Introduction
Vasculitides are a group of highly variable disorders characterized by inflammation of the vessel walls in various organ systems. Vasculitis can target large, medium, and small-sized arteries, capillaries, and veins. Mesenteric vasculitis is a disorder of the vessels of the gastrointestinal tract, that usually occurs in association with vasculitis of other organ systems, though it can occur in isolation. This activity will broadly discuss the various disorders that can cause mesenteric vasculitis, their presentation, diagnosis, and management.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
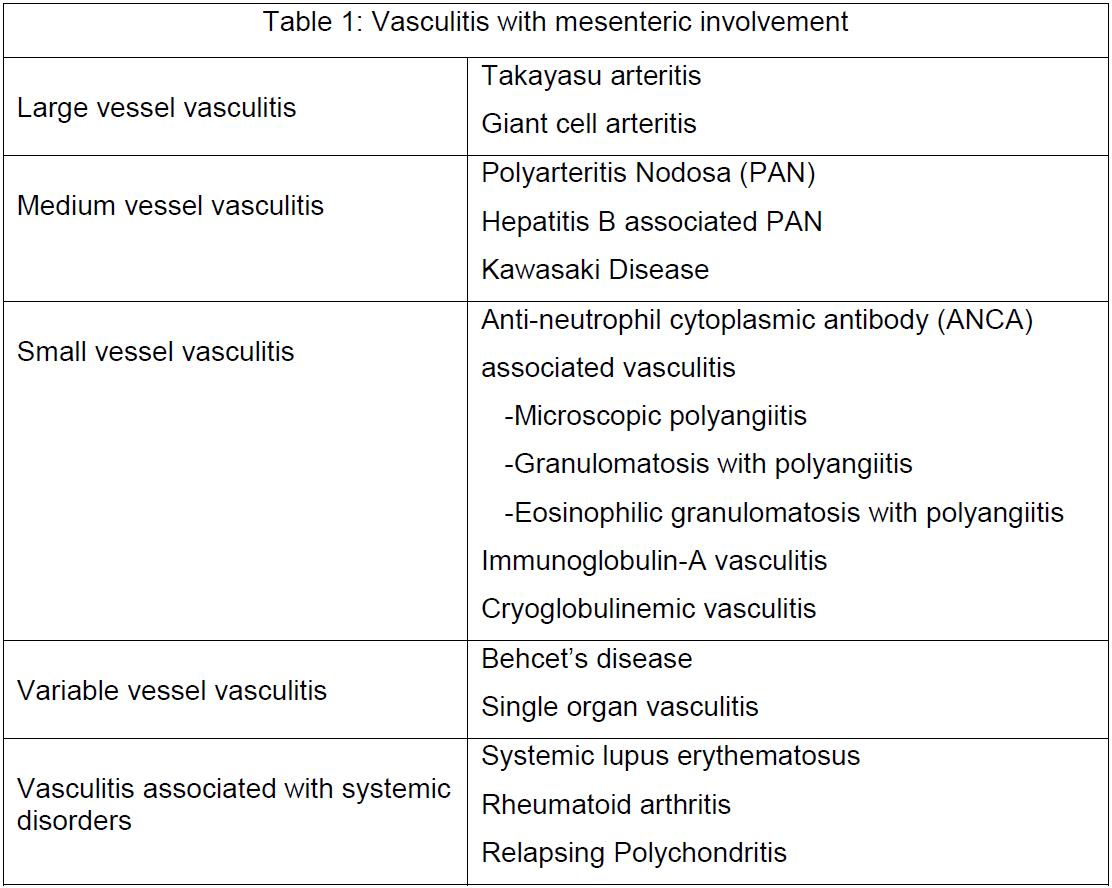
Though vasculitis is commonly classified based on the size of vessels predominantly involved there is often overlap in the involvement. Several types of vasculitis can have mesenteric involvement, as shown in Table 1.[2]
Epidemiology
There is only limited literature on the epidemiology of mesenteric vasculitis itself. However, data is available on the different types of vasculitis and systemic diseases that can have mesenteric involvement.[3][4][5]
Polyarteritis nodosa (PAN) is commonly seen in adults 35 to 60 years of age, with a male to female ratio of 1.5 to 1. Idiopathic and hepatitis B virus (HBV) infection-associated PAN are both considered clinically different entities.[6] The latter conditions commonly occur in areas endemic for HBV, and their incidence has been decreasing with increasing vaccination and successful treatment regimens for HBV. A genetically determined form of PAN called deficiency of ADA2 (DADA2) PAN was reported simultaneously from NIH and an Israeli group.[7][8] This condition is due to a mutation in the ADA2 gene (previously known as cat-eye syndrome critical region candidate 1 or CECR1 gene) resulting in the deficiency of the enzyme adenosine deaminase 2 (ADA2). Anti-neutrophilic cytoplasmic antibody (ANCA) associated vasculitis is another type of vasculitis with male predominance (1.5 to 1) with an age of onset around 65 to 74. Immunoglobulin-A (IgA) vasculitis is the most common vasculitis in children, with a peak age of onset between 4 and 6 years. It is reported to be slightly more common in males and the Asian population. Takayasu arteritis is seen across the world, though some reports suggest it is more common in Asia. Women constitute over 80% of the cases, and the age of onset is between 10 to 40 years. Behcet disease is more common among the Mediterranean and eastern Asian populations. It mostly affects people 20 to 40 years of age, with no gender predominance. Kawasaki disease mainly occurs in young children (under two years) of east Asian origin. Systemic lupus erythematosus is more common in females, with a ratio ranging from 3 to 1 in children and up to 12 to 1 in middle-aged adults. Two-thirds of these patients receive a diagnosis between 16 to 55 years. Rheumatoid arthritis is more common in women and is a disease of older adults, with most cases diagnosed after age 50.
History and Physical
