Introduction
Hydrofluoric acid was discovered in 1771 by Swedish pharmaceutical chemist Carl Wilhelm Scheele when he was investigating the mineral called fluorite (Calcium fluoride). Hydrogen fluoride (HF) has several synonyms: Hydrofluoric acid, Fluoric acid, Hydrofluoride, Fluorine monohydride, Fluorane. Hydrofluoric (HF) acid is an extremely powerful inorganic acid and a vigorous dehydrating agent that is used in many industrial branches including production of aluminum, stainless steel and hydrofluorocarbons, glass etching, stevedoring and transportation industries, inorganic and organic chemical manufacturing, mineral processing, petroleum oil refineries, fire extinguishers manufacturing, steel mills, cleaning HVAC systems, and as the precursor to all fluorine compands in the pharmaceutical industry. [1][2][3][4] Consumer products containing hydrofluoric acid include rust removers, detergents, marble, brick and stone cleaning, toilet bowl clearners, insecticides, automobile wheel cleaners and air conditioner cleaners. [4][5]
Hydrofluoric acid is comprised of a diatomic compound of hydrogen and fluoride atoms as a gas, while in the liquid state it has strong hydrogen bonds between the chains forming a polymeric compound. [6] Anhydrous hydrofluoric acid and hydrofluoric acid in aqueous solutions range in appearance from colorless to slightly tinted based upon the concentration and impurities. It has a boiling point of 20 degrees celcius (68 degrees fahrenheit) at 760 mmHg, vapour density greater than air and readily dissolves in water that when diluted (exothermal reaction) is visibly indistinguishable from water. Hydrofluoric acid has a disagreeable, pungent odor at concentrations of 0.04 ppm which is way below the OSHA PEL (Permissible Exposure Limit) of 3 ppm and is extremely corrosive and has the ability to dissovle a number of materials especially oxides. [4]
The Major source of production of hydrofluoric acid is by treating fluorite with concentrated sulfuric acid at temperatues of 265 degrees fahrenheit to produce hydrofluic acid and calcium sulfate. Alternate production is a by-product in the production of phosphoric acid from the mineral apatite. Hydrofluoric acid is also produced by the release from industrial and welding processes and environmental activities such as volcanoes. HF production exceeds one million tons world wide by a number of manufactors and is transported and stored under high pressure as a highly concentrated liquid. [7] In the United States of America, the Department of Transportation Hazard Label and National Fire Protection Assocation (NFPA) 704 lists the health value of 4 (can be lethal), flammability value of 0 (will not burn under typical fire conditions), instability value of 2 (readily undergoes violent chamical changes at elevated temperatures and pressures) and special value of W with line through (reacts violently or exposevely with water). Domestic concentrations of hydrofluoric acid is typically around 0.5% with industrial concentrations approaching 100%.
Primary health consequences including dermal burns, eye injury, acute respiratory symptoms, gastrointestinal symptoms and cardiac abnormalities can occur from direct skin / eye contact, ingestion of solutions or inhalation of fumes and vapors with unintentional and intentional exposures. Unintentional exposure of hydrofluoric acid in and out of the workplace include inappropriate operations, mechanical failure of equipment, explosions of containers and tanks containing HF, during traffic incidents with leakage of HF, inadequate protective equipment and children accidentally exposed through ingestion of domestic cleaners. [4][8][9][10] Intentional cases of ingestion, with suicidal and homicidal intent, of hydrofluoric acid have been documented.[4][11]
Hydrofluoric acid is highly toxic and damaging to humans due to the “double danger” properties of the corrisive nature of the hydrogen ions and toxic effect due to the ability of fluoride ions to penetrate into deep tissue causing liquefactive necrosis and release of cellular products. Hydrofluoric acid burns present with a unique concern for systemic fluoride toxicity including cardiovascular, pulmonary, renal and neuromuscular symptoms, electrolyte imbalance and enzyme inhibition which can lead to cardiac arrhythmias and death. [12] Chronic symptoms may occur or persist for months after HF ingestion or respiratory exposure. [3][9]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Hydrofluoric acid exposure requires immediate specific and specialized medical treatment to prevent penetration of the hydrofluoric acid into the deep tissues, decrease the dissemination of the fluoride ions through the bloodstream and subsequently reduce the toxic effects on organs or minimize the progression of damage to organ systems. [4] Hydrofluoric acid is technically classified as a weak acid compared to other hydrogen halide acids, but the fluoride ion can be quickly absorbed through the skin causing potential life-threatening burns and cardiac arrhythmias. With the dilute solutions, there will have delayed injury because ions will penetrate through the skin before dissociating and causing complications. A dermal injury is reported as the most common observed injury with burns to the fingers being one of the most concerning injuries for workers. [13]
