Introduction
The ileocolic artery is the most inferior branch of the superior mesenteric artery (SMA), supplying blood to the distal ileum, ileocecal valve, cecum, vermiform appendix, and the proximal ascending colon (see Image. Conventional Angiogram of the Superior Mesenteric Artery). The ileocolic artery and its branches are of major surgical and clinical significance for the following reasons:
- Ligation and complete hemostasis of the ileocolic artery or its branches must occur during appendectomy or Meckel diverticulectomy.
- Ischemia with possible necrosis of the viscus organs supplied by the ileocolic artery may occur in the setting of intussusception.
- Ischemia in the ileocolic distribution may occur with SMA thromboembolism.
- Special attention must be paid in the setting of colon cancer resection to sites of vessel anastomoses, including the right colic to ileocolic arteries, for purposes of hemostasis.
- Lymphatic drainage mirrors vascular supply; understanding anatomy and anatomic variation is essential for successful oncologic surgery.
- Understanding the vascular anatomy of the gastrointestinal tract is essential for diagnosing and treating gastrointestinal bleeds. See Illustration. Ileocolic Artery, Intestine.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The major branches of the SMA are the inferior pancreaticoduodenal, right colic, middle colic, and ileocolic. Additionally, multiple branches supplying the jejunum and ileum arise from the left aspect of the SMA. The middle colic artery is the first of the colic branches of the SMA, providing blood supply to the proximal two-thirds of the transverse colon. The right colic artery is the second branch supplying the right colon, primarily the ascending colon. The ileocolic artery is the SMA's most inferior branch (often called the terminal branch). The ileocolic artery courses inferiorly and retroperitoneally after arising from the SMA, traversing towards the right iliac fossa. The ileocolic artery divides into the inferior and superior branches at this location. The superior branch of the ileocolic artery anastomoses with the right colic artery. It supplies the terminal ileum, cecum, and appendix. The inferior branch gives rise to the anterior and posterior cecal arteries, the ileal branch of the ileocolic artery, and the appendicular artery. The anterior and posterior cecal arteries are found anterior and posterior to the terminal ileum. The ileal branch of the ileocolic artery forms an anastomosis with the last intestinal (ileal) artery. Additionally, the ileocolic artery anastomoses with the right colic artery superiorly. Finally, the appendicular artery is suspended in the mesoappendix and found posterior to the terminal ileum.
It should be noted that there are normal anatomic variations of the right colonic vasculature and branches of the SMA, the most common being separate origins of the right, middle, and ileocolic arteries as described above. The other 2 most common variations include a common origin of the middle and right colic arteries with a separate origin of the ileocolic and a common origin of the right colic and ileocolic arteries with a separate origin of the middle colic. Additionally, it is important to note that the arteries of the mid and hindgut form an anastomosis, the marginal artery of Drummond. The artery of Drummond is an anastomosis between the terminal branches of the superior and inferior mesenteric arteries running along the inner margin of the colon within the mesentery. It gives off small branches to the colon called vasa recta.[1][2][3][4][5][6]][7]
The ileocolic artery and its branches supply blood to the distal ileum, ileocecal valve, cecum, vermiform appendix, and the proximal ascending colon.
Key Relations
- The ileocolic artery is found anterior to the right gonadal vessels and ureter.
- The posterior cecal artery is found posterior to the terminal ileum/cecum.
- The anterior cecal artery is found anterior to the terminal ileum/cecum.
- The appendicular artery is found posterior to the terminal ileum.
- The ileocolic artery forms an anastomosis with the right colic artery.
- Terminal branches of both the superior and inferior mesenteric arteries form an anastomosis via the marginal artery of Drummond.
