Introduction
The optic chiasm, or optic chiasma, is the part of the brain where the optic nerves cross and is therefore of primary importance to the visual pathway. It is located at the base of the brain inferior to the hypothalamus, and approximately 10 mm superior to the pituitary gland within the suprasellar cistern. It has important anatomical relationships with the third ventricle, forming part of its anterior floor, and the anterior communicating and anterior cerebral arteries.[1] Being in close proximity to vascular structures and the pituitary gland it is vulnerable to compression from their associated pathologies, and this manifests clinically as visual field loss.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The visual pathway refers to the series of anatomic structures responsible for transporting visual information from the eye to the brain. Most visual information follows the same course throughout the visual pathway:
Retina -> optic nerve (cranial nerve II) -> optic chiasm -> optic tract -> lateral geniculate bodies (majority) + hypothalamus -> optic radiations -> visual cortex[2]
After exiting the orbit, the right and left optic nerves travel posteriorly and intersect at the ventral midline to form the optic chiasm.[3] It is located at the inferior aspect of the forebrain at the base of the hypothalamus, approximately 10 mm superior to the pituitary fossa, also known as the Sella turcica.[4] It is adjacent to the junction of the anterior wall and floor of the third ventricle.[5]
Orientation of Fibers
At the optic chiasm, a proportion of axons from the left and right optic nerves decussate (cross the midline) to join with uncrossed fibers of the contralateral optic nerve. [6] Posterior to the decussation, the newly grouped fibers emerge as the right and left optic tracts. It is named for the characteristic “x”-configuration of this joining and crossing of fibers, resembling the Greek letter chi (χ). [7].
RGC axons remain grouped with other axons from the same retinal quadrant and exit the retina in the same position within the optic nerve; i.e., superior-temporal axons exit the eye within the superior-temporal optic nerve. Within the intracranial optic nerve, macular fibers migrate to the center of the nerve; all other axons remain grouped by quadrant. At the chiasm, decussating axons from the superior-nasal retina travel posteriorly within the chiasm, while those originating from the inferior-nasal retina travel anteriorly.[8]
There has been extensive debate regarding the route of decussating nasal fibers within the chiasm and the existence of physiologic loops of fibers known as the knees of Wilbrand. There are four theoretical “knees”; two anteriorly and two posteriorly. The anterior knees are thought to be formed from inferior-nasal fibers after they cross within the anterior chiasm and travel approximately 4 mm into the contralateral optic nerve before looping back on course to join with the uncrossed temporal RGC axons. In contrast, the posterior knees are thought to result from the looping of superior-nasal fibers into the ipsilateral optic tracts prior to their decussation cross within the posterior aspect of the chiasm.[9]
Some advocates argue that damage to the anterior knee of Wilbrand is the sole explanation for the existence of a junctional scotoma visual field defect. This theory has since been debunked (see Clinical Significance). Recent studies using more advanced neuroimaging techniques have failed to identify the presence of the knees of Wilbrand; much of the literature is shifting towards rejecting its presence in patients without pathology.[10][11] Some, however, still cite its presence as an abnormal sequela of long-term monocular optic neuropathy. Axons rotate 90 degrees as they exit the chiasm and enter the optic tract; inferior RGC axons travel medially within the tract, while superior axons travel laterally.[10]
The proportion of decussating axons is directly related to the position of the eyes and thus varies amongst species. In most species (e.g., chicken), the eyes are positioned laterally with no overlap in the visual field; accordingly, all RGC axons project contralaterally at the chiasm.[12] In some species, however, the eyes are positioned medially, allowing for some overlap in the visual field of the right and left eyes; this area is referred to as the “binocular visual field.” Convergence and divergence eye movements allow both eyes to simultaneously fixate on an object of interest within the binocular visual field. Since the two eyes are separated in space, they will produce slightly differing (or “disparate”) retinal images.[3] The stereopsis hypothesis suggests that this small degree of binocular disparity enhances the ability to estimate the depth and localize an object in the visual field. It is thought that this is an evolutionary advantage allowing for predators to target their prey more accurately. Other theories suggest binocularity enhances motor control and hand-eye coordination.[13]
In humans, the medial location of the eyes results in an overlap of approximately half of the visual field; thus, virtually all temporal nasal fibers decussate to and join the temporal fibers of the contralateral eye.[14][3] Typically, the ratio of crossed to uncrossed fibers is 53:47, although this ratio may vary in some pathological conditions (see “Clinical Significance”).[6] Decussating nasal axons carry information from the temporal visual field and join with non-decussating temporal axons carrying information from the nasal visual field of the same eye. Thus, posterior to the chiasm, the newly grouped axons (known as the optic tracts) carry information from the contralateral eye. For example, axons carrying information from the left visual field exit the chiasm as the right optic tract, and vice versa. The axons traveling within the optic tract travel posteriorly and eventually synapse in one of two locations: (1) the lateral geniculate nucleus (LGN), located in the thalamus, or (2) the superior colliculus. Second-order neurons from the thalamus collectively form the optic radiations and end their journey in the striate visual cortex for integration and interpretation.[14]
Size
Various studies have sought to estimate normal chiasmal size using magnetic resonance imaging (MRI) studies. Measurements are, to some degree, subjective and differ between radiologists; inconsistency amongst studies primarily results from interobserver variability of measurements. Table 1 lists measurements for mean anatomical width, height, and area of the optic chiasm obtained in recent studies.[15][16][17]
|
Table 1. Chiasmal Size Measurements Reported in Various Studies |
|||||
|
Juenger et al. (2020) [18] |
Polat et al. (2020) [17] |
Mncube et al. (2019)[15] |
Wagner et al. (1997) [16] |
Parravano et al. (1993) [19] |
|
|
Mean Width (mm) |
12.23 |
12.93 |
13.63 |
14.0 |
15.0 |
|
Mean Height (mm) |
1.93 |
2.82 |
2.26 |
n/a |
3.5 |
|
Mean Area (mm) |
27.07 |
n/a |
n/a |
43.7 |
n/a |
Studies have found no statistically significant differences in chiasmal size based on gender. Clinically, chiasmal size may indicate pathology (see Clinical Significance).
