Introduction
The sinoatrial node (SA) is the default pacemaker and is located subepicardially and is crescent in shape. The atrioventricular node (AV) is a subendocardial structure situated in the inferior-posterior right atrium. It sits within an anatomic region bordered posteriorly by the coronary sinus ostium, superiorly by the tendon of Todaro, and anteriorly by the septal tricuspid valve annulus. This anatomic region is also commonly referred to as the triangle of Koch. The sinoatrial nodal artery supplies blood to the sinoatrial node, it branches off the right coronary artery in 60% of cases, whereas in 40% of cases, it comes from the left circumflex coronary artery. The blood supply to the AV node is from the AV nodal branch of the right coronary artery (90%) or the left circumflex artery (10%) depending on the right or left dominant blood supply to the heart. The first septal perforator of the left anterior descending artery also supplies blood to the AV node. A junctional rhythm is where the heartbeat originates from the AV node or His bundle, which lies within the tissue at the junction of the atria and the ventricle (see Image. Junctional Rhythm). Generally, in sinus rhythm, a heartbeat is originated at the SA node. This electrical activity then travels through the atria to the AV node from where it reaches the Bundle of His from where the electrical signals travel to the ventricles through the Purkinje fibers.[1][2][3][4][5][6]
The terminology used to identify the type junctional rhythm depends on its rate and is as follows:
- Junctional bradycardia: rate below 40 beats per minute
- Junction escape rhythm: rate 40 to 60 beats per minute
- Accelerated junctional rhythm: rate of 60 to 100 beats per minute
- Junctional tachycardia: rate above 100 beats per minute
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
When the electrical activity of the SA node is blocked or is less than the automaticity of the AV node/His bundle, a junctional rhythm originates. Numerous conditions and medications can lead to a diseased SA node and lead to the AV node/His bundle taking over due to the higher automaticity of the ectopic pacemaker.[7][8][9]
Some of these conditions and medications are listed below.
- Chest trauma
- Sick sinus syndrome
- Radiation therapy
- Collagen vascular disease
- Myocarditis
- Clonidine
- Reserpine
- Adenosine
- Cimetidine
- Antiarrhythmics class I to IV
- Lithium
- Amitriptyline
- Neuromuscular disorder
- X-linked muscular dystrophy
- Familial disorder
- Vasovagal simulation (endotracheal suctioning)
- Carotid sinus hypersensitivity
- Beta-blockers
- Calcium channel blockers
- Digoxin
- Ivabradine
- Opioids
- Cannabinoids
- Isoproterenol infusion
- Hypothyroidism
- Sleep apnea
- Hypoxia
- Intracranial hypertension
- Hyperkalemia
- Anorexia nervosa
- Amyloidosis
- Pericarditis
- Lyme disease
- Rheumatic fever
- Ischemic heart disease
- Acute myocardial infarction
- Acute and chronic coronary artery disease
- Repair of congenital heart disease
- Inherited channelopathy
Other than the above-listed causes of severe SA node disease, which can result in junctional rhythm, a high-grade second-degree heart block and a third-degree heart block can also result in a junctional rhythm. Digoxin toxicity can also lead to an accelerated junctional rhythm.
