Introduction
Mucinous carcinoma of the breast is a relatively rare subtype of breast cancer, accounting for about 2% of all breast carcinomas (see Image. Mucinous Cancer).[1] According to the latest WHO classification of tumors of the breast, mucinous carcinoma is classified as a special type of breast cancer. Based on the cellularity of the tumor, mucinous carcinomas are divided into two subtypes:
- The pure type mucinous carcinoma.
- The mixed type mucinous carcinoma.
The pure type consists exclusively of tumor tissue with extracellular mucin production in over 90% of the tumor, while the mixed form also contains an infiltrating ductal epithelial component without mucin [2]. Mucinous breast cancer carries a favorable prognosis with a low recurrence rate and a low incidence of lymph node metastasis. The definitive diagnosis and classification of mucinous breast carcinomas are mainly based on histopathological examination.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The origin of mucinous breast cancer is multifactorial and involves diet, reproductive factors, and hormones.
Epidemiology
Mucinous breast carcinoma prevails in postmenopausal women with a median age of 70 years [3]. Pure mucinous carcinoma is rarely encountered in young patients under 35 (1%)[2].
Pathophysiology
Transcriptomic studies have demonstrated that mucinous tumors are of luminal A molecular subtype [4]. The transcriptomic features of mucinous A are distinct from those of mucinous B tumors, the latter showing a gene expression pattern similar to neuroendocrine carcinomas [4]. Pure mucinous carcinomas harbor a low level of genetic instability and rare recurrent amplifications, and the genomic profiles of the tumor components of mixed mucinous tumors are remarkably similar to those of pure mucinous carcinomas. More than 90% of pure mucinous carcinomas are diploid, whereas only 42% of mixed mucinous carcinomas are diploid [5].
Histopathology
Macroscopic findings:
A gross examination of mucinous carcinoma of the breast shows a glistening gelatinous lesion with pushing margins and a readily recognizable soft consistency. The tumors range from less than 1 cm to over 20 cm (mean = 3 cm).
Microscopic findings:
Histologically, mucinous carcinoma is characterized by nests of cells floating in lakes of mucin partitioned by delicate fibrous septae containing capillary blood vessels. The cell clusters are variable in shape and size with an occasional tubular arrangement. Nuclear atypia is generally low in classic mucinous carcinoma, but in rare cases, atypia and mitoses may prevail [6]. A micropapillary or cribriform intraepithelial component is rarely seen. Mucinous carcinoma presenting with large cell clusters, reported by Capella as hypercellular or type B mucinous carcinoma, shows frequent neuroendocrine differentiation [7]. Type A mucinous carcinoma with larger quantities of extracellular mucin represents the classic non-endocrine variety. Pure and mixed variants have been described [8]. The most common admixture is with invasive carcinoma of no special type. A pure tumor must be composed of more than 90% mucinous carcinoma [6]. The in situ component may have a papillary, micropapillary, or cribriform pattern. In some cases, the in situ carcinoma may exhibit prominent luminal mucin production. Neuroendocrine differentiation can sometimes be identified using immunohistochemistry and special stains (Grimelius).
Immunohistochemistry:
Typically, mucinous carcinoma is positive for estrogen and progesterone receptors [9], while androgen receptors are expressed at a low level, and HER2 is not amplified [10]. Pure and mixed mucinous carcinomas are reported to express WT [11]. Mucinous breast carcinoma expresses predominantly MUC2 and MUC6 among the family of MUC genes [12].
History and Physical
Mucinous carcinoma usually grows slowly and can reach a large size during diagnosis. This can be explained by the fact that the mucinous content of the tumor does not feel firm or solid upon examination [13]. Most patients with mucinous breast carcinoma present with a palpable breast mass. Fixation to the skin or chest wall is rare but is reported in large lesions. With widespread screening, many patients are diagnosed because of a mammographic abnormality [14].
Evaluation
Mammography:
On mammography, circumscribed and lobulated breast lesions are common findings for a mucinous carcinoma. A circumscribed margin would favor the diagnosis of a pure mucinous carcinoma [15].
Ultrasonography:
On ultrasonography, mucinous carcinoma is usually a complex mass with cystic and solid components, including microlobulation, vascularity, and distal enhancement. The histologic subtype of mucinous carcinoma can be predicted based on echogenicity. Isoechoic masses are found in pure mucinous carcinoma, whereas hypoechoic masses are found in mixed mucinous carcinoma [16].