In any patient presenting with abdominal symptoms, vasculitis should merit consideration if the history, examination, investigation, or imaging data lead to suspicion of the same. Most of the symptoms are due to ischemia of the intestines, leading to infarction. Ischemic colitis due to mesenteric vasculitis presents similar to ischemic colitis from atherosclerotic disease. Abdominal pain, tenderness, and rectal bleeding are the most common symptoms, while nausea, vomiting, and diarrhea can also be present.[9] Patients with acute mesenteric ischemia resulting from thrombus occlusion are more likely to present with acute, sudden onset pain that is disproportionate to the examination findings and lower gastrointestinal bleeding.[10][11] Chronic mesenteric ischemia resulting in reduced blood flow to the intestines can present with chronic post-prandial abdominal pain (abdominal angina) and weight loss.[12] Hemodynamic deterioration and change in mental status can occur in those presenting with severe complications like intestinal gangrene or perforation.
Evaluation
Initial laboratory workup should include a basic metabolic panel, complete blood count, liver function test, and urinalysis. Inflammatory markers like erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) can be useful, though they are non-specific. More specific testing like viral hepatitis serology, serum cryoglobulins, ANCA, antinuclear antibody (ANA), and rheumatoid factor are necessary for selected patients. Serum lactic acid should always get tested in patients with suspected bowel ischemia. In patients with suspected DADA2, genetic testing and functional ADA2 estimation are a recommendation.[13] Computerized tomography (CT) of the abdomen with intravenous contrast is the imaging of choice for suspected mesenteric ischemia from vasculitis.[14] In patients with mesenteric ischemia who cannot undergo contrast CT, magnetic resonance angiography is a good alternative.[12] Endoscopy should be considered with caution in patients with gastrointestinal vasculitis, as ischemia predisposes these patients to perforation during the procedure. Colonoscopic findings can be non-specific, though these may be useful in excluding other diagnoses. Classical finding in acute ischemia is pale, edematous, and necrotic mucosa that may become interspersed with normal segments. In severe cases, hemorrhages and ulcerations can be present. In chronic cases, atrophy of the mucosa and strictures can occur. Histopathology usually reveals mucosal damage and varying degrees of fibrosis.
Treatment / Management
Treatment consists of two major components: management of the underlying vasculitic process and specific interventions for the gastrointestinal pathology. Medical management of systemic vasculitis usually consists of glucocorticoids and other forms of immunosuppressive therapy, including cyclophosphamide, azathioprine, and mycophenolate mofetil.[15] The biological agents, including rituximab and TNF alpha inhibitors, may be useful depending upon the underlying etiology.