Epidemiology
Hydrofluoric acid exposure is a rare occurrence throughout the globe compared to other industrial injuries with an estimated 1000 cases annually, though actual incident rates are not known. 15 year study from Stuke et al showed an incident rate of 35 patients (17%) out of 204 chemical burns. [2] A 10-year study in China reported 690 patients with chemical burns and a little over half being involved with hydrofluoric acid and sulfuric acid. Most of the chemical burns occurred in the summer and autumn seasons. [14] A 20-year survey from Taiwan only had 324 identified calls of hydrofluoric acid with the majority of those incidents being dermal in nature. [1] Because of the nature of the occupations with the greatest potential injury from and exposure to hydrofluoric acid exposure, the majority of patients are adult males. Upper extremity location was most commonly involved. [2]
Pathophysiology
There are three (3) routes of entry for hydrofluoric acid into the human body - skin / eye exposure, inhalation and ingestion. Cutaneous exposure, with skin intact or damaged, is the most frequent pathway for entry with regards to aqueous solutions. Inhalation can arise from the exposure of the hydrogen fluoride gas as well as from the vapors eminating from the hydrogen fluoride liquid. [4]
Hydrofluoric acid is highly lipophilic acid and readily penetrates through the skin into the deeper tissues. [4][12] It has three separate mechanisms of injury:
- At high concentrations (> 50%), the hydrofluoric acid acts as a strong acid which causes corrosive burns with immediate contact to the skin, eyes, respiratory and gastrointestional mucous membrane. The resulting corrosive burns occur immediately with visible tissue destruction, areas of ulceration and necrosis followed by intense pain from activiation of underlying pain receptors
- With lower contractions of hydrofluoric acid, the small fluoride ion is able to penetrate the dermal layer. The fluoride ion differs from other forms of acid that releases hydrogen cations causing coagulative necorsis in that the fluoride ion continues dissolves through the skin causing further tissue destruction of nerves, blood vessles, underlying soft tissue via liquefaction necrosis and cellular death [4][12]
- Fluoride ion absorption into the bloodstream when in the presence of other cations (specifically calcium and magnesium) forms insoluble chelate salt via hydrofluoric fixation. The binding of the fluoride ion to the calcium and magnesium will produce hypocalcemia and hypomagnesemia as well as the destruction of the underlying tissue. The depletion of calcium causes inhibition of the Sodium-Potassium ATPase Pump resulting cellular membrane permeability of potassium leading to hyperkalemia. The electrolyte imbalance will lead to cardiac arrhythmias including prolonged QTc (from hypocalcemia), polymorphic ventricular tachycardia (from hypomagnesemia) and T wave elevation and QRS widening (from hyperkalemia) [4][12]
History and Physical
Depending on the location of the hydrofluoric acid exposure and the percentage of the acid, patients can present immediately with severe caustic burns to the body and severe pain, with pain out of proportion as the hallmark finding. Solutions greater than 14.5% will produce immediate symptoms, 12% solutions can take up to an hour, and solutions less than 7% can take hours before symptoms occur. The concern exists for ocular and respiratory injury when any chemical is splashed / sprayed in the face.
History should include any exposure to hydrofluoric acid through workplace or domestic type exposures to include potential products containing hydrofluoric acid such as rust removers or cleaning agents within the past 24 hours. One should ascertain the concentration of the solution, exposure time of HF, use of protective agents or any other chemicalsthat was contained in the solution. Additional information inclucdes any treatment that has been given thus far to the individual.