Magnetic resonance imaging:
On an MRI, mucinous carcinoma has a lobular shape, rim or heterogeneous enhancement, a persistent pattern on the time-intensity curve, and homogeneous strongly high signal intensity on T2-weighted images [17] [15].
Tissue biopsy:
Tissue biopsy is mandatory in the evaluation of mucinous breast carcinoma. Tissue specimens can be obtained by core biopsy, fine needle aspiration cytology, and incisional or excisional biopsy.
Treatment / Management
The treatment of mucinous breast carcinoma is based on surgery associated with post-operative hormone therapy in hormone-responsive (estrogen/progesterone) tumors. A recent study recommended axillary staging by sentinel lymph node biopsy and administration of adjuvant radiotherapy and hormone therapy after breast-conservation for mucinous carcinoma [9][18]. Since most mucinous carcinomas are negative for the protein HER2/neu, they are not treated with trastuzumab. Trastuzumab is approved for both the treatment of advanced breast cancer and as adjuvant therapy for early-stage HER2-positive tumors [19]. Some authors have stated that adjuvant chemotherapy can be omitted in cases with favorable risk factors [20].(B2)
Differential Diagnosis
Histological differential diagnosis:
- Mucocele-like-lesion
- Metastatic mucinous carcinoma
Radiological differential diagnosis:
- Myxomatous fibroadenoma
Treatment Planning
The following factors may impact treatment decisions:
- Tumor biology: Since mucinous carcinoma is more prevalent in the older population, estrogen and progesterone receptors are expressed more often than in younger women. Similarly, there are lower rates of HER-2 overexpression. This impacts the selection of appropriate therapy.
- General health status: A higher prevalence of comorbidity, frailty, and cognitive decline in elderly patients are considered limiting factors when selecting treatment.
- Functional status: This refers to the ability to perform routine daily tasks. Functional limitation is independently associated with worse life expectancy and hence determines the overall survival of the patients. Comprehensive Geriatric Assessment (GCA) can be utilized to evaluate elderly patients and optimize mucinous cancer treatment.
Staging
Staging of mucinous breast carcinoma is determined clinically by physical examination and imaging studies. The stage is determined pathologically by histological examination of the tumor and lymph nodes after surgery. The TNM classification system is used to classify mucinous breast carcinoma based on:
- Primary tumor size (T)
- Regional lymph node status (N)
- Distant metastasis (M)
The system that is most recently used is that of the American Joint Committee on Cancer (8th edition).
Prognosis
Mucinous carcinoma has a favorable prognosis and infrequent lymphatic metastasis compared to invasive ductal carcinoma. Axillary lymph node metastases occur in 12%-14% of the cases [19]. Pure mucinous carcinoma has a better prognosis than mixed mucinous breast carcinoma [3]. The 5-year disease-free survival rates range from 81% to 94% (the latter if lymph nodes are negative). Late distant metastases may occur in pure mucinous carcinoma [21]. In a multivariate analysis of 11,422 patients with pure mucinous carcinoma, tumor size was found to be an independent prognostic indicator but less significant than nodal status [2]. Other studies have found that tumor size is not a significant prognostic factor and does not affect survival since most tumor volume consists of mucin[13].
Complications
Complications of breast mucinous carcinoma include:
- Axillary lymph node metastases
- Late distant metastases
- Recurrence after surgical excision
Consultations
Consultations that are typically requested for patients with breast mucinous carcinoma include:
- Surgical oncology
- Oncology
Deterrence and Patient Education
Women aged 40 and over need to talk to a doctor, discuss the benefits and drawbacks of breast cancer screening, and decide when to get screening. Women 40 to 74 years old or some older healthy women may be offered a screening test with the mammogram. Some women who are at high risk (BRCA gene or first-degree relatives with breast cancer) may need to begin screening at a younger age. Nine out of 10 women with an abnormal mammogram turn out not to have breast cancer. Many experts suggest a screening mammogram every 2 years.
Enhancing Healthcare Team Outcomes
The diagnosis of mucinous breast carcinoma requires an interprofessional team involving a surgical oncologist, an oncologist, a pathologist, and a radiologist. Treatment involves a surgeon, specialty care nurses, pharmacists, and oncologists. Pharmacists review drug regimens and check for drug-drug interactions. Specialty care nurses are involved and should assist the clinical team in patient education, monitor treatment, and provide feedback to the team. After treatment of mucinous breast carcinoma, long-term follow-up is necessary to detect local and distant relapse.
