Introduction
The supraorbital nerve block is a procedure performed to provide immediate localized anesthesia for a multitude of injuries such as complex lacerations to the forehead, upper eyelid laceration repair, debridement of abrasions, or burns to the forehead, removal of foreign bodies, or pain relief from acute herpes zoster. A regional block allows for minimal anesthetic use, which permits the operator to obtain the intended anesthesia over a larger surface area versus that of local infiltration. The smaller anesthetic volume used also allows for minimal dissemination of anesthetic into tissues, which will prevent the distortion of normal anatomy during the intended procedure.[1] This procedure requires knowledge of appropriate anatomical landmarks and minimal equipment.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The recognition of the appropriate anatomy for this procedure is critical, as it is landmark-based. The supraorbital nerve is one of the terminal branches of the trigeminal nerve. The trigeminal nerve divides into three branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3).[2] The supraorbital nerve is a branch of the ophthalmic nerve. This sensory nerve branches into two separate terminal branches, known as the smaller supratrochlear nerve and the larger supraorbital nerve. The supraorbital nerve exits the cranium through an opening above the orbit known as the supraorbital notch or supraorbital foramen which lies within the medial one-third of the supraorbital margin, 2 to 3 cm lateral to the midline. The nerve then ascends the forehead and terminates at the region of the anterior scalp, thus providing sensory input for tissues up to the region of the lambdoidal suture (connection of the parietal and occipital bones). The supratrochlear nerve provides sensory information in a small area that is close to the midline. The supraorbital foramen can be visually identified by having the patient look straight ahead and then transect the pupil at the level of the patient’s orbital ridge. Palpation of this region reveals the area of interest for performing this nerve block.[3][4][5] A majority of supraorbital nerve exits existed as notches (73.8%) and the rest as foramina (26.2%).[6] Accessory exits were seen in 18.9% of skulls. Of the skulls examined, 55.1% displayed bilateral supraorbital notches, 8.6% had bilateral supraorbital foramina, and 36.3% had a notch on one side and a foramen on the contralateral side.[6]
Beyond the orbital rim, the supraorbital nerve has two consistently present divisions: (1) a superficial (medial) division that passes over the frontalis muscle, providing sensory supply to the forehead skin and only to the anterior margin of the scalp; and (2) a deep (lateral) division that runs cephalad across the lateral forehead between the galea aponeurotica and the pericranium as the sensory nerve to the frontoparietal scalp.[7]
Patients with supraorbital neuralgia present with pain, tenderness, hypoesthesia, and allodynia in the territory supplied by the affected nerve. Fractures of the orbital roof, blunt trauma to the face, tumors of the orbit, and tight swimming goggles and motorcycle helmets can cause supraorbital nerve entrapment.
Indications
Indications for supraorbital nerve block encompass procedures of the forehead near the ipsilateral side of injection and at the anterior aspect of the scalp which may include:
- Debridement of burns or abrasions[8]
- Immediate relief of acute pain from herpes zoster[9]
- Postherpetic itch[10]
- Repair of complex lacerations[8]
- Removal of foreign bodies[8]
- Migraine (episodic and chronic)[11][12][13]
- Neuralgia (supratrochlear or supraorbital)[12][14][15]
- Trigeminal neuralgia[5][16]
- Cluster headache[12]
- Trabeculectomy surgery[17]
- Upper eyelid surgery[4]
- Oculoplastic surgery[18]
- Awake craniotomy[19][20]
- Cranial fixation and stereotactic frames placement[21]
- Hemicrania continua [22]
- Dermatologic/oncologic procedures[23]
Contraindications
Contraindications to the supraorbital nerve block include:
- Refusal of the patient
- Distortion of anatomical landmarks
- Overlying infection at the site of injection
- Allergy to local anesthetics
Equipment
Required equipment for the supraorbital nerve block include:
- Anesthetic agent: the choice of an anesthetic agent depends on the patient’s reported allergies and the intended duration of the nerve block. Lidocaine for up to 90-minutes of local anesthesia, bupivacaine for up to 8 hours of local anesthesia, and tetracaine for up to 3 hours of local anesthesia.
- Consider local diphenhydramine if the patient is allergic to both amides and esters local anesthetics.
