Introduction
The medial pectoral nerve, which is also known as the medial anterior thoracic nerve, arises as a branch of the medial cord of the brachial plexus with fibers originating from the eighth cervical and first thoracic nerve roots. It runs along the lower border of the pectoralis minor muscle, innervating it and also the lower half of the pectoralis major muscle through its distal branch.[1] There may be anatomical variations where the medial pectoral nerve arises from the anterior division of the inferior trunk of the brachial plexus and less frequently from the lower trunk.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The medial pectoral nerve arises posterior to the axillary artery, curves forward between the axillary artery and vein before receiving a communicating branch from the lateral pectoral nerve. The medial pectoral nerve enters the pectoralis minor muscle in which it gives off several branches that supply the muscle. The nerve then perforates the pectoralis minor muscle to reach the pectoralis major muscle. The pectoralis major muscle consists of a clavicular part and a sternal part. The sternal portion receives innervation from the medial pectoral nerve, which functions to extend the arm at the shoulder from a flexed position. Due to the insertion of the pectoralis minor muscle to the coracoid apophysis, this muscle helps produce a medial rotation of the scapula against resistance, with the scapula and the upper limb fixed. Therefore, an injury to the medial pectoral nerve can lead to an inability to elevate the shoulder. The pectoralis minor muscle can also work as an accessory muscle for forced inspiration.
The medial pectoral nerve arises from the medial cord of the brachial plexus with C8 and T1 nerve roots.[2] The medial pectoral nerve may arise directly from the anterior division of the inferior trunk of the brachial plexus. The origin of the nerve directly from the middle trunk of the brachial plexus has also been reported.[3] There are two main patterns of branching of this nerve. In the more common pattern, the nerve pierces the deep aspect of the pectoralis minor muscle as a single trunk, ramifies in the muscle, and gives out branches that appear on the superficial aspect to enter the pectoralis major. In the other pattern, the nerve divides before entering the pectoralis minor, and its branches pass through the muscle or around its lower border to reach the pectoralis major.[4]
Embryology
The medial pectoral nerve is a peripheral nerve that arises from the brachial plexus. The brachial plexus is formed by the ventral rami of C5 through T1 to form trunks. The trunks form anterior and posterior divisions, which in turn form cords, and the cords end as terminal branches. The neuroectoderm differentiates from the ectoderm into the neural plate, which folds in upon itself to form the neural tube. This process is called neurulation. The neural crest cells located at the most dorsal portion subsequently undergo an epithelial to mesenchymal transition, delaminate from the neural tube, and migrate to different and sometimes distant regions of the embryo.[5] The primordium of the dorsal nerves ends at the level of the humerus, which is the location of the sheath of the primordium of the muscles of the arm. On day 32, nerve extensions form from C5-T1, and on day 33, the nerves join together, and the plexus brachialis begins to form. A similar provision and orientation of the plexus brachialis to that of the adult are observable by days 49 and 50. The abundant anastomosis of the nerve roots from the fourth cervical through the first thoracic segment marks a primitive brachial plexus, where the medial pectoral nerve arises from its medial cord.
Blood Supply and Lymphatics
The axillary artery is closely related to the cords of the brachial plexus.[6] The medial pectoral nerve is posterior to the axillary artery and passes between the axillary artery and vein. The axillary lymph nodes drain the arm, the walls of the thorax, the mammary gland, and the upper walls of the abdomen. Therefore, the axillary nodes also receive lymph from the pectoralis minor muscle and the sternal portion of the pectoralis major muscle that is the region innervated by the medial pectoral nerve.
Nerves
The ventral rami of C5 through T1 form the brachial plexus, and the lateral and medial pectoral nerves arise from the lateral and medial cords, respectively.
