around age 8.
The odontoid process depends primarily on the terminal apical arcade for its blood supply, which anastomoses caudally with the deep penetrating branches originating from the posterior ascending arteries, derived from the vertebral artery. Due to the precarious nature of this vascular supply, any insufficiency in the terminal arcade can result in ischemia and necrosis during embryologic development.[27]
History and Physical
Clinical presentation varies, ranging from asymptomatic incidental findings on imaging to neck discomfort or neurological deficits with permanent paralysis in severe cases.[10]
The initial clinical presentation is often nonspecific, with neck pain, shoulder pain, torticollis or headache, and upper extremity paresthesia-like intermittent tingling and numbness in the neck and upper limbs. Other common complaints are lower limb weakness and gait difficulties.[11] These symptoms are thought to result from static or dynamic compression or repeated minor trauma to the spinal cord.[28]
Increased motion at the C1-C2 level can lead to vertebral artery occlusion and ischemia of the brainstem and posterior fossa structures, resulting in seizures, syncope, vertigo, visual disturbances, and even sudden death after minor trauma.[29][30][31][32][33]
During the physical examination, it is expected to find neurological deficits or loss of motor milestones. Hypoesthesia, hyperreflexia (patellar tendon reflex), scapulohumeral (Shimizu) reflex, Tromner reflex, Hoffmann reflex, Babinski reflex, and clonus may be present in chronic spinal cord compression.[6] Spastic or broad-based gait and decreased hand dexterity are signs of myelopathy. All those previous signs and symptoms are nonspecific, and other diagnoses that cause myelopathy should be ruled out.
Evaluation
Early and accurate diagnosis is critical in mitigating morbidity and mortality associated with os odontoideum. Minor trauma in undiagnosed cervical instability can lead to catastrophic neurological outcomes. Therefore, routine anteroposterior and lateral cervical spine radiographs, along with an open-mouth odontoid view, serve as the initial diagnostic approach, facilitating timely identification of the condition.
The lateral radiograph of the cervical spine reveals a posterior widening of the anterior atlantoaxial distance and disruption of the spinolaminar junction line. Additionally, a well-corticated rounded ossicle is observed just dorsal and slightly cranial to the anterior arch of C1 in this projection, with no prevertebral soft tissue widening. Cervical spine flexion-extension radiographs help to determine the degree of atlantoaxial instability.[29] Some authors also perform bedside lateral radiographs during preoperative skull traction, considering them crucial for assessing atlantoaxial joint instability and subluxation, aiding in determining the appropriate surgical approach.[34]
CT images confirm the corticated margin of the ossicle, depicting a shortened odontoid process and a smooth bone ossicle. Additionally, reconstruction of CT images may reveal the congenital incomplete union of the C1 posterior arch.[11] A hypertrophied anterior arch of C1 often suggests underlying chronic instability (see Image. Hypoplastic Odontoid Process).[35] CT scans are also used to assess anatomical landmarks, including the length and direction of the pedicles, as well as vascular anatomy (VA), with particular emphasis on detecting anomalous VA.[34]
MRI reveals fluid within the widened anterior atlantoaxial space, along with a potential focal narrowing of the spinal canal due to the posteriorly tilted odontoid process pressing against the ventral cervical spinal cord. Additionally, areas of increased T2-weighted signal within the central gray matter may be present, indicative of myelomalacia.[10]
Certain measurements obtained from lateral cervical radiographs or sagittal CT reconstruction can assist in defining cervical instability or determining the appropriate surgical approach, as mentioned below.