Embryology
The ileocolic artery is of midgut origin as it is the most inferior branch of the SMA, and it supplies midgut organs. Consistent with most vasculature, the ileocolic artery is of mesoderm origin.[8]
Blood Supply and Lymphatics
The blood supply to the ileocolic artery is the SMA. The SMA is the second major branch of the abdominal aorta, just distal to the celiac trunk. The celiac trunk is the vascular supply to the stomach, proximal small bowel, liver, spleen, and pancreas. The inferior mesenteric artery is a branch of the abdominal aorta serving as the vascular supply to the hindgut. The lymphatics associated with the ileocolic artery are the lymph nodes located within the mesentery of the viscus organs: the mesoileum, the mesocecum, the mesoappendix, and the mesocolon.[2]
Nerves
The ileocolic artery supplies the portion of the myenteric plexus that coincides with the viscus organ distribution of the artery. Thus, it spans the myenteric plexus embedded from the distal ileum to the proximal ascending colon.[9]
Muscles
The muscles supplied by the ileocolic artery are within the bowel walls. For peristalsis to occur, the muscular layer, consisting of the inner transverse layer and outer longitudinal layer, must receive its blood supply. In addition to providing blood to the muscles in the bowel wall, the ileocolic artery supplies the intrinsic anatomic sphincter muscle comprising the ileocecal valve. Finally, the ileocolic artery supplies the proximal portion of the taeniae coli. Beginning from where they coalesced at the vermiform appendix up through the proximal portion of the ascending colon where the anastomosis with the right colic artery occurs.[8][10]
Physiologic Variants
The ileocolic artery is present in more than 95% of people. In roughly 50% of patients, the ileocolic artery travels anterior and superior to the superior mesenteric vein. The most common variations of the right colon vasculature include the common origin of the right and middle colic arteries, with separate vascular of the ileocolic, and the common origin of the right colic and ileocolic, with a distinct origin of the middle colic. An additional anatomic variation includes the absence of the right colic artery.[4][5]
Surgical Considerations
The appendicular artery runs in the mesoappendix of the vermiform appendix. The artery runs very close to the free margin of the mesoappendix and terminates in multiple small branches that supply the appendix. When an appendectomy is performed, the inferior branch of the ileocolic artery must be ligated at the base of the appendix. Otherwise, postoperative bleeding can occur. Complete hemostasis must be obtained, and the mesoappendix must be checked for the absence of bleeding before the patient is closed. Similarly, during Meckel diverticulectomies, care must be taken to ligate branches of the ileocolic artery to ensure hemostasis.[1][2]
