Introduction
Marcus Gunn jaw-winking syndrome (MGJWS) is noted in congenital blepharoptosis. MGJWS was first described by a Scottish ophthalmologist Dr.Robert Marcus Gunn in the year 1883. This syndrome was initially reported in a 15-year-old girl as unilateral ptosis associated with the upper eyelid contraction on the same side.[1] Other names of MGJWS include Marcus-Gunn jaw winking phenomenon (MGP), Marcus Gunn ptosis, Marcus Gunn jaw winking trigemino-oculomotor synkinesis, Maxillopalpebral synkinesis, and Pterygoid-levator synkinesis. It is one of the congenital cranial dysinnervation disorders (CCDD), and these individuals have variable degrees of blepharoptosis in the resting, primary position.[2] It is associated with synkinetic movements of the upper eyelid during masticating movements of the jaw. It is usually unilateral but may present bilaterally also.[3][4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The occurrence of a coordinated sequence of movements of the muscles innervated by different branches of the same nerve or different nerve is known as synkinesis. In Marcus Gunn jaw-winking syndrome (MGJWS), there occurs a coordinated synkinetic movement of the upper eyelid and the jaw as a result of an abnormal connection between the motor branches of the trigeminal nerve and superior division of oculomotor nerve.[5] This is a congenital condition, and the abnormal neurological connection is postulated as fibers of the fifth cranial nerve are responsible for either directly or indirectly innervating the levator muscle. Familial cases with autosomal dominant inheritance have been described in the literature, but are exceedingly rare.[6] There have been few published reports on acquired MGJWS presumed to develop after complicated ocular surgery and trauma.[5]
Epidemiology
Approximately 50% of the blepharoptosis cases are congenital. The incidence of Marcus Gunn jaw-winking syndrome (MGJWS) among individuals with congenital ptosis is approximately 2% to 13%.[7] Although present at birth, MGJWS can occur at a wide range of ages. Bilateral cases have been reported, but mostly MGJWS are unilateral and occurs more frequently on the left.[4] There is no gender predisposition, and males and females are affected equally.[8]
Pathophysiology
Electromyographic studies have reported that the impulses for this synkinetic movement in Marcus Gunn jaw-winking syndrome originate from the proprioceptive receptors of the external pterygoid muscle.[9] The movement can be triggered by chewing, suction, lateral mandibular movement, smiling, Valsalva maneuver, sternocleidomastoid muscle contraction, tongue protrusion, and even breathing. In a few patients, the synkinetic movement has been documented between the internal pterygoid and levator palpebrae superioris (LPS) muscles. In such individuals, the eyelid elevates on closing the mouth and clenching the teeth.[10]
There exists a lack of explanation in the literature regarding the rationale of the jaw-winking phenomenon. Various theories have been presumed to explain this synkinetic jaw winking movement. The most acceptable theory of MGP is the concept of aberrant connection.[11] This location of aberrant connection may differ as follows:
- Cortical or the subcortical connections
- Internuclear connections or faulty distribution in the posterior longitudinal bundle
- Infranuclear misconnection between the trigeminal nerve (CN V3) and the oculomotor nerve (CN III).[11]
- Peripherally - some trigeminal nerve fibers may reach the LPS muscle through the auriculotemporal nerve.[11]
Histopathology
Marcus Gunn jaw-winking syndrome (MGJWS) is believed to be due to the abnormal innervation of the LPS from the motor branch of the trigeminal nerve, so most of the histopathologic studies have revealed normal striated muscle.[12] Few studies have found some degrees of fibrosis within the affected LPS muscle.[13]
History and Physical
The jaw-wink reflex consists of a momentary retraction/elevation of the upper eyelid (which was ptotic) upon stimulation of the ipsilateral pterygoid muscle, which is followed by a rapid return to a lower position. The magnitude of the wink is worse in downgaze. This synkinetic phenomenon may be elicited not only by opening the mouth, but also by thrusting the jaw to the contralateral side, jaw protrusion, chewing, smiling, or sucking. The ocular associations of Marcus Gunn jaw-winking syndrome (MGJWS) include strabismus in 50% to 60% individuals, superior rectus palsy in 25% individuals, and double elevator palsy in 25% individuals.[1]
Almost 5-25 % of these patients are reported to have anisometropia, and 30% to 60% are reported to have amblyopia.[1] The cause for underlying amblyopia could be secondary to strabismus, anisometropia, or occlusion by the ptotic lid. Rare ocular associations include Morning Glory anomaly, Duane retraction syndrome.[14] The systemic associations with MGJWS include cleft lip/ cleft palate, olfactory nerve disturbance, CHARGE syndrome (coloboma, heart defects, choanal atresia, retardation of growth and development, genital abnormalities, and ear abnormalities), and renal calculi.[4][15]
Usually, this synkinetic movement of the eyelid will be observed first by the mother when the child is breastfeeding or bottle feeding. History of ocular trauma or strabismus surgery may also be present. The diagnosis is made based on the signs as described below:[16]
- Unilateral blepharoptosis
- Upper eyelid movement is seen on opening the mouth, movement of the jaw to the contralateral side, chewing, sucking, swallowing, clenching teeth, and protrusion of the jaw.