Physical assessment should include immediate evaluation for life-threatening emergencies including airway compromise, respiratory distress, and cardiac arrhythmias. Additionally, one can assess for pulmonary edema, ocular injuries, and symptoms of hypocalcemia including Chvostek and Trousseau signs and tetany.
- Chemical burns should be assessed based upon the route of exposure but should include:
- Dermal exposure: Location of the burn with the most common sites of injury are the head and neck, hands, legs and arms, color of the skin surrounding the burn, degree of ulceration and necrosis along with underlying structures such as tendon or bone involvement. [15][16] Exposure to 70% HF for only 20 seconds can cause cellular alteration in four to five epidermal layers within one minute and have complete penetration to the dermis within five minutes. Necrosis of all skin layers have been detected after one hour of exposure with complete necrosis of the epidermal skin layer and underlying structures after 24 hours. [4][17][4]
- Ocular exposure: Signs of irritation with pain are the initial first signs followed by conjunctivitis with edema and congestion. Subsequent corneal erosion with sloughing and ulceration of the corneal epithelium can occur leadering to corneal opacification in minor splashes with hydrofluoric acid. [7] Low concentrations of hydrofluoric acid (2.5%) can have complete diffusion into the cornea with ocular burns being detected with 4 minutes. [7][4] Prolonged exposure can lead to total eye destruction and loss of vision. Occular evaluation involves the simple and widely utilized Roper-Hall's classification of ocular chemical burns.
- Inhalation exposure: Toxic gases or vapors will cause nasal irritation with inflammation of the mucosa, mucosal bleeding, ulceration and/or perforation of the nasal septum. Additional respiratory symptoms based upon the concentration of the hydrofluoric acid and chronicity of exposure can include coughing, dyspnea, upper airway symptoms of laryngitis, laryngospasms, tracheobronchitis as evident with stridor or lower airway symptoms including wheezing, bronchiolar obstruction, bleeding of the airway, pulmonary edema and congestion or pneumothorax. Chronic dyspnea has been reported in patients with chronic, repeated exposure to fumes or gases containing hydrofluoric acid. [4]
- Ingestion exposure: Caustic type burns of the mucosa of the oropharynx, esophagus and stomach are evident with ingestion of solutions containing hydrofluoric acid. Individuals will complain of dysphagia, nausea, vomiting, diarrhea and severe abdominal pain. Hydrofluoric acid ingestions can lead to erosive gastritis leading to hematemesis and melana from the hemorrhagic gastritis or more importantly potential perforation of the stomach. [4]
- Neuromuscular symptoms: Individualizes exposed through all routes can develop neurologic and muscular disorders from the hypocalcemia and hyperkalemia causing interference with normal electrical signal transmission in neurons. These symptoms can include anxiousness, confusion, headaches, paresthesia, seizures or paralysis, carpopedal and generalized tetany, and coma secondary to cerebral edema. [4]
Evaluation
Electrolyte imbalance is one of the hallmark concerns for systemic poisoning from hydrofluoric acid exposure through all routes of entry. Immediate electrolyte assessment at minimum includes calcium, potassium, and magnesium levels to ascertain hypocalcemia, hypomagnesia and hyperkalemia. Even though the concern is with systemic poisoning, patients with simple exposures can develop hypocalcemia, hypomagnesia, and hyperkalemia.
Cardiac monitoring and electrocardiography (EKG / ECG) are important to assess for clinically significant electrolyte imbalance to include QT prolongation from hypocalcemia (Figure 1), peaked T waves/arrhythmias from hyperkalemia, and polymorphic ventricular tachycardia (specifically Torsades de Pointes) from hypomagnesia.
Chest x-rays should be performed on all patients with respiratory exposure to evaluate for pulmonary edema or pneumonitis. Inclusion of EtCO2 monitoring can be considered for individuals with inhalation type exposures. Urinalysis with evaluation for hematuria and proteinuria will indicate renal dysfunction, insufficiency and renal cortical necrosis.
