Introduction
The laryngeal muscles are critical to voice production, breathing, and airway protection during swallowing. These muscles are categorized into intrinsic and extrinsic based on their location and function (see Image. Laryngeal Muscles).
Intrinsic laryngeal muscles are confined within the larynx and are primarily responsible for controlling sound production by adjusting the vocal cords' tension, length, and position. The primary intrinsic muscles include the cricothyroid, thyroarytenoid, lateral and posterior cricoarytenoid, and interarytenoid muscles. These muscles are innervated by branches of the vagus nerve, particularly the recurrent laryngeal nerve (RLN). The cricothyroid is the exception, as this muscle is innervated by the external branch of the superior laryngeal nerve (SLN).[1][2]
On the other hand, extrinsic laryngeal muscles have one attachment site outside the larynx and play a role in positioning and stabilizing the larynx during swallowing and speech. These muscles include the suprahyoid muscles, including the digastric, stylohyoid, mylohyoid, and geniohyoid, and the infrahyoid muscles, including the sternohyoid, sternothyroid, thyrohyoid, and omohyoid. The suprahyoid muscles elevate the larynx, while the infrahyoid muscles depress the larynx.[3][4]
The intricate coordination of these muscles ensures that the larynx functions effectively during phonation and airway protection. Surgical interventions involving the laryngeal muscles and nerves require a detailed understanding of their anatomy and innervation to prevent complications such as voice changes and aspiration.[5]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The larynx is a cartilaginous skeleton with intricate neuromuscular control. The hyoid is the only bone in the larynx and articulates with many extrinsic laryngeal muscles. The anterior prominence of the thyroid cartilage is a notable external landmark of the larynx. The hyoid bone is palpable superiorly, and the thyroid gland is palpable inferiorly.
The larynx is divided into the supraglottis, glottis, and subglottis. The cartilages of the supraglottis are the epiglottis, 2 arytenoids, and 2 corniculates. The arytenoid cartilages contain medial vocal processes from which the vocal ligaments extend anteriorly to the thyroid cartilage. The vestibular folds, the false cords, are mucosal folds positioned superolateral to the vocal ligaments. The lateral surfaces of the arytenoids contain the muscular processes to which several intrinsic laryngeal muscles attach.[6]
The aryepiglottic folds connect the arytenoids' superior surfaces to the epiglottis' lateral borders. The arytenoids' inferior surfaces articulate with the cricoid cartilage. The corniculate cartilages are superior to the arytenoids and do not have muscular insertions. The cuneiform cartilages exist as sesamoid cartilages within the aryepiglottic folds.
The glottis is understood to be functionally divided into the phonatory (anterior glottis) and respiratory (posterior glottis) portions. The supraglottis and subglottis define the boundaries of the glottis. The superior border is located at the midpoint of the ventricle, while the inferior border is situated 1 cm below the vocal folds.
The most inferior portion of the larynx is the subglottis, extending from 1 cm below the vocal ligaments to the cricoid cartilage's inferior border.[7] The major cartilaginous structures of the subglottis are the cricoid and thyroid cartilages. The cricoid cartilage is the only cartilaginous structure of the larynx to surround the airway. Extending superiorly from the cricoid cartilage is the conus elasticus, which thickens at its most superior border to form the vocal ligaments of the glottis.[8]
The larynx is critical to respiration, airway protection during deglutition, and phonation. During respiration, vocal folds are optimally in abduction, increasing the glottis' total area to facilitate the work of breathing. When swallowing, the epiglottis is pulled posteroinferiorly to cover the glottis, allowing the bolus to pass safely into the hypopharynx and esophagus without compromising the airway. During phonation, the vocal ligaments, muscles, and overlying mucosa are tensed and adducted to vibrate at frequencies appropriate for human speech.[9]
Embryology
Laryngeal development begins approximately during the 3rd week of gestation with the generation of the laryngotracheal groove in the 6th pharyngeal arch. This groove eventually deepens to form the laryngotracheal diverticulum, also known as the lung bud. The diverticulum extends rostrally, giving rise to the trachea and the rest of the lower respiratory system. The laryngeal mucosa derives from the endoderm of the pharyngeal arches, whereas laryngeal cartilage and musculature arise from the mesoderm.
