Introduction
Hair growth is cyclical, and follicles undergo corresponding phases of growth (anagen), involution (catagen), and quiescence (telogen).[1][2]
Loose anagen hair syndrome (LAS) is a condition inherited in autosomal dominant fashion with incomplete penetrance or as sporadic cases. It is characterized by non-scarring alopecia with increased hair shedding due to poorly anchored anagen hairs. The disease presents most commonly in female children with diffuse thinning and textural changes characterized as unruly.[1] Hairs are easily and painlessly removed during daily activities and reproduced with a hair pull test. On light microscopy, a deformed anagen bulb, absent inner root sheath, and ruffled cuticle are present.[1][3] Histopathologic exam, although not a part of routine diagnosis, reveals premature and defective keratinization of the inner root sheath. Most cases resolve spontaneously, but topical minoxidil may be used as first-line therapy in infants and children.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hair loss is a common phenomenon encountered among physicians. It has a myriad of underlying causes. Loose anagen hair syndrome is a non-scarring alopecia that results from defects of keratinization.[1] Abnormalities are primarily of the inner root sheath of anagen follicles. As opposed to normal anagen follicles that demonstrate dense, compact, well-oriented cells of the inner root sheath and cuticle, hairs of loose anagen hair syndrome exhibit vacuolization and intercellular edema of Huxley cells and dyskeratotic changes in Henle cells and the hair shaft.
The inner root sheath at the level of the bulb normally provides anchoring support for anagen hairs. Degenerative changes as described above disrupt the interdigitation of cuticle cells and inner root sheath leading to hairs easily pulled away by minor trauma.
As the rest of the follicular structure is uninvolved in loose anagen hair syndrome hair replaces itself normally and regrowth is prompt. Clinically this presents as frequent “shedding” of hair and an overall thinned appearance.[3]
Epidemiology
Loose anagen hair syndrome has an estimated incidence of 2 cases per million per year and is either spontaneous or inherited in an autosomal dominant pattern with incomplete penetrance. Most cases occur in young children with light colored hair with an average onset at 3 years of age. This diffuse hair loss must be distinguished from other types of non-scarring alopecia and may account for up to 10% of cases of childhood alopecia.[1]
Pathophysiology
Each hair follicle is divided into bulb, suprabulbar, isthmus, and infundibular zones. Hair collectively participates in the normal hair cycle of anagen, catagen, and telogen (growth, involution, and quiescence respectively). The anagen phase typically lasts for 3 to 5 years with a growth rate of 1 cm per month.[4] Long inner root sheaths cover anagen hairs, and the outer root sheaths are rooted deeply in the reticular dermis. Therefore, under normal circumstances, these are difficult to detach and do not come off with routine hair brushing or light traction. Anagen follicles are continuously and actively replicating and sensitive to nutritional and metabolic insults.[5]
An anagen hair shaft has 3 layers: the medulla, cortex, and cuticle from the center out. The cuticle interlocks with the inner root sheath cuticle and it is abnormal keratinization of this inner root sheath that is central to loose anagen hair syndrome.[5]
A K6HF mutation of keratin has been described in some families with loose anagen hair syndrome.[6] This mutation results in premature keratinization of the inner root sheath and impaired adhesion of the cuticle of the inner root sheath to neighboring structures.[1]
History and Physical
Clinical history is usually that of a young female child with light hair that sheds easily. A classic contextual clue is a history of hair that does not require frequent cutting. The hair is often described to have unusual textures such as "sticky, matted, frizzy, and unmanageable." Often, parents report diffuse hair loss, and despite this, areas of complete hair loss usually are not present. Most commonly thinning is seen over the entire scalp or, as classically associated, the occipital scalp. Involvement of the eyebrows is uncommon but may be seen.[1]