Treatment / Management
Primary concern with the high corrosiveness and toxicity of hydrofluoric acid should be through the prevention of exposure. All individuals that use HF should be aware of the toxic properties of the agent which include information and procedures for safe handling of the acid, appropirate means of transporting and storage, management of waste containing HF, gross and fine decontaminiation procedures and medical treatment for exposure and intoxication. Hydrofluoric acid should be exclusively used in industrial settings and laboratories that are appropriately equipped to handle the chemical, have appropriate exposure control plans in place which includes having appropriate treatment modalities on site to initiate therapy prior to transport of the exposed individual to the hospital. Likewise, household and cleaning agents should be stored out of the reach of children.
Personal and general protectice equipment and measures should be implemented and adhered to at all times with equipment including:
- Perosnal protective equipment
- Laboratory coat
- Long pants
- Acid resistant apron
- Closed-toed shoes
- Full-face shiled in conjunction with tightly sealed goggles
- Rubber gloves made from nitrile, butyl or neoprene
- Respiratory filter device
- General protective equipment
- Handled inside of a fume hood
- Ventilation / exhaust system
- Sign "Danger, Hydrofluoric Acid Used in this Area"
- Easy access to a good supply of running water
- Safety shower and eyewash
- Standard Operating Procedure (SOP) document
- HFA Containers
- Polyethylene or Teflon
- Clearly labelled
- Securely supported and not likely to tip over
- Tightly cosed and kept in a safe place
- Away from heat and direct sunlight
- First aid kit / medication
- 2.5% calcium gluconate gel
- 1% calcium gluconate eyewash solution of 0.13% benzalkonium choloride (Zephiran Chloride)
Initial treatment for HF acid includes quick assessment, removal of contaminated clothing, as well as jewellery that could trap HF, should be immediately removed and double-bagged to prevent secondary exposure. Decontamination with copious amounts of water, saline or solution of soap and water along with neutralization using calcium gluconate, benzalkonium chloride polyethelene glycol, magnesium oxide or Hexafluorine. [4] Assessment and management life-threating conditions such as airway compromise or cardiac arrythmias.
The decontaminzation and neutralzing process for hydrofluoric acid exposure is primarily through the mechanical rinsing and diluting effect of water, as a hypotonic solution. Likewise it has no active ability to bind or chelate any chemical substance with the concerning hydrofluoric acid exposure and thefore neutralizing agents with their mechanism of actions can help reduce the necrosis from the fluoride ion. Calcium gluconate is the primary neutralizing agent and is capable of chelating the free fluoride ions, forming insoluble salts. Calcium gluconate should be applied multiple times to mitigate the damage from the fluoride ions. [4]
Hexafluorine solution developed by PREVOR laboratories was designed for active washing of hydrofluoric acid splashes. The solution has a triple effect in that it has the same rinsing and diluting properties as water, can neutralize the hydrogen ions and chelate the fluoride ions thus reducing the corrosive and cytotoxic effects of hydrofluoric acid. Though in an experimental study by Hulten et al, there was little difference in reducing the electrolyte disturbances caused from dermal exposure of hydrofluoric acid when compared to water rinsing. [4] [18](B3)
Treatment modalities
- Dermal exposure (initially or at the hospital)
- Most commonly used decontaminating procedure is rinsing with cold or warm running water or saline for at least 30 minutes. Decontamination procedures using a soft brush, moving in a downward motion (from head to toe) with household dish soaps (Dawn, Palmolive) and water, with a pH value of at least 8 and should not exceed a pH value of 10.5, will help neutralize hydrofluoric acid with a low pH. Rinsing should be thoroughly performed until the contaminant is removed.
- Primary neutralizing process for HF with with use of calcium gluconate soaking, intravenous calcium gluconate (10%), and topical use of calcium gluconate gel (2.5%).
- When used as a gel, 2.5 % calcium gluconate should be applied and rubbed into the affected area for 15 - 30 minutes and should be reapplied every 10 - 15 minutes. The Calcium gluconate gel will turn white as the calcium binds to the fluoride ions creating Calcium fluoride (CaF). If used as a definitive treatment, 2.5% calcium gluconate should be applied 4 to 6 times daily, for 3 to 4 days. [4]
- After 30 minutes, reassess the patient, and if pain persists, subcutaneous infiltration of calcium gluconate is recommended at a dose of 0.5 mL of a 5% solution per square centimeter of surface burn extending 0.5 cm beyond the margin of involved tissue. [19]
- With the concern for compartment syndrom, injections into the hand should be limited to 0.5 ml per phalanx with repeat injections as needed. [20]
- Additional topical therapy includes iced solution of benzalkonium chloride (Zephiran Chloride) concentration of (0.13%). Side effects of use include stinging pain or allergic reaction (urticaria, pruritus, dyspnea, chest tightness, swelling of the face, lips or tongue) or Hexafluorine solution. [12][13][21][22]
(B3)
- Eye exposure
- HF may penetrate to internal structures.