- Hypotropia on the affected side may be present with the cover test due to associated superior rectus palsy.
Detailed clinical examination includes the following:[17]
- Visual acuity (It is important to rule out amblyopia in infants and children)
- Pupillary examination
- Cycloplegic refraction mainly to rule out anisometropia
- Fundus evaluation, extraocular motility test, cover test to rule out superior rectus or double elevator palsy)
- Adequacy of Bell phenomenon as it can be decreased with superior rectus or double elevator palsy
- Head position: As a result of ptosis, the child may have chin lifting for better vision. If a child is not attempting to lift the chin in the presence of moderate-to-severe ptosis, then it is imperative to exclude amblyopia.
- Ptosis evaluation: The degree of ptosis should be assessed with the jaw immobilized in a central position and after disrupting the fusion with brief ocular occlusion.[18] Ptosis can be graded as mild ptosis (maximum 2mm), moderate ptosis (3 mm), and severe ptosis (at least 4 mm).
- Vertical palpebral fissure which is the widest distance between the upper and lower lid
- Marginal reflex distance (MRD), which is measured with eyes in primary gaze position. MRD1 is the measurement of the corneal reflex to the central upper lid margin. MRD2 is the measurement of the corneal reflex to the central lower lid margin. MRD3 is the distance of the corneal reflex to the central upper-lid margin when the patient looks in extreme upgaze and is used to determine the measurement of LPS resection in ptosis surgery.
- Levator function, which is the distance the upper lid travels from downgaze to upgaze while the frontalis muscle is held firmly at the brow region. Levator function can be graded as normal (at least 15 mm), good (12-14 mm), fair (5-11 mm), or poor (less than or equal to 4 mm).
- Measurement of eyelid position in downgaze and presence of any lid lag
Evaluation
It is crucial to exclude the association of dry eyes in these patients before proceeding with ptosis surgery. Complete blood investigations and Chest x-ray may be needed for preoperative fitness/ pre-anesthetic checkup before surgery. ECG should be done in patients with Marcus Gunn jaw-winking syndrome (MGJWS) as they are predisposed to cardiac arrhythmias. It is important to ensure the anesthetist is well informed of clinical diagnosis and its potential significance before proceeding with ptosis surgery.[19]
Treatment / Management
The treatment options for Marcus Gunn jaw-winking syndrome (MGJWS) include the following:
Medical Care
The patient needs aggressive treatment with occlusion therapy and/or correction of anisometropia before any consideration of ptosis surgery if amblyopia is encountered. Close follow up is usually advised while the patient is undergoing therapy for amblyopia.[20] Clinical photographs can help in monitoring patients.
Surgical Care
Thoughts on surgery for MGJWS are currently controversial. Some surgeons believe that the child should not have surgery until the age of one to two years old as general anesthesia is safer at 1-2 years than infancy. Any surgical correction to repair only the ptosis without correcting the synkinetic jaw winking may result in an aggravation of the aberrant eyelid movement, which may be cosmetically disfiguring to the patient. Indications for surgery include the presence of amblyopia and vertical strabismus, severe ptosis with levator muscle dysfunction, and severe ptosis with normal levator function.
The jaw-winking phenomenon is considered cosmetically significant only if it is 2 mm or more. If the jaw-winking is cosmetically insignificant or if the ptosis is mild, it is advisable not to proceed with surgery. If a correction is desired in mild ptosis, then procedures of choice include Muller muscle and conjunctival resection, a Fasanella– Servat procedure, or a standard external levator resection.
If the ptosis is moderate to severe, then resection of LPS with bilateral frontalis suspension may be indicated.[21] This procedure is a commonly followed surgical technique with better results in both synkinesis elimination and bilateral symmetry.[22][23] Satisfactory and predictable results were obtained after only unilateral levator excision on the affected side, combined with bilateral frontalis suspension. This leaves the normal functioning levator muscle to elevate the normal eyelid in the primary position but produces a downgaze lag for improved symmetry.[21] Some surgeons advocated performing more resection than normal to avoid under correction. In severe ptosis, a super-maximum (>30 mm) levator resection with frontalis suspension is necessary.[24][25](B3)
Relative contraindications for surgical intervention of MGJWS are poor Bell phenomena, reduced corneal sensations. and dry eye. All these clinical conditions can ultimately result in vision-threatening exposure keratitis.