Epidemiology
Junctional rhythm is typical among individuals who have a sinus node dysfunction (SND), and 1 in every 600 cardiac patients above the age of 65 within the United States has SND. Patients with sick sinus syndrome, young children, and athletes who have increased vagal tone may also intermittently exhibit junctional rhythm, especially during sleep. Junctional rhythm is reported equally among males and females.[10]
Pathophysiology
A heart has numerous pacemaker sites within its conduction system, which are independently able to keep the heart beating. And the rate of a heartbeat depends upon the pacemaker site, and as we go down its conduction system, the rate of spontaneous depolarization at pacemaker sites decreases. [1][2][3]
Pacemaker sites and their depolarization rates are listed below:
- Sinoatrial node: 60 to 100 beats per minute
- Atria: less than 60 beats per minute
- Atrioventricular node: 40 to 60 beats per minute
- Ventricles: 20 to 40 beats per minute
Histopathology
Histopathology of a disease SA node that can contribute to the AV node/His bundle taking over as a pacemaker secondary to their intrinsic automaticity includes SA node fibrosis, atrophy, hypoplasia, or amyloidosis. A normal SA node histopathology does not rule out reduced SA node automaticity contributing to a junctional rhythm.[11][12]
History and Physical
Patients with junctional rhythm may present with a varied array of symptoms or may be asymptomatic. Symptoms mostly depend on the underlying cause of the junctional rhythm, for instance, a patient presenting with heart failure exacerbation may present with shortness of breath, wheezing, and lower extremity edema. Patients with rheumatic fever may present with a heart murmur secondary to the damage to the heart valves, fever, joint pain, and a rash with an electrocardiogram showing a junctional rhythm. Some patients might present with generalized complaints such as dizziness, fatigue, syncope/presyncope, and intermittent palpitations. Non-specific physical exam findings include pulsating veins and regular heart rate with the heart rate varying from 20 to over 100 beats per minute.[13][14][15]
Evaluation
A significant component of an assessment for a patient who presents with signs and symptoms of junctional rhythm is history and physical exam. These should include vital signs (respiratory rate, blood pressure, temperature, and heart rate), a review of the patient's medication list, and an electrocardiogram. See the image below. During their evaluation, it should be established if the patient is hemodynamically stable. The patient should be assessed for any underlying ischemic heart disease or heart failure. A healthcare provider should consider thyroid function testing, pulmonary function testing, including routine blood work, and echocardiography as part of their initial evaluation.[13][14][15]
Treatment / Management
Treatment of a junctional rhythm primarily depends on the underlying cause of the rhythm. In circumstances where the junctional rhythm is a result of underlying sinus node dysfunction that is leading to asystole or bradycardia, it should not be terminated, for it is maintaining the heart rate. Therefore, before establishing a management plan for patients presenting with a junctional rhythm, an underlying etiology must be determined first. Otherwise, healthy individuals who have junctional rhythm and are asymptomatic need no medical management as the rhythm is usually a result of their increased vagal tone suppressing the SA node intrinsic automaticity. In the setting of digoxin toxicity, a patient must be treated with atropine and digoxin-specific antibody. If a patient is refractory to these pharmacologic treatments and goes into junctional tachycardia, intravenous phenytoin can be administered in a monitored setting as these patients can develop hypotension. In the pediatric population, persistent symptomatic junctional tachycardia is an indication for percutaneous radiofrequency ablation. In patients with sick sinus syndrome, or complete or high-grade AV block, a permanent pacemaker is indicated.[16][17][18][19][20](B2)
Differential Diagnosis
- Digoxin toxicity
- Atrioventricular nodal reentrant tachycardia
- Atrioventricular reentrant tachycardia
- Sinus node dysfunction
- High-grade second-degree heart block
- Third-degree heart block
Prognosis
Prognosis is good when the rhythm is promptly identified by a healthcare provider.
Complications
If not identified promptly symptomatic complications such as syncope, fatigue, or dizziness can occur.
Deterrence and Patient Education
If available patient education should be provided using resources familiar to the patient including online resources and pamphlets.
Pearls and Other Issues
Always check serum digoxin levels in patients who are on it for comorbidities. Also, check Lyme titers and empirically treat those patients who present with junctional rhythm and have possible exposure to ticks with antibiotics.