- The atlanto-dental interval (ADI): ADI refers to the distance between the odontoid process and the posterior border of the anterior arch of the atlas. In adults, an ADI measurement greater than 3.5 mm suggests instability, with values exceeding 10 mm indicating a need for surgery. Conversely, an ADI of up to 5 mm in pediatric patients is considered normal.[6]
- Space-available-cord (SAC) or posterior ADI (PADI): Another important measurement is the SAC or PADI, which refers to the distance between the posterior surface of dens and the anterior surface of the posterior arch of the atlas. In adults, a PADI measurement of less than 14 mm is associated with an elevated risk of neurological injury and warrants consideration for surgical intervention.[36]
Treatment / Management
Treatment options vary from conservative management to surgical intervention, depending on the severity of symptoms and evidence of atlantoaxial instability as assessed through radiological imaging. For asymptomatic patients, an ongoing debate exists regarding the merits of conservative therapies with imaging surveillance versus prophylactic spinal fusion.[10] Regular clinical and radiographic follow-up is advised for those without symptoms and lacking evidence of C1-C2 instability, coupled with avoiding all contact sports to mitigate potential risks.[34](B3)
Asymptomatic patients with radiographic evidence of atlantoaxial instability should consider surgery, although there is a controversy regarding whether C1-C2 fusion can significantly influence patients' neck rotation and daily activities. Although the procedure could induce the loss of normal neck rotation by as much as 50%, the remaining joints could compensate for most of the function of C1-C2. The benefits of avoiding neurological compromise secondary to cord compression outweigh the loss of neck rotation associated with this procedure.[34]
All symptomatic patients are considered candidates for surgery.[10][11][37] Surgery is typically recommended for patients presenting with neurological involvement, regardless of its transient nature, as well as for those exhibiting radiological signs of instability, such as more than 5 mm of translation in flexion and extension x-rays. Additionally, surgical intervention may be warranted in cases of progressive instability or persistent neck pain associated with atlantoaxial instability.[9](B3)
The principles of treatment aim to prevent sudden death from neurological compromise, enhance neurological status, stabilize the cervical spine, and improve the overall quality of life. Treatment strategies for this condition can be outlined in the following 4 steps:
- Identifying the primary pathology contributing to the symptoms of myelopathy, such as the odontoid peg or posterior arch of C1.
- Determining whether the atlantoaxial subluxation is reducible or irreducible.
- Deciding whether decompression of the lesion is necessary.
- Selecting the appropriate surgical option for stabilization and fusion.
Surgical options include atlantoaxial fusion, occiput-C2 fusion, and occiput-C3 fusion.[28][7] The decision depends on spinal cord compression location, area for arthrodesis, and bone quality.[9] All of them can be complemented with an additional transoral decompression in cases of irreducible subluxation of C1–C2.[38][39] However, this procedure often has accompanying complications such as wound infection, cerebrospinal fluid leakage, neurological injury, and hardware loosening.(B2)
In a recent publication, Goel et al. reported a series of 190 patients who were effectively treated with segmental atlantoaxial fixation without bony decompression, including neither trans-oral nor foramen magnum approaches, and without incorporating the occipital bone into the construct.[40] Fusion is indicated in cases of occipito-cervical instability or following unsuccessful attempts at atlantoaxial fusion. Additionally, fusion is suggested for cases involving poor bone quality, as there is an elevated risk of screw pull-out in such instances.[41][42](B2)
Summary of Treatment Options for Os Odontoideum
Treatment options for os odontoideum vary and are tailored depending on the clinical presentation and severity of instability.
- Clinically asymptomatic os odontoideum: Clinically asymptomatic cases may be managed through clinical and radiographic surveillance or, alternatively, posterior C1-C2 internal fixation and fusion.
- Symptomatic os odontoideum or C1-C2 instability: Symptomatic cases or those with C1-C2 instability typically require posterior C1-C2 internal fixation and fusion.
- Infeasibility of achieving rigid C1-C2 fixation: In situations where achieving rigid C1-C2 fixation is not feasible, postoperative halo immobilization may be implemented.
- Os odontoideum with irreducible dorsal cervico-medullary compression: For os odontoideum cases presenting with irreducible dorsal cervico-medullary compression, with or without occipito-atlantal instability, treatment may involve occipital-cervical fixation and fusion, with or without C1 laminectomy.
- Irreducible ventral cervico-medullary compression: Irreducible ventral cervico-medullary compression often necessitates ventral decompression as part of the treatment strategy.