In patients with intestinal ischemia, when there is a suspicion of complications like infarction or perforation, surgical exploration should be performed at the earliest. Segmental resection of the affected bowel can be life-saving. In patients presenting with chronic bowel ischemia, timely intervention can reduce the risk of these complications. Triple-phase CT angiography can help identify stenosis and occlusion in the mesenteric circulation. Symptomatic stenosis can be treated with percutaneous transluminal angioplasty (PTA) with or without stenting for revascularization.[16] Since some of these diseases present at a younger age, a surgical bypass may be a better long-term solution than these relatively less invasive interventions.
The following section discusses the presentation and management of mesenteric vasculitis in detail, more specifically relative to the underlying etiology.
Polyarteritis Nodosa
Polyarteritis nodosa (PAN) is a necrotizing vasculitis predominantly affecting the medium-sized and small-sized visceral arteries. HBV infection is an environmental association in almost one-third of PAN cases, while the rest of them are idiopathic. The clinical presentation is highly variable due to the extent of arteries that can be involved in the disease. Gastrointestinal symptoms are a patient complaint in more than 50% of patients, and abdominal pain is the most common[17]. Postprandial pain in these patients is a manifestation of transmural vasculitis involving the mesenteric vasculature causing bowel ischemia.[11] Inflammation of the mucosal and submucosal arteries can present as ischemia or perforation involving the gallbladder, appendix, or colon. There are also reports of splenic infarcts, hepatic infarcts, and Budd Chiari syndrome.(B2)
In patients presenting with gastrointestinal symptoms, imaging evidence of bowel wall thickening or visceral infarction or rupture should raise suspicion for PAN. CT Angiography and catheter-based angiography can reveal typical findings in the form of scattered aneurysms and stenotic segments, giving rise to a beaded appearance.[18] All patients should undergo screening for underlying viral infections, including HBV, hepatitis C virus (HCV), and human immunodeficiency virus (HIV). Whenever a genetic variant like DADA2 is under consideration due to presentations like childhood PAN, livedoid rash, stroke, mononeuritis multiplex, and digital gangrene, genetic testing and functional ADA2 estimation are in order.[13] The prognosis has been improving with treatment, though it largely depends on the extent of disease involvement at diagnosis. Immunosuppression is the mainstay of treatment in most cases with mesenteric involvement. Induction therapy usually involves pulse doses of glucocorticoids with cyclophosphamide. In patients with underlying HBV, antiviral therapy is the primary treatment modality, along with plasmapheresis and a short course of corticosteroids. Anti TNFs are the preferred treatment for DADA2.[13]
ANCA Vasculitis
An ANCA-associated vasculitis is a group of three necrotizing vasculitic diseases involving the small arteries, capillaries, and venules. It includes granulomatosis with polyangiitis (GPA, previously Wegener granulomatosis), eosinophilic granulomatosis with polyangiitis (EGPA, also called Churg-Strauss syndrome), and microscopic polyangiitis (MPA). GPA characteristically demonstrates granulomatous inflammation of the upper and lower respiratory tract and sometimes immune glomerulonephritis. MPA also involves the respiratory tract and is associated with crescentic glomerulonephritis. Clinical features of EGPA include asthma, recurrent rhinosinusitis, and eosinophilia. ANCA-associated vasculitis can also affect the eye, ear, and nervous system. Gastrointestinal involvement by these disorders is less common and usually occurs in the advanced stages of the disease. The presentation can range from benign and non-specific symptoms like abdominal pain and vomiting to more serious complications like bleeding or perforation resulting from ischemia and ulceration in the small and large intestines.[19](B3)
In patients with suspicion for ANCA-associated vasculitis, serological testing is vital. More than 80% of patients with GPA and MPA are positive for ANCA. The antibodies in GPA are anti-proteinase-3, whereas those in MPA are anti-myeloperoxidase in most patients. ANCA can be negative in about half of EGPA cases. ANCA can also be positive in other conditions, which can make the diagnosis of these disorders very challenging. Patients with mesenteric involvement tend to have severe disease and usually receive treatment with cyclophosphamide and glucocorticoids for induction, followed by some form of immunosuppression. Rituximab is also an option in patients with mesenteric ischemia from underlying GPA and MPA.[20](A1)
Immunoglobulin-A Vasculitis
IgA vasculitis, also known as Henoch-Schonlein purpura (HSP), is the small-vessel vasculitis that is more common in the pediatric population. The classical presentation of IgA vasculitis consists of palpable purpura, mostly involving the lower extremities, hematuria, and arthralgia. Gastrointestinal manifestations are seen in about one-half of these patients and generally occur following the rash. Acute onset, colicky abdominal pain is the most common symptom. Inflammation leading to intestinal wall edema, bleeding, and ischemia her thought to be the underlying pathology for the abdominal pain. Both upper and lower gastrointestinal hemorrhage can occur in these patients. In children, bowel wall ischemia can lead to intussusception. Most patients describe a preceding upper respiratory infection. Though the disease course can be waxing and waning, it is usually self-limited. About 12 to 50% of patients suffer from a relapse.