Enhancing Healthcare Team Outcomes
Educating patients at risk for this rhythm and making a closed-loop communication between them and their providers can help further improve the management of these rhythms. An interprofessional team best manages this condition. Initial diagnosis is by primary care or emergency providers. Referral to a cardiologist may be indicated. Cardiology and emergency department nurses administer treatment, monitor responses, and report back to the physician or nurse practitioner. Pharmacists should review prescribed medications, check for drug-drug interactions, and educate patients about dosing and side effects. [Level 5]
Media
(Click Image to Enlarge)
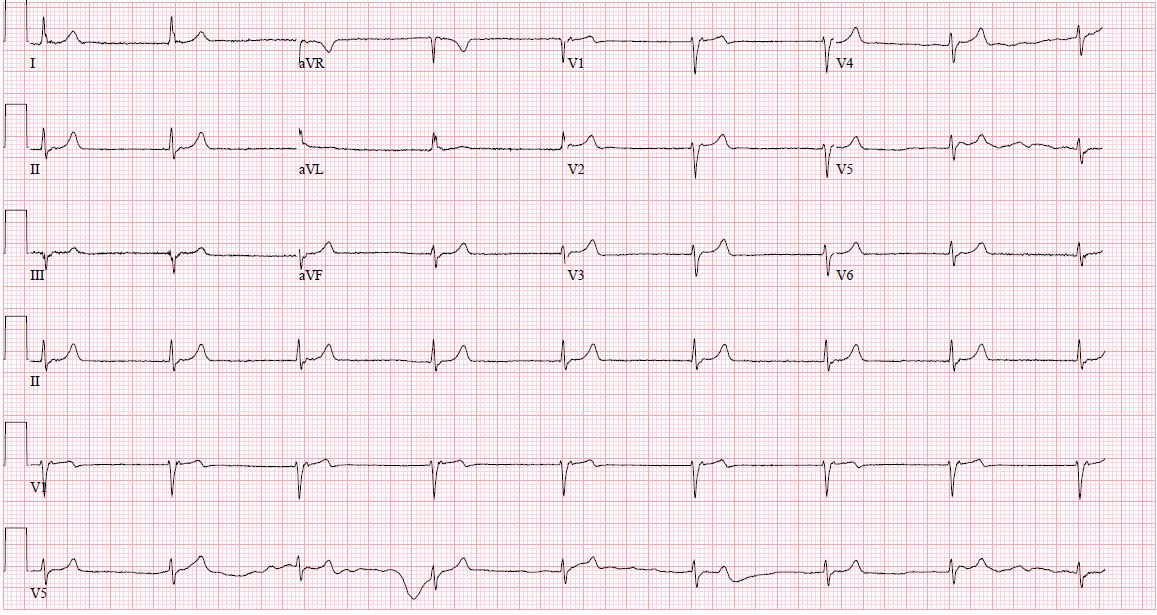
Junctional Rhythm
Contributed by D Desai, MD, MPH
References
Spodick DH. Normal sinus heart rate: sinus tachycardia and sinus bradycardia redefined. American heart journal. 1992 Oct:124(4):1119-21 [PubMed PMID: 1529897]
Thery C, Gosselin B, Lekieffre J, Warembourg H. Pathology of sinoatrial node. Correlations with electrocardiographic findings in 111 patients. American heart journal. 1977 Jun:93(6):735-40 [PubMed PMID: 871100]
Dobrzynski H, Anderson RH, Atkinson A, Borbas Z, D'Souza A, Fraser JF, Inada S, Logantha SJ, Monfredi O, Morris GM, Moorman AF, Nikolaidou T, Schneider H, Szuts V, Temple IP, Yanni J, Boyett MR. Structure, function and clinical relevance of the cardiac conduction system, including the atrioventricular ring and outflow tract tissues. Pharmacology & therapeutics. 2013 Aug:139(2):260-88. doi: 10.1016/j.pharmthera.2013.04.010. Epub 2013 Apr 20 [PubMed PMID: 23612425]
Level 3 (low-level) evidenceVan der Hauwaert LG, Stroobandt R, Verhaeghe L. Arterial blood supply of the atrioventricular node and main bundle. British heart journal. 1972 Oct:34(10):1045-51 [PubMed PMID: 5086972]
Pejković B, Krajnc I, Anderhuber F, Kosutić D. Anatomical aspects of the arterial blood supply to the sinoatrial and atrioventricular nodes of the human heart. The Journal of international medical research. 2008 Jul-Aug:36(4):691-8 [PubMed PMID: 18652764]
Chua K, Upadhyay GA, Lee E, Aziz Z, Beaser AD, Ozcan C, Broman M, Nayak HM, Tung R. High-resolution mapping of the triangle of Koch: Spatial heterogeneity of fast pathway atrionodal connections. Heart rhythm. 2018 Mar:15(3):421-429. doi: 10.1016/j.hrthm.2017.10.030. Epub 2017 Nov 26 [PubMed PMID: 29081398]
Semelka M, Gera J, Usman S. Sick sinus syndrome: a review. American family physician. 2013 May 15:87(10):691-6 [PubMed PMID: 23939447]