Embryology
Embryologic development of the visual pathway occurs in an anterior-to-posterior manner. The inner and outer layers of the optic cup are derived from the neuroectoderm. Around 3 to 4 weeks gestation, RPE cells begin to form on the outer layer of the optic cup.[20] They are the first retinal cells to begin development and play a crucial role in the proper differentiation of neural retinal cells later in the later stages of development. Retinal ganglion cells differentiate from the inner neuroblastic layer around week 7 of gestation and develop rapidly.[21] By week 6, their RGC axons begin to migrate towards the LGN with the help of various biochemical “guidance” molecules. Between 7 and 8 weeks gestation, crossed nerve fibers first appear; uncrossed fibers do not develop until about 11 weeks gestation.[20]
Myelination of retinal ganglion cells proceeds in a central-to-peripheral manner. Myelination begins at five months gestation in the LGN, proceeding to the optic tract at six months, optic chiasm at 6 to 7 months, and the optic nerve at eight months.[20]
Blood Supply and Lymphatics
The circle of Willis, otherwise known as the cerebral arterial circle, encircles the optic chiasm. It is composed of anastomoses of blood vessels that communicate the anterior and posterior blood supply of the brain. The following vessels comprise the circle of Willis:
- The left and right anterior cerebral arteries are connected through the anterior communicating artery.
- The left and right internal carotid arteries
- The left and right posterior cerebral arteries
- The left and right posterior communicating arteries, which connect the left and right internal carotid arteries to the left and right posterior cerebral arteries, respectively
Vascular branches from the circle of Willis perfuse the intracranial optic nerve and optic chiasm; however, this arterial network is notoriously complicated. There is minimal literature regarding the specific vascular supply to the optic nerve and chiasm. Understanding the vascular supply in this area has significant clinical relevance in neurosurgery – inadvertent injury to the blood vessels in this area is a common cause of post-surgical morbidity and mortality. Baykal et al. studied the vascular supply to the optic nerve and chiasm (the “opto-chiasmatic area”) to determine which neurosurgical treatment approach is least associated with vascular complications. They organized the optic structures into four zones and determined vascular supply as listed in Table 2.[22]
|
Table 2. Vascular Supply to the Opto-Chiasmatic Area (adapted from Baykal et al.) [22] |
||
|
Zone |
Location |
Vascular Supply |
|
Zone 1A |
Superior surfaces of the optic nerves |
- Proximal segment of the internal carotid artery |
|
Zone 2A |
The superior surface of the optic chiasm |
- Anterior cerebral artery - Anterior communicating artery |
|
Zone 1B |
The inferior surface of the optic nerves |
- Proximal segment of the internal carotid artery - Superior pituitary artery - Posterior communicating artery |
|
Zone 2B |
The inferior surface of the optic chiasm |
- Distal segment of the internal carotid artery - Posterior communicating artery - Anterior choroidal artery |
Surgical Considerations