The diagnosis of IgA-associated vasculitis is mostly clinical. Elevated serum IgA levels are neither sensitive nor specific to these disorders. Histopathology of the skin reveals leukocytoclastic vasculitis, and direct immunofluorescence shows deposition of IgA. In children presenting with severe abdominal pain and suspicion of IgA vasculitis, CT abdomen should be done to rule out intussusception or intestinal obstruction. Glucocorticoids, commonly prednisone at a dose of 1 mg/kg per day, have been shown to offer symptomatic benefit in patients with abdominal pain. However, it remains unclear if they affect the course of the disease. The role of other immunosuppressive agents and rituximab in these patients is still not well established.
Single Organ Vasculitis
Localized vasculitis of the gastrointestinal tract usually gets diagnosed after abdominal imaging or histopathology examination of organs from surgery reveals evidence suggestive of vasculitis.[21] This condition can occur in the esophagus, stomach, intestines, appendix, or gallbladder. Intestinal involvement usually presents with abdominal pain, nausea, vomiting, and weight loss. The natural history of the disease and the treatment will depend on the organ involved. Laparoscopic resection is associated with excellent results in vasculitis involving the gallbladder or appendix. Bowel resection is helpful in patients with intestinal involvement, though the outcome depends on the extent of disease and severity of presentation.(B2)
Takayasu Arteritis
Takayasu arteritis is a granulomatous vasculitis, commonly affecting the aorta and its primary branches. Though the classical pathology is stenotic lesions involving the subclavian, carotid, or abdominal aorta, involvement of the mesenteric circulation is also not uncommon. Most patients with mesenteric involvement are asymptomatic due to the establishment of extensive collateral circulation in the mesenteric bed. Glucocorticoids are the mainstay of therapy, and some require additional immunosuppression. Patients can present with mesenteric ischemia from critical occlusion of the celiac axis or superior mesenteric artery, in which cases percutaneous intervention with stenting is beneficial.[22]
Behcet Disease
This pathology is an idiopathic vasculitic syndrome characterized by recurrent painful ocular and genital ulcerations. Though it can involve any vessel, it has a propensity more towards the venous system. Gastrointestinal symptoms are due to mucosal ulceration that most commonly involved the terminal ileum, cecum, and ascending colon.[1] The clinical features include recurrent abdominal pain, diarrhea, and blood in the stool and can be difficult to distinguish from inflammatory bowel disease. A high index of clinical suspicion is necessary to diagnose these patients. Glucocorticoids, azathioprine, and infliximab have been used successfully to treat Behcet disease patients with mesenteric involvement.[23](B3)
Systemic Lupus Erythematosus
Gastrointestinal vasculitis in SLE is usually accompanied by active vasculitis of other organ systems as well. Lupus mesenteric vasculitis (LMV) has been known to occur in up to 10% of patients with SLE, and the prevalence is highest in patients with active disease.[24] Immune complex deposition in the arterioles and venules causes occlusion of the mesenteric circulation, ultimately leading to intestinal ulceration and ischemia. The presence of antiphospholipid antibodies represents a predisposition to thrombosis in the intestinal vessels that can also contribute to ischemia. Abdominal pain is the commonest presenting symptom. The clinical spectrum of LMV can range anywhere from patchy intestinal edema to gangrene and perforation.[25] Patients with SLE presenting with abdominal symptoms require investigation with imaging. CT findings in LMV can include intestinal wall thickening, dilated bowel loops, abnormal enhancement of the bowel wall (target sign), occlusion in the mesenteric circulation, and ascites.[26](B2)
Prompt institution of anti-inflammatory and immunosuppressive treatment can be life-saving in these patients. High doses of intravenous steroids are the first line of treatment, and refractory cases get therapy with cyclophosphamide. In patients presenting with frank signs of peritonitis, surgical exploration to identify large areas of bowel ischemia or complications like perforation should not delay. The prognosis of LMV is variable and depends on the extent of ischemia. However, some data shows mortality rates of up to 50%.
