Introduction
Leukemia cutis characteristically demonstrates the infiltration of the skin by neoplastic leukocytes.[1] While the extramedullary collection of leukemic cells is generally regarded as myeloid sarcoma (previously chloroma/granulocytic sarcoma), leukemia cutis is a generic term to describe specific cutaneous involvement. Although any subtype of leukemia can involve the skin, the most common types seen in clinical practice are chronic lymphocytic leukemia (CLL) and acute myeloid leukemia (AML) with monocytic or myelomonocytic morphology.[2] Involvement by chronic myeloid leukemia (CML) is extremely rare and may be indicative of the blast phase. Patients usually have a prior diagnosis of systemic leukemia or myelodysplasia. However, cutaneous lesions may present as the primary manifestation of systemic disease in rare cases. Cutaneous involvement is generally indicative of advanced disease and should stipulate the investigation of other body sites for extramedullary involvement.
Subtypes of Leukemia Involving Skin:
Myeloid/monocytic disorders:
- Acute myeloid leukemia (monocytic or myelomonocytic) (AML)
- Chronic myeloid leukemia
- Chronic myelomonocytic leukemia (transformation)
- Myelodysplastic syndrome (transformation)
Lymphoproliferative disorders:
- B- cell leukemia/lymphomas
- Precursor B-cell acute lymphoblastic leukemia
- Chronic lymphocytic leukemia (CLL)
- Hairy cell leukemia
- T- cell leukemia/lymphomas
- Precursor T-cell acute lymphoblastic leukemia
- Adult T-cell leukemia/lymphoma (ATLL)
- T- cell prolymphocytic leukemia
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Both genetic and environmental components are involved in the etiology of any leukemia and are responsible for maturation arrest and clonal expansion of precursor cells. While the neoplastic cells carry the genetic abnormality of underlying leukemia, aneuploidy of chromosome 8, chromosome 3 translocations and t(6;9) are particularly notable in patients with leukemia cutis.[3] Environmental risk factors for leukemia cutis are same as for developing any systemic leukemia and include benzene, ionizing radiation, alkylating and viral agents. Use of all-trans retinoic acid (ATRA) to treat acute promyelocytic leukemia may increase the risk of extramedullary involvement including the skin.[4]
Epidemiology
Leukemia cutis is rare, and the exact data on incidence and demographic predilections do not exist. However, children with congenital leukemia are prone to develop leukemia cutis, ranging from 25% to 30% of cases.[5] Although the highest rate of leukemia cutis occurs in patients with adult T-cell leukemia/lymphoma (ATLL), the incidence of this leukemia is quite rare. Thus the most common subtypes seen in clinical practice are AML and CLL involving 13% and 8% of total cases, respectively.
Majority of skin lesions occur in patients already diagnosed with leukemia (55% to 77%), cutaneous lesions may appear at the presentation of systemic leukemia (23% to 44%), or even precede the development of leukemia in the peripheral blood and/or bone marrow in 2% to 3% of cases.[3] This latter condition termed as "aleukemic" cutis eventually develops AML.[6][7][8]
Pathophysiology
The pathophysiology of leukemia cutis involves the migration of leukemic cells into the skin. The exact mechanism is unknown, but recent molecular analysis is beginning to provide more information on cell-cell interaction and the role of adhesion molecules. Mechanisms involving various chemokines and the molecular expression on leukemic cells mediating the migration of leukemic cells to the skin via skin-selective homing processes are the proposed etiology.[9][10]
Histopathology
Histology of skin biopsy shows nodular or diffuse infiltrates of leukemic cells in the dermis and/or subcutaneous tissue. These lesions spare the epidermis along with a narrow band of uninvolved upper dermis known as the grenz zone. However T-cell leukemia including ATLL may show epidermotropism. The size of cells varies depending on the subtype of leukemia. CLL cells are smaller, mature-appearing cells that may show perivascular, periadnexal, or nodular distribution. Myeloid leukemia cells are larger with high nuclear to cytoplasmic ratio, often prominent nucleoli and involving dermis and subcutis in a diffuse pattern. Immunohistochemical staining and history remain essential to distinguish reactive from neoplastic infiltrates.
History and Physical
The clinical and morphological findings of leukemia cutis vary widely. These lesions may be localized or disseminated and may occur alone or in combination on any site of the skin.[11] Leukemia cutis may also present as diffuse purpura and is one of the causes of blueberry muffin syndrome in infants.