The optic chiasm may be compressed in a number of intracranial pathologies, causing visual deterioration. Principally pituitary tumors, craniopharyngioma, Rathke's cleft cyst, and meningioma can be responsible for visual deterioration. Rapid visual deterioration indicates emergency surgery, whereas known tumors in this region without acute visual loss may be managed on an elective basis.[23][24][23][25]
Traditional approaches to pathology in this region were via a transcranial fronto-basal interhemispheric approach and a transsphenoidal microsurgical approach.[26][27][28][29] Modern neurosurgical practice, however, is moving towards the increasing use of an extended endonasal endoscopic approach for accessing the parasellar region, including the hypothalamic-pituitary axis, third ventricle, and optic chiasm.[30] The extended endonasal endoscopic approach can provide superior visualization of key parasellar structures in patients where the optic chiasm may be pre-fixed or displaced anteriorly, thus preventing an adequate operative view of the region.[31]
The location of the chiasm relative to the sella turcica is an important consideration when performing neurosurgery in this area. In most patients, the chiasm is situated directly above the diaphragm sella ("normo-fixed"); however, it may be horizontally displaced in some patients. The chiasm is "pre-fixed" when anteriorly displaced and situated superiorly to tuberculum sellae. The chiasm is "post-fixed" when posteriorly displaced and situated superiorly to the dorsum sellae.[4] In a study of adult human cadavers, the chiasm was normo-fixed in 85% of test subjects, while pre-fixed and post-fixed chiasmal anatomy occurred in 7.5% and 8% of patients, respectively.[32] This anatomic relationship may be significant when planning the operative approach to pathology in the parasellar area.[4][32]
Clinical Significance
Chiasmal Syndrome
"Chiasmal syndrome" is an umbrella term for signs and symptoms associated with chiasmal pathology of any etiology. Causes of chiasmal compression include:
- Pituitary macroadenoma (most common)
- Craniopharyngioma
- Meningioma
- Optic nerve glioma
- Pilocytic astrocytoma
- Anterior communicating artery aneurysm
- Internal carotid artery aneurysm[5][33][22]
Clinical findings often overlap despite differing pathological mechanisms. Blurred vision is the most common presenting symptom, followed by peripheral visual field loss. Other findings may include optic disc changes, headache, relative afferent pupillary defect, and reduced color vision.[5] Measurements of chiasmal width have been cited as the most clinically useful marker for optic atrophy and is defined as a width of <13.5 mm.[19]
Standard automated perimetry (SAP) can be used to detect visual field defects that result from lesions in the optic chiasm. Research has found SAP to be more accurate in earlier detection of lesions than Goldmann visual field testing.[34] Chiasmal syndromes may produce different patterns of visual field loss based on the specific part of the chiasm which is affected:
- Bitemporal hemianopsia - bilateral temporal visual field loss that respects the vertical midline. Results from compression of decussating nasal fibers within the chiasm. The “textbook” appearance of this defect is a complete temporal scotoma that is perfectly symmetric between both eyes. Clinically, compressive lesions vary in location and often involve other adjacent axons and/or do not affect all nasal axons. Therefore, bitemporal hemianopsia should not be ruled out even if some of the temporal hemifield is spared or if the defect crosses the vertical midline.[10]