- 25 ga needle for adults, 30 ga needle for pediatrics
- 5-10 mL syringe
- Skin cleansing agents such as chlorhexidine or betadine
- Access to lipid emulsion solution in case of local anesthetic systemic toxicity
- Ultrasound if desired for guided injection
Preparation
Prior to starting the procedure, one should educate the patient regarding the risks and benefits of the supraorbital nerve block and then obtain informed consent from the patient. One should then bring all necessary equipment to the bedside and prepare the materials for the procedure.
When lidocaine is combined with epinephrine, the maximum amount that the patient can be given 7 mg/kg per dose. The total dosage of lidocaine with epinephrine given should not exceed 500 mg total. When lidocaine is given without epinephrine the patient can be given 4.5 mg/kg per dose, not to exceed 300 mg total.
When bupivacaine is combined with epinephrine, the maximum amount that the patient can be given is 3 mg/kg per dose. The total dosage of bupivacaine with epinephrine given should not exceed 225 mg per dose with a maximum dose of 400 mg/24h. When bupivacaine is given without epinephrine the maximum amount that the patient can be given is 2.5 mg/kg per dose, not to exceed 175 mg per dose with a maximum of 400 mg/24h.
Technique or Treatment
The supraorbital nerve block procedure utilizes the following steps:
- Identify appropriate landmarks
- Using an aseptic technique clean the injection area using a skin cleansing agent
- Place the patient in a supine position
- From a position lateral to the patient’s head, insert a 25-30-gauge needle in a medial and cephalad direction into the inferior edge of the supraorbital ridge approximately 0.5 cm below the supraorbital notch
- Advance the needle slightly being careful not to penetrate the supraorbital foramen
- Perform a test aspirate
- Inject 0.5-1 mL of the local anesthetic solution to form a subcutaneous wheal and then continue to inject 1-3 mL of local anesthetic
- Firmly place a small roll of gauze above the orbital rim to prevent ballooning of anesthetic at the superior aspect of the eyelid
Due to the various branching of the ophthalmic nerve, the nerve block may not be successful after the first attempt. Injection of additional local anesthetic medial and laterally along the orbital rim will adequately reach all nerve branches.[4]
Complications
Complications of the supraorbital nerve block may include:
- Formation of hematoma or eyelid swelling
- Delayed periorbital ecchymosis
- Infection
- Bleeding
- Vascular injection of anesthetic
- Nerve injury including neurapraxia or neurolysis
- Local anesthetic systemic toxicity
- Allergic reaction to the local anesthetic
Clinical Significance
There are numerous ways in which to provide anesthesia to patients that are in pain so that they may obtain relief. Aside from the management of pain, this anesthesia will also allow the clinician to perform procedures effectively and prevent further discomfort to the patient. A method of providing this anesthesia resides in the form of targeting tissues or a peripheral nerve itself, both of which propagate signals of pain from tissues to the brain and brainstem.
Adequate anesthesia may be accomplished by the local infiltration of an anesthetic directly into a tissue, or in a targeted manner such as a nerve block. Local infiltration of an anesthetic agent allows for the repair of simple injuries to a given anatomic location, but its use is limited in those who have suffered injuries to a larger surface area or have multiple separated injuries. Additionally, local infiltration of a wound may distort the area of repair. In such cases, a nerve block is an option to provide a larger region of anesthesia with a smaller relative amount of anesthetic.[24]
Enhancing Healthcare Team Outcomes
The supraorbital nerve block is a procedure best performed with a group of professionals in the healthcare team, which includes a physician or midlevel provider, nursing staff, and a pharmacist. The staff must elicit a full history and physical exam including a history of adverse drug reactions, in particular, prior history of local anesthetic use to identify alternatives if needed. Approaching this procedure in a team-based manner will help to limit adverse events. The interprofessional team paradigm is optimally suited to manage these cases, leading to better outcomes via coordination and communication between clinicians, nursing, pharmacists, and other ancillary personnel. [Level 5]
The following list should be assessed and adequate provisions identified before the start of the procedure:
- Assessment of any adverse events that the patient may have had to local anesthetics
- Calculation of maximum weight-based dosage of chosen local anesthetic
- Consultation with a pharmacist about the availability of a lipid emulsifying agent in the event of local anesthetic systemic toxicity
- Patient monitoring for signs and symptoms of local anesthetic systemic toxicity such as the perception of a metallic taste, altered mental status, respiratory distress, seizures, tachycardia, dysrhythmia, atrioventricular block, or cardiovascular collapse.[25] [Level 3]
- Availability of staff trained in advanced cardiac life support in the event of cardiovascular symptoms or emergency.