Rheumatoid Arthritis
Vasculitis can occur in patients with longstanding and severe rheumatoid arthritis. Patients who receive inadequate therapy, dose with high titers of antibody, and erosive arthritis are predisposed to developing vasculitis. Vasculitis of the gastrointestinal tract is very rare. The involvement of arterioles can present with ulcers, while vasculitis of medium-sized arteries can result in bowel ischemia. Medical treatment involves therapy for the underlying disease with glucocorticoids, other immunosuppressive agents, and biologicals.[27]
Mesenteric vasculitis has also been described infrequently in other systemic vasculitides like giant cell arteritis, relapsing polychondritis, Kawasaki disease, and cryoglobulinemic vasculitis.[28][29][30](B3)
Differential Diagnosis
A complete history and physical examination are crucial in the diagnosis of these patients. Some of the more common etiologies with similar presentations include atherosclerotic mesenteric ischemia, infections, malignancies, adverse medication effects, and other vessel occlusive processes. In patients with a known diagnosis of vasculitis who present with abdominal symptoms, the approach should be ruling out other causes and then focusing on treating the underlying vasculitic disorder. The diagnosis is more challenging in patients without an established diagnosis of vasculitis. Symptomatology suggesting the involvement of other organ systems or symptoms of bowel ischemia in patients without the risk factor profile of atherosclerosis should prompt investigations on the lines of mesenteric vasculitis.
Prognosis
The most important factors determining the prognosis are the severity and extent of mesenteric involvement at the presentation time. The underlying disorder and the extent of other organ systems involved are also vital in the overall prognosis. In most of these patients, mesenteric involvement is seen late during the disease course. Untreated, they have a very poor prognosis. Early recognition and treatment are pivotal in decreasing morbidity and mortality in patients with mesenteric vasculitis.
Complications
Vasculitis of the mesenteric vessels can lead to varying degrees of intestinal ischemia, leading to infarction. The most common underlying etiology is thrombosis of the superior mesenteric artery. Less common but serious complications include significant gastrointestinal bleeding, obstruction from strictures, and intussusception due to submucosal small-bowel edema. Occlusion from a thrombus in the mesenteric circulation can result in acute mesenteric ischemia. Less common but potentially fatal complications include bowel infarction, perforation, peritonitis, and sepsis from bacterial translocation. Ischemic hepatitis resulting from vasculitis is often asymptomatic and usually manifests in the form of abnormal liver function tests.
Deterrence and Patient Education
Given the relative rarity, prolonged course, and variable manifestations of mesenteric vasculitis, and vasculitis in general, it is essential for health care providers to educate patients and their family members about the disease. They can provide this through direct counseling, educational materials, or group meetings. In addition, the importance and possible adverse effects of the medications used in their management have to be discussed with patients in detail to ensure proper compliance and patient safety.
Enhancing Healthcare Team Outcomes
The management of mesenteric vasculitis can be challenging. an interprofessional approach is central in providing comprehensive care to these patients. A patient-centered team consisting of the primary care physician, rheumatologist, gastroenterologist, nurses must be involved in careful monitoring of the disease, titration of therapy, and early recognition of complications should they occur. Pharmacists need to coordinate with prescribers on dosing and interactions and educate patients on the types of drugs used to treat vasculitis, their benefits, and potential complications. Since there is no cure for vasculitis disorders, life-long follow-up is necessary. Also, when initiating biological treatments, patients require monitoring for infections and malignancies.