- Initial treatment for eye exposure includes irrigation with large amount of gently flowing cool plain water or sterile 0.9 % saline solution for 15-30 minutes. A topical ophthalmic anesthetic solution can be used to help mitigate the irritation from the hydrofluoric acid and water irrigation.
- Intermittent irrigation using a sterile 1% calcium gluconate solution via a Morgan lens for 20 minutes.
- Other treatment modalities include irrigation with Hexafluorine. [7]
- Inhalation exposure
- In high concentrations may cause glossitis (obstruction of the airway) and acute pulmonary edema.
- Management would include artificial respiration for the patient with severe exposure. Individuals who are breathing require 100 % oxygen with a 2.5% to 3% calcium gluconate nebulized solution.
- Noninvasive positive pressure ventilation may be necessary for individuals who develop pulmonary edem.
- Treatment of severe cases includes endotracheal intubation for airway protection and a surgical airway if necessary.
Burns with concentrated HF are usually very serious, with the potential for significant complications due to fluoride toxicity. Concentrated HF liquid or vapor may cause severe burns, metabolic imbalances, pulmonary edema, and life-threatening cardiac arrhythmias. Even moderate exposures to concentrated HF may rapidly progress to fatality if left untreated. Burns larger than 25 square inches (160 square cm) may result in serious systemic toxicity. Relief of pain is the only indication of the effectiveness of treatment. Therefore, the use of any analgesic agents is not advisable. [12][13][21](B3)
A person who has HF burns greater than four square inches should be admitted immediately to an intensive care unit and carefully monitored for 24 to 48 hours. Anyone who has been exposed to gaseous HF and experiences respiratory irritation also should be admitted to and monitored in an intensive care unit. Blood sampling should be taken to monitor fluoride, potassium, and calcium levels. In some cases, hemodialysis is necessary for fluoride removal and correction of hyperkalemia and recurrent hypocalcemia.
Differential Diagnosis
- Chemical burns
- Chlorine toxicity
- Fluoride toxicity
- Ocular burns and chemical injuries
Pearls and Other Issues
Isolation and Evacuation
- As an immediate precautionary measure, isolate spill or leak area in all directions for at least 50 meters (150 feet) for liquids and at least 25 meters (75 feet) for solids.
- SPILL: Increase, in the downwind direction, as necessary, the isolation distance shown above.
- FIRE: If tank, rail car or tank truck is involved in a fire, ISOLATE for 800 meters (1/2 mile) in all directions; also, consider initial evacuation for 800 meters (1/2 mile) in all directions.
Firefighting
- Note: Some foams will react with the material and release corrosive/toxic gases.
- SMALL FIRE: CO2 (except for Cyanides), dry chemical, dry sand, alcohol-resistant foam.
- LARGE FIRE: Water spray, fog or alcohol-resistant foam. Move containers from fire area if you can do it without risk. Use water spray or fog; do not use straight streams. Dike fire-control water for later disposal; do not scatter the material.
- FIRE INVOLVING TANKS OR CAR/TRAILER LOADS: Fight fire from maximum distance or use unmanned hose holders or monitor nozzles. Do not get water inside containers. Cool containers with flooding quantities of water until well after fire is out. Withdraw immediately in case of rising sound from venting safety devices or discoloration of tank. ALWAYS stay away from tanks engulfed in fire.
Non-Fire Response
- ELIMINATE all ignition sources (no smoking, flares, sparks or flames in immediate area). All equipment used when handling the product must be grounded. Do not touch damaged containers or spilled material unless wearing appropriate protective clothing. Stop leak if you can do it without risk. A vapor-suppressing foam may be used to reduce vapors. DO NOT GET WATER INSIDE CONTAINERS. Use water spray to reduce vapors or divert vapor cloud drift. Avoid allowing water runoff to contact spilled material. Prevent entry into waterways, sewers, basements or confined areas.