Common findings:
- Papules and nodules (60%) - nodules are typically firm, or rubbery in consistency
- Plaques
Rare findings (combined appearance and transitions between individual morphologies are possible)
- Erythema
- Erythroderma
- Ulcer
- Blisters
- Colors: Red, brown, yellow, blue, gray, hemorrhagic, purpuric, deep lesions may have skin-colored surfaces
Distribution:
- No predilection sites - head, trunk, and extremities are equally affected
- Singular, grouped or disseminated
- Exanthematous spread
Involvement of oral mucosa:
- Gingival hyperplasia
- Nodules, ulcers
Evaluation
In the absence of established systemic leukemia, confirming the diagnosis of suspected cases of leukemia cutis proves to be challenging. In all cases, a judicious correlation between clinical features, histopathology, and immunophenotyping is necessary.
A complete blood count and peripheral smear must be performed to assess abnormalities in cell counts (cytopenias generally present) and evidence of circulating leukemic cells. A bone marrow biopsy is imperative for the definitive diagnosis of systemic leukemia. In addition to immunohistochemistry, biopsy samples should have cytogenetics and flow cytometry studies.
A skin biopsy and immunophenotyping must be performed in all suspected patients, regardless of prior leukemia history, as transformation or development of different leukemia may occur. The identification of leukemia can be performed based on CD markers. Common CD markers associated with each of the leukemias are below in table 1.
Other appropriate tests needed may include coagulation studies, complete metabolic profile, liver and kidney function tests, uric acid, and lactate dehydrogenase. If the patient develops high unrelenting fevers, especially during the course of treatment, an infectious workup is necessary as these patients are immunocompromised and prone to infections.
A thorough search for other sites of systemic involvement is crucial. Imaging studies can invariably help to determine the extent of systemic involvement.
Treatment / Management
Treatment of leukemia cutis points toward addressing underlying leukemia using aggressive systemic chemotherapy. Systemic chemotherapy for leukemia depends on cancer subtype. Usually, remission of hematological abnormalities occurs concurrently with complete or partial resolution of cutaneous lesions. While chemotherapy is the mainstay of treatment, radiation therapy, in the form of electron beam therapy may be used for refractory or palliative cases.[12][13](B3)
Differential Diagnosis
The differential diagnosis of leukemia cutis is broad, as a wide range of neoplastic, inflammatory, and infectious skin lesions can mimic the lesions both clinically and on histologic examination.[14][15]
Some of the common diseases that may appear similar to leukemia cutis lesions are as follows. One should keep in mind that the list is not exhaustive, and these entities may appear in conjunction with leukemia cutis.
- Lymphoma and pseudolymphoma
- Metastatic solid tumors
- Pyoderma gangrenosum
- Vasculitis
- Drug reactions
- Urticaria
- Viral exanthem
- Hidradenitis
- Erythema multiforme
- Erythema nodosum
- Infections due to immune suppression: cellulitis, herpes zoster, herpes simplex
- Graft vs. host disease
Toxicity and Adverse Effect Management
Patients on chemotherapy should be monitored for infections and receive prophylaxis for common infectious agents.
Medical Oncology
Initial treatment of myeloid leukemia is based on age, history of prior myelodysplastic syndrome or cytotoxic chemotherapy, and performance status. The use of cytogenetics and molecular markers gained through next-generation sequencing is necessary for risk stratification and can guide upfront frontline therapy. Several molecular markers such as FLT3, NPM1, CEBPA, IDH, And other mutations are important for risk assessment. However, although karyotyping and molecular markers are robust predictors of disease-free survival, induction chemotherapy is often initiated before this information is available. Standard induction regimens have as their basis the backbone of cytarabine in combination with anthracycline popularly known as the 7+3 regimen. The therapy intends to reduce the leukemic burden and restore normal hematopoiesis. For people that are found to be FLT3 mutated, midostaurin, an FLT3 inhibitor to both ITD and TKD mutations, is now added to standard chemotherapy as part of frontline treatment based on the RATIFY Alliance Trial.
Prognosis
Leukemia cutis is regarded as a systemic manifestation of underlying leukemia and generally carries an unfavorable prognosis.[16]
While some patients can experience remission of skin lesions after systemic chemotherapy, a diagnosis of leukemia cutis strongly correlates with additional sites of extramedullary involvement, with meninges being the most common site of spread (40%).[8]
A 2-year follow-up in AML patients showed a 6% survival rate with skin involvement vs. 30% in those without skin infiltrates.[17]
Complications
Many of the complications are the result of underlying leukemia or its treatment, and not specifically as a result of cutaneous skin lesions.