- Junctional scotoma -central scotoma in one eye and temporal field defect (usually superior) in the contralateral eye. Results from compression of the chiasm and ipsilateral pre-chiasmal optic nerve. Most often caused by lateral chiasmal compression secondary to meningioma.[35]
Pituitary Adenoma
Pituitary adenomas are tumors of the pituitary gland, an endocrine organ responsible for the secretion of hormones that regulate growth and the reproductive system. They are generally considered benign but may enlarge over time. Tumors are classified as microadenomas (<10 mm in size) or macroadenomas (>10 mm in size). Larger lesions are more likely to disrupt proximal structures, particularly the optic chiasm superiorly, causing compression of nerve fibers and corresponding visual field loss. Lesions less than 20 mm in size are unlikely to cause visual impairment.[36] Tumors generally initially compress the inferior aspect of the chiasm where superior nasal fibers travel, causing corresponding superior temporal visual field loss.
Over time, slow tumor growth eventually causes compression of the entire chiasm and corresponding bitemporal visual field loss. Magnetic resonance imaging (MRI) is the preferred method of imaging pituitary tumors, determining lesion characteristics, and predicting surgical outcomes. Treatment failure to relieve chiasmal compression is highly likely in large lesions (>40 mm in size) and fibrotic lesions. Conversely, tumors with cystic/necrotic and hemorrhagic components are associated with high success rates of chiasmal decompression.[33]
Optic Nerve Glioma
Glial cells are non-neuronal support cells that provide physical and metabolic support to neurons and play a crucial role in maintaining proper homeostatic balance. They are found within the central nervous system, including the optic nerve. Oligodendrocytes are the primary glial cells in the optic pathway and act to support axons of RGCs as they travel toward the visual cortex. Malignant glial cell tumors (gliomas) of the optic pathway are common in the pediatric population (3 to 5% of all pediatric brain tumors) and are even more common in patients with neurofibromatosis type 1 (6.6 to 20%). Chiasmal gliomas may result in visual field loss (possibly bitemporal hemianopsia), nystagmus, and decreased visual acuity. Chiasmal tumor location poses are uniquely challenging to treat – anatomical proximity to the hypothalamus increases the risk of inadvertent damage and severe complications. Surgery is generally reserved for cases with a high risk of severe vision loss. Other treatment options include chemotherapy, corticosteroids, and radiation. [37]
Ocular Albinism/Oculocutaneous Albinism
Ocular albinism is an X-linked inherited condition resulting from a mutation of the GPR143 gene responsible for the maturation of the protein melanin.[38] Oculocutaneous albinism is an autosomal recessive inherited condition resulting from a mutation in one of the four OCA genes responsible for melanin biosynthesis.[39] These genes are expressed extensively in RPE cells and play a critical role in normal retinal function and development. During embryologic development, abnormal RPE function delays retinal maturation, including proper development of RGCs that travel within the optic nerve and optic chiasm. Normally, non-decussating (ipsilateral) chiasmal fibers develop earlier than decussating (contralateral) fibers; the likelihood of decussation progressively decreases as the gestation time increases; thus, delayed RGCs are more likely to egregiously decussate by the time they reach the chiasm.[38]