Since adverse drug reactions can be a part of the etiology of vasculitis, the pharmacist should consult about the potential for this by verifying the patient's medication record and reporting their findings to the treating physician(s). Once medical therapy begins, they should be involved with medication reconciliation and dose verification to assist the healthcare team. Nursing will also counsel, administer medication, and are in the best position to monitor treatment progress and watch for any drug adverse reactions, charting and communicating their observations to the team. This is the type of interprofessional team approach needed to take therapy to its optimal course. [Level V]
Though mesenteric vasculitis is uncommon, failure to diagnose or a delay in management can lead to dire consequences. In most patients with vasculitis, gastrointestinal involvement occurs with severe disease. Therefore, it is important to maintain a high index of suspicion in patients with abdominal symptoms and other evidence to suspect vasculitis. With several advances in medical treatment, endovascular interventions, and surgical options, the prognosis of patients with mesenteric vasculitis has improved significantly.
Media
(Click Image to Enlarge)
Mesenteric Vasculitis Contributed by Karthik Gnanapandithan, MD
References
Koster MJ, Warrington KJ. Vasculitis of the mesenteric circulation. Best practice & research. Clinical gastroenterology. 2017 Feb:31(1):85-96. doi: 10.1016/j.bpg.2016.12.003. Epub 2017 Jan 5 [PubMed PMID: 28395792]
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis and rheumatism. 2013 Jan:65(1):1-11. doi: 10.1002/art.37715. Epub [PubMed PMID: 23045170]
Level 3 (low-level) evidenceWatts RA, Robson J. Introduction, epidemiology and classification of vasculitis. Best practice & research. Clinical rheumatology. 2018 Feb:32(1):3-20. doi: 10.1016/j.berh.2018.10.003. Epub 2018 Nov 16 [PubMed PMID: 30526896]
Watts RA,Scott DG, Epidemiology of the vasculitides. Current opinion in rheumatology. 2003 Jan; [PubMed PMID: 12496504]
Level 2 (mid-level) evidenceWatts RA, Lane S, Scott DG. What is known about the epidemiology of the vasculitides? Best practice & research. Clinical rheumatology. 2005 Apr:19(2):191-207 [PubMed PMID: 15857791]
Sharma A, Sharma K. Hepatotropic viral infection associated systemic vasculitides-hepatitis B virus associated polyarteritis nodosa and hepatitis C virus associated cryoglobulinemic vasculitis. Journal of clinical and experimental hepatology. 2013 Sep:3(3):204-12. doi: 10.1016/j.jceh.2013.06.001. Epub 2013 Jul 8 [PubMed PMID: 25755502]
Zhou Q, Yang D, Ombrello AK, Zavialov AV, Toro C, Zavialov AV, Stone DL, Chae JJ, Rosenzweig SD, Bishop K, Barron KS, Kuehn HS, Hoffmann P, Negro A, Tsai WL, Cowen EW, Pei W, Milner JD, Silvin C, Heller T, Chin DT, Patronas NJ, Barber JS, Lee CC, Wood GM, Ling A, Kelly SJ, Kleiner DE, Mullikin JC, Ganson NJ, Kong HH, Hambleton S, Candotti F, Quezado MM, Calvo KR, Alao H, Barham BK, Jones A, Meschia JF, Worrall BB, Kasner SE, Rich SS, Goldbach-Mansky R, Abinun M, Chalom E, Gotte AC, Punaro M, Pascual V, Verbsky JW, Torgerson TR, Singer NG, Gershon TR, Ozen S, Karadag O, Fleisher TA, Remmers EF, Burgess SM, Moir SL, Gadina M, Sood R, Hershfield MS, Boehm M, Kastner DL, Aksentijevich I. Early-onset stroke and vasculopathy associated with mutations in ADA2. The New England journal of medicine. 2014 Mar 6:370(10):911-20. doi: 10.1056/NEJMoa1307361. Epub 2014 Feb 19 [PubMed PMID: 24552284]