Trappe HJ. Tachyarrhythmias, bradyarrhythmias and acute coronary syndromes. Journal of emergencies, trauma, and shock. 2010 Apr:3(2):137-42. doi: 10.4103/0974-2700.62112. Epub [PubMed PMID: 20606790]
Silvestri NJ, Ismail H, Zimetbaum P, Raynor EM. Cardiac involvement in the muscular dystrophies. Muscle & nerve. 2018 May:57(5):707-715. doi: 10.1002/mus.26014. Epub 2017 Nov 28 [PubMed PMID: 29130502]
Romhilt DW, Doyle M, Sagar KB, Hastillo A, Wolfgang TC, Lower RR, Hess ML. Prevalence and significance of arrhythmias in long-term survivors of cardiac transplantation. Circulation. 1982 Aug:66(2 Pt 2):I219-22 [PubMed PMID: 6177443]
Rodriguez RD, Schocken DD. Update on sick sinus syndrome, a cardiac disorder of aging. Geriatrics. 1990 Jan:45(1):26-30, 33-6 [PubMed PMID: 2403955]
Sanders P, Kistler PM, Morton JB, Spence SJ, Kalman JM. Remodeling of sinus node function in patients with congestive heart failure: reduction in sinus node reserve. Circulation. 2004 Aug 24:110(8):897-903 [PubMed PMID: 15302799]
Kim D, Shinohara T, Joung B, Maruyama M, Choi EK, On YK, Han S, Fishbein MC, Lin SF, Chen PS. Calcium dynamics and the mechanisms of atrioventricular junctional rhythm. Journal of the American College of Cardiology. 2010 Aug 31:56(10):805-12. doi: 10.1016/j.jacc.2010.03.070. Epub [PubMed PMID: 20797495]
Level 3 (low-level) evidenceCools E, Missant C. Junctional ectopic tachycardia after congenital heart surgery. Acta anaesthesiologica Belgica. 2014:65(1):1-8 [PubMed PMID: 24988822]
Di Biase L, Gianni C, Bagliani G, Padeletti L. Arrhythmias Involving the Atrioventricular Junction. Cardiac electrophysiology clinics. 2017 Sep:9(3):435-452. doi: 10.1016/j.ccep.2017.05.004. Epub [PubMed PMID: 28838549]
Tuohy S, Saliba W, Pai M, Tchou P. Catheter ablation as a treatment of atrioventricular block. Heart rhythm. 2018 Jan:15(1):90-96. doi: 10.1016/j.hrthm.2017.08.015. Epub 2017 Aug 18 [PubMed PMID: 28823599]
Antman EM, Wenger TL, Butler VP Jr, Haber E, Smith TW. Treatment of 150 cases of life-threatening digitalis intoxication with digoxin-specific Fab antibody fragments. Final report of a multicenter study. Circulation. 1990 Jun:81(6):1744-52 [PubMed PMID: 2188752]
Level 2 (mid-level) evidenceHauptman PJ, Kelly RA. Digitalis. Circulation. 1999 Mar 9:99(9):1265-70 [PubMed PMID: 10069797]
Kelly RA, Smith TW. Recognition and management of digitalis toxicity. The American journal of cardiology. 1992 Jun 4:69(18):108G-118G; disc. 118G-119G [PubMed PMID: 1626485]
Dobrzynski H, Boyett MR, Anderson RH. New insights into pacemaker activity: promoting understanding of sick sinus syndrome. Circulation. 2007 Apr 10:115(14):1921-32 [PubMed PMID: 17420362]
Level 3 (low-level) evidence