Most laryngeal structures develop from the 4th pharyngeal arch, including the thyroid cartilage, cuneiform cartilages, part of the epiglottis, SLN, cricopharyngeus muscles, and cricothyroid muscles, and the 6th pharyngeal arch, including the RLNs, the cricoid, arytenoid, and corniculate cartilages, and the remaining intrinsic muscles. The 2nd pharyngeal arch gives rise to most of the hyoid bone, while the 3rd pharyngeal arch engenders the greater cornu of the hyoid and a portion of the epiglottis.
By the 10th week of gestation, the laryngeal inlet develops a covering membrane.[10] This membrane recanalizes, opening the larynx to the lower respiratory system and forming the laryngeal vestibule.
Blood Supply and Lymphatics
Superior Larynx
The blood supply to the superior larynx originates from branches of the thyroid arteries. The superior thyroid artery diverges from the external carotid artery inferior to the greater cornu of the hyoid bone and gives rise to 2 laryngeal branches: the superior laryngeal and cricothyroid arteries. The superior laryngeal artery follows the course of the internal branch of the SLN and pierces the thyrohyoid membrane to perfuse the superior structures of the larynx. The cricothyroid artery predominantly supplies the cricothyroid muscle.
Inferior Larynx
The blood supply to the inferior larynx comes from the thyrocervical trunk via the inferior thyroid artery. This artery gives rise to the inferior laryngeal artery, which runs anterior to the inferior pharyngeal constrictor muscle and posterior to the trachea, following the path of the RLN.
Laryngeal Venous Drainage
Laryngeal venous drainage follows a similar pattern to its supply. Arteries and veins form an anastomotic network around the larynx, forming good collateral circulation.
Laryngeal Lymphatic Drainage
Lymphatic drainage is important to understand due to the aggressive metastasis of some laryngeal cancers. Lymphatic drainage varies individually, but consistencies exist. Supraglottic structures drain lymph to the deep cervical lymph nodes, which can further subdivide into levels. Subglottic structures drain lymph to the paratracheal and pretracheal lymph nodes.
Nerves
Laryngeal innervation arises from the vagus nerve (cranial nerve X), which innervates the intrinsic laryngeal musculature. The extrinsic musculature innervation divides between the vagus nerve and the cervical rootlets.
The laryngeal branches of the vagus nerve are the SLN and the RLN. The SLN has external and internal branches. The external branch primarily carries somatic motor fibers to the cricothyroid muscle.[11] The internal branch enters the larynx through a foramen in the thyrohyoid membrane, with the superior laryngeal artery providing somatosensory innervation to the mucosa of the glottis and supraglottis.
The RLN branches are inferior to the SLN and supply motor sensation to the remaining intrinsic laryngeal muscles. The nerve also carries somatosensory fibers to the subglottis and upper trachea.[12] Due to embryologic anatomical differences, the left RLN's course differs from that of its right-sided counterpart. The right RLN descends anterior to the subclavian artery and then ascends posteriorly toward the larynx. The left RLN courses around the aorta posterior to the ligamentum arteriosum, which connects the pulmonary trunk to the arch of the aorta.