Rather than receiving an equal distribution of visual information in both eyes, each brain hemisphere receives abnormal high visual input from the contralateral eye.[12] Abnormal embryologic development and a high ratio of decussating fibers result in characteristic clinical findings such as nystagmus, high refractive error, reduced visual acuity, reduced depth perception, foveal hypoplasia, and “blonde” (lightly pigmented) fundus appearance.[38][39]
Achiasmia
Although its name suggests the complete absence of the optic chiasm, achiasmia describes a congenital reduction in the number of decussating fibers within the optic chiasm. The complete absence of the optic chiasm is more appropriately termed chiasmal aplasia. The pathogenesis of achiasmia is thought to result from abnormalities in the biochemical molecules responsible for axonal guidance during development (see Embryology section). Clinical findings include reduced visual acuity, stereopsis, and seesaw nystagmus; visual fields and optic nerve appearance are normal.[12][40] Chiasmal hypoplasia often (but not always) coexists with optic nerve hypoplasia. Reduced chiasmal size can be appreciated with neuroimaging studies. Monocular visually evoked potentials (VEPs) reveal a characteristic pattern of asymmetry in response to a flash of light.[40]
Non-Decussating Retinal Fugal Fibre Syndrome (NDRFFS)
A congenital condition resulting from the isolated absence of decussating chiasmal fibers. It is characterized by combined horizontal and see-saw nystagmus and abnormal asymmetry in monocular VEP (similar to achiasmia).[40]
Media
(Click Image to Enlarge)
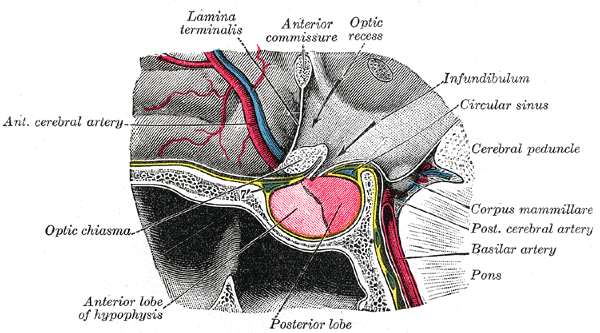
The Fore-brain or Prosencephalon, The hypophysis cerebral; sagittal section, Lamina Terminalis, Optic Recess, Infundibulum, Posterior and Anterior lobe of the Hypophysis, Optic Chiasma, Pons,
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
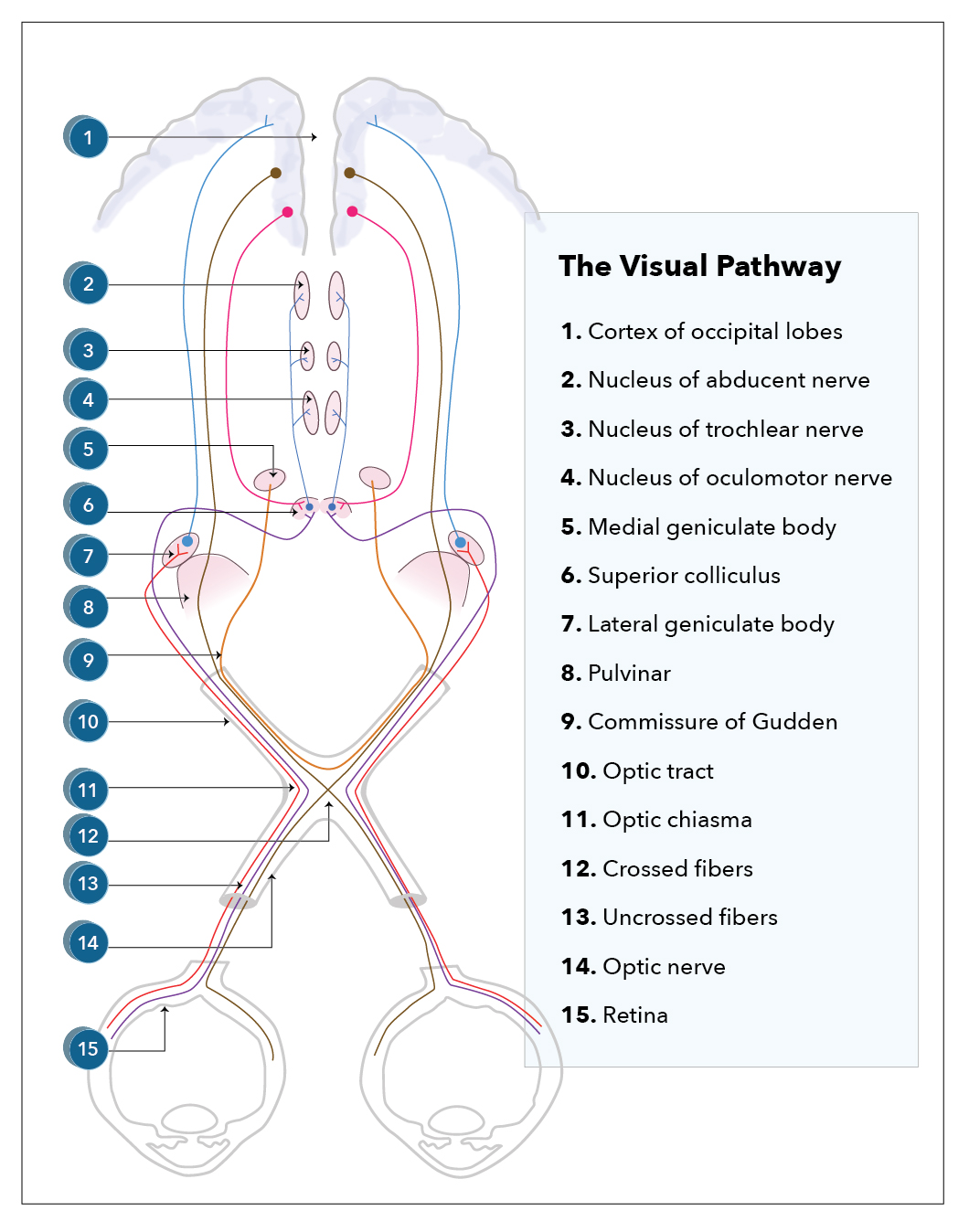
Visual Pathway
Contributed by Katherine Humphreys
(Click Image to Enlarge)
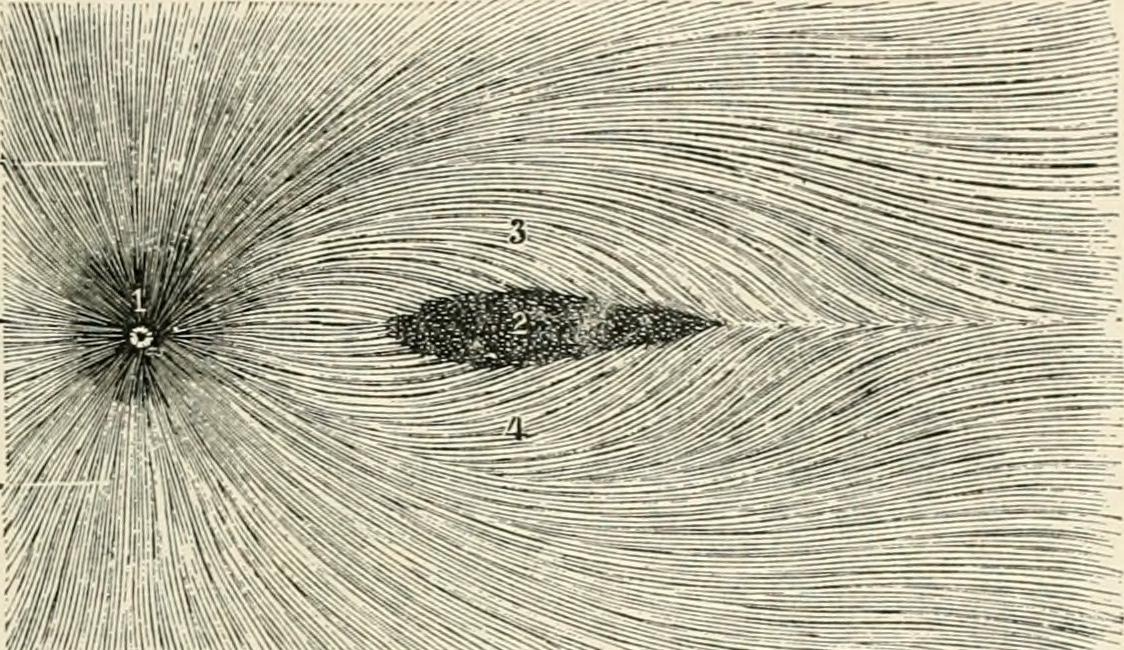
Radiation of retinal nerve fibers in retina Internet Archive Book Images, No restrictions, via Wikimedia Commons
(Click Image to Enlarge)
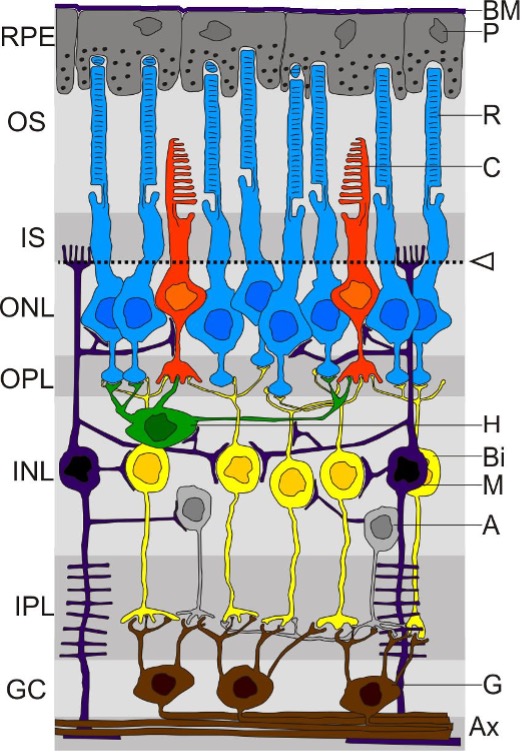
Diagram of retinal layers Contributed From Wikimedia By Hartpete, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=4557528
(Click Image to Enlarge)
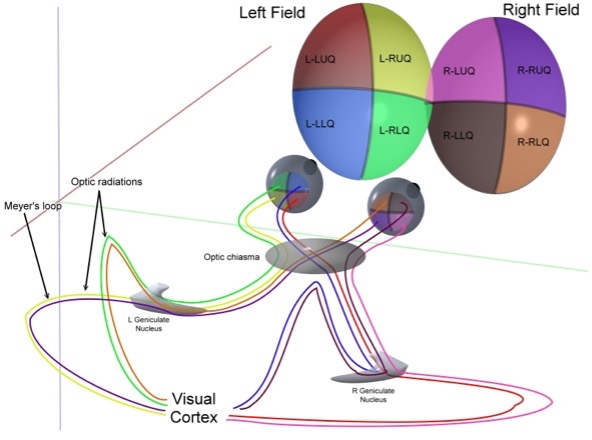
Projection of optic nerve fibers from the visual field to the visual cortex Contributed From Wikimedia By Ratznium at en.wikipedia, CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=3199004
References
Najera E, Truong HQ, Belo JTA, Borghei-Razavi H, Gardner PA, Fernandez-Miranda J. Proximal Branches of the Anterior Cerebral Artery: Anatomic Study and Applications to Endoscopic Endonasal Surgery. Operative neurosurgery (Hagerstown, Md.). 2019 Jun 1:16(6):734-742. doi: 10.1093/ons/opy308. Epub [PubMed PMID: 30649510]