Differential Diagnosis
Os odontoideum is among the causes of atlantoaxial instability and dislocation.[11] The differential diagnoses that can produce similar instability include acute dens fracture (characterized by a thinner and more irregular space, in contrast to the wide and smooth space observed in os odontoideum), abnormalities in dens morphology (such as aplasia of the dens, bifid dens, dens duplicated, and persistent ossiculum terminale),[43] Down syndrome, juvenile rheumatoid arthritis, Klippel–Feil syndrome, Morquio syndrome, neurofibromatosis, normal development in the pediatric population (refer to the Etiology section), rheumatoid arthritis, and transverse ligament injury.
Prognosis
The prognosis of os odontoideum varies depending on symptoms and radiological parameters. C1-C2 instability is defined as greater than 3 mm of anterior displacement of the posterior cortex of the atlas relative to the anterior aspect of the dens in adults and more than 4 mm in children.[6] Greater displacement predicts worse outcomes. The degree of atlantoaxial instability is less sensitive than the absolute diameter of the spinal canal in predicting poor outcomes.[30][2] In addition, a PADI measurement indicating a spinal canal diameter of less than 12 mm predicts paralysis development in all cases of C1-C2 instability.[36]
Complications
Complications of os odontoideum hinge on the severity of cord compression, instability, and unforeseen events, as even minor trauma can result in catastrophic neurological damage, including sudden death. This risk arises from potential C1-C2 instability due to abnormal dens development and dysfunction in the associated atlantoaxial ligamentous complex, stemming from the anomalous position of the free ossicle. Accurate detection of radiological signs of instability is crucial to prevent complications related to spinal cord compression.