Clinical Significance
The ileocolic artery is of major clinical significance for the following reasons:
Ileocecal Intussusception: Occlusion of the ileocolic artery can occur as the terminal ileum enters the cecum. As 1 layer of the bowel telescopes within the other, the blood supply can become compressed. This compression can be significant enough to occlude the artery, leading to ischemia in the distribution of the ileocolic artery. The extent of ischemic bowel associated with intussusception depends on where the artery gets compressed, eg, proximally, distally, or 1 of the named branches. Anywhere from a small portion of the bowel to the entire distribution of the ileocolic artery can become ischemic. With continued intussusception, whether repetitively occurring or occurring for long durations of time, ischemia can lead to necrosis and, ultimately, perforation, both of which can result in an acute abdomen/surgical emergency. Intussusception most commonly occurs in young children, generally 2 to 3 years of age. The patients may present with a combination of intermittent abdominal pain, vomiting, a right upper quadrant mass, and bloody stools. A lead point is rarely identified in young children while commonly present in older children and adults. Potential lead points include both benign and malignant neoplasms. Drummond can be performed with water-soluble contrast or air enema in most cases of young children without complications or surgery. However, a surgeon should be on standby in case of perforation. Reports exist of recurrence rates as high as 30%.[11][12][13][14]
Ischemia status post SMA thromboembolism: Occlusion of the SMA can lead to ischemia in the distribution of the SMA in its entirety. Additionally, smaller thromboembolic may lodge in a more distal branch of the SMA, including the inferior terminal branch, the ileocolic artery. Similarly to intussusception, depending on the exact location of the occlusion, the extent of ischemia or necrosis can vary.[15][16]
Surgery: A thorough understanding of the vascular anatomy and anatomic variations of the right colon is essential for successful surgical intervention to include but not limited to jejunum treatment of appendicitis, Meckel diverticulitis, inflammatory bowel disease, colon cancer, and symptomatic benign neoplasms of the bowel or mesentery. Knowledge of anatomy is important to ensure proper hemostasis and healing of bowel anastomosis. The areas of surgical anastomosis in the colon are at higher risk for ischemia in tumor/bowel resection surgery. Anastomosis is critical, ensuring adequate blood supply to the colon, especially in elderly or diabetic patients. Adequate blood supply ensures the normal healing of colic anastomosis.[1]
