Introduction
Mesenteric artery thrombosis (MAT) is a condition involving occlusion of the arterial vascular supply of the intestinal system. It is a severe and potentially fatal illness typically of the superior mesenteric artery (SMA), which provides the primary arterial supply to the small intestine and ascending colon.[1] The occlusion may occur due to in-situ thrombosis of the vessel, most commonly due to underlying atherosclerotic disease, or embolic occlusion from a distant source, as may occur in patients with atrial fibrillation. The condition possesses a high mortality rate, and prompt recognition and treatment are of utmost importance.
This articles will focus on acute arterial occlusion of the superior mesenteric artery. Other mesenteric vascular entities including chronic intestinal ischemia, mesenteric veno-occlusive disease, SMA syndrome, etc., are reviewed separately.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The two main causes of acute superior mesenteric artery thrombosis are:
- Atherosclerotic occlusion
- Embolic occlusion
In one autopsy series, the embolus/thrombus ratio was 1.4 to 1.[2] Other rare causes, including vasculitis and aortic dissection, may be predisposing factors.
Epidemiology
The incidence of MAT has been reported to be 12.9 per 100000 person-years.[3] The condition increases exponentially with age and is more common in women. Thrombotic occlusions are typically located more proximal in the SMA, which frequently leads to more extensive intestinal infarction. Embolic occlusions may lodge more distally, depending on the size of the embolus. Risk factors include[4]:
- Atherosclerosis
- Arrhythmias (specifically atrial fibrillation)
- Hypovolemia
- Cardiac disease including CHF, recent MI, and valvular disease
- Advanced age
- Intra-abdominal malignancy
- Inflammatory bowel disease (IBD) has also been implicated in the pathogenesis of acute mesenteric thrombosis.
The overall prevalence of the condition is estimated to account for 0.1% of all hospital admissions.
Pathophysiology
Thrombosis of the superior mesenteric artery, whether in-situ or embolic, causes an abrupt cessation in the primary blood flow to the majority of the small bowel as well as (typically) the ascending colon. This disruption leads to malperfusion of the involved end organ leading to ischemia and, ultimately, infarction. The severity of the injury directly relates to the amount of small bowel affected. In general, the more proximal the occlusion, the more severe the injury. Other factors, including the duration of ischemia, hypotension, and the presence (or absence) of collateral circulation may have a direct impact on the severity of the insult.
History and Physical
The presentation of mesenteric artery thrombosis is fairly consistent. The most common presenting complaint is abdominal pain which is classically out of proportion to the physical exam findings. Pain is typically moderate to severe, diffuse and constant. Other presenting symptoms may include nausea/vomiting, diarrhea, and rectal bleeding. In a study of acute mesenteric ischemia, 95% of patients presented with abdominal pain, 44% presented with nausea, 35% presented with vomiting, 35% presented with diarrhea, and 16% presented with rectal bleeding.[5] A rapid deterioration of the clinical condition is common. Signs of peritonitis may be subtle, and the key to early diagnosis hinges on strong clinical suspicion.
Evaluation
Early detection and treatment are crucial in the management of mesenteric artery thrombosis. Reports exist that there is a 50% chance of survival if diagnosis takes palce within 24 hours. However, survival drops to 30% if the diagnosis delays beyond the 24-hour window.[6] The initial evaluation should involve a basic set of laboratory analyses. The most common lab abnormalities are hemoconcentration, metabolic acidosis, with a high lactate concentration, as well as leukocytosis. Hyperkalemia and hyperphosphatemia and typically late signs and often correlates with bowel infarction. Plain film evaluation of the abdomen is non-specific and typically not particularly helpful from a diagnostic standpoint. Mesenteric angiography was historically considered the gold standard in diagnostic evaluation. However, this has been supplanted by CT angiography, which not only provides exquisite detail of the vascular anatomy but also provides extremely useful information regarding the integrity of the affected bowel. CT findings such as pneumoperitoneum, pneumatosis, portal venous gas, and bowel wall thickening can provide valuable information which is critical in guiding therapy. Mesenteric artery thrombosis may also be diagnosed with magnetic resonance angiography (MRA), particularly when intravenous contrast cannot be administered. However, it is prone to an artifact which can limit diagnostic accuracy and is dependent on a compliant patient because of the length of the examination. Duplex sonography may be helpful in the evaluation of mesenteric patency, which can be of particular value in patients with profound renal insufficiency in whom intravenous contrast may have a detrimental and occasionally irreversible impact on renal function. However, duplex sonography it is heavily operator dependent and is subject to limitations by poor acoustic windows secondary to bowel distention.