Deterrence and Patient Education
When diagnosing symptomatic os odontoideum, surgical intervention should be promptly considered. Conservative treatment options are suitable solely for asymptomatic patients without evidence of atlantoaxial instability. Patients must be informed about the potential catastrophic outcomes associated with this condition. Regular clinical and radiographic monitoring is imperative, and clinicians should strongly advocate avoiding all contact sports. If patients exhibit symptoms related to os odontoideum or radiographic evidence of C1-C2 instability, surgical stabilization is the most suitable treatment option.
Enhancing Healthcare Team Outcomes
Although os odontoideum is a rare diagnosis, timely recognition and accurate identification of both radiological and clinical signs of instability are crucial to prevent catastrophic complications related to spinal cord compression. Following confirmation of the diagnosis, patients and their families should receive comprehensive education from healthcare providers and nurses regarding potential outcomes.
Managing os odontoideum necessitates a team effort among interprofessional healthcare professionals, involving physicians, surgeons, specialists, and specially trained nurses, collaborating across disciplines to attain optimal patient outcomes.
Media
(Click Image to Enlarge)
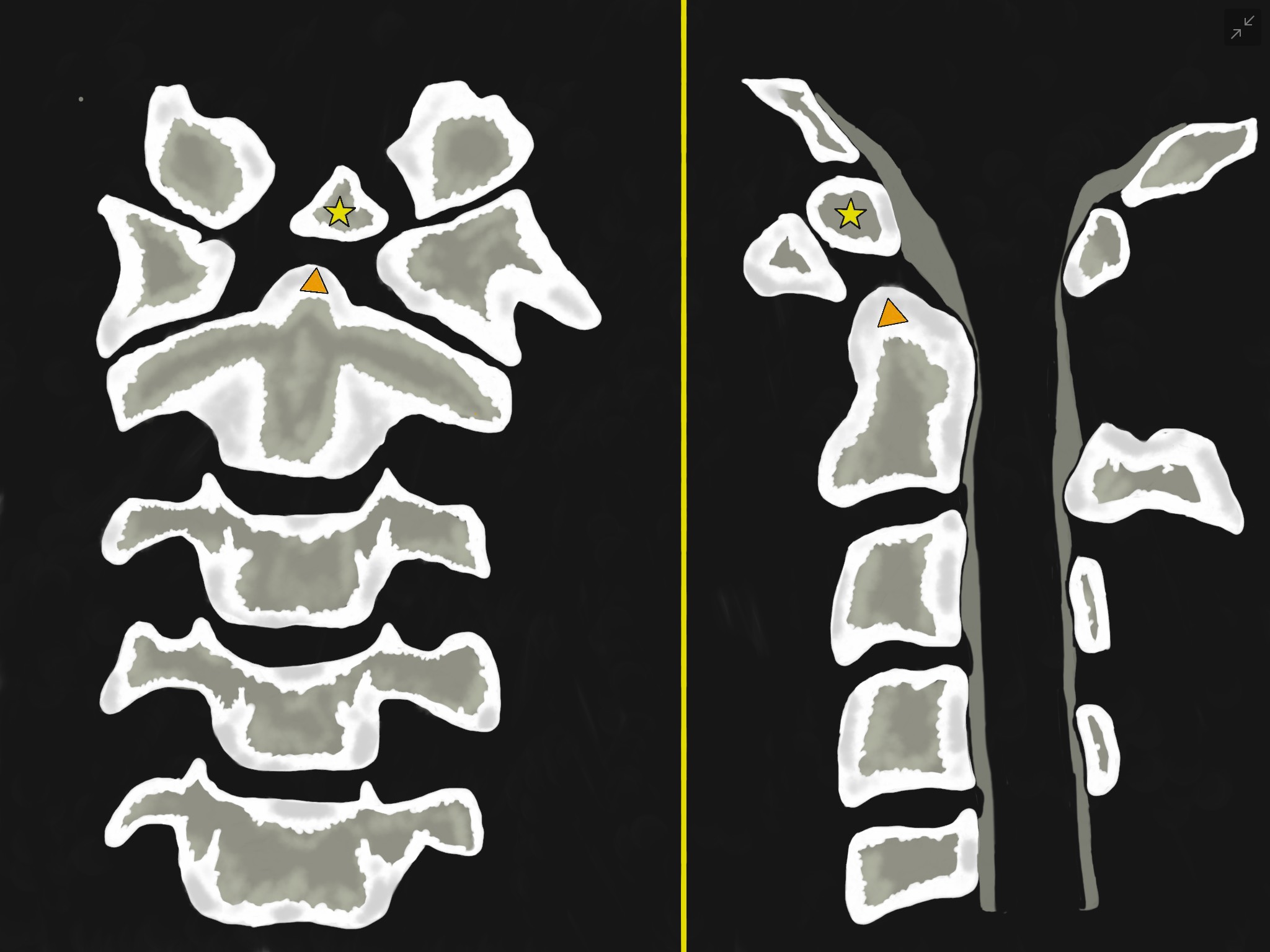
Os Odontoideum. Anterior-posterior (left-sided image) and lateral (Right-sided image) views. They show an oval or round-shaped ossicle with smooth circumferential cortical margins (yellow star) representing a hypoplastic odontoid process (Orange triangle) that has no continuity with the C2 vertebral body. It is often attached to the anterior arch of C1 through an intact transverse ligament.