A pull test is the cornerstone of diagnosis in loose anagen hair syndrome. It is performed by using gentle traction on approximately 40 to 60 scalp hairs. Telogen hairs normally represent 10% of scalp hairs, and thus, removal of 4 to 6 hairs is a normal finding in the hair pull test. Loose anagen hair syndrome, similar to telogen effluvium, will result in greater amounts of hair removed. Despite easy removal from the scalp, individual hairs in loose anagen hair syndrome have normal tensile strength and are not brittle. Hairs can be examined under light microscopy by dry-mounting the hair on a glass slide with a cover slip placed over top. In loose anagen hair syndrome anagen, hairs lack inner root sheaths and external root sheaths with a ruffled cuticle.[5] As loose hairs may be seen in unaffected individuals some propose a positive hair test contain 50% or more of anagen hairs.[1]
Evaluation
Diagnosis is usually based upon clinical history, physical exam, and light microscopy. Further stratification into clinical subtypes of loose anagen hair syndrome includes (1) sparse short hair, (2) diffuse or patchy unruly hair, and (3) adults with the excessive shedding of anagen hairs.[7] The utility of this is uncertain as it does not relate to changes in treatment and effect on prognosis is also uncertain. Additional laboratory testing is not routinely necessary.[8] Although usually a solitary self-resolving condition, if other comorbidities occur investigation of underlying syndromic diseases may be needed. Sporadic cases of loose anagen hair syndrome coexisting with Noonan syndrome, neurofibromatosis type 1, atopic dermatitis, trichorhinophalangeal syndrome, nail-patella syndrome, and FG syndrome have been described.[2]
Treatment / Management
Treatment is often unnecessary as the disease is often self-limited and improves with age. If treatment is pursued, topical minoxidil has been used as first-line therapy for those with significant disease burden.[1] The mechanism by which minoxidil is thought to be beneficial is by prolongation of the anagen phase.[3] Biotin therapy has been shown to be of no benefit,[7] and otherwise, only gentle hair care to avoid removal of loosely anchored hairs is recommended.[5](B2)
Differential Diagnosis
Non-Scarring Alopecias of Childhood
- Short anagen syndrome (SAS): Caused by a shortened anagen phase.Similar clinical history (i.e., hair does not grow long and does not require cutting, short hair, diffuse alopecia)
- Distinguished by SAS having a predominance of telogen hairs with trichoscopy and a lack of distinguishing features)
- Similar treatment to loose anagen syndrome [9]
- Telogen effluvium: Also presents as diffuse thinning but is uncommon in childhood. Clinical history may reveal physical or psychological trauma 3 to 4 months preceding onset. Telogen hairs will be seen with light microscopy.
- Aopecia areata: Often focal or diffuse areas of complete hair loss as opposed to the diffuse areas of thinning hair as seen in loose anagen hair syndrome.
- Androgenetic alopecia: Gradual thinning; miniaturization of follicles seen with a frontal or temporal distribution of hair loss. Telogen hair is seen with light microscopy.
- Trichotillomania: Unusual shape and size of hair loss. Often patchy with hairs at different stages of growth. Telogen hairs with fractures on light microscopy.[1]
Hair Shaft Disorders without Increased Fragility
- Uncombable hair syndrome: Clinically hair cannot be combed flat. The entire hair shaft is rigid with a triangular shape. Hair loss is not a predominant feature.
- Pili Annulati: characteristic alternating light and dark bands in the hair shafts that can be seen on clinical and microscopic exam.[5]
Prognosis
Prognosis of those affected by loose anagen hair syndrome is generally good with spontaneous recovery being common and most recovering by adulthood.[1][5]
Complications
Complications are few to none. The psychosocial aspect has not been reviewed. The disease is self-limited, resolves with age, and does not require treatment, and complications from the disease process or iatrogenic are minimal.[1][8]
Consultations
Consultation with a dermatologist may be needed but likely only to establish a diagnosis and distinguish the condition from other causes of non-scarring alopecia in childhood. If presenting as a part of a syndrome, for example, Noonan or neurofibromatosis 1, then appropriate specialists for other organ involvement will be necessary.[1]
Deterrence and Patient Education
- Loose anagen syndrome is an inherited and often self-limited condition resulting in short hair that is easily broken and often does not require cutting.
- Lifestyle modifications that minimize trauma or manipulation of hairs are the best initial form of therapy.
- If treatment is desired topical minoxidil can be tried to lengthen the anagen cycle and reduce shedding.
- The prognosis is generally good with improvement often beginning during adolescence.