Treatment / Management
Upon diagnosing mesenteric artery thrombosis, prompt, definitive treatment is essential. Aggressive fluid resuscitation is imperative to correct hypotension and metabolic derangement. If there is no absolute contraindication, anticoagulation with heparin sodium administered intravenously should be promptly initiated. Other intravenous medications such as glucagon and papaverine may help manage vasospasm which frequently accompanies the thrombotic event. If peritoneal signs are present, bowel infarction should be presumed, and emergency laparotomy are necessary. If the occlusive source is embolic, a simple surgical embolectomy may be performed. If in-situ thrombosis is present, the underlying vessel is frequently too diseased to salvage. In these cases, a mesenteric bypass should be performed, ideally with an autologous vein to minimize the risk of contamination, particularly in cases with bowel perforation. Bowel resection should additionally be performed, as needed, at this time. Occasionally, second look surgery may be necessary to reassess the integrity of the small bowel.
Patients with documented mesenteric thrombosis who have not developed peritoneal signs may be considered for minimally invasive treatment alternatives such as catheter-directed thrombolytic infusion. This approach involves the intra-arterial placement of an infusion catheter into the thrombosed segment of superior mesenteric artery followed by infusion of tissue plasminogen activator (TPA). Studies have shown TPA to be very effective in dissolving acute superior mesenteric artery clot.[7][8] This procedure typically involves infusion over the course of 12 to 24 hours, and the benefits of this treatment modality should be weighed against the time required to complete therapy. Only stable patients should be considered for thrombolytic therapy. More recently, catheter-directed thrombectomy procedures utilizing small caliber intravascular thrombectomy devices have been used in conjunction with TPA with some degree of success, thereby shortening the length of treatment.[9](B2)
Differential Diagnosis
The differential diagnosis of mesenteric artery thrombosis extensive, given the common presenting symptom of abdominal pain. Differential diagnoses include (but are not limited to):
- Acute colitis
- Bowel obstruction
- Abdominal aortic aneurysm
- Biliary obstruction
- Intestinal perforation
- Malignancy
Prognosis
The prognosis of mesenteric artery thrombosis is generally poor. A large retrospective study found thirty-day postoperative morbidity of 56.6% and thirty-day mortality of 27.9%.[10] For patients undergoing surgical revascularization, the reported range of mortality rates is from 44 to 90%.[11]
Complications
- Short bowel syndrome
- Colostomy
- Multiorgan failure
- Peritonitis
- Occlusion of vein graft
- Death
Enhancing Healthcare Team Outcomes
Mesenteric artery thrombosis is a serious illness with potentially catastrophic implications absent the initiation of prompt diagnosis and treatment. Diagnosis and treatment require an efficient, collaborative approach involving physicians, nursing, as well as laboratory and radiology personnel. Because there is no specific test to make the diagnosis of mesenteric artery thrombosis, the general surgeon should be consulted early in the care of the patient. Most patients need immediate resuscitation and treatment. The overall outlook for most patients is poor.[12][13]