- SMALL SPILL: Cover with DRY earth, DRY sand or other non-combustible material followed with plastic sheet to minimize spreading or contact with rain. Use clean, non-sparking tools to collect material and place it into loosely covered plastic containers for later disposal.
Protective Clothing
- Wear positive pressure self-contained breathing apparatus (SCBA).
- Wear chemical protective clothing that is specifically recommended by the manufacturer. It may provide little or no thermal protection.
- Structural firefighters' protective clothing provides limited protection in fire situations ONLY; it is not effective in spill situations where direct contact with the substance is possible.
Excerpt from
- Emergency Response Guide (ERG) 157, 2016
- Substances - Toxic and/or Corrosive (Non-Combustible / Water-Sensitive)
Enhancing Healthcare Team Outcomes
Hydrofluoric acid is a common chemical that is utilized in several domestic and industrial products and treatments for producing other manufactured products. Though the literature for treatment of hydrofluoric acid is based upon animal studies and some case reports / small case series, the mainstay treatment has not changed since the mid 1970's. Prehospital and emergency medicine physicians should be familiar with the initial and ongoing management and treatment with potential life threatening arrhythmias from the sequestration of calcium, magnesium and release of potassium. Easy transfer to burn centers should be in place for continued monitoring and treatment for patients with profound hydrofluroic acid burns.
Media
(Click Image to Enlarge)
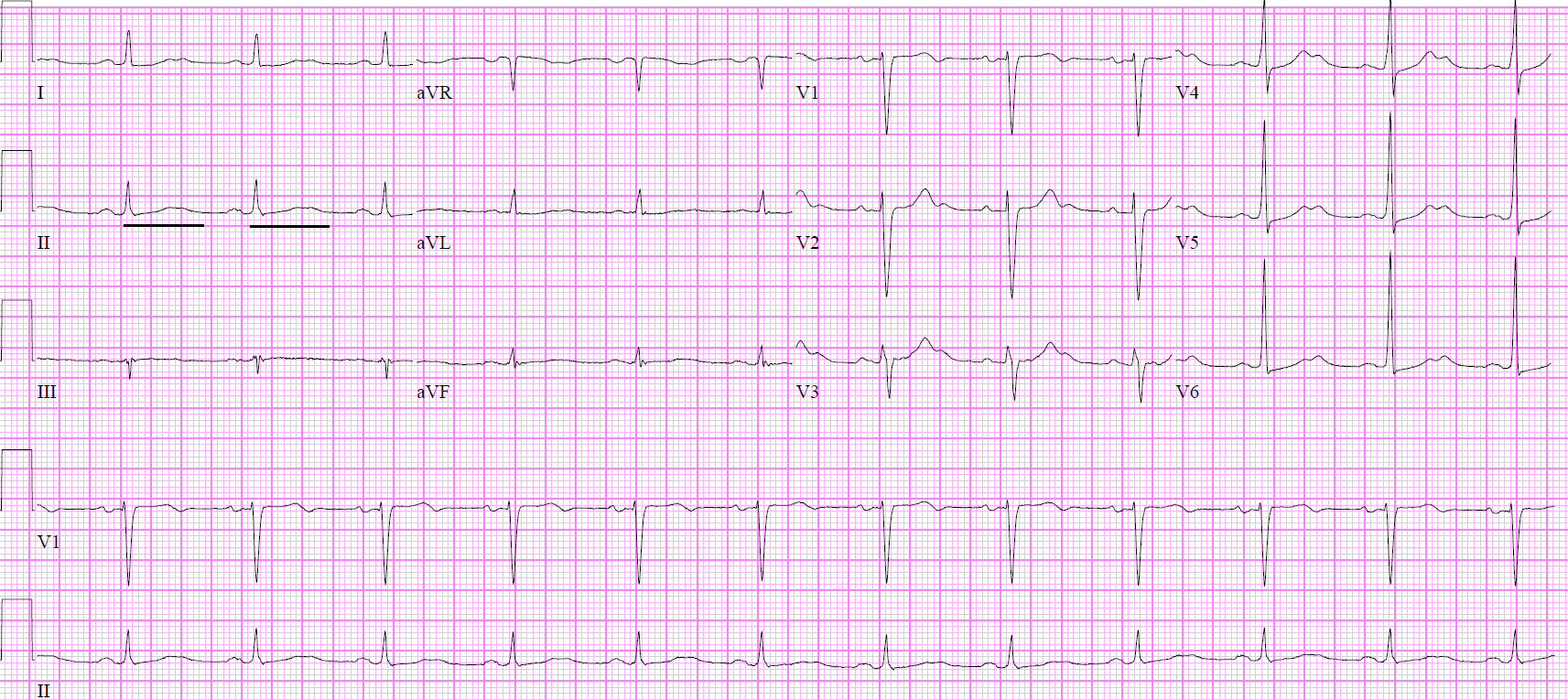
EKG Prolonged QTc Contributed by Daniel Schwerin, MD, FACEP, FAEMS, FAAEM
References
Wu ML, Yang CC, Ger J, Tsai WJ, Deng JF. Acute hydrofluoric acid exposure reported to Taiwan Poison Control Center, 1991-2010. Human & experimental toxicology. 2014 May:33(5):449-54. doi: 10.1177/0960327113499165. Epub 2013 Jul 25 [PubMed PMID: 23892993]
Level 2 (mid-level) evidenceStuke LE, Arnoldo BD, Hunt JL, Purdue GF. Hydrofluoric acid burns: a 15-year experience. Journal of burn care & research : official publication of the American Burn Association. 2008 Nov-Dec:29(6):893-6. doi: 10.1097/BCR.0b013e31818b9de6. Epub [PubMed PMID: 18849854]
Level 2 (mid-level) evidenceKim Y, Shin J, Kang S, Kyung S, Park JW, Lee S, Lee S, Jeong SH. Pulmonary alveolar proteinosis induced by hydrofluoric acid exposure during fire extinguisher testing. Journal of occupational medicine and toxicology (London, England). 2015:10():6. doi: 10.1186/s12995-015-0048-7. Epub 2015 Feb 25 [PubMed PMID: 25737738]