Contributed by Franco De Cicco, MD
(Click Image to Enlarge)
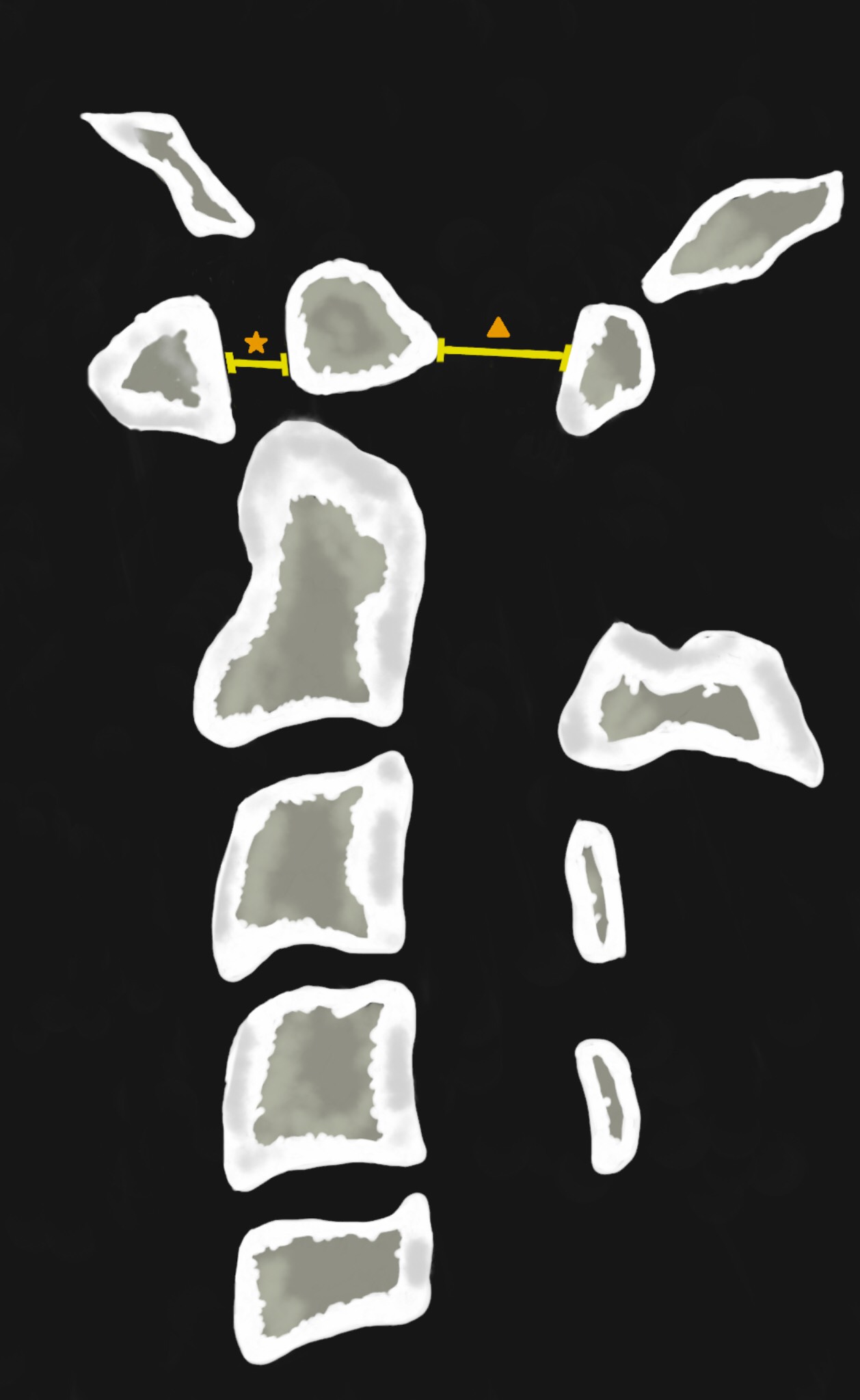
Hypoplastic Odontoid Process. Illustration that represents an upper cervical spine lateral view. It shows an oval or round-shaped ossicle with smooth circumferential cortical margins representing a hypoplastic odontoid process that has no continuity with the C2 vertebral body. The atlanto-dens interval (ADI) (orange star) is the distance between the odontoid process and the posterior border of the anterior arch of the atlas. The space-available-cord (SAC) or posterior atlanto-dens-interval (PADI) (orange triangle) is the distance between the posterior surface of dens and the anterior surface of the posterior arch of the atlas.
Contributed by Franco De Cicco, MD.