Media
(Click Image to Enlarge)
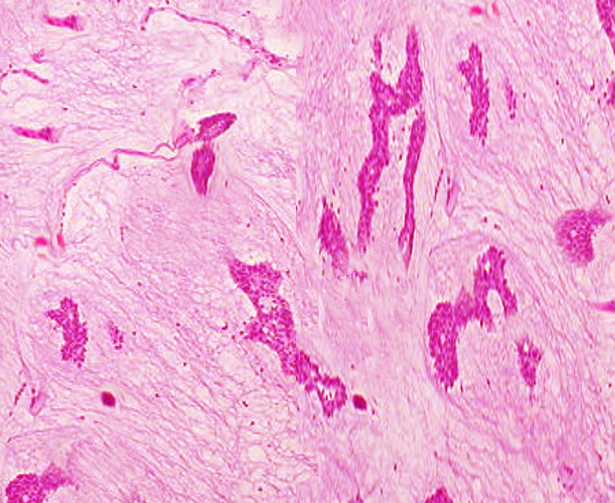
Mucinous Cancer
Contributed by S Bhimji, MD
References
Kaoku S, Konishi E, Fujimoto Y, Tohno E, Shiina T, Kondo K, Yamazaki S, Kajihara M, Shinkura N, Yanagisawa A. Sonographic and pathologic image analysis of pure mucinous carcinoma of the breast. Ultrasound in medicine & biology. 2013 Jul:39(7):1158-67. doi: 10.1016/j.ultrasmedbio.2013.02.014. Epub 2013 May 15 [PubMed PMID: 23683410]
Di Saverio S, Gutierrez J, Avisar E. A retrospective review with long term follow up of 11,400 cases of pure mucinous breast carcinoma. Breast cancer research and treatment. 2008 Oct:111(3):541-7 [PubMed PMID: 18026874]
Level 2 (mid-level) evidenceZhang L, Jia N, Han L, Yang L, Xu W, Chen W. Comparative analysis of imaging and pathology features of mucinous carcinoma of the breast. Clinical breast cancer. 2015 Apr:15(2):e147-54. doi: 10.1016/j.clbc.2014.11.005. Epub 2014 Nov 18 [PubMed PMID: 25523373]
Level 2 (mid-level) evidenceWeigelt B, Horlings HM, Kreike B, Hayes MM, Hauptmann M, Wessels LF, de Jong D, Van de Vijver MJ, Van't Veer LJ, Peterse JL. Refinement of breast cancer classification by molecular characterization of histological special types. The Journal of pathology. 2008 Oct:216(2):141-50. doi: 10.1002/path.2407. Epub [PubMed PMID: 18720457]
Toikkanen S, Eerola E, Ekfors TO. Pure and mixed mucinous breast carcinomas: DNA stemline and prognosis. Journal of clinical pathology. 1988 Mar:41(3):300-3 [PubMed PMID: 2834422]
Tan PH, Tse GM, Bay BH. Mucinous breast lesions: diagnostic challenges. Journal of clinical pathology. 2008 Jan:61(1):11-9 [PubMed PMID: 17873114]
Righi L, Sapino A, Marchiò C, Papotti M, Bussolati G. Neuroendocrine differentiation in breast cancer: established facts and unresolved problems. Seminars in diagnostic pathology. 2010 Feb:27(1):69-76 [PubMed PMID: 20306832]
Komaki K, Sakamoto G, Sugano H, Morimoto T, Monden Y. Mucinous carcinoma of the breast in Japan. A prognostic analysis based on morphologic features. Cancer. 1988 Mar 1:61(5):989-96 [PubMed PMID: 2827884]
Barkley CR, Ligibel JA, Wong JS, Lipsitz S, Smith BL, Golshan M. Mucinous breast carcinoma: a large contemporary series. American journal of surgery. 2008 Oct:196(4):549-51. doi: 10.1016/j.amjsurg.2008.06.013. Epub [PubMed PMID: 18809061]
Level 2 (mid-level) evidenceLacroix-Triki M, Suarez PH, MacKay A, Lambros MB, Natrajan R, Savage K, Geyer FC, Weigelt B, Ashworth A, Reis-Filho JS. Mucinous carcinoma of the breast is genomically distinct from invasive ductal carcinomas of no special type. The Journal of pathology. 2010 Nov:222(3):282-98. doi: 10.1002/path.2763. Epub [PubMed PMID: 20815046]
Domfeh AB, Carley AL, Striebel JM, Karabakhtsian RG, Florea AV, McManus K, Beriwal S, Bhargava R. WT1 immunoreactivity in breast carcinoma: selective expression in pure and mixed mucinous subtypes. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2008 Oct:21(10):1217-23. doi: 10.1038/modpathol.2008.69. Epub 2008 May 9 [PubMed PMID: 18469795]