Costello F. The afferent visual pathway: designing a structural-functional paradigm of multiple sclerosis. ISRN neurology. 2013:2013():134858. doi: 10.1155/2013/134858. Epub 2013 Nov 6 [PubMed PMID: 24288622]
Murcia-Belmonte V, Erskine L. Wiring the Binocular Visual Pathways. International journal of molecular sciences. 2019 Jul 4:20(13):. doi: 10.3390/ijms20133282. Epub 2019 Jul 4 [PubMed PMID: 31277365]
Gulsen S, Dinc AH, Unal M, Cantürk N, Altinors N. Characterization of the anatomic location of the pituitary stalk and its relationship to the dorsum sellae, tuberculum sellae and chiasmatic cistern. Journal of Korean Neurosurgical Society. 2010 Mar:47(3):169-73. doi: 10.3340/jkns.2010.47.3.169. Epub 2010 Mar 31 [PubMed PMID: 20379467]
Astorga-Carballo A, Serna-Ojeda JC, Camargo-Suarez MF. Chiasmal syndrome: Clinical characteristics in patients attending an ophthalmological center. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2017 Oct-Dec:31(4):229-233. doi: 10.1016/j.sjopt.2017.08.004. Epub 2017 Sep 6 [PubMed PMID: 29234224]
Takizawa G, Miki A, Maeda F, Goto K, Araki S, Yamashita T, Ieki Y, Kiryu J, Yaoeda K. Relative Afferent Pupillary Defects in Homonymous Visual Field Defects Caused by Stroke of the Occipital Lobe Using Pupillometer. Neuro-ophthalmology (Aeolus Press). 2018 Jun:42(3):139-145. doi: 10.1080/01658107.2017.1367012. Epub 2017 Aug 31 [PubMed PMID: 29796045]
Costea CF, Turliuc Ş, Buzdugă C, Cucu AI, Dumitrescu GF, Sava A, Turliuc MD. The history of optic chiasm from antiquity to the twentieth century. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2017 Nov:33(11):1889-1898. doi: 10.1007/s00381-017-3564-1. Epub 2017 Aug 14 [PubMed PMID: 28808784]
Jain NS, Jain SV, Wang X, Neely AJ, Tahtali M, Jain S, Lueck CJ. Visualization of Nerve Fiber Orientations in the Human Optic Chiasm Using Photomicrographic Image Analysis. Investigative ophthalmology & visual science. 2015 Oct:56(11):6734-9. doi: 10.1167/iovs.15-17443. Epub [PubMed PMID: 26567784]
HOYT WF, LUIS O. Visual fiber anatomy in the infrageniculate pathway of the primate. Archives of ophthalmology (Chicago, Ill. : 1960). 1962 Jul:68():94-106 [PubMed PMID: 14449443]
Level 3 (low-level) evidenceHorton JC. Wilbrand's Knee: To Be or Not to Be a Knee? Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2020 Sep:40 Suppl 1(Suppl 1):S7-S14. doi: 10.1097/WNO.0000000000000988. Epub [PubMed PMID: 32796340]
Grzybowski A, Kanclerz P. The Wilbrand's knee does not exist in the optic chiasm. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2018 Nov:34(11):2133. doi: 10.1007/s00381-018-3969-5. Epub 2018 Sep 8 [PubMed PMID: 30196392]
Prieur DS, Rebsam A. Retinal axon guidance at the midline: Chiasmatic misrouting and consequences. Developmental neurobiology. 2017 Jul:77(7):844-860. doi: 10.1002/dneu.22473. Epub 2017 Feb 12 [PubMed PMID: 27907266]
Larsson M. The optic chiasm: a turning point in the evolution of eye/hand coordination. Frontiers in zoology. 2013 Jul 18:10(1):41. doi: 10.1186/1742-9994-10-41. Epub 2013 Jul 18 [PubMed PMID: 23866932]
Erskine L, Herrera E. Connecting the retina to the brain. ASN neuro. 2014:6(6):. doi: 10.1177/1759091414562107. Epub 2014 Dec 12 [PubMed PMID: 25504540]
Level 3 (low-level) evidenceMncube SS,Goodier MD, Normal measurements of the optic nerve, optic nerve sheath and optic chiasm in the adult population. SA journal of radiology. 2019; [PubMed PMID: 31754545]