References
Perrini P, Montemurro N, Iannelli A. The contribution of Carlo Giacomini (1840-1898): the limbus Giacomini and beyond. Neurosurgery. 2013 Mar:72(3):475-81; discussion 481-2. doi: 10.1227/NEU.0b013e31827fcda3. Epub [PubMed PMID: 23208067]
Spierings EL, Braakman R. The management of os odontoideum. Analysis of 37 cases. The Journal of bone and joint surgery. British volume. 1982:64(4):422-8 [PubMed PMID: 7096415]
Level 3 (low-level) evidenceMatsui H, Imada K, Tsuji H. Radiographic classification of Os odontoideum and its clinical significance. Spine. 1997 Aug 1:22(15):1706-9 [PubMed PMID: 9259779]
Level 3 (low-level) evidenceKlassov Y, Benkovich V, Kramer MM. Post-traumatic os odontoideum - case presentation and literature review. Trauma case reports. 2018 Dec:18():46-51. doi: 10.1016/j.tcr.2018.11.004. Epub 2018 Nov 27 [PubMed PMID: 30533483]
Level 3 (low-level) evidenceArvin B, Fournier-Gosselin MP, Fehlings MG. Os odontoideum: etiology and surgical management. Neurosurgery. 2010 Mar:66(3 Suppl):22-31. doi: 10.1227/01.NEU.0000366113.15248.07. Epub [PubMed PMID: 20173524]
Robson KA. Os odontoideum: rare cervical lesion. The western journal of emergency medicine. 2011 Nov:12(4):520-2. doi: 10.5811/westjem.2011.4.2029. Epub [PubMed PMID: 22224150]
Fielding JW, Hensinger RN, Hawkins RJ. Os Odontoideum. The Journal of bone and joint surgery. American volume. 1980 Apr:62(3):376-83 [PubMed PMID: 7364809]
Hedequist DJ, Mo AZ. Os Odontoideum in Children. The Journal of the American Academy of Orthopaedic Surgeons. 2020 Feb 1:28(3):e100-e107. doi: 10.5435/JAAOS-D-18-00637. Epub [PubMed PMID: 31977608]
Pluemvitayaporn T, Kunakornsawat S, Piyaskulkaew C, Pruttikul P, Pongpinyopap W. Chronic posterior atlantoaxial subluxation associated with os odontoideum: a rare condition. A case report and literature review. Spinal cord series and cases. 2018:4():110. doi: 10.1038/s41394-018-0143-y. Epub 2018 Dec 19 [PubMed PMID: 30588336]
Level 3 (low-level) evidenceNguyen JC, Pollock AN. Os odontoideum. Pediatric emergency care. 2015 Mar:31(3):225-7. doi: 10.1097/PEC.0000000000000411. Epub [PubMed PMID: 25738246]
Level 3 (low-level) evidenceTang X, Tan M, Yi P, Yang F, Hao Q. Atlantoaxial dislocation and os odontoideum in two identical twins: perspectives on etiology. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2018 Jul:27(Suppl 3):259-263. doi: 10.1007/s00586-017-5116-5. Epub 2017 May 15 [PubMed PMID: 28508240]
Level 3 (low-level) evidenceFielding JW, Griffin PP. Os odontoideum: an acquired lesion. The Journal of bone and joint surgery. American volume. 1974 Jan:56(1):187-90 [PubMed PMID: 4812163]
Schuler TC, Kurz L, Thompson DE, Zemenick G, Hensinger RN, Herkowitz HN. Natural history of os odontoideum. Journal of pediatric orthopedics. 1991 Mar-Apr:11(2):222-5 [PubMed PMID: 2010525]
Level 3 (low-level) evidenceVerska JM, Anderson PA. Os odontoideum. A case report of one identical twin. Spine. 1997 Mar 15:22(6):706-9 [PubMed PMID: 9089945]
Level 3 (low-level) evidenceWang S, Wang C. Acquired os odontoideum: a case report and literature review. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2012 Feb:28(2):315-9. doi: 10.1007/s00381-011-1642-3. Epub 2011 Dec 2 [PubMed PMID: 22134416]