The ansa cervicalis is a neural loop in the neck that innervates the infrahyoid muscles, which include the sternohyoid, sternothyroid, and omohyoid muscles. The thyrohyoid—another infrahyoid muscle—receives innervation from the cervical plexus via the hypoglossal nerve (cranial nerve XII). The ansa cervicalis is formed by the union of the ventral rami of the first 3 or 4 cervical spinal nerves, comprising both superior and inferior roots.[13]
The suprahyoid muscles, which include the mylohyoid, geniohyoid, stylohyoid, and digastric, are innervated by different nerves. The mylohyoid is innervated by the mylohyoid nerve, a branch of the inferior alveolar nerve, which diverges from the mandibular nerve (cranial nerve V3), a branch of the trigeminal nerve (cranial nerve V). The geniohyoid is innervated by fibers from the 1st cervical nerve (C1) that travel with the hypoglossal nerve (cranial nerve XII). The stylohyoid is innervated by the facial nerve (cranial nerve VII).
The digastric muscle has 2 bellies with different innervations. The anterior belly is innervated by the mylohyoid nerve (a branch of the mandibular nerve). The posterior belly is innervated by the facial nerve (cranial nerve VII). Pharyngeal branches from the vagus nerve innervate the pharyngeal constrictors, which act with the suprahyoid muscles to elevate the larynx during swallowing.[14][15]
Muscles
The intrinsic laryngeal muscles serve various functions, many of which can be categorized by their action on the vocal ligament. The adductors are the thyroarytenoid (vocalis), lateral cricoarytenoid, and interarytenoid muscles. The thyroarytenoid originates from the oblique line of the thyroid cartilage and inserts on the anterior surface of the ipsilateral arytenoid cartilage. This muscle's functions include adducting the ipsilateral cord and decreasing the tension of the vocal ligament to modulate pitch. The lateral cricoarytenoid, which originates from the lateral cricoid cartilage and inserts on the muscular process of the arytenoid, adducts the ipsilateral cord and internally rotates the arytenoid.
The interarytenoid (transverse arytenoid) muscle works synergistically with the lateral cricoarytenoid to maintain glottic closure when the cords are adducted. This muscle originates from the medial aspect of the arytenoid cartilage and inserts onto the contralateral interarytenoid muscle.
The sole abductor of the vocal ligament is the posterior cricoarytenoid. This muscle originates from the posterior cricoid and inserts onto the posterior muscular process of the ipsilateral arytenoid. The posterior cricoarytenoid abducts and externally rotates the arytenoid in antagonism to the lateral cricoarytenoid muscle. The cricothyroid muscle originates from the anterolateral surface of the cricoid and inserts on the inferolateral surface of the thyroid cartilage. This muscle displaces the thyroid cartilage downward and tenses the vocal cords when contracted. The cricothyroid is the only intrinsic laryngeal muscle that receives innervation from the external branch of the SLN instead of the RLN.
The epiglottis is drawn posteriorly over the laryngeal inlet to prevent bolus aspiration. The aryepiglottic muscles originate from the apex of the arytenoids and insert on the lateral epiglottic borders. Similarly, the oblique arytenoid muscles originate from the arytenoid apex and insert on the aryepiglottic folds. The thyroepiglottic muscle arises from the internal surface of the thyroid cartilage and inserts on the margin of the epiglottis. Contraction of this muscle inferiorly displaces the epiglottis. The muscles in this area work synergistically to close the laryngeal inlet by pulling the epiglottis posteriorly and inferiorly.
Several cervical muscles act extrinsically on the larynx to aid in phonation and swallowing. Muscles inserted on the superior aspect of the hyoid (geniohyoid, digastric, mylohyoid, thyrohyoid, and stylohyoid muscles) and pharynx (stylopharyngeus, palatopharyngeus, and pharyngeal constrictor muscles) act in conjunction to elevate the larynx. Those muscles inserted on the inferior surface of the hyoid (sternohyoid and omohyoid muscles) and the sternothyroid muscle act to depress the larynx. Physical examination maneuvers to examine the thyroid often involve the patient voluntarily swallowing to localize this gland better because of laryngeal elevation during swallowing.