Differential Diagnosis
The differential diagnosis of Marcus Gunn jaw-winking syndrome (MGJWS) is the other synkinetic abnormalities, like inverted Marcus Gunn Phenomenon and Marin-Amat syndrome. In the inverse Marcus Gunn phenomenon, the ptosis in the primary gaze is worsened with mouth opening as apposed to MGJWS where the ptosis improves with mouth opening. The underlying mechanism in the inverse M-G phenomenon is the abnormal connection between the superior division of the third nerve and the motor division of the fifth nerve supplying the internal pterygoid muscle. A case report on the rare association of classical Marcus Gunn on one side and inverse Marcus Gunn on the other side has been described in the literature. The patient exhibited a "see-saw" pattern of lid movement on opening as well as closing the mouth and on moving the jaw from side to side.[26][26]
In Marin Amat syndrome, there is an abnormal connection between the motor branch of the fifth nerve and frontal, zygomatic branches of the seventh cranial nerve. Here, both eyes close momentarily like blepharospasm with mouth opening secondary to the action of orbicularis oculi muscle.[27][28] Other differential diagnoses of the disease include chronic progressive external ophthalmoplegia, congenital fibrosis syndrome, and myasthenia gravis.
Staging
The amount of jaw winking is the excursion of the upper lid in mm with the opening of the mouth.[5] It is graded into
- Mild (maximum 2 mm)
- Moderate (2 mm-5 mm)
- Severe (higher than 5 mm)
Prognosis
Prognosis is usually good in the majority of cases. With careful monitoring of these patients and treatment, amblyopia can be treated successfully.
Complications
The complications following ptosis surgery include under-correction, overcorrection, lagophthalmos, suture granuloma, slippage of the sling, extrusion of the sling, asymmetric lid crease, and exposure keratitis.[29] The reported prevalence of amblyopia among MGJWS is 30% to 60%.
Deterrence and Patient Education
Marcus Gunn jaw-winking syndrome (MGJWS) will not cause any other symptoms except for jaw-winking in the majority of the individuals. Treatment is only indicated if the disease nature is moderate to severe causing visual disturbances or for cosmetic purposes. Besides, the parents need to be sensitized regarding the ocular and systemic associations of MGJWS as well as the outcomes following ptosis surgery.[29] Also, the significance of periodical follow-up with an ophthalmic health care provider requires emphasis.
Pearls and Other Issues
Affected children with MGJWS should have their periodical vision testing to diagnose amblyopia at an earlier stage and treat accordingly. It is imperative to exclude all the reported ocular and systemic associations with Marcus Gunn jaw-winking syndrome (MGJWS) although they are exceedingly rare. It is crucial to treat amblyopia and strabismus in these patients before proceeding with ptosis surgery. It has been noted in the literature that some children may learn to alter the position of their jaw, which reduces the degree of ptosis in primary gaze; thus, surgery may not be necessary for all children.
Enhancing Healthcare Team Outcomes
It is well reported in the literature that an atypical oculocardiac reflex is easily initiated in these patients so that precautions must be taken for its prevention and early detection during ptosis surgery.[30] The operating surgeons as well as anaesthetists need to be well prepared to tackle these cardiac arrhythmias. Also, a detailed history of any previous anesthetic exposure needs to be elucidated as this syndrome has a high probability of association with malignant hyperthermia.[19]
Media
(Click Image to Enlarge)
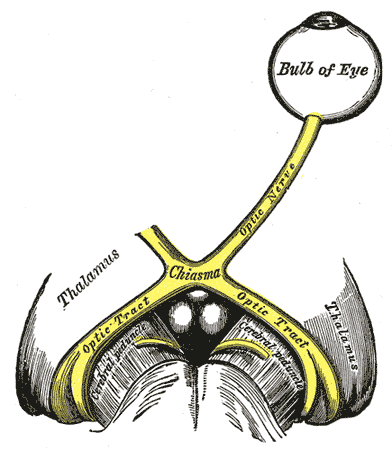
The left optic nerve and the optic tracts. A Marcus Gunn pupil indicates an afferent defect, usually at the level of the retina or optic nerve. Moving a bright light from the unaffected eye to the affected eye would cause both eyes to dilate, because the ability to perceive the bright light is diminished.