Level 3 (low-level) evidenceBajraktarova-Valjakova E, Korunoska-Stevkovska V, Georgieva S, Ivanovski K, Bajraktarova-Misevska C, Mijoska A, Grozdanov A. Hydrofluoric Acid: Burns and Systemic Toxicity, Protective Measures, Immediate and Hospital Medical Treatment. Open access Macedonian journal of medical sciences. 2018 Nov 25:6(11):2257-2269. doi: 10.3889/oamjms.2018.429. Epub 2018 Nov 20 [PubMed PMID: 30559898]
Franzblau A, Sahakian N. Asthma following household exposure to hydrofluoric acid. American journal of industrial medicine. 2003 Sep:44(3):321-4 [PubMed PMID: 12929153]
Level 3 (low-level) evidenceSmędra-Kaźmirska A, Kędzierski M, Barzdo M, Jurczyk A, Szram S, Berent J. Accidental intoxication with hydrochloric acid and hydrofluoric acid mixture. Archiwum medycyny sadowej i kryminologii. 2014 Jan-Mar:64(1):50-8 [PubMed PMID: 25184427]
Atley K, Ridyard E. Treatment of hydrofluoric acid exposure to the eye. International journal of ophthalmology. 2015:8(1):157-61. doi: 10.3980/j.issn.2222-3959.2015.01.28. Epub 2015 Feb 18 [PubMed PMID: 25709926]
Ozsoy G, Kendirli T, Ates U, Perk O, Azapagasi E, Ozcan S, Baran C, Goktug A, Dindar H. Fatal Refractory Ventricular Fibrillation Due to Ingestion of Hydrofluoric Acid. Pediatric emergency care. 2019 Nov:35(11):e201-e202. doi: 10.1097/PEC.0000000000001548. Epub [PubMed PMID: 30020244]
Gradinger R, Jung C, Reinhardt D, Mall G, Figulla HR. Toxic myocarditis due to oral ingestion of hydrofluoric acid. Heart, lung & circulation. 2008 Jun:17(3):248-50 [PubMed PMID: 17822953]
Level 3 (low-level) evidenceVohra R, Velez LI, Rivera W, Benitez FL, Delaney KA. Recurrent life-threatening ventricular dysrhythmias associated with acute hydrofluoric acid ingestion: observations in one case and implications for mechanism of toxicity. Clinical toxicology (Philadelphia, Pa.). 2008 Jan:46(1):79-84 [PubMed PMID: 17906993]
Level 3 (low-level) evidenceWhiteley PM, Aks SE. Case files of the Toxikon Consortium in Chicago: survival after intentional ingestion of hydrofluoric acid. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2010 Sep:6(3):349-54. doi: 10.1007/s13181-010-0088-4. Epub [PubMed PMID: 20661686]
Level 3 (low-level) evidenceMcKee D, Thoma A, Bailey K, Fish J. A review of hydrofluoric acid burn management. Plastic surgery (Oakville, Ont.). 2014 Summer:22(2):95-8 [PubMed PMID: 25114621]