Physiologic Variants
Slight variations in the laryngeal musculature can affect voice quality and tone. The differences in voice quality are apparent between male and female larynxes. In men, testosterone thickens the vocal ligaments, causing deeper voice quality. The strength and fine control of the muscles are acquired from use. Singers can improve fine motor control over their intrinsic laryngeal muscles through years of practice to better modulate pitch. Though anatomic variations can exist in the musculature, cartilaginous variations are more frequent, with the thyroid cartilage most commonly involved.[16]
Laryngeal muscle innervation frequently appears as described above, though variants are common. The SLN and RLN branches often form a plexus, and aberrant branches provide motor innervation to nearby muscles.[17]
Surgical Considerations
The internal, external, and recurrent laryngeal nerves are critical for voice production and airway protection. These nerves are vulnerable to injury during neck and thyroid surgeries.
Injury to the internal laryngeal nerve can lead to a loss of sensation in the laryngeal mucosa, increasing the risk of aspiration. The nerve passes through the thyrohyoid membrane alongside the superior laryngeal artery, making it susceptible to damage during surgical procedures involving the upper thyroid pole or the carotid artery.
The external laryngeal nerve is at risk during thyroidectomy due to its proximity to the superior thyroid artery. Identifying and preserving this nerve is crucial to prevent postsurgical vocal changes. Surgeons often use anatomical landmarks and intraoperative neuromonitoring to minimize injury to this nerve.[18]
The RLN's course is highly variable, often running in the tracheoesophageal groove and looping under the aortic arch on the left or the subclavian artery on the right. The nerve is particularly vulnerable during thyroid, parathyroid, and thoracic procedures, including lung biopsy and aortic aneurysm repair. Injuries to the RLN can cause vocal cord paralysis, leading to hoarseness, breathing difficulties, and aspiration. Techniques such as careful dissection, the use of anatomical landmarks like the Berry ligament and Zuckerkandl tubercle, and intraoperative nerve monitoring have been shown to reduce the incidence of RLN injury.[19][20]
Hoarseness is a frequent complaint following long surgeries or prolonged intensive care admissions. Often, the patient's hoarseness is related to trauma from intubation. Risk factors for intubation-related laryngeal injury include prolonged intubation (greater than 36 hours), intubation without myorelaxant drugs, the use of large endotracheal tubes, aspiration, and the presence of a nasogastric tube.[21] Vocal cord paralysis occasionally occurs due to prolonged RLN compression between the endotracheal tube balloon and the thyroid cartilage in the subglottis.
Clinical Significance
Assessing laryngeal function and mobility is valuable for both the otolaryngologist and primary care physician. In the outpatient setting, primary care physicians can use laryngeal mirrors to visualize the larynx for basic screening to investigate foreign bodies, masses, or inflammation. An otolaryngologist or another trained practitioner can use a flexible laryngoscope to better assess laryngeal function and visualize anatomy.
After the nasal administration of a topical anesthetic, the scope is passed through the nasopharynx as far as the patient can tolerate. Performing this well-tolerated procedure in an alert patient allows for outpatient visualization of the dynamic larynx. Rigid laryngoscopy under sedation is necessary for most diagnostic visualization procedures and biopsies.
Hoarseness and dysphagia may arise from various conditions, including trauma, stroke, malignancy, neuromuscular disorders, and psychiatric illnesses. An appropriate differential may be generated based on demographics, exposures, and a detailed history.