Level 3 (low-level) evidenceNavon Elkan P, Pierce SB, Segel R, Walsh T, Barash J, Padeh S, Zlotogorski A, Berkun Y, Press JJ, Mukamel M, Voth I, Hashkes PJ, Harel L, Hoffer V, Ling E, Yalcinkaya F, Kasapcopur O, Lee MK, Klevit RE, Renbaum P, Weinberg-Shukron A, Sener EF, Schormair B, Zeligson S, Marek-Yagel D, Strom TM, Shohat M, Singer A, Rubinow A, Pras E, Winkelmann J, Tekin M, Anikster Y, King MC, Levy-Lahad E. Mutant adenosine deaminase 2 in a polyarteritis nodosa vasculopathy. The New England journal of medicine. 2014 Mar 6:370(10):921-31. doi: 10.1056/NEJMoa1307362. Epub 2014 Feb 19 [PubMed PMID: 24552285]
Camilleri M, Pusey CD, Chadwick VS, Rees AJ. Gastrointestinal manifestations of systemic vasculitis. The Quarterly journal of medicine. 1983 Spring:52(206):141-9 [PubMed PMID: 6604292]
Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: a clinical review. Archives of internal medicine. 2004 May 24:164(10):1054-62 [PubMed PMID: 15159262]
Ebert EC, Hagspiel KD, Nagar M, Schlesinger N. Gastrointestinal involvement in polyarteritis nodosa. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2008 Sep:6(9):960-6. doi: 10.1016/j.cgh.2008.04.004. Epub 2008 Jun 27 [PubMed PMID: 18585977]
Gnanapandithan K, Feuerstadt P. Review Article: Mesenteric Ischemia. Current gastroenterology reports. 2020 Mar 17:22(4):17. doi: 10.1007/s11894-020-0754-x. Epub 2020 Mar 17 [PubMed PMID: 32185509]
Human A, Pagnoux C. Diagnosis and management of ADA2 deficient polyarteritis nodosa. International journal of rheumatic diseases. 2019 Jan:22 Suppl 1():69-77. doi: 10.1111/1756-185X.13283. Epub 2018 Apr 6 [PubMed PMID: 29624883]
Ha HK, Lee SH, Rha SE, Kim JH, Byun JY, Lim HK, Chung JW, Kim JG, Kim PN, Lee MG, Auh YH. Radiologic features of vasculitis involving the gastrointestinal tract. Radiographics : a review publication of the Radiological Society of North America, Inc. 2000 May-Jun:20(3):779-94 [PubMed PMID: 10835128]
Angle JF, Nida BA, Matsumoto AH. Managing mesenteric vasculitis. Techniques in vascular and interventional radiology. 2015 Mar:18(1):38-42. doi: 10.1053/j.tvir.2014.12.006. Epub 2014 Dec 29 [PubMed PMID: 25814202]
Rits Y, Oderich GS, Bower TC, Miller DV, Cooper L, Ricotta JJ 2nd, Kalra M, Gloviczki P. Interventions for mesenteric vasculitis. Journal of vascular surgery. 2010 Feb:51(2):392-400.e2. doi: 10.1016/j.jvs.2009.08.082. Epub [PubMed PMID: 20141962]
Pagnoux C, Seror R, Henegar C, Mahr A, Cohen P, Le Guern V, Bienvenu B, Mouthon L, Guillevin L, French Vasculitis Study Group. Clinical features and outcomes in 348 patients with polyarteritis nodosa: a systematic retrospective study of patients diagnosed between 1963 and 2005 and entered into the French Vasculitis Study Group Database. Arthritis and rheumatism. 2010 Feb:62(2):616-26. doi: 10.1002/art.27240. Epub [PubMed PMID: 20112401]
Level 2 (mid-level) evidenceStanson AW, Friese JL, Johnson CM, McKusick MA, Breen JF, Sabater EA, Andrews JC. Polyarteritis nodosa: spectrum of angiographic findings. Radiographics : a review publication of the Radiological Society of North America, Inc. 2001 Jan-Feb:21(1):151-9 [PubMed PMID: 11158650]
Steele C, Bohra S, Broe P, Murray FE. Acute upper gastrointestinal haemorrhage and colitis: an unusual presentation of Wegener's granulomatosis. European journal of gastroenterology & hepatology. 2001 Aug:13(8):993-5 [PubMed PMID: 11507371]