Pearls and Other Issues
Loose anagen hair syndrome is an inherited disease diagnosed clinically. Poorly adherent anagen hairs result in easy shedding and non-scarring alopecia. It is important to understand the benign, self-limited nature and good prognosis as the disease typically resolves with age. Distinguishing it from other causes of non-scarring alopecia is paramount, and a dermatologist can facilitate this differentiation. Foundations of treatment revolve around minimizing hair trauma and patient reassurance.[8]
Enhancing Healthcare Team Outcomes
Loose anagen hair syndrome is a disease in which diagnosis is made clinically, and treatment revolves around decreasing trauma to easily detached anagen hairs. As the disease process primarily affects young children, pediatricians and pediatric nurse practitioners and physician assistants are likely to be the first to encounter these patients. Awareness of loose anagen hair syndrome and differentials is crucial for diagnosis, and referral to a dermatologist may assist in providing the best patient care. Discussion with parents revolves around lifestyle modification and minimizing trauma to hair with routine combing, washing, and styling. Treatment may be considered with minoxidil applied topically. Biotin or additional nutritional supplementation has not been shown to be helpful.[1][5][8] (Level V)
Media
(Click Image to Enlarge)
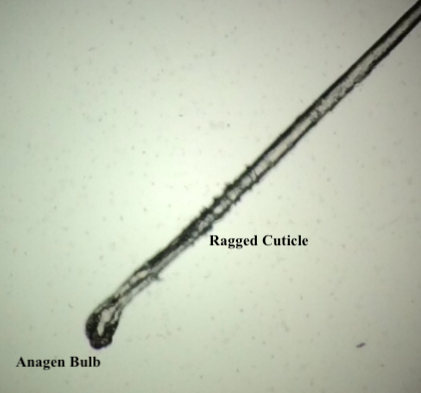
Loose anagen hair syndrome. Note the ragged cuticle and bulb shape denoting anagen hair. Contributed by Christopher Cook DO and Joseph Prohaska DO
References
Cantatore-Francis JL, Orlow SJ. Practical guidelines for evaluation of loose anagen hair syndrome. Archives of dermatology. 2009 Oct:145(10):1123-8. doi: 10.1001/archdermatol.2009.220. Epub [PubMed PMID: 19841399]
Level 2 (mid-level) evidenceFeingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, New M, Purnell J, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Asfour L, Cranwell W, Sinclair R. Male Androgenetic Alopecia. Endotext. 2000:(): [PubMed PMID: 25905192]
Mirmirani P, Uno H, Price VH. Abnormal inner root sheath of the hair follicle in the loose anagen hair syndrome: an ultrastructural study. Journal of the American Academy of Dermatology. 2011 Jan:64(1):129-34. doi: 10.1016/j.jaad.2010.01.026. Epub [PubMed PMID: 21167408]
Baden HP, Kvedar JC, Magro CM. Loose anagen hair as a cause of hereditary hair loss in children. Archives of dermatology. 1992 Oct:128(10):1349-53 [PubMed PMID: 1417022]
Cheng AS, Bayliss SJ. The genetics of hair shaft disorders. Journal of the American Academy of Dermatology. 2008 Jul:59(1):1-22; quiz 23-6. doi: 10.1016/j.jaad.2008.04.002. Epub [PubMed PMID: 18571596]
Chapalain V, Winter H, Langbein L, Le Roy JM, Labrèze C, Nikolic M, Schweizer J, Taïeb A. Is the loose anagen hair syndrome a keratin disorder? A clinical and molecular study. Archives of dermatology. 2002 Apr:138(4):501-6 [PubMed PMID: 11939812]
Zarbo A, Shwayder T. Loose Anagen Hair Syndrome. The Journal of pediatrics. 2018 Aug:199():282-282.e1. doi: 10.1016/j.jpeds.2018.03.005. Epub 2018 Apr 25 [PubMed PMID: 29705113]
Santiago F, Vieira R, Figueiredo A. Loose anagen hair syndrome: an unusual cause of alopecia of cosmetic importance only. Journal of cosmetic dermatology. 2009 Sep:8(3):226-7. doi: 10.1111/j.1473-2165.2009.00450.x. Epub [PubMed PMID: 19735522]
Level 3 (low-level) evidenceOberlin KE, Maddy AJ, Martínez-Velasco MA, Vázquez-Herrera NE, Schachner LA, Tosti A. Short anagen syndrome: Case series and literature review. Pediatric dermatology. 2018 May:35(3):388-391. doi: 10.1111/pde.13478. Epub 2018 Mar 26 [PubMed PMID: 29582461]
Level 2 (mid-level) evidence