 Anatomy, Abdomen and Pelvis: Hepatoduodenal Ligament
Anatomy, Abdomen and Pelvis: Hepatoduodenal Ligament
Introduction
The hepatoduodenal ligament is a thick anatomical structure wrapped in the peritoneum that constitutes part of the lesser omentum. The hepatoduodenal ligament runs from the porta hepatis to the proximal 2 cm of the duodenum. The hepatic artery proper, common bile duct, and portal vein run through the ligament near its free edge to reach the liver. These 3 structures are often referred to as the portal triad.[1] The hepatic artery proper is a branch of the common hepatic artery originating from the celiac trunk. The hepatic portal vein is the main drainage site of the spleen and the small and large intestines. It brings nutrient-rich but oxygen-poor blood from these organs via the splenic, superior, and inferior mesenteric veins. The common bile duct is a tube-like structure that helps carry bile from the gallbladder to the lumen of the duodenum. It forms from unifying the cystic duct from the gallbladder and the common hepatic duct. These 3 important structures exist within the hepatoduodenal ligament. Understanding the location, content, and function of the hepatoduodenal ligament is important when pathology arises or performing surgery in surrounding structures.[2][1][3][4] See image. Abdominal Cavity Organs.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The hepatoduodenal ligament is a double-layered tubular structure composed of a peritoneum that encloses the portal triad. The opening behind the free edge of the hepatoduodenal ligament is the omental foramen (foramen of Winslow), the only opening of the lesser sac and the sole connection between the lesser sac and the greater peritoneal cavity.[5] To locate the hepatoduodenal ligament, 1 may start from the hepatogastric ligament and follow the lesser curvature of the stomach inferiorly towards the pylorus. The hepatoduodenal ligament is felt or seen connected to the proximal portion of the duodenum. The primary function of this ligament is to protect and encompass the 3 important structures known as the portal triad, which provides adequate blood supply to the liver and promotes bile flow into the lumen of the duodenum. About 75% of the liver's blood supply comes from the portal vein, and the remaining 25% comes from the hepatic artery.[6] The hepatoduodenal ligament can also be a landmark during certain surgical procedures, such as the Pringle maneuver.[4]
Embryology
During the embryological formation of the gastrointestinal tract, the foregut is suspended from the abdominal wall by a double layer of peritoneum called the mesentery. The hepatoduodenal ligament derives from the ventral mesentery between the liver and the stomach as part of the lesser omentum. After the stomach migrates to its final location, the space posterior to it becomes the lesser sac, and the opening to this sac appears at the distal edge of the hepatoduodenal ligament. This opening is called the foramen of Winslow.[5]
Blood Supply and Lymphatics
Various vessels surround the hepatoduodenal ligament that may contribute to the blood supply of this ligament. Aside from the hepatic artery proper and the portal vein that runs through the ligament, other vessels are adjacent to this structure. The right gastric artery, which derives from the left hepatic artery, the common hepatic artery, and part of the gastroduodenal artery, seems to be associated with the blood supply of the hepatoduodenal ligament, and the right gastric vein typically drains blood.[7] The hepatoduodenal ligament has lymphatic pathways, which flow into the Pecquet cistern at a sub-diaphragmatic level. It also has the name "pars tensa" of the small omentum; its thickness contains the portal triad, the portal vein, the hepatic artery, and the common bile duct.
Nerves
The nerve supply of the hepatoduodenal ligament remains undetermined, but postsynaptic sympathetic nerve fibers may be associated with the vascular structure. The vagus nerve divides into anterior and posterior branches as it enters the abdominal region. The anterior branch further divides into smaller branches, which travel through the lesser omentum. The vagus nerve also runs through the portal triad, which may play a role in the parasympathetic nerve supply of the ligament.[8]
Muscles
No clinically significant skeletal or smooth muscle fibers have associations with the hepatoduodenal ligament.