The medial pectoral nerve communicates with other nerves to innervate certain structures. This is the case of the lateral and medial pectoral nerves, which together form a loop called the ansa pectoralis, through which the lateral pectoral nerve also contributes to the pectoralis minor muscle innervation.[2]
Muscles
The medial pectoral nerve innervates the lower part of the pectoralis major and the pectoralis minor muscle, which contributes to the thoraco-brachial motion. The pectoralis major is a fan-shaped muscle located across the upper chest from the shoulder to the sternum and is the most superficial muscle in the pectoral region. The pectoralis minor muscle lies beneath the pectoralis major muscle and inserts superolaterally into the coracoid process of the anterior scapula and anteromedially into the third, fourth, and fifth ribs.[7] The accessory muscles of the shoulder girdle, such as pectoralis quartus, chondrofascialis, axillary arch, chondroepitrochlearis, and sternalis muscles, may be innervated by the medial pectoral nerve.[8]
Physiologic Variants
The reports of variants of the medial pectoral nerve are scanty because they are less frequent than, for example, the variants of the lateral pectoral nerve. It is most likely to arise from the medial cord, but sometimes it can arise from the anterior division of the lower trunk, and less frequently, the medial pectoral nerve can arise directly from the trunk of the brachial plexus. There are reports of the medial pectoral nerve originating from the C6 root and the anterior division of the middle trunk, but origin directly from the middle trunk of the brachial plexus has not been reported until now.[3]
Surgical Considerations
The pectoral nerves may be injured by direct trauma, muscle compression, and iatrogenic scenarios such as breast surgery and axillary node dissection. The nerve can also be injured in pectoralis major muscle transfers, but surgical recovery is possible through nerve transfers. The surgical approach to the medial pectoral nerve is from either the supraclavicular or the infraclavicular route at the level of the medial cord. Its surgical accessibility, expandability, and a high number of motor fibers make it an attractive donor nerve for upper plexus injuries.[8] On the other hand, there are different opinions about the use of the medial pectoral nerve as a viable motor donor for brachial plexus injuries. Reports exist of favorable results, for example, in the restoration of elbow flexion, shoulder abduction, and improved serratus anterior strength with transfer to the musculocutaneous nerve, axillary nerve, and long thoracic nerve, respectively, when using the medial pectoral nerve as a donor.[9]
As mentioned previously, the medial pectoral nerve mostly courses through the pectoralis minor muscle, whereas other times, it exits around the lateral aspect of this muscle. If a surgeon dissects between the pectoralis major and minor muscles, a portion of the innervation to the pectoralis major muscle is at risk of disruption.
Clinical Significance
The modified radical mastectomy has become a common surgery for breast cancer.[10] Surgeons should avoid the medial pectoral nerve and the thoracoacromial vessel branches found at the apex of the axillary space during the removal of the lymph nodes. In some procedures such as mastectomy and shoulder dislocations, a neurovascular block of the medial and lateral nerves is necessary to reduce post-operative pain and muscle spasm.[3] Even in breast augmentation procedures using breast implants or the transfer of the pectoralis major muscle in myocutaneous free flap surgery, the cosmetic surgeons have to know the exact course of these nerves and their possible variations.[1]
Other Issues