Trauma: There are rare reports of isolated rupture of the ileocolic artery in the setting of blunt abdominal trauma.[17]
Other Issues
Finally, there is a possibility of using colic vessels to include the ileocolic artery and the status of post-cancer resection as a marker of the quantity of resection. Arterial stumps seen on routine portal venous computed tomography have shown potential as in vivo markers of surgical quality and extent of mesenteric resection.[18]
Media
(Click Image to Enlarge)
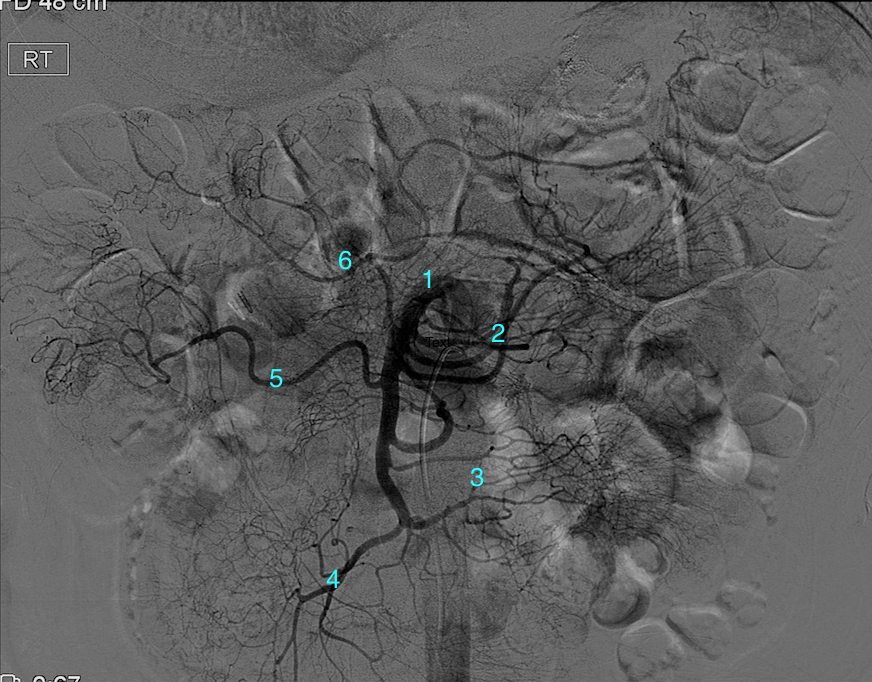
Conventional Angiogram of the Superior Mesenteric Artery. (1) proximal SMA (2) jejunal branches (3) ileal branches (4) ileocolic artery (5) right colic artery and (6) middle colic artery.
Contributed by DW Byerly, MD, PhD
(Click Image to Enlarge)
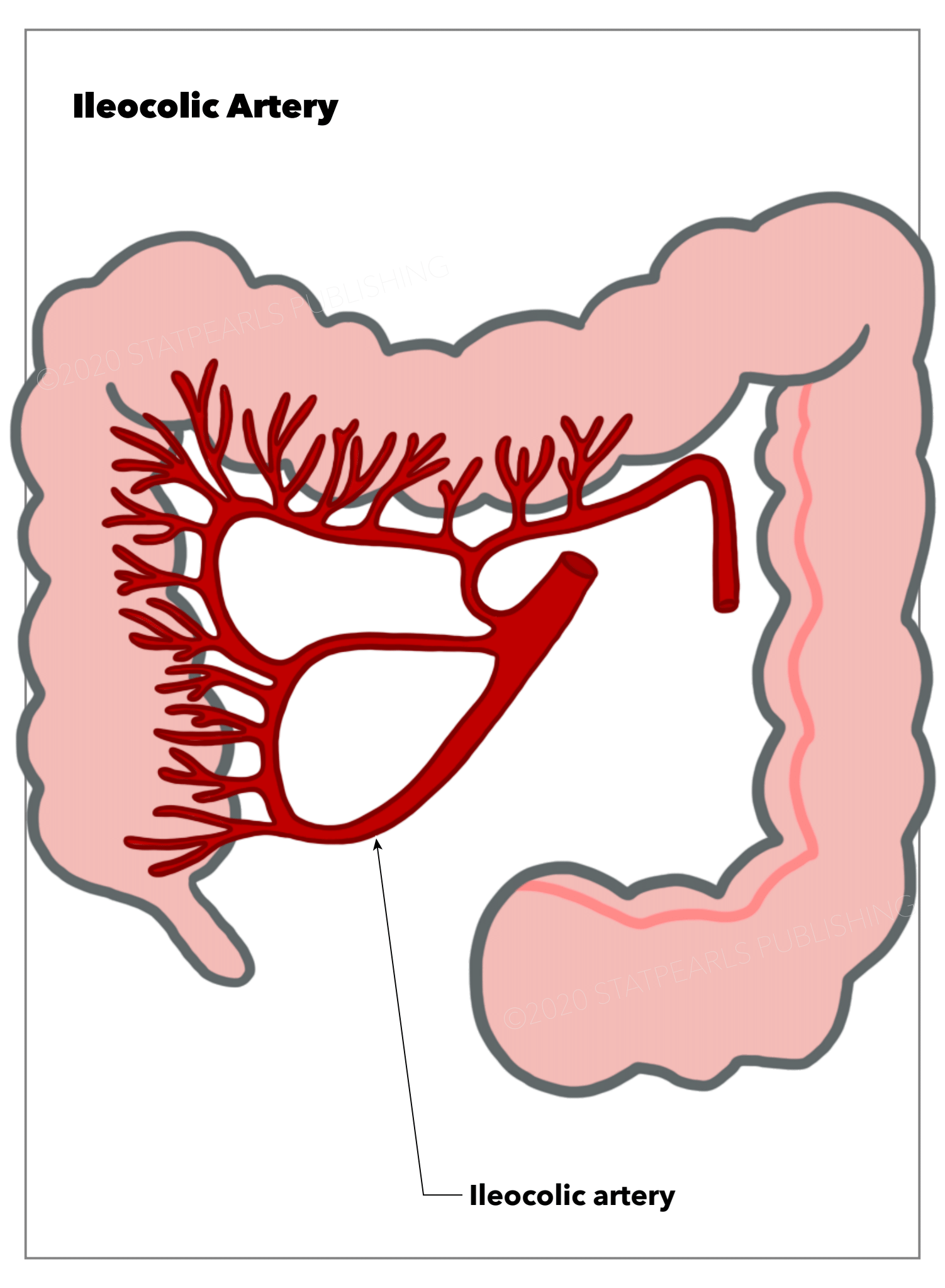
Ileocolic Artery, Intestine
Illustration by E Gregory
References
Pan K. [Measures to anatomic variations of the colonic vessels in laparoscopic operations]. Zhonghua wei chang wai ke za zhi = Chinese journal of gastrointestinal surgery. 2013 Oct:16(10):944-6 [PubMed PMID: 24158864]
Sun HL, Wang W, Yao L, Chen SX, Ren A, Hu YY, Xu YY. [Preoperative evaluation of mesenteric vascular anatomy using 256 multi-slice computed tomography before laparoscopic surgery]. Zhonghua wei chang wai ke za zhi = Chinese journal of gastrointestinal surgery. 2011 Nov:14(11):855-8 [PubMed PMID: 22116719]
Charnsangavej C, DuBrow RA, Varma DG, Herron DH, Robinson TJ, Whitley NO. CT of the mesocolon. Part 1. Anatomic considerations. Radiographics : a review publication of the Radiological Society of North America, Inc. 1993 Sep:13(5):1035-45 [PubMed PMID: 8210588]
Haywood M,Molyneux C,Mahadevan V,Srinivasaiah N, Right colic artery anatomy: a systematic review of cadaveric studies. Techniques in coloproctology. 2017 Dec; [PubMed PMID: 29196959]
Level 1 (high-level) evidenceGamo E, Jiménez C, Pallares E, Simón C, Valderrama F, Sañudo JR, Arrazola J. The superior mesenteric artery and the variations of the colic patterns. A new anatomical and radiological classification of the colic arteries. Surgical and radiologic anatomy : SRA. 2016 Jul:38(5):519-27. doi: 10.1007/s00276-015-1608-3. Epub 2016 Jan 4 [PubMed PMID: 26728989]
Kuzu MA, İsmail E, Çelik S, Şahin MF, Güner MA, Hohenberger W, Açar Hİ. Variations in the Vascular Anatomy of the Right Colon and Implications for Right-Sided Colon Surgery. Diseases of the colon and rectum. 2017 Mar:60(3):290-298. doi: 10.1097/DCR.0000000000000777. Epub [PubMed PMID: 28177991]