Media
(Click Image to Enlarge)
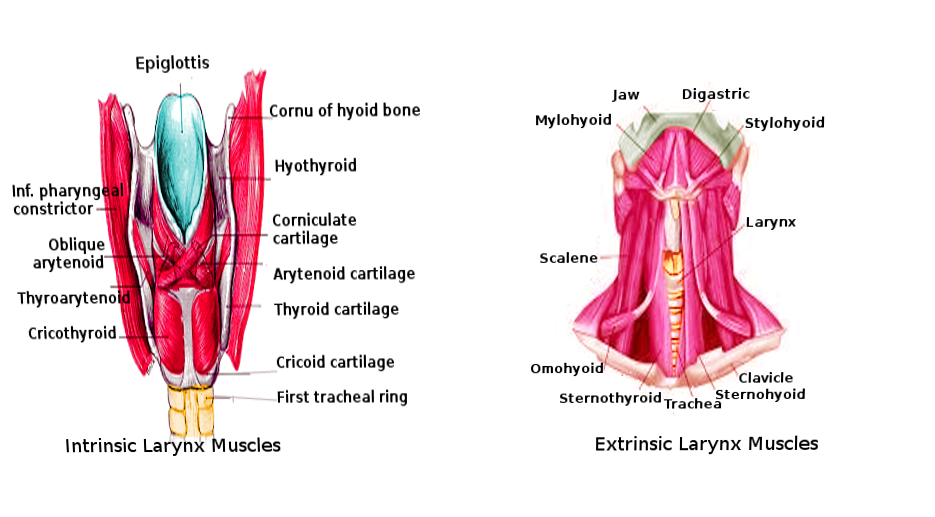
Laryngeal Muscles. These images show the anatomic relationships between the intrinsic and extrinsic laryngeal muscles. Structures in the left image include the epiglottis, cornu of the hyoid bone, hyothyroid, laryngeal cartilages (corniculate, arytenoid, thyroid, and cricoid), 1st tracheal ring, inferior pharyngeal constrictor, and laryngeal muscles (oblique arytenoid, thyroarytenoid, and cricothyroid). Structures in the right image include the jaw, digastric, stylohyoid, larynx, clavicle, sternohyoid, trachea, sternothyroid, omohyoid, scalene, and mylohyoid.
Image courtesy Orawan
References
Benner A, Sharma P, Sharma S. Anatomy, Head and Neck: Cervical, Respiratory, Larynx, and Cricoarytenoid. StatPearls. 2024 Jan:(): [PubMed PMID: 30855891]
Bourabaa S, Settaf A. Is identification and dissection of the external laryngeal nerve necessary during thyroidectomy? A prospective study. BMC surgery. 2024 Feb 4:24(1):46. doi: 10.1186/s12893-023-02287-x. Epub 2024 Feb 4 [PubMed PMID: 38311753]
Kelly E, Nazeer S, Fazzini B, Sutt AL, Olusanya S, Campion T, Puthucheary Z. Assessing the oral and suprahyoid muscles in healthy adults using muscle ultrasound to inform the swallowing process: a proof-of-concept study. Scientific reports. 2024 Jun 8:14(1):13198. doi: 10.1038/s41598-024-62032-z. Epub 2024 Jun 8 [PubMed PMID: 38851791]
Mazurek A, Wysiadecki G, Wójcik B, Dubrowski A, Skrzat J, Walocha J. Unusual anatomical variants of infrahyoid muscles - case report. Folia morphologica. 2024 Jul 5:():. doi: 10.5603/fm.100840. Epub 2024 Jul 5 [PubMed PMID: 38967006]
Level 3 (low-level) evidenceSingh JM, Wang R, Winters R, Kwartowitz G. Unilateral Vocal Fold Paralysis. StatPearls. 2024 Jan:(): [PubMed PMID: 30085602]
Noordzij JP, Ossoff RH. Anatomy and physiology of the larynx. Otolaryngologic clinics of North America. 2006 Feb:39(1):1-10 [PubMed PMID: 16469651]
Merati AL, Rieder AA. Normal endoscopic anatomy of the pharynx and larynx. The American journal of medicine. 2003 Aug 18:115 Suppl 3A():10S-14S [PubMed PMID: 12928069]
Mathews S, Jain S. Anatomy, Head and Neck, Cricoid Cartilage. StatPearls. 2024 Jan:(): [PubMed PMID: 30969643]
Hoh JF. Laryngeal muscle fibre types. Acta physiologica Scandinavica. 2005 Feb:183(2):133-49 [PubMed PMID: 15676055]
Level 3 (low-level) evidenceO'Rahilly R, Tucker JA. The early development of the larynx in staged human embryos. I. Embryos of the first five weeks (to stage 15). The Annals of otology, rhinology, and laryngology. 1973 Sep-Oct:82():1-27 [PubMed PMID: 4746614]