Level 3 (low-level) evidenceZygourakis CC, Cahill KS, Proctor MR. Delayed development of os odontoideum after traumatic cervical injury: support for a vascular etiology. Journal of neurosurgery. Pediatrics. 2011 Feb:7(2):201-4. doi: 10.3171/2010.11.PEDS10289. Epub [PubMed PMID: 21284467]
Level 3 (low-level) evidenceWada E, Matsuoka T, Kawai H. Os odontoideum as a consequence of a posttraumatic displaced ossiculum terminale. A case report. The Journal of bone and joint surgery. American volume. 2009 Jul:91(7):1750-4. doi: 10.2106/JBJS.H.01182. Epub [PubMed PMID: 19571099]
Level 3 (low-level) evidenceCurrarino G. Segmentation defect in the midodontoid process and its possible relationship to the congenital type of os odontoideum. Pediatric radiology. 2002 Jan:32(1):34-40 [PubMed PMID: 11819061]
Level 3 (low-level) evidenceFLEMMING C, HODSON CJ. Os odontoideum; a congenital abnormality of the axis; case report. The Journal of bone and joint surgery. British volume. 1955 Nov:37-B(4):622-3 [PubMed PMID: 13271492]
Level 3 (low-level) evidenceEllies DL, Krumlauf R. Bone formation: The nuclear matrix reloaded. Cell. 2006 Jun 2:125(5):840-2 [PubMed PMID: 16751095]
Level 3 (low-level) evidenceMcHugh BJ, Grant RA, Zupon AB, DiLuna ML. Congenital os odontoideum arising from the secondary ossification center without prior fracture. Journal of neurosurgery. Spine. 2012 Dec:17(6):594-7. doi: 10.3171/2012.9.SPINE12824. Epub 2012 Oct 5 [PubMed PMID: 23039156]
Level 3 (low-level) evidenceWhite IK, Mansfield KJ, Fulkerson DH. Sequential imaging demonstrating os odontoideum formation after a fracture through the apical odontoid epiphysis: case report and review of the literature. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2013 Nov:29(11):2111-5. doi: 10.1007/s00381-013-2132-6. Epub 2013 May 7 [PubMed PMID: 23649960]
Level 3 (low-level) evidenceMorgan MK, Onofrio BM, Bender CE. Familial os odontoideum. Case report. Journal of neurosurgery. 1989 Apr:70(4):636-9 [PubMed PMID: 2926504]
Level 3 (low-level) evidenceHadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, Ryken TC. Os odontoideum. Neurosurgery. 2002 Mar:50(3 Suppl):S148-55. doi: 10.1097/00006123-200203001-00023. Epub [PubMed PMID: 12431299]
Straus D, Xu S, Traynelis VC. Os odontoideum in identical twins: Comparative gene expression analysis. Surgical neurology international. 2014:5():37. doi: 10.4103/2152-7806.129259. Epub 2014 Mar 20 [PubMed PMID: 24818044]
Level 2 (mid-level) evidencePerdikakis E, Skoulikaris N. The odontoid process: various configuration types in MR examinations. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2014 May:23(5):1077-83. doi: 10.1007/s00586-013-3135-4. Epub 2013 Dec 24 [PubMed PMID: 24366357]
Level 2 (mid-level) evidenceRaj A, Srivastava SK, Marathe N, Bhosale S, Purohit S. Dystopic Os Odontoideum Causing Cervical Myelopathy: A Rare Case Report and Review of Literature. Asian journal of neurosurgery. 2020 Jan-Mar:15(1):236-240. doi: 10.4103/ajns.AJNS_35_19. Epub 2020 Feb 25 [PubMed PMID: 32181211]
Level 3 (low-level) evidenceShirasaki N, Okada K, Oka S, Hosono N, Yonenobu K, Ono K. Os odontoideum with posterior atlantoaxial instability. Spine. 1991 Jul:16(7):706-15 [PubMed PMID: 1925742]
Level 3 (low-level) evidenceWatanabe M, Toyama Y, Fujimura Y. Atlantoaxial instability in os odontoideum with myelopathy. Spine. 1996 Jun 15:21(12):1435-9 [PubMed PMID: 8792520]