Contributed by Wikimedia Commons, Henry Vandyke Carter - Henry Gray (1918) (Public Domain)
References
Pratt SG, Beyer CK, Johnson CC. The Marcus Gunn phenomenon. A review of 71 cases. Ophthalmology. 1984 Jan:91(1):27-30 [PubMed PMID: 6709318]
Level 2 (mid-level) evidenceTraboulsi EI. Congenital cranial dysinnervation disorders and more. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2007 Jun:11(3):215-7 [PubMed PMID: 17572338]
Shah AD, Kumar AB, Kothari K. Bilateral Marcus Gunn jaw winking synkinesis with monocular elevation deficiency: a case report and literature review. International ophthalmology. 2012 Apr:32(2):199-201. doi: 10.1007/s10792-012-9538-0. Epub 2012 Feb 19 [PubMed PMID: 22350119]
Level 3 (low-level) evidenceWeaver RG Jr, Seaton AD, Jewett T. Bilateral Marcus Gunn (jaw-winking) phenomenon occurring with CHARGE association. Journal of pediatric ophthalmology and strabismus. 1997 Sep-Oct:34(5):308-9 [PubMed PMID: 9310920]
Level 3 (low-level) evidenceDemirci H, Frueh BR, Nelson CC. Marcus Gunn jaw-winking synkinesis: clinical features and management. Ophthalmology. 2010 Jul:117(7):1447-52. doi: 10.1016/j.ophtha.2009.11.014. Epub 2010 Feb 25 [PubMed PMID: 20188419]
Level 2 (mid-level) evidenceKannaditharayil D, Geyer H, Hasson H, Herskovitz S. Bilateral Marcus Gunn jaw-winking syndrome. Neurology. 2015 Mar 10:84(10):1061. doi: 10.1212/WNL.0000000000001338. Epub [PubMed PMID: 25754805]
Level 3 (low-level) evidenceZiga N, Biscevic A, Pjano MA, Pidro A. Marcus Gunn Jaw-Winking Syndrome: a Case Report. Medical archives (Sarajevo, Bosnia and Herzegovina). 2019 Aug:73(4):282-284. doi: 10.5455/medarh.2019.73.282-284. Epub [PubMed PMID: 31762566]
Level 3 (low-level) evidenceKhwarg SI, Tarbet KJ, Dortzbach RK, Lucarelli MJ. Management of moderate-to-severe Marcus-Gunn jaw-winking ptosis. Ophthalmology. 1999 Jun:106(6):1191-6 [PubMed PMID: 10366092]
Level 2 (mid-level) evidenceLehman AM, Dong CC, Harries AM, Patel A, Honey CR, Patel MS. Evidence of ancillary trigeminal innervation of levator palpebrae in the general population. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2014 Feb:21(2):301-4. doi: 10.1016/j.jocn.2013.03.029. Epub 2013 Oct 10 [PubMed PMID: 24120706]
Su YH, Ong CT. Marcus Gunn jaw-winking syndrome. Acta neurologica Taiwanica. 2010 Mar:19(1):76-7 [PubMed PMID: 21046852]
Level 3 (low-level) evidenceFreedman HL, Kushner BJ. Congenital ocular aberrant innervation--new concepts. Journal of pediatric ophthalmology and strabismus. 1997 Jan-Feb:34(1):10-6 [PubMed PMID: 9027674]
Level 3 (low-level) evidenceD'Esposito M, Sanna G, Turra MV, CCaccia-Perugini G. [Electromyographic study of the Marcus Gunn phenomenon]. Bulletins et memoires de la Societe francaise d'ophtalmologie. 1970:83():177-87 [PubMed PMID: 5512168]
Rao MV, Syeda A. Jaw-winking movement (Marcus-Gunn phenomenon). Indian journal of medical sciences. 1973 Dec:27(12):925-7 [PubMed PMID: 4790418]
Level 3 (low-level) evidenceAlshamrani AA, Alghulaydhawi FA, Al Shamrani M. Marcus Gunn Jaw-Winking Syndrome Associated with Morning Glory Disc Anomaly. Middle East African journal of ophthalmology. 2019 Jan-Mar:26(1):37-39. doi: 10.4103/meajo.MEAJO_279_18. Epub [PubMed PMID: 31114123]
Dżaman K, Zborowska-Piskadło K, Pietniczka-Załęska M, Kantor I. Marcus Gunn (jaw-winking) phenomenon in pediatric otorhinolaryngology practice. International journal of pediatric otorhinolaryngology. 2019 Feb:117():153-156. doi: 10.1016/j.ijporl.2018.11.035. Epub 2018 Nov 30 [PubMed PMID: 30579071]