Physiologic Variants
Although anatomic variations of the hepatoduodenal ligament are rare, the content of the ligament may differ in the general population. Variation of the hepatic artery is common and is clinically important to identify before any surgery in this region is performed. If a specific significant variation exists, devastating hemorrhagic complications may occur. The most common variants include the right hepatic artery arising from the superior mesenteric artery that runs behind the pancreatic head along the right posterolateral flank of the portal vein, and the left hepatic artery as it arises from the left gastric artery that runs in the lesser omentum.[9]
Surgical Considerations
When the liver is injured during surgery or penetrating trauma, the bleeding can be torrential and quickly lead to hemorrhagic shock or death. A lifesaving maneuver sometimes performed to stop the bleeding is the Pringle maneuver, first described in 1908 by a surgeon named James Hogarth Pringle in Glasgow, Scotland. This surgical maneuver involves compressing the hepatoduodenal ligament with a clamp. This clamping interrupts blood flow to the liver and helps control bleeding. If no clamp is available, 1 may use their fingers to compress the ligament. If the bleeding from the liver continues, the inferior vena cava or the hepatic vein may have suffered an injury.[2] Complications of the Pringle maneuver include ischemia and portal hypertension. It may also lead to a reperfusion phenomenon if the clamping time is prolonged. There are no absolute contraindications to the Pringle maneuver. However, in patients with a compromised liver function, such as cirrhosis, 1 should not clamp for more than 10 minutes at a time.[10] Otherwise, it can lead to permanent injury to the liver. The clamp should be intermittently released at 30 to 45 minutes so that the liver is not completely without blood for an extended period to minimize complications.[2]
Clinical Significance
Viscera of the upper abdomen, pelvis, retroperitoneum, and body wall connect via many peritoneal ligaments, including the hepatoduodenal ligament. As a result of this proximity, the hepatoduodenal ligament is an important pathway of inflammatory and neoplastic disease between the stomach, retroperitoneum, and the porta hepatis through mechanisms such as direct invasion and lymphatic extension. Lymph nodes that surround this ligament can facilitate the spread of disease.[11] For example, cancer from the pancreas and colon can spread to the nodes surrounding the superior mesenteric artery and eventually travel up the lymphatic channels in the hepatoduodenal ligament to the liver. Lymphatic fluid can also travel from the liver and biliary system to lymph nodes adjacent to the duodenum and pancreas, spreading disease to the retroperitoneum. Direct invasion can occur with certain inflammatory diseases, such as pancreatitis and inflammation from the biliary system. A disease that originates from the lesser curvature of the stomach, such as gastric cancer, can also spread to lymph nodes via direct invasion.[12] The hematologic spread of disease can occur through the portal vein and carry disease from the gastrointestinal tract to the liver.[11] On rare occasions, vascular complications may occur when disease travels through the hepatoduodenal ligament, such as in hepatic arterial pseudoaneurysms and portal vein thrombosis.[13][4][14]
Other Issues
The tools for assessing the hepatoduodenal ligament are different:
- Ultrasonography is the simplest and most informative tool for blood flow evaluation.
- Multidetector computed tomography can provide a general evaluation.
- Magnetic resonance imaging has a higher resolution for soft tissues.
- Magnetic resonance cholangiography is useful to understand the clinical situation of the biliary tract.
- Endoscopic retrograde cholangiopancreatography is used for an initial and general evaluation.
- Fludeoxyglucose positron emission tomography-computed tomography is used when there is a need to evaluate the presence of tumors.