Level 2 (mid-level) evidenceKlimo P Jr, Kan P, Rao G, Apfelbaum R, Brockmeyer D. Os odontoideum: presentation, diagnosis, and treatment in a series of 78 patients. Journal of neurosurgery. Spine. 2008 Oct:9(4):332-42. doi: 10.3171/SPI.2008.9.10.332. Epub [PubMed PMID: 18939918]
Level 2 (mid-level) evidenceDai L, Yuan W, Ni B, Jia L. Os odontoideum: etiology, diagnosis, and management. Surgical neurology. 2000 Feb:53(2):106-8; discussion 108-9 [PubMed PMID: 10713186]
Sasaki H, Itoh T, Takei H, Hayashi M. Os odontoideum with cerebellar infarction: a case report. Spine. 2000 May 1:25(9):1178-81 [PubMed PMID: 10788864]
Level 3 (low-level) evidenceChang H, Park JB, Kim KW, Choi WS. Retro-dental reactive lesions related to development of myelopathy in patients with atlantoaxial instability secondary to Os odontoideum. Spine. 2000 Nov 1:25(21):2777-83 [PubMed PMID: 11064523]
Level 2 (mid-level) evidenceWu X, Wood KB, Gao Y, Li S, Wang J, Ge T, Zhao B, Shao Z, Yang S, Yang C. Surgical strategies for the treatment of os odontoideum with atlantoaxial dislocation. Journal of neurosurgery. Spine. 2018 Feb:28(2):131-139. doi: 10.3171/2017.5.SPINE161211. Epub 2017 Nov 17 [PubMed PMID: 29148933]
Holt RG, Helms CA, Munk PL, Gillespy T 3rd. Hypertrophy of C-1 anterior arch: useful sign to distinguish os odontoideum from acute dens fracture. Radiology. 1989 Oct:173(1):207-9 [PubMed PMID: 2781009]
Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A long-term analysis with predictors of paralysis and recovery. The Journal of bone and joint surgery. American volume. 1993 Sep:75(9):1282-97 [PubMed PMID: 8408150]
Level 2 (mid-level) evidenceStulik J, Vyskocil T, Sebesta P, Kryl J. Atlantoaxial fixation using the polyaxial screw-rod system. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2007 Apr:16(4):479-84 [PubMed PMID: 17051397]
Qureshi MA, Afzal W, Malik AS, Ullah JS, Aebi M. Os-odontoideum leading to atlanto-axial instability--report of surgery in four cases. JPMA. The Journal of the Pakistan Medical Association. 2008 Nov:58(11):640-2 [PubMed PMID: 19024140]
Level 3 (low-level) evidenceSalunke P, Behari S, Kirankumar MV, Sharma MS, Jaiswal AK, Jain VK. Pediatric congenital atlantoaxial dislocation: differences between the irreducible and reducible varieties. Journal of neurosurgery. 2006 Feb:104(2 Suppl):115-22 [PubMed PMID: 16506499]
Level 2 (mid-level) evidenceGoel A, Patil A, Shah A, Dandpat S, Rai S, Ranjan S. Os Odontoideum: Analysis of 190 Surgically Treated Cases. World neurosurgery. 2020 Feb:134():e512-e523. doi: 10.1016/j.wneu.2019.10.107. Epub 2019 Oct 26 [PubMed PMID: 31669688]
Level 3 (low-level) evidenceBourdillon P, Perrin G, Lucas F, Debarge R, Barrey C. C1-C2 stabilization by Harms arthrodesis: indications, technique, complications and outcomes in a prospective 26-case series. Orthopaedics & traumatology, surgery & research : OTSR. 2014 Apr:100(2):221-7. doi: 10.1016/j.otsr.2013.09.019. Epub [PubMed PMID: 24629457]
Level 2 (mid-level) evidenceStock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. Instructional course lectures. 2007:56():319-28 [PubMed PMID: 17472317]
Sánchez-Aparcero B, Alemán I, Botella MC. Fracture of the odontoid process in a male individual from the medieval necropolis of Maro (Málaga, Spain). International journal of paleopathology. 2018 Sep:22():158-162. doi: 10.1016/j.ijpp.2018.02.002. Epub 2018 Feb 16 [PubMed PMID: 30126702]