Wagner AL, Murtagh FR, Hazlett KS, Arrington JA. Measurement of the normal optic chiasm on coronal MR images. AJNR. American journal of neuroradiology. 1997 Apr:18(4):723-6 [PubMed PMID: 9127037]
Level 2 (mid-level) evidencePolat SÖ, Öksüzler FY, Öksüzler M, Uygur AG, Yücel AH. The determination of the pituitary gland, optic chiasm, and intercavernous distance measurements in healthy subjects according to age and gender. Folia morphologica. 2020:79(1):28-35. doi: 10.5603/FM.a2019.0058. Epub 2019 May 20 [PubMed PMID: 31106844]
Juenger V, Cooper G, Chien C, Chikermane M, Oertel FC, Zimmermann H, Ruprecht K, Jarius S, Siebert N, Kuchling J, Papadopoulou A, Asseyer S, Bellmann-Strobl J, Paul F, Brandt AU, Scheel M. Optic chiasm measurements may be useful markers of anterior optic pathway degeneration in neuromyelitis optica spectrum disorders. European radiology. 2020 Sep:30(9):5048-5058. doi: 10.1007/s00330-020-06859-w. Epub 2020 Apr 26 [PubMed PMID: 32335748]
Parravano JG, Toledo A, Kucharczyk W. Dimensions of the optic nerves, chiasm, and tracts: MR quantitative comparison between patients with optic atrophy and normals. Journal of computer assisted tomography. 1993 Sep-Oct:17(5):688-90 [PubMed PMID: 8370820]
Edward DP, Kaufman LM. Anatomy, development, and physiology of the visual system. Pediatric clinics of North America. 2003 Feb:50(1):1-23 [PubMed PMID: 12713101]
Fuhrmann S, Zou C, Levine EM. Retinal pigment epithelium development, plasticity, and tissue homeostasis. Experimental eye research. 2014 Jun:123():141-50. doi: 10.1016/j.exer.2013.09.003. Epub 2013 Sep 21 [PubMed PMID: 24060344]
Level 3 (low-level) evidenceBaykal D, Yilmazlar S, Fedakar R. A neurosurgical assessment of the blood supply in the optochiasmatic system: a cadaveric-anatomic study. Anatomical science international. 2021 Mar:96(2):294-300. doi: 10.1007/s12565-020-00595-3. Epub 2021 Jan 5 [PubMed PMID: 33400249]
Müller HL, Merchant TE, Warmuth-Metz M, Martinez-Barbera JP, Puget S. Craniopharyngioma. Nature reviews. Disease primers. 2019 Nov 7:5(1):75. doi: 10.1038/s41572-019-0125-9. Epub 2019 Nov 7 [PubMed PMID: 31699993]
Takahashi M, Goseki T, Ishikawa H, Hiroyasu G, Hirasawa K, Shoji N. Compressive Lesions of the Optic Chiasm: Subjective Symptoms and Visual Field Diagnostic Criteria. Neuro-ophthalmology (Aeolus Press). 2018 Dec:42(6):343-348. doi: 10.1080/01658107.2018.1438477. Epub 2018 Sep 11 [PubMed PMID: 30524487]
Raverot G, Burman P, McCormack A, Heaney A, Petersenn S, Popovic V, Trouillas J, Dekkers OM, European Society of Endocrinology. European Society of Endocrinology Clinical Practice Guidelines for the management of aggressive pituitary tumours and carcinomas. European journal of endocrinology. 2018 Jan:178(1):G1-G24. doi: 10.1530/EJE-17-0796. Epub 2017 Oct 18 [PubMed PMID: 29046323]
Level 1 (high-level) evidenceShirane R, Hayashi T, Tominaga T. Fronto-basal interhemispheric approach for craniopharyngiomas extending outside the suprasellar cistern. Child's nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery. 2005 Aug:21(8-9):669-78 [PubMed PMID: 16034620]
Ganna A, Dehdashti AR, Karabatsou K, Gentili F. Fronto-basal interhemispheric approach for tuberculum sellae meningiomas; long-term visual outcome. British journal of neurosurgery. 2009 Aug:23(4):422-30. doi: 10.1080/02688690902968836. Epub [PubMed PMID: 19637015]