- Endoscopic and intraductal ultrasonography are more effective for some authors as assessment tools for the biliary area.[15]
Media
(Click Image to Enlarge)
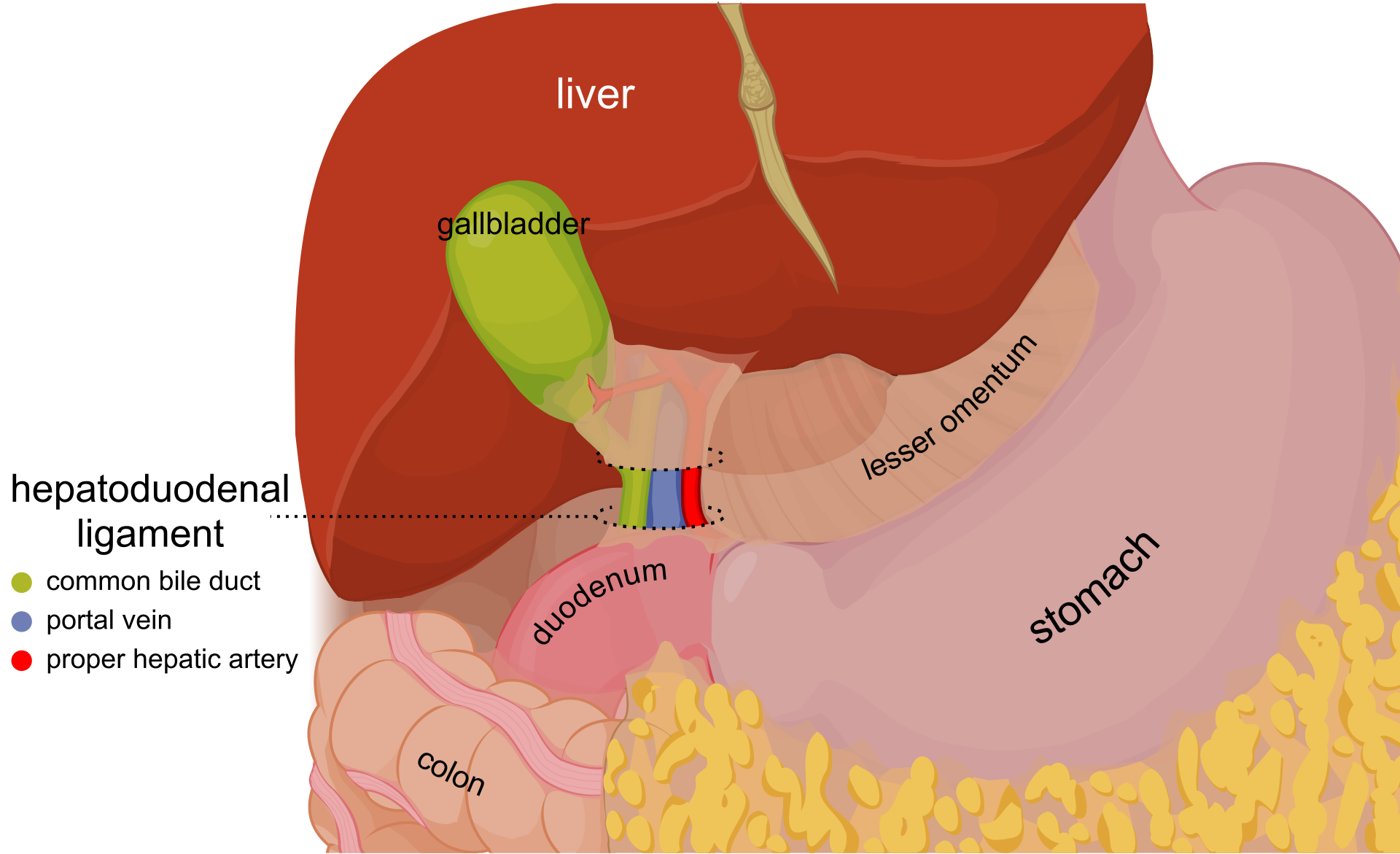
Abdominal Cavity Organs. The abdominal cavity organs with the anterior margin of the liver dragged to the top. The hepatoduodenal ligament is marked, and the partially serous membrane is cut off to show its content.