Media
(Click Image to Enlarge)
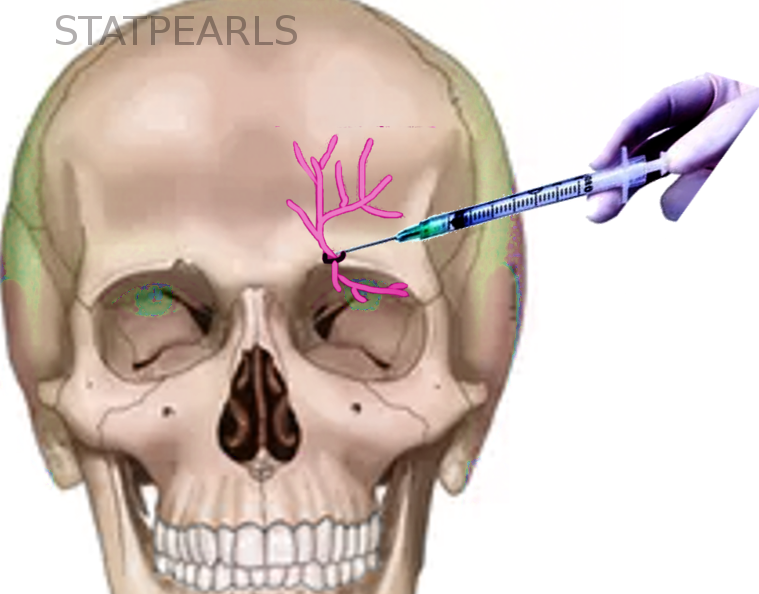
Supraorbital Nerve Block
Courtesy of S Bhimji MD
References
De Buck F, Devroe S, Missant C, Van de Velde M. Regional anesthesia outside the operating room: indications and techniques. Current opinion in anaesthesiology. 2012 Aug:25(4):501-7. doi: 10.1097/ACO.0b013e3283556f58. Epub [PubMed PMID: 22673788]
Level 3 (low-level) evidenceJoo W, Yoshioka F, Funaki T, Mizokami K, Rhoton AL Jr. Microsurgical anatomy of the trigeminal nerve. Clinical anatomy (New York, N.Y.). 2014 Jan:27(1):61-88. doi: 10.1002/ca.22330. Epub 2013 Dec 9 [PubMed PMID: 24323792]
Tomaszewska A, Kwiatkowska B, Jankauskas R. The localization of the supraorbital notch or foramen is crucial for headache and supraorbital neuralgia avoiding and treatment. Anatomical record (Hoboken, N.J. : 2007). 2012 Sep:295(9):1494-503. doi: 10.1002/ar.22534. Epub 2012 Jul 16 [PubMed PMID: 22807312]
Shin KJ, Shin HJ, Lee SH, Song WC, Koh KS, Gil YC. Emerging Points of the Supraorbital and Supratrochlear Nerves in the Supraorbital Margin With Reference to the Lacrimal Caruncle: Implications for Regional Nerve Block in Upper Eyelid and Dermatologic Surgery. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.]. 2016 Aug:42(8):992-8. doi: 10.1097/DSS.0000000000000818. Epub [PubMed PMID: 27355574]
Allam AE, Khalil AAF, Eltawab BA, Wu WT, Chang KV. Ultrasound-Guided Intervention for Treatment of Trigeminal Neuralgia: An Updated Review of Anatomy and Techniques. Pain research & management. 2018:2018():5480728. doi: 10.1155/2018/5480728. Epub 2018 Apr 2 [PubMed PMID: 29808105]
Nanayakkara D, Manawaratne R, Sampath H, Vadysinghe A, Peiris R. Supraorbital nerve exits: positional variations and localization relative to surgical landmarks. Anatomy & cell biology. 2018 Mar:51(1):19-24. doi: 10.5115/acb.2018.51.1.19. Epub 2018 Mar 28 [PubMed PMID: 29644106]
Knize DM. A study of the supraorbital nerve. Plastic and reconstructive surgery. 1995 Sep:96(3):564-9 [PubMed PMID: 7638280]
Ferrera PC, Chandler R. Anesthesia in the emergency setting: Part II. Head and neck, eye and rib injuries. American family physician. 1994 Sep 15:50(4):797-800 [PubMed PMID: 8079909]
Eker HE, Yalçın Çok O, Açıl M, Ülger H, Arıboğan A. [Modified van-Lint technique for the management of postherpetic neuralgia: case report]. Agri : Agri (Algoloji) Dernegi'nin Yayin organidir = The journal of the Turkish Society of Algology. 2011 Apr:23(2):84-7 [PubMed PMID: 21644109]
Level 3 (low-level) evidenceYamanaka D, Kawano T, Shigematsu-Locatelli M, Nishigaki A, Kitamura S, Aoyama B, Tateiwa H, Kitaoka N, Yokoyama M. Peripheral nerve block with a high concentration of tetracaine dissolved in bupivacaine for intractable post-herpetic itch: a case report. JA clinical reports. 2016:2(1):43. doi: 10.1186/s40981-016-0069-y. Epub 2016 Dec 5 [PubMed PMID: 29492438]