Level 2 (mid-level) evidenceKaptain GJ, Vincent DA, Sheehan JP, Laws ER Jr. Transsphenoidal approaches for the extracapsular resection of midline suprasellar and anterior cranial base lesions. Neurosurgery. 2008 Jun:62(6 Suppl 3):1264-71. doi: 10.1227/01.neu.0000333791.29091.83. Epub [PubMed PMID: 18695546]
Maira G, Anile C, Albanese A, Cabezas D, Pardi F, Vignati A. The role of transsphenoidal surgery in the treatment of craniopharyngiomas. Journal of neurosurgery. 2004 Mar:100(3):445-51 [PubMed PMID: 15035280]
Sankhla SK, Jayashankar N, Khan GM. Extended endoscopic endonasal transsphenoidal approach for retrochiasmatic craniopharyngioma: Surgical technique and results. Journal of pediatric neurosciences. 2015 Oct-Dec:10(4):308-16. doi: 10.4103/1817-1745.174457. Epub [PubMed PMID: 26962333]
Liu JK, Christiano LD, Gupta G, Carmel PW. Surgical nuances for removal of retrochiasmatic craniopharyngiomas via the transbasal subfrontal translamina terminalis approach. Neurosurgical focus. 2010 Apr:28(4):E6. doi: 10.3171/2010.1.FOCUS09309. Epub [PubMed PMID: 20367363]
Level 3 (low-level) evidenceGriessenauer CJ, Raborn J, Mortazavi MM, Tubbs RS, Cohen-Gadol AA. Relationship between the pituitary stalk angle in prefixed, normal, and postfixed optic chiasmata: an anatomic study with microsurgical application. Acta neurochirurgica. 2014 Jan:156(1):147-51. doi: 10.1007/s00701-013-1944-1. Epub 2013 Nov 28 [PubMed PMID: 24287682]
Tantiwongkosi B, Mafee MF. Imaging of Optic Neuropathy and Chiasmal Syndromes. Neuroimaging clinics of North America. 2015 Aug:25(3):395-410. doi: 10.1016/j.nic.2015.05.004. Epub [PubMed PMID: 26208416]
Kedar S, Ghate D, Corbett JJ. Visual fields in neuro-ophthalmology. Indian journal of ophthalmology. 2011 Mar-Apr:59(2):103-9. doi: 10.4103/0301-4738.77013. Epub [PubMed PMID: 21350279]
Shin WJ, Song BJ, Kim JM. Junctional scotoma in giant cerebral aneurysm. Korean journal of ophthalmology : KJO. 2002 Dec:16(2):124-9 [PubMed PMID: 12546452]
Level 3 (low-level) evidenceHo RW, Huang HM, Ho JT. The influence of pituitary adenoma size on vision and visual outcomes after trans-sphenoidal adenectomy: a report of 78 cases. Journal of Korean Neurosurgical Society. 2015 Jan:57(1):23-31. doi: 10.3340/jkns.2015.57.1.23. Epub 2015 Jan 31 [PubMed PMID: 25674340]
Level 3 (low-level) evidenceFried I, Tabori U, Tihan T, Reginald A, Bouffet E. Optic pathway gliomas: a review. CNS oncology. 2013 Mar:2(2):143-59. doi: 10.2217/cns.12.47. Epub [PubMed PMID: 25057976]
De Silva SR, Arno G, Robson AG, Fakin A, Pontikos N, Mohamed MD, Bird AC, Moore AT, Michaelides M, Webster AR, Mahroo OA. The X-linked retinopathies: Physiological insights, pathogenic mechanisms, phenotypic features and novel therapies. Progress in retinal and eye research. 2021 May:82():100898. doi: 10.1016/j.preteyeres.2020.100898. Epub 2020 Aug 26 [PubMed PMID: 32860923]
Grønskov K, Ek J, Brondum-Nielsen K. Oculocutaneous albinism. Orphanet journal of rare diseases. 2007 Nov 2:2():43 [PubMed PMID: 17980020]
Sami DA, Saunders D, Thompson DA, Russell-Eggitt IM, Nischal KK, Jeffrey G, Dattani M, Clement RA, Liasis A, Taylor DS. The achiasmia spectrum: congenitally reduced chiasmal decussation. The British journal of ophthalmology. 2005 Oct:89(10):1311-7 [PubMed PMID: 16170123]
Level 2 (mid-level) evidence