Level 3 (low-level) evidenceStone JH, Merkel PA, Spiera R, Seo P, Langford CA, Hoffman GS, Kallenberg CG, St Clair EW, Turkiewicz A, Tchao NK, Webber L, Ding L, Sejismundo LP, Mieras K, Weitzenkamp D, Ikle D, Seyfert-Margolis V, Mueller M, Brunetta P, Allen NB, Fervenza FC, Geetha D, Keogh KA, Kissin EY, Monach PA, Peikert T, Stegeman C, Ytterberg SR, Specks U, RAVE-ITN Research Group. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. The New England journal of medicine. 2010 Jul 15:363(3):221-32. doi: 10.1056/NEJMoa0909905. Epub [PubMed PMID: 20647199]
Level 1 (high-level) evidenceSalvarani C, Calamia KT, Crowson CS, Miller DV, Broadwell AW, Hunder GG, Matteson EL, Warrington KJ. Localized vasculitis of the gastrointestinal tract: a case series. Rheumatology (Oxford, England). 2010 Jul:49(7):1326-35. doi: 10.1093/rheumatology/keq093. Epub 2010 Apr 1 [PubMed PMID: 20360040]
Level 2 (mid-level) evidenceSetty HS, Rao M, Srinivas KH, Srinivas BC, Usha MK, Jayaranganath M, Patil SS, Manjunath CN. Clinical, angiographic profile and percutaneous endovascular management of Takayasu's arteritis - A single centre experience. International journal of cardiology. 2016 Oct 1:220():924-8. doi: 10.1016/j.ijcard.2016.06.194. Epub 2016 Jun 26 [PubMed PMID: 27420344]
Hisamatsu T, Ueno F, Matsumoto T, Kobayashi K, Koganei K, Kunisaki R, Hirai F, Nagahori M, Matsushita M, Kobayashi K, Kishimoto M, Takeno M, Tanaka M, Inoue N, Hibi T. The 2nd edition of consensus statements for the diagnosis and management of intestinal Behçet's disease: indication of anti-TNFα monoclonal antibodies. Journal of gastroenterology. 2014 Jan:49(1):156-62. doi: 10.1007/s00535-013-0872-4. Epub 2013 Aug 18 [PubMed PMID: 23955155]
Level 3 (low-level) evidenceTian XP, Zhang X. Gastrointestinal involvement in systemic lupus erythematosus: insight into pathogenesis, diagnosis and treatment. World journal of gastroenterology. 2010 Jun 28:16(24):2971-7 [PubMed PMID: 20572299]
Yuan S, Ye Y, Chen D, Qiu Q, Zhan Z, Lian F, Li H, Liang L, Xu H, Yang X. Lupus mesenteric vasculitis: clinical features and associated factors for the recurrence and prognosis of disease. Seminars in arthritis and rheumatism. 2014 Jun:43(6):759-66. doi: 10.1016/j.semarthrit.2013.11.005. Epub 2013 Nov 12 [PubMed PMID: 24332116]
Level 2 (mid-level) evidenceKo SF, Lee TY, Cheng TT, Ng SH, Lai HM, Cheng YF, Tsai CC. CT findings at lupus mesenteric vasculitis. Acta radiologica (Stockholm, Sweden : 1987). 1997 Jan:38(1):115-20 [PubMed PMID: 9059413]
Puéchal X, Gottenberg JE, Berthelot JM, Gossec L, Meyer O, Morel J, Wendling D, de Bandt M, Houvenagel E, Jamard B, Lequerré T, Morel G, Richette P, Sellam J, Guillevin L, Mariette X, Investigators of the AutoImmunity Rituximab Registry. Rituximab therapy for systemic vasculitis associated with rheumatoid arthritis: Results from the AutoImmunity and Rituximab Registry. Arthritis care & research. 2012 Mar:64(3):331-9. doi: 10.1002/acr.20689. Epub [PubMed PMID: 22076726]
Scola CJ, Li C, Upchurch KS. Mesenteric involvement in giant cell arteritis. An underrecognized complication? Analysis of a case series with clinicoanatomic correlation. Medicine. 2008 Jan:87(1):45-51. doi: 10.1097/MD.0b013e3181646118. Epub [PubMed PMID: 18204370]
Level 3 (low-level) evidenceSharma A, Gnanapandithan K, Sharma K, Sharma S. Relapsing polychondritis: a review. Clinical rheumatology. 2013 Nov:32(11):1575-83. doi: 10.1007/s10067-013-2328-x. Epub 2013 Jul 26 [PubMed PMID: 23887438]
Colomba C, La Placa S, Saporito L, Corsello G, Ciccia F, Medaglia A, Romanin B, Serra N, Di Carlo P, Cascio A. Intestinal Involvement in Kawasaki Disease. The Journal of pediatrics. 2018 Nov:202():186-193. doi: 10.1016/j.jpeds.2018.06.034. Epub 2018 Jul 17 [PubMed PMID: 30029859]