Level 3 (low-level) evidenceÖzer D, Bölük C, Türk Börü Ü, Altun D, Taşdemir M, Köseoğlu Toksoy C. Greater occipital and supraorbital nerve blockade for the preventive treatment of migraine: a single-blind, randomized, placebo-controlled study. Current medical research and opinion. 2019 May:35(5):909-915. doi: 10.1080/03007995.2018.1532403. Epub 2018 Oct 31 [PubMed PMID: 30285507]
Level 3 (low-level) evidenceSantos Lasaosa S, Gago Veiga A, Guerrero Peral ÁL, Viguera Romero J, Pozo-Rosich P. Patterns of anaesthetic pericranial nerve block in headache patients. Neurologia. 2018 Apr:33(3):160-164. doi: 10.1016/j.nrl.2016.05.016. Epub 2016 Jul 25 [PubMed PMID: 27461182]
Ilhan Alp S, Alp R. Supraorbital and infraorbital nerve blockade in migraine patients: results of 6-month clinical follow-up. European review for medical and pharmacological sciences. 2013 Jul:17(13):1778-81 [PubMed PMID: 23852904]
Pareja JA, López-Ruiz P, Mayo D, Villar-Quiles RN, Cárcamo A, Gutiérrez-Viedma Á, Lastarria CP, Romeral M, Yangüela J, Cuadrado ML. Supratrochlear Neuralgia: A Prospective Case Series of 15 Patients. Headache. 2017 Oct:57(9):1433-1442. doi: 10.1111/head.13158. Epub 2017 Aug 18 [PubMed PMID: 28833061]
Level 2 (mid-level) evidenceSjaastad O, Stolt-Nielsen A, Pareja JA, Fredriksen TA, Vincent M. Supraorbital neuralgia. On the clinical manifestations and a possible therapeutic approach. Headache. 1999 Mar:39(3):204-12 [PubMed PMID: 15613215]
Level 3 (low-level) evidencePerloff MD, Chung JS. Urgent care peripheral nerve blocks for refractory trigeminal neuralgia. The American journal of emergency medicine. 2018 Nov:36(11):2058-2060. doi: 10.1016/j.ajem.2018.08.019. Epub 2018 Aug 8 [PubMed PMID: 30119988]
Tay E, Gupta M, Franks W. Supraorbital nerve block in trabeculectomy surgery: an observational case series. Clinical & experimental ophthalmology. 2006 Sep-Oct:34(7):637-9 [PubMed PMID: 16970754]
Level 2 (mid-level) evidenceIsmail AR, Anthony T, Mordant DJ, MacLean H. Regional nerve block of the upper eyelid in oculoplastic surgery. European journal of ophthalmology. 2006 Jul-Aug:16(4):509-13 [PubMed PMID: 16952086]
Chaki T, Sugino S, Janicki PK, Ishioka Y, Hatakeyama Y, Hayase T, Kaneuchi-Yamashita M, Kohri N, Yamakage M. Efficacy and Safety of a Lidocaine and Ropivacaine Mixture for Scalp Nerve Block and Local Infiltration Anesthesia in Patients Undergoing Awake Craniotomy. Journal of neurosurgical anesthesiology. 2016 Jan:28(1):1-5. doi: 10.1097/ANA.0000000000000149. Epub [PubMed PMID: 25493926]
Kerscher C, Zimmermann M, Graf BM, Hansen E. [Scalp blocks. A useful technique for neurosurgery, dermatology, plastic surgery and pain therapy]. Der Anaesthesist. 2009 Sep:58(9):949-58; quiz 959-60. doi: 10.1007/s00101-009-1604-2. Epub [PubMed PMID: 19779756]
Kocuj F, Epple J, Polarz H, Tronnier VM, Martin E. Nerve blocks in stereotactic neurosurgery. Stereotactic and functional neurosurgery. 2002:78(1):29-38 [PubMed PMID: 12381883]