Olek Remesz, Public Domain, via Wikimedia Commons
References
Vernon H, Wehrle CJ, Alia VSK, Kasi A. Anatomy, Abdomen and Pelvis: Liver. StatPearls. 2024 Jan:(): [PubMed PMID: 29763190]
Jurkovich GJ, Hoyt DB, Moore FA, Ney AL, Morris JA Jr, Scalea TM, Pachter HL, Davis JW. Portal triad injuries. The Journal of trauma. 1995 Sep:39(3):426-34 [PubMed PMID: 7473903]
Level 2 (mid-level) evidenceTakahashi N, Itoh K, Itoh H, Haba H, Ishii Y. [Anatomy of hepatoduodenal ligament on MR imaging]. Rinsho hoshasen. Clinical radiography. 1989 Dec:34(13):1585-9 [PubMed PMID: 2622050]
Kalra A, Yetiskul E, Wehrle CJ, Tuma F. Physiology, Liver. StatPearls. 2024 Jan:(): [PubMed PMID: 30571059]
Thomas JM, Van Fossen K. Anatomy, Abdomen and Pelvis: Foramen of Winslow (Omental Foramen, Epiploic Foramen). StatPearls. 2024 Jan:(): [PubMed PMID: 29489171]
Qiao JL, Sun J, Li J, Zhang JJ, Meng XK. Liver dual arterial blood supply maintains liver regeneration: Analysis of signaling pathways in rats. Molecular medicine reports. 2018 Jan:17(1):979-987. doi: 10.3892/mmr.2017.7961. Epub 2017 Nov 3 [PubMed PMID: 29115531]
Level 2 (mid-level) evidenceIbukuro K, Fukuda H, Tobe K, Akita K, Takeguchi T. The vascular anatomy of the ligaments of the liver: gross anatomy, imaging and clinical applications. The British journal of radiology. 2016 Aug:89(1064):20150925. doi: 10.1259/bjr.20150925. Epub 2016 May 10 [PubMed PMID: 27163944]
Abdel-Misih SR,Bloomston M, Liver anatomy. The Surgical clinics of North America. 2010 Aug; [PubMed PMID: 20637938]
Noussios G, Dimitriou I, Chatzis I, Katsourakis A. The Main Anatomic Variations of the Hepatic Artery and Their Importance in Surgical Practice: Review of the Literature. Journal of clinical medicine research. 2017 Apr:9(4):248-252. doi: 10.14740/jocmr2902w. Epub 2017 Feb 21 [PubMed PMID: 28270883]
Delva E, Camus Y, Paugam C, Parc R, Huguet C, Lienhart A. Hemodynamic effects of portal triad clamping in humans. Anesthesia and analgesia. 1987 Sep:66(9):864-8 [PubMed PMID: 3619092]
Alessandrino F, Ivanovic AM, Souza D, Chaoui AS, Djokic-Kovac J, Mortele KJ. The hepatoduodenal ligament revisited: cross-sectional imaging spectrum of non-neoplastic conditions. Abdominal radiology (New York). 2019 Apr:44(4):1269-1294. doi: 10.1007/s00261-018-1829-0. Epub [PubMed PMID: 30448917]
Level 2 (mid-level) evidenceLee SL,Lee HH,Ko YH,Song KY,Park CH,Jeon HM,Kim SS, Relevance of hepatoduodenal ligament lymph nodes in resectional surgery for gastric cancer. The British journal of surgery. 2014 Apr; [PubMed PMID: 24615472]
Okada Y, Yao YK, Yunoki M, Sugita T. Lymph nodes in the hepatoduodenal ligament: US appearances with CT and MR correlation. Clinical radiology. 1996 Mar:51(3):160-6 [PubMed PMID: 8605744]
Taylor I, Bennett R, Sherriff S. The blood supply of colorectal liver metastases. British journal of cancer. 1978 Dec:38(6):749-56 [PubMed PMID: 743492]
Sharma M, Rameshbabu CS, Dietrich CF, Rai P, Bansal R. Endoscopic ultrasound of the hepatoduodenal ligament and liver hilum. Endoscopic ultrasound. 2018 May-Jun:7(3):168-174. doi: 10.4103/2303-9027.193584. Epub [PubMed PMID: 27824022]