- Patients with leukemia are prone to a variety of opportunistic infections due to pancytopenia
- Bleeding is a result of thrombocytopenia or as a result of erosion of skin lesions
- Reactions to chemotherapy
- Mass effect if leukemia cutis manifests as a tumor
Consultations
- A dermatologist is typically the primary clinician sought to identify and differentiate various skin lesions
- A hematologist-oncologist is generally on board for the management of underlying leukemia
- A bone marrow transplant physician may be involved, if the patient is a candidate for bone/stem cell transplant
- A radiation oncologist may be deemed necessary for skin-directed therapy
- A dermatopathology/hematopathology consultation remains essential for definitive diagnosis and subtyping of leukemia
Enhancing Healthcare Team Outcomes
An understanding of the various presentations of leukemia cutis and a complete history of the patient is essential as the lesions can easily be confused with other diagnoses. Given this, the recommendation is that evidence-based guidelines be utilized to manage and treat all cases of leukemia cutis. When available, morphology and immunophenotype of the prior systemic leukemia should be reviewed by the pathologist to match the neoplastic clones in the skin.
The interprofessional team should include healthcare professionals from a broad range of disciplines to coordinate care, including dermatologists, oncologists, bone marrow transplant physicians, radiation oncologists, and dermatopathology/hematopathology pathologists, as well as oncology specialty trained nursing, and pharmacists. The high morbidity and mortality of leukemia cutis reiterate the necessity for reliable communication between involved providers and the need for aggressive treatment. interprofessional hematologic, dermatologic and pathology follow up is essential in all patients, even those in remission, for prompt identification of cutaneous recurrences [level V].
Media
(Click Image to Enlarge)
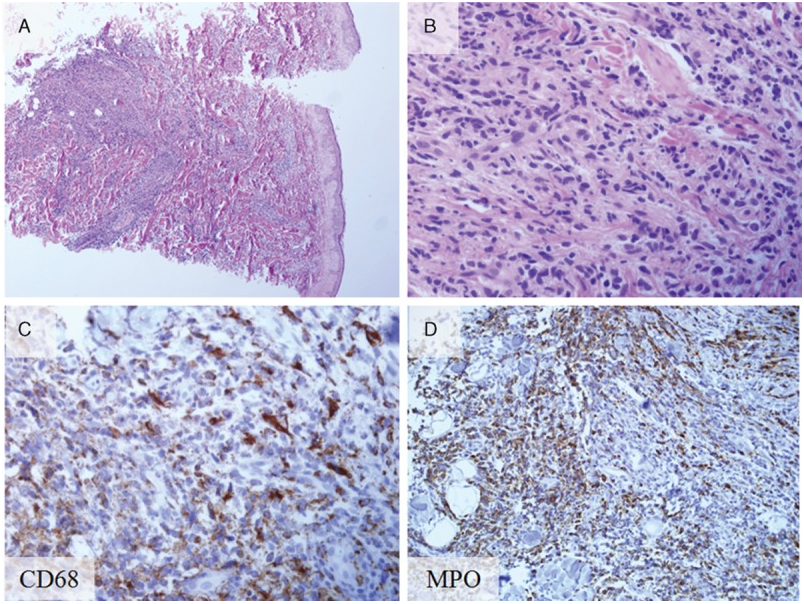