Guerrero ÁL, Herrero-Velázquez S, Peñas ML, Mulero P, Pedraza MI, Cortijo E, Fernández R. Peripheral nerve blocks: a therapeutic alternative for hemicrania continua. Cephalalgia : an international journal of headache. 2012 Apr:32(6):505-8. doi: 10.1177/0333102412439800. Epub 2012 Mar 21 [PubMed PMID: 22436371]
Monarca C, Rizzo MI, Corrias F, Marcasciano M, Parisi P, Scuderi N. Supraorbital and supratrochlear nerves block for oncologic surgery of the anterior scalp and forehead in the elderly. Annali italiani di chirurgia. 2012 Jan-Feb:83(1):79-80 [PubMed PMID: 22352224]
Level 3 (low-level) evidenceJiménez-Almonte JH, Wyles CC, Wyles SP, Norambuena-Morales GA, Báez PJ, Murad MH, Sierra RJ. Is Local Infiltration Analgesia Superior to Peripheral Nerve Blockade for Pain Management After THA: A Network Meta-analysis. Clinical orthopaedics and related research. 2016 Feb:474(2):495-516. doi: 10.1007/s11999-015-4619-9. Epub 2015 Nov 16 [PubMed PMID: 26573322]
Level 1 (high-level) evidenceWadlund DL. Local Anesthetic Systemic Toxicity. AORN journal. 2017 Nov:106(5):367-377. doi: 10.1016/j.aorn.2017.08.015. Epub [PubMed PMID: 29107256]
Fernandes L, Randall M MD FRCP, Idrovo L DMed FRCP. Peripheral nerve blocks for headache disorders. Practical neurology. 2020 Oct 23:():. pii: practneurol-2020-002612. doi: 10.1136/practneurol-2020-002612. Epub 2020 Oct 23 [PubMed PMID: 33097609]
Zetlaoui PJ, Gauthier E, Benhamou D. Ultrasound-guided scalp nerve blocks for neurosurgery: A narrative review. Anaesthesia, critical care & pain medicine. 2020 Dec:39(6):876-882. doi: 10.1016/j.accpm.2020.06.019. Epub 2020 Oct 8 [PubMed PMID: 33039656]
Level 3 (low-level) evidencePatel D, Yadav K, Taljaard M, Shorr R, Perry JJ. Effectiveness of Peripheral Nerve Blocks for the Treatment of Primary Headache Disorders: A Systematic Review and Meta-Analysis. Annals of emergency medicine. 2022 Mar:79(3):251-261. doi: 10.1016/j.annemergmed.2021.08.007. Epub 2021 Oct 28 [PubMed PMID: 34756448]
Level 1 (high-level) evidenceSimon KS, Rout S, Lionel KR, Joel JJ, Daniel P. Anatomical considerations of cutaneous nerves of scalp for an effective anesthetic blockade for procedures on the scalp. Journal of neurosciences in rural practice. 2023 Jan-Mar:14(1):62-69. doi: 10.25259/JNRP-2022-2-4-R2-(2362). Epub 2023 Jan 2 [PubMed PMID: 36891119]
Macfarlane AJR, Gitman M, Bornstein KJ, El-Boghdadly K, Weinberg G. Updates in our understanding of local anaesthetic systemic toxicity: a narrative review. Anaesthesia. 2021 Jan:76 Suppl 1():27-39. doi: 10.1111/anae.15282. Epub [PubMed PMID: 33426662]
Level 3 (low-level) evidencePatel D,Taljaard M,Yadav K,James D,Perry JJ, Current practice for primary headache disorders and perspectives on peripheral nerve blocks among emergency physicians in Canada: A national survey. Headache. 2022 Apr; [PubMed PMID: 35403242]
Level 3 (low-level) evidence