Alper N, Desai K, Rabinowitz S. Management of hydrofluoric Acid burns. Eplasty. 2014:14():ic42 [PubMed PMID: 25525489]
Level 3 (low-level) evidenceYe C, Wang X, Zhang Y, Ni L, Jiang R, Liu L, Han C. Ten-year epidemiology of chemical burns in western Zhejiang Province, China. Burns : journal of the International Society for Burn Injuries. 2016 May:42(3):668-74. doi: 10.1016/j.burns.2015.12.004. Epub 2016 Jan 20 [PubMed PMID: 26803372]
Zhang Y, Zhang J, Jiang X, Ni L, Ye C, Han C, Sharma K, Wang X. Hydrofluoric acid burns in the western Zhejiang Province of China: a 10-year epidemiological study. Journal of occupational medicine and toxicology (London, England). 2016:11():55 [PubMed PMID: 27980604]
Level 2 (mid-level) evidencePu Q, Qian J, Tao W, Yang A, Wu J, Wang Y. Extracorporeal membrane oxygenation combined with continuous renal replacement therapy in cutaneous burn and inhalation injury caused by hydrofluoric acid and nitric acid. Medicine. 2017 Dec:96(48):e8972. doi: 10.1097/MD.0000000000008972. Epub [PubMed PMID: 29310404]
Level 2 (mid-level) evidenceDennerlein K, Kiesewetter F, Kilo S, Jäger T, Göen T, Korinth G, Drexler H. Dermal absorption and skin damage following hydrofluoric acid exposure in an ex vivo human skin model. Toxicology letters. 2016 Apr 25:248():25-33. doi: 10.1016/j.toxlet.2016.02.015. Epub 2016 Feb 27 [PubMed PMID: 26930472]
Level 3 (low-level) evidenceHultén P, Höjer J, Ludwigs U, Janson A. Hexafluorine vs. standard decontamination to reduce systemic toxicity after dermal exposure to hydrofluoric acid. Journal of toxicology. Clinical toxicology. 2004:42(4):355-61 [PubMed PMID: 15461243]
Level 3 (low-level) evidenceDibbell DG, Iverson RE, Jones W, Laub DR, Madison MS. Hydrofluoric acid burns of the hand. The Journal of bone and joint surgery. American volume. 1970 Jul:52(5):931-6 [PubMed PMID: 5479482]
Edelman P. Hydrofluoric acid burns. Occupational medicine (Philadelphia, Pa.). 1986 Jan-Mar:1(1):89-103 [PubMed PMID: 3299779]
Robinson EP, Chhabra AB. Hand chemical burns. The Journal of hand surgery. 2015 Mar:40(3):605-12; quiz 613. doi: 10.1016/j.jhsa.2014.07.056. Epub 2015 Feb 1 [PubMed PMID: 25653184]
Ohtani M, Nishida N, Chiba T, Muto H, Yoshioka N. Pathological demonstration of rapid involvement into the subcutaneous tissue in a case of fatal hydrofluoric acid burns. Forensic science international. 2007 Mar 22:167(1):49-52 [PubMed PMID: 16426786]
Level 3 (low-level) evidence