Mike M, Kano N. Reappraisal of the vascular anatomy of the colon and consequences for the definition of surgical resection. Digestive surgery. 2013:30(4-6):383-92. doi: 10.1159/000343156. Epub 2013 Oct 10 [PubMed PMID: 24135859]
Bhatia A, Shatanof RA, Bordoni B. Embryology, Gastrointestinal. StatPearls. 2024 Jan:(): [PubMed PMID: 30725857]
Timmermans JP, Hens J, Adriaensen D. Outer submucous plexus: an intrinsic nerve network involved in both secretory and motility processes in the intestine of large mammals and humans. The Anatomical record. 2001 Jan 1:262(1):71-8 [PubMed PMID: 11146430]
Level 3 (low-level) evidencePollard MF, Thompson-Fawcett MW, Stringer MD. The human ileocaecal junction: anatomical evidence of a sphincter. Surgical and radiologic anatomy : SRA. 2012 Jan:34(1):21-9. doi: 10.1007/s00276-011-0865-z. Epub 2011 Aug 24 [PubMed PMID: 21863224]
Liu X, Yu HK, Gu LX, Chen JK, Wen ZB. Atropine Premedication Facilitates Ultrasound-Guided Reduction by Saline Enema in Children With Intussusception. Frontiers in pharmacology. 2019:10():43. doi: 10.3389/fphar.2019.00043. Epub 2019 Jan 31 [PubMed PMID: 30766486]
Gollub MJ. Colonic intussusception: clinical and radiographic features. AJR. American journal of roentgenology. 2011 May:196(5):W580-5. doi: 10.2214/AJR.10.5112. Epub [PubMed PMID: 21512048]
Level 2 (mid-level) evidenceApplegate KE. Clinically suspected intussusception in children: evidence-based review and self-assessment module. AJR. American journal of roentgenology. 2005 Sep:185(3 Suppl):S175-83 [PubMed PMID: 16120899]
Level 3 (low-level) evidenceKlein EJ, Kapoor D, Shugerman RP. The diagnosis of intussusception. Clinical pediatrics. 2004 May:43(4):343-7 [PubMed PMID: 15118777]
Level 2 (mid-level) evidenceKamiya C, Deguchi J, Kitaoka T, Suzuki J, Abe K, Sato O. Obstruction of the superior mesenteric artery due to emboli from the thoracic aorta in a patient with thromboangiitis obliterans. Annals of vascular diseases. 2014:7(3):320-4. doi: 10.3400/avd.cr.14-00035. Epub 2014 Jul 30 [PubMed PMID: 25298837]
Level 3 (low-level) evidenceSakai A, Hara H, Nakamura M. Successful endovascular treatment for simultaneous multiple thromboemboli following myocardial infarction. The Journal of invasive cardiology. 2013 Jun:25(6):E133-5 [PubMed PMID: 23735368]
Level 3 (low-level) evidenceBastuev NV, Bekenov BM, Ivankov VT. [Isolated rupture of the ileocolic artery in blunt trauma to the abdomen]. Sudebno-meditsinskaia ekspertiza. 1976 Oct-Dec:19(4):47 [PubMed PMID: 1014059]
Level 3 (low-level) evidenceKaye TL, West NP, Jayne DG, Tolan DJ. CT assessment of right colonic arterial anatomy pre and post cancer resection - a potential marker for quality and extent of surgery? Acta radiologica (Stockholm, Sweden : 1987). 2016 Apr:57(4):394-400. doi: 10.1177/0284185115583033. Epub 2015 May 4 [PubMed PMID: 25940063]
Level 2 (mid-level) evidence