The medial pectoral nerve can be used for nerve transfer procedures (neurotization) to restore the function of the shoulder after an injury to the upper trunk of the brachial plexus.[9] Nerve transfers have better outcomes with a greater potential for functional recovery because the shoulder's muscular biomechanics are not altered as in the case of tendon transfers.[11] For this type of injury, the primary purpose is to focus on the stabilization of the shoulder with the restoration of shoulder abduction and external rotation because the most distal functions depend on the functionality and stability of the shoulder.[12]
Media
(Click Image to Enlarge)
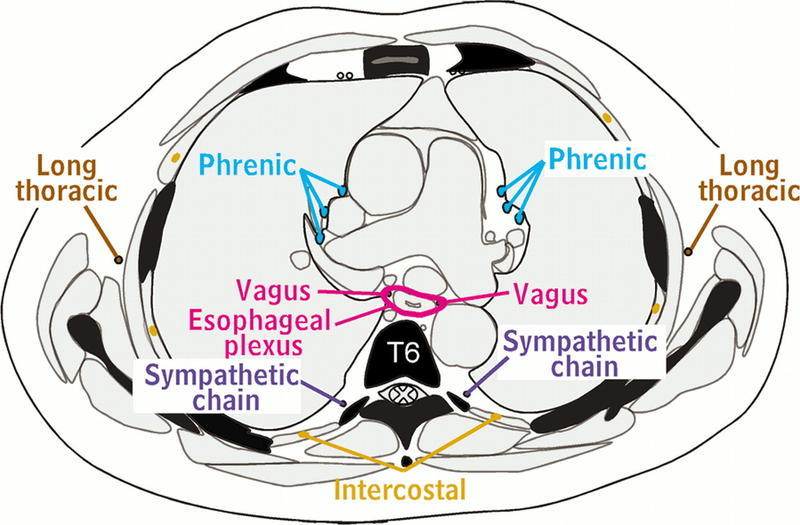
Nerves of Thorax Aquino et al, Radiographics, Long Thoracic Nerves, Phrenic Nerves, Vagus Nerves, Esophageal Plexus, Sympathetic Chain, Intercostal Nerve, T6 Contributed by chestatlas.com (H. Shulman MD)
References
Kg P, K S. Anatomical study of pectoral nerves and its implications in surgery. Journal of clinical and diagnostic research : JCDR. 2014 Jul:8(7):AC01-5. doi: 10.7860/JCDR/2014/8631.4545. Epub 2014 Jul 20 [PubMed PMID: 25177552]
Tigga SR, Wadhwa S, Goswami P. Unusual communications of the brachial plexus. International journal of applied & basic medical research. 2016 Jan-Mar:6(1):68-70. doi: 10.4103/2229-516X.174021. Epub [PubMed PMID: 26958529]
Shetty P, Nayak SB, Kumar N, Thangarajan R, D'Souza MR. Origin of medial and lateral pectoral nerves from the supraclavicular part of brachial plexus and its clinical importance - a case report. Journal of clinical and diagnostic research : JCDR. 2014 Feb:8(2):133-4. doi: 10.7860/JCDR/2014/7082.4029. Epub 2014 Feb 3 [PubMed PMID: 24701504]
Level 3 (low-level) evidenceMacchi V,Tiengo C,Porzionato A,Parenti A,Stecco C,Mazzoleni F,De Caro R, Medial and lateral pectoral nerves: course and branches. Clinical anatomy (New York, N.Y.). 2007 Mar; [PubMed PMID: 16583383]
Butler SJ, Bronner ME. From classical to current: analyzing peripheral nervous system and spinal cord lineage and fate. Developmental biology. 2015 Feb 15:398(2):135-46. doi: 10.1016/j.ydbio.2014.09.033. Epub 2014 Oct 24 [PubMed PMID: 25446276]
Level 3 (low-level) evidenceMonem M, Iskandarani MK, Gokaraju K. Axillary artery pseudoaneurysm resulting in brachial plexus injury in a patient taking new oral anticoagulants. BMJ case reports. 2016 Aug 17:2016():. doi: 10.1136/bcr-2016-216976. Epub 2016 Aug 17 [PubMed PMID: 27535738]
Level 3 (low-level) evidenceLeiman D, Barlow M, Carpin K, Piña EM, Casso D. Medial and lateral pectoral nerve block with liposomal bupivacaine for the management of postsurgical pain after submuscular breast augmentation. Plastic and reconstructive surgery. Global open. 2014 Dec:2(12):e282. doi: 10.1097/GOX.0000000000000253. Epub 2015 Jan 8 [PubMed PMID: 25587516]
Level 3 (low-level) evidencePorzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, De Caro R. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clinical anatomy (New York, N.Y.). 2012 Jul:25(5):559-75. doi: 10.1002/ca.21301. Epub 2011 Nov 28 [PubMed PMID: 22125052]
Level 1 (high-level) evidenceRay WZ, Murphy RK, Santosa K, Johnson PJ, Mackinnon SE. Medial pectoral nerve to axillary nerve neurotization following traumatic brachial plexus injuries: indications and clinical outcomes. Hand (New York, N.Y.). 2012 Mar:7(1):59-65. doi: 10.1007/s11552-011-9378-9. Epub 2011 Nov 29 [PubMed PMID: 23449552]
Level 2 (mid-level) evidenceMoosman DA. Anatomy of the pectoral nerves and their preservation in modified mastectomy. American journal of surgery. 1980 Jun:139(6):883-6 [PubMed PMID: 7386746]
Colbert SH, Mackinnon S. Posterior approach for double nerve transfer for restoration of shoulder function in upper brachial plexus palsy. Hand (New York, N.Y.). 2006 Dec:1(2):71-7. doi: 10.1007/s11552-006-9004-4. Epub [PubMed PMID: 18780028]
Terzis JK, Kostas I, Soucacos PN. Restoration of shoulder function with nerve transfers in traumatic brachial plexus palsy patients. Microsurgery. 2006:26(4):316-24 [PubMed PMID: 16649194]
Level 3 (low-level) evidence