Uludag M, Aygun N, Kartal K, Besler E, Isgor A. Innervation of the human posterior cricoarytenoid muscle by the external branch of the superior laryngeal nerve. Head & neck. 2017 Nov:39(11):2200-2207. doi: 10.1002/hed.24896. Epub 2017 Aug 17 [PubMed PMID: 28815834]
Allen E, Minutello K, Murcek BW. Anatomy, Head and Neck, Larynx Recurrent Laryngeal Nerve. StatPearls. 2024 Jan:(): [PubMed PMID: 29261997]
Kikuta S, Jenkins S, Kusukawa J, Iwanaga J, Loukas M, Tubbs RS. Ansa cervicalis: a comprehensive review of its anatomy, variations, pathology, and surgical applications. Anatomy & cell biology. 2019 Sep:52(3):221-225. doi: 10.5115/acb.19.041. Epub 2019 Aug 26 [PubMed PMID: 31598349]
Brooks M, McLaughlin E, Shields N. Expiratory muscle strength training improves swallowing and respiratory outcomes in people with dysphagia: A systematic review. International journal of speech-language pathology. 2019 Feb:21(1):89-100. doi: 10.1080/17549507.2017.1387285. Epub 2017 Nov 1 [PubMed PMID: 29090601]
Level 1 (high-level) evidencePearson WG Jr, Langmore SE, Zumwalt AC. Evaluating the structural properties of suprahyoid muscles and their potential for moving the hyoid. Dysphagia. 2011 Dec:26(4):345-51. doi: 10.1007/s00455-010-9315-z. Epub 2010 Nov 11 [PubMed PMID: 21069388]
Pinheiro J, Cascallana JL, Lopez de Abajo B, Otero JL, Rodriguez-Calvo MS. Laryngeal anatomical variants and their impact on the diagnosis of mechanical asphyxias by neck pressure. Forensic science international. 2018 Sep:290():1-10. doi: 10.1016/j.forsciint.2018.06.019. Epub 2018 Jun 25 [PubMed PMID: 29979976]
Mu L, Chen J, Li J, Arnold M, Sobotka S, Nyirenda T, Fowkes M, Christopherson M, Sanders I. Sensory Innervation of the Human Soft Palate. Anatomical record (Hoboken, N.J. : 2007). 2018 Nov:301(11):1861-1870. doi: 10.1002/ar.23864. Epub 2018 Aug 6 [PubMed PMID: 30079585]
Kuo CT, Chiu CH, Fang TJ, Chao YK. Prognostic Factors for Recovery from Left Recurrent Laryngeal Nerve Palsy After Minimally Invasive McKeown Esophagectomy: A Retrospective Study. Annals of surgical oncology. 2024 Mar:31(3):1546-1552. doi: 10.1245/s10434-023-14560-7. Epub 2023 Nov 21 [PubMed PMID: 37989958]
Level 2 (mid-level) evidenceRosenthal LH, Benninger MS, Deeb RH. Vocal fold immobility: a longitudinal analysis of etiology over 20 years. The Laryngoscope. 2007 Oct:117(10):1864-70 [PubMed PMID: 17713451]
Level 2 (mid-level) evidencePatra A, Asghar A, Chaudhary P, Ravi KS. Identification of valid anatomical landmarks to locate and protect recurrent laryngeal nerve during thyroid surgery: a cadaveric study. Surgical and radiologic anatomy : SRA. 2023 Jan:45(1):73-80. doi: 10.1007/s00276-022-03054-y. Epub 2022 Dec 2 [PubMed PMID: 36459179]
Santos PM, Afrassiabi A, Weymuller EA Jr. Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1994 Oct:111(4):453-9 [PubMed PMID: 7936678]