Adsay NV, Merati K, Nassar H, Shia J, Sarkar F, Pierson CR, Cheng JD, Visscher DW, Hruban RH, Klimstra DS. Pathogenesis of colloid (pure mucinous) carcinoma of exocrine organs: Coupling of gel-forming mucin (MUC2) production with altered cell polarity and abnormal cell-stroma interaction may be the key factor in the morphogenesis and indolent behavior of colloid carcinoma in the breast and pancreas. The American journal of surgical pathology. 2003 May:27(5):571-8 [PubMed PMID: 12717243]
Komenaka IK, El-Tamer MB, Troxel A, Hamele-Bena D, Joseph KA, Horowitz E, Ditkoff BA, Schnabel FR. Pure mucinous carcinoma of the breast. American journal of surgery. 2004 Apr:187(4):528-32 [PubMed PMID: 15041505]
Wilson TE, Helvie MA, Oberman HA, Joynt LK. Pure and mixed mucinous carcinoma of the breast: pathologic basis for differences in mammographic appearance. AJR. American journal of roentgenology. 1995 Aug:165(2):285-9 [PubMed PMID: 7618541]
Level 2 (mid-level) evidenceChang YW, Kwon KH, Lee DW. Synchronous bilateral mucinous carcinoma of the breast: case report. Clinical imaging. 2009 Jan-Feb:33(1):62-6. doi: 10.1016/j.clinimag.2008.05.004. Epub [PubMed PMID: 19135933]
Level 3 (low-level) evidenceMemis A, Ozdemir N, Parildar M, Ustun EE, Erhan Y. Mucinous (colloid) breast cancer: mammographic and US features with histologic correlation. European journal of radiology. 2000 Jul:35(1):39-43 [PubMed PMID: 10930764]
Level 2 (mid-level) evidenceOkafuji T, Yabuuchi H, Sakai S, Soeda H, Matsuo Y, Inoue T, Hatakenaka M, Takahashi N, Kuroki S, Tokunaga E, Honda H. MR imaging features of pure mucinous carcinoma of the breast. European journal of radiology. 2006 Dec:60(3):405-13 [PubMed PMID: 16963218]
Yang M, Li X, Chun-Hong P, Lin-Ping H. Pure mucinous breast carcinoma: a favorable subtype. Breast care (Basel, Switzerland). 2013 Mar:8(1):56-9. doi: 10.1159/000346828. Epub [PubMed PMID: 24715844]
Garcia Hernandez I, Canavati Marcos M, Garza Montemayor M, Lopez Sotomayor D, Pineda Ochoa D, Gomez Macias GS. Her-2 positive mucinous carcinoma breast cancer, case report. International journal of surgery case reports. 2018:42():242-246. doi: 10.1016/j.ijscr.2017.12.025. Epub 2017 Dec 26 [PubMed PMID: 29291541]
Level 3 (low-level) evidencePark S, Koo J, Kim JH, Yang WI, Park BW, Lee KS. Clinicopathological characteristics of mucinous carcinoma of the breast in Korea: comparison with invasive ductal carcinoma-not otherwise specified. Journal of Korean medical science. 2010 Mar:25(3):361-8. doi: 10.3346/jkms.2010.25.3.361. Epub 2010 Feb 19 [PubMed PMID: 20191033]
Level 2 (mid-level) evidenceToikkanen S, Kujari H. Pure and mixed mucinous carcinomas of the breast: a clinicopathologic analysis of 61 cases with long-term follow-up. Human pathology. 1989 Aug:20(8):758-64 [PubMed PMID: 2545592]
Level 3 (low-level) evidence