Histopathology and immunohistochemical staining of biopsy from the skin leukemia cutis. (A) Leukemic cell infiltration beneath the epidermis (hematoxylin and eosin stain; original magnification ×40). (B) Magnified view of the leukemic cell infiltration (hematoxylin and eosin stain; original magnification ×400). (C) CD68-positive cells (CD68 staining; original magnification ×400). (D) Myeloperoxidase-positive (MPO) cells (MPO staining; magnification ×400). MPO cells = myeloperoxidase-positive cells. contributed by http://creativecommons.org/licenses/by-nd/4.0
(Click Video to Play)
(Click Image to Enlarge)
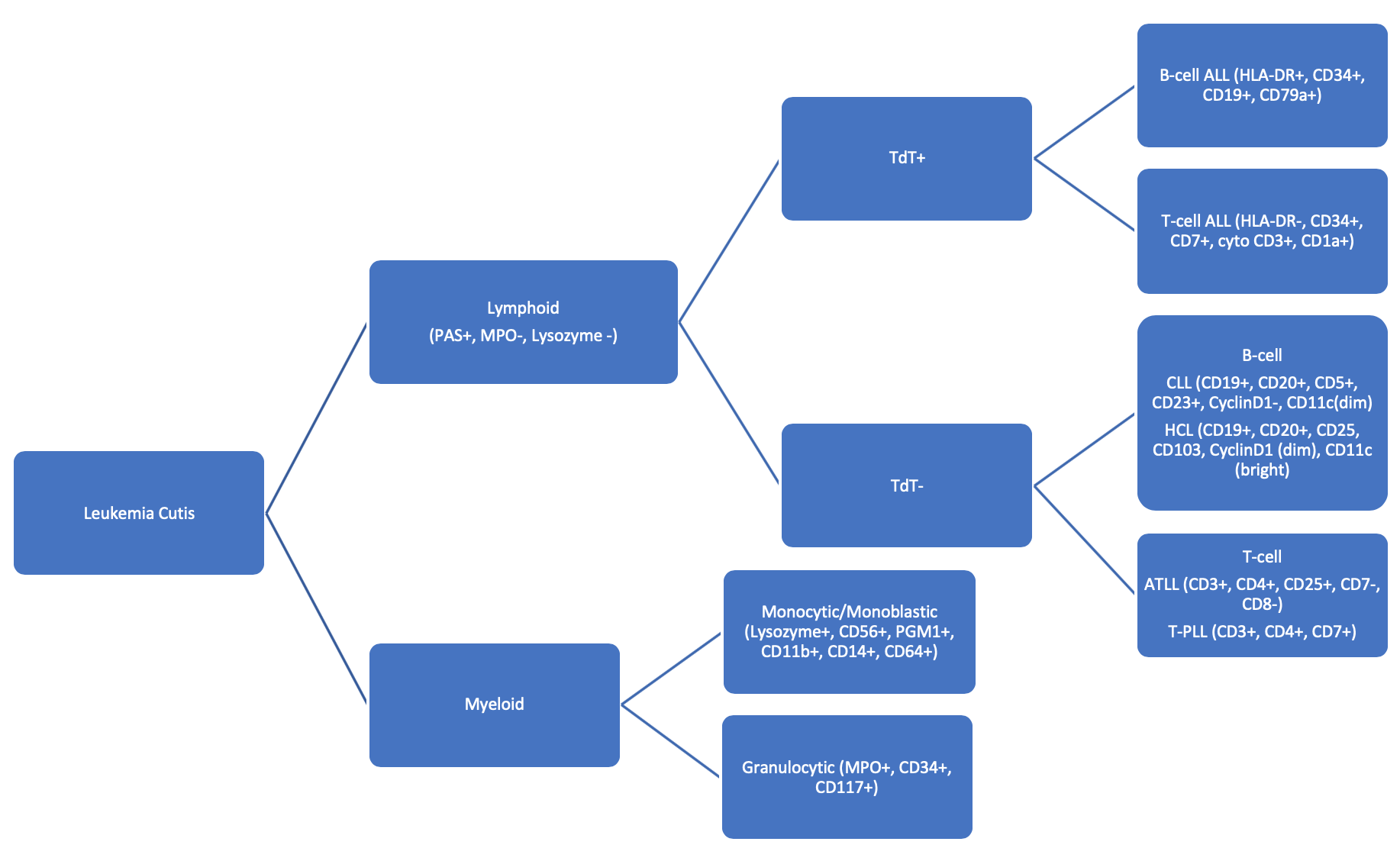
Flow chart with a brief description of cytochemical and immunohistochemical markers to differentiate subtypes of leukemias involving the skin. Contributed by Aadil Ahmed, MD
(Click Image to Enlarge)

Leukemic cutis Image courtesy S Bhimji MD
References
Obiozor C, Ganguly S, Fraga GR. Leukemia cutis with lymphoglandular bodies: a clue to acute lymphoblastic leukemia cutis. Dermatology online journal. 2015 Aug 15:21(8):. pii: 13030/qt6m18g35f. Epub 2015 Aug 15 [PubMed PMID: 26437164]
Wagner G, Fenchel K, Back W, Schulz A, Sachse MM. Leukemia cutis - epidemiology, clinical presentation, and differential diagnoses. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2012 Jan:10(1):27-36. doi: 10.1111/j.1610-0387.2011.07842.x. Epub 2011 Nov 17 [PubMed PMID: 22115500]
Ratnam KV, Khor CJ, Su WP. Leukemia cutis. Dermatologic clinics. 1994 Apr:12(2):419-31 [PubMed PMID: 8045053]
Giralt S, O'Brien S, Weeks E, Luna M, Kantarjian H. Leukemia cutis in acute promyelocytic leukemia: report of three cases after treatment with all-trans retinoic acid. Leukemia & lymphoma. 1994 Aug:14(5-6):453-6 [PubMed PMID: 7812204]
Level 3 (low-level) evidenceZhang IH, Zane LT, Braun BS, Maize J Jr, Zoger S, Loh ML. Congenital leukemia cutis with subsequent development of leukemia. Journal of the American Academy of Dermatology. 2006 Feb:54(2 Suppl):S22-7 [PubMed PMID: 16427986]
Level 3 (low-level) evidenceAgis H, Weltermann A, Fonatsch C, Haas O, Mitterbauer G, Müllauer L, Schreiber S, Schwarzinger I, Juretzka W, Valent P, Jäger U, Lechner K, Geissler K. A comparative study on demographic, hematological, and cytogenetic findings and prognosis in acute myeloid leukemia with and without leukemia cutis. Annals of hematology. 2002 Feb:81(2):90-5 [PubMed PMID: 11907789]
Level 2 (mid-level) evidenceSu WP, Buechner SA, Li CY. Clinicopathologic correlations in leukemia cutis. Journal of the American Academy of Dermatology. 1984 Jul:11(1):121-8 [PubMed PMID: 6736347]