Awan KJ. Marcus gunn (jaw-winking) syndrome. American journal of ophthalmology. 1976 Sep:82(3):503-4 [PubMed PMID: 961806]
Level 3 (low-level) evidencePark DH, Choi WS, Yoon SH. Treatment of the jaw-winking syndrome. Annals of plastic surgery. 2008 Apr:60(4):404-9. doi: 10.1097/SAP.0b013e31812f7dc2. Epub [PubMed PMID: 18362569]
Level 3 (low-level) evidenceWong JF, Thériault JF, Bouzouaya C, Codère F. Marcus Gunn jaw-winking phenomenon: a new supplemental test in the preoperative evaluation. Ophthalmic plastic and reconstructive surgery. 2001 Nov:17(6):412-8 [PubMed PMID: 11766020]
Level 2 (mid-level) evidencePandey M, Baduni N, Jain A, Sanwal MK, Vajifdar H. Abnormal oculocardiac reflex in two patients with Marcus Gunn syndrome. Journal of anaesthesiology, clinical pharmacology. 2011 Jul:27(3):398-9. doi: 10.4103/0970-9185.83693. Epub [PubMed PMID: 21897519]
Level 3 (low-level) evidenceTian N, Zheng YX, Zhou SY, Liu JL, Huang DP, Zhao HY. [Clinical characteristics of moderate and severe Marcus-Gunn jaw-winking synkinesis and its surgical treatment]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2007 Dec:43(12):1069-72 [PubMed PMID: 18331673]
Morax S, Mimoun G. [Surgical treatment of the Marcus-Gunn syndrome. Indications and results. Apropos of 15 cases]. Ophtalmologie : organe de la Societe francaise d'ophtalmologie. 1989 Apr-May:3(2):160-3 [PubMed PMID: 2641099]
Level 3 (low-level) evidencePutterman AM. Jaw-winking blepharoptosis treated by the Fasanella-Servat procedure. American journal of ophthalmology. 1973 Jun:75(6):1016-22 [PubMed PMID: 4708631]
Ning Q, Cao J, Xie J, Gao Q, Wang C, Ye J. Unilateral Levator Aponeurosis Excision for Marcus Gunn Syndrome and Risk Factors of Residual Jaw Winking. Journal of ophthalmology. 2019:2019():2058047. doi: 10.1155/2019/2058047. Epub 2019 Nov 4 [PubMed PMID: 31781375]
Betharia SM, Kumar S. Levator sling for Marcus Gunn ptosis. The British journal of ophthalmology. 1987 Sep:71(9):685-9 [PubMed PMID: 3663562]
Sthapit PR, Saiju R. Surgical Outcomes in Cases of Marcus-Gunn Jaw-Winking Phenomenon. Kathmandu University medical journal (KUMJ). 2015 Jan-Mar:13(49):34-7 [PubMed PMID: 26620746]
Level 3 (low-level) evidenceKumar V, Goel N, Raina UK, Ghosh B. "See-saw" Marcus Gunn syndrome. Ophthalmic plastic and reconstructive surgery. 2011 Nov-Dec:27(6):e144-5. doi: 10.1097/IOP.0b013e3182078e15. Epub [PubMed PMID: 21346672]
Level 3 (low-level) evidenceGarcía Ron A, Jensen J, Garriga Braun C, Gómez E, Sierra J. [Marin-Amat and inverted Marcus-Gunn syndrome. Two case reports]. Anales de pediatria (Barcelona, Spain : 2003). 2011 May:74(5):324-6. doi: 10.1016/j.anpedi.2011.01.017. Epub 2011 Mar 4 [PubMed PMID: 21377433]
Level 3 (low-level) evidenceJethani J. Marin-Amat syndrome: a rare facial synkinesis. Indian journal of ophthalmology. 2007 Sep-Oct:55(5):402-3 [PubMed PMID: 17699965]
Level 3 (low-level) evidenceDoucet TW, Crawford JS. The quantification, natural course, and surgical results in 57 eyes with Marcus Gunn (jaw-winking) syndrome. American journal of ophthalmology. 1981 Nov:92(5):702-7 [PubMed PMID: 7304698]
Kwik RS. Marcus Gunn Syndrome associated with an unusual oculo-cardiac reflex. Anaesthesia. 1980 Jan:35(1):46-9 [PubMed PMID: 7396112]
Level 3 (low-level) evidence