Media
(Click Image to Enlarge)
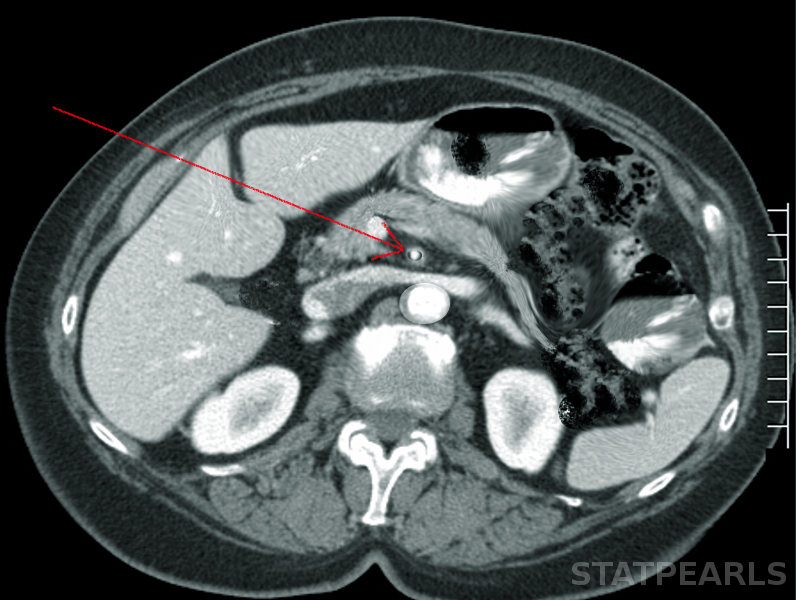
Superior mesenteric artery thrombosis Image courtesy S Bhimji MD
References
Ehlert BA, Acute Gut Ischemia. The Surgical clinics of North America. 2018 Oct; [PubMed PMID: 30243457]
Acosta S,Ogren M,Sternby NH,Bergqvist D,Björck M, Clinical implications for the management of acute thromboembolic occlusion of the superior mesenteric artery: autopsy findings in 213 patients. Annals of surgery. 2005 Mar [PubMed PMID: 15729076]
Acosta S, Epidemiology of mesenteric vascular disease: clinical implications. Seminars in vascular surgery. 2010 Mar; [PubMed PMID: 20298944]
Zezos P,Kouklakis G,Saibil F, Inflammatory bowel disease and thromboembolism. World journal of gastroenterology. 2014 Oct 14; [PubMed PMID: 25320522]
Park WM,Gloviczki P,Cherry KJ Jr,Hallett JW Jr,Bower TC,Panneton JM,Schleck C,Ilstrup D,Harmsen WS,Noel AA, Contemporary management of acute mesenteric ischemia: Factors associated with survival. Journal of vascular surgery. 2002 Mar; [PubMed PMID: 11877691]
Boley SJ,Feinstein FR,Sammartano R,Brandt LJ,Sprayregen S, New concepts in the management of emboli of the superior mesenteric artery. Surgery, gynecology [PubMed PMID: 7280946]
Björnsson S,Björck M,Block T,Resch T,Acosta S, Thrombolysis for acute occlusion of the superior mesenteric artery. Journal of vascular surgery. 2011 Dec [PubMed PMID: 21889287]
Level 2 (mid-level) evidenceOkamura S,Fujiwara H,Sonoyama T,Ochiai T,Ikoma H,Kubota T,Nakanishi M,Kikuchi S,Ichikawa D,Okamoto K,Sakakura C,Kokuba Y,Taniguchi H,Otsuji E, Management of Acute Superior Mesenteric Artery Occlusion by Thrombolytic Therapy. Case reports in gastroenterology. 2009 Sep 22; [PubMed PMID: 21103245]
Level 3 (low-level) evidenceKuhelj D,Kavcic P,Popovic P, Percutaneous mechanical thrombectomy of superior mesenteric artery embolism. Radiology and oncology. 2013; [PubMed PMID: 24133388]
Gupta PK,Natarajan B,Gupta H,Fang X,Fitzgibbons RJ Jr, Morbidity and mortality after bowel resection for acute mesenteric ischemia. Surgery. 2011 Oct; [PubMed PMID: 22000191]
Christensen MG,Lorentzen JE,Schroeder TV, Revascularisation of atherosclerotic mesenteric arteries: experience in 90 consecutive patients. European journal of vascular surgery. 1994 May; [PubMed PMID: 8013680]
Shchegolev AA,Papoian SA,Mitichkin AE,Gromov DG,Ishevskiĭ AG,Chevokin AI,Mutaev MM, [Endovascular treatment of acute mesenteric ischaemia in thrombosis of superior mesenteric artery]. Angiologiia i sosudistaia khirurgiia = Angiology and vascular surgery. 2017 [PubMed PMID: 29240055]
Loeffler JW,Obara H,Fujimura N,Bove P,Newton DH,Zettervall SL,van Petersen AS,Geelkerken RH,Charlton-Ouw KM,Shalhub S,Singh N,Roussel A,Glebova NO,Harlander-Locke MP,Gasper WJ,Humphries MD,Lawrence PF, Medical therapy and intervention do not improve uncomplicated isolated mesenteric artery dissection outcomes over observation alone. Journal of vascular surgery. 2017 Jul [PubMed PMID: 28506477]