Baer MR, Barcos M, Farrell H, Raza A, Preisler HD. Acute myelogenous leukemia with leukemia cutis. Eighteen cases seen between 1969 and 1986. Cancer. 1989 Jun 1:63(11):2192-200 [PubMed PMID: 2785843]
Level 3 (low-level) evidenceCho-Vega JH, Medeiros LJ, Prieto VG, Vega F. Leukemia cutis. American journal of clinical pathology. 2008 Jan:129(1):130-42 [PubMed PMID: 18089498]
Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011 Oct 6:118(14):3785-93. doi: 10.1182/blood-2011-04-347229. Epub 2011 Jul 27 [PubMed PMID: 21795742]
Seymour JF, Pierce SA, Kantarjian HM, Keating MJ, Estey EH. Investigation of karyotypic, morphologic and clinical features in patients with acute myeloid leukemia blast cells expressing the neural cell adhesion molecule (CD56). Leukemia. 1994 May:8(5):823-6 [PubMed PMID: 7514247]
Level 3 (low-level) evidenceElsayad K, Oertel M, Haverkamp U, Eich HT. The effectiveness of radiotherapy for leukemia cutis. Journal of cancer research and clinical oncology. 2017 May:143(5):851-859. doi: 10.1007/s00432-016-2338-6. Epub 2017 Jan 16 [PubMed PMID: 28093639]
Zweegman S, Vermeer MH, Bekkink MW, van der Valk P, Nanayakkara P, Ossenkoppele GJ. Leukaemia cutis: clinical features and treatment strategies. Haematologica. 2002 Apr:87(4):ECR13 [PubMed PMID: 11940495]
Level 3 (low-level) evidenceSambasivan A, Keely K, Mandel K, Johnston DL. Leukemia cutis: an unusual rash in a child. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2010 Feb 9:182(2):171-3. doi: 10.1503/cmaj.090703. Epub 2009 Nov 9 [PubMed PMID: 19901041]
Level 3 (low-level) evidencePaydas S, Sahin B, Zorludemir S. Sweet's syndrome accompanying leukaemia: seven cases and review of the literature. Leukemia research. 2000 Jan:24(1):83-6 [PubMed PMID: 10634651]
Level 3 (low-level) evidencePaydaş S, Zorludemir S. Leukaemia cutis and leukaemic vasculitis. The British journal of dermatology. 2000 Oct:143(4):773-9 [PubMed PMID: 11069455]
Kaddu S, Zenahlik P, Beham-Schmid C, Kerl H, Cerroni L. Specific cutaneous infiltrates in patients with myelogenous leukemia: a clinicopathologic study of 26 patients with assessment of diagnostic criteria. Journal of the American Academy of Dermatology. 1999 Jun:40(6 Pt 1):966-78 [PubMed PMID: 10365929]