Introduction
The greater petrosal nerve, also known as the greater superficial petrosal nerve, is a branch of the nervus intermedius (nerve of Wrisberg) that carries parasympathetic, taste, and general sensory fibers from the facial nerve (10th cranial nerve or cranial nerve VII). This nerve arises from the superior salivatory nucleus in the brainstem, passes through the geniculate ganglion without synapsing, and exits through the facial hiatus of the petrous bone. The greater petrosal nerve fuses with the deep petrosal nerve to form the Vidian nerve, which courses toward the pterygopalatine ganglion. The parasympathetic branches of the greater petrosal nerve stimulate the lacrimal, nasopharyngeal, and palatine mucosal glands.[1] Lesions along the greater petrosal nerve may cause xerophthalmia, facial palsy, hearing loss, and altered taste sensations. This nerve is also a vital landmark for middle cranial fossa procedures. Understanding the anatomy and function of the greater petrosal nerve is essential in managing various head and neck disorders.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The preganglionic parasympathetic fibers of the greater petrosal nerve originate from the superior salivatory nucleus within the tractus solitarius of the pontine tegmentum, progressing in the nervus intermedius before joining the facial nerve (see Image. Greater Petrosal Nerve).[2] These fibers transverse the geniculate ganglion without synapsing and exit anteriorly as the greater petrosal nerve.[3] The nerve courses anteromedially, leaving the superior surface of the temporal bone through the greater petrosal nerve hiatus (facial hiatus or hiatus fallopii) and entering the middle temporal fossa.[4] Within the facial hiatus, the greater petrosal nerve travels alongside the middle meningeal artery. From there, the nerve crosses the floor of the middle temporal fossa, moving medially to the lesser petrosal nerve and laterally to the internal carotid artery. The nerve then travels anteromedially and slightly inferiorly, passing beneath the Gasserian ganglion in the Meckel cave before continuing towards the foramen lacerum and the pterygoid (Vidian) canal.[5][6] Some authors thus divide the nerve into 4 segments as follows:
- Intrapetrosal segment running from the geniculate ganglion to the facial hiatus
- Suprapetrosal portion running from the facial hiatus to the foramen lacerum
- Segment traversing the foramen lacerum
- Segment running through the pterygoid canal [7]
The greater petrosal nerve joins the deep petrosal nerve in the proximal region of the pterygoid canal, forming the Vidian nerve (nerve of the pterygoid canal).[8][9] This union allows the Vidian nerve to carry preganglionic, sensory, and taste fibers from the greater petrosal nerve and postganglionic sympathetic fibers from the internal carotid plexus through the deep petrosal nerve. The Vidian nerve continues anteriorly within the pterygoid canal to the pterygopalatine fossa (see Image. Pterygopalatine Fossa Nerves). The sympathetic fibers of the deep petrosal nerve cross the pterygopalatine fossa without synapsing and provide all branches of the trigeminal nerve's maxillary division (second division of the fifth cranial nerve or cranial nerve V2) with sympathetic innervation. The parasympathetic fibers synapse at the pterygopalatine ganglion (sphenopalatine ganglion). Postganglionic parasympathetic fibers provide secretory and vasomotor innervation to the lacrimal, nasopharyngeal, and palatine glands.
Function
The greater petrosal nerve is a mixed nerve carrying parasympathetic, taste, and sensory fibers. The parasympathetic fibers synapse at the pterygopalatine ganglion, as mentioned. Parasympathetic fibers exit the pterygopalatine ganglion through 4 routes as follows:
- The greater palatine nerve that innervates the bony hard palate of the mouth
- The lesser palatine branch that supplies the uvula, tonsils, and soft palate
- The nasopalatine and posterior nasal branches that innervate the nasal mucous membranes
- The pharyngeal branch that supplies the nasopharyngeal glands and mucosa
The nerves in these regions also carry postganglionic sympathetic fibers from the deep petrosal nerve. The pterygopalatine ganglion receives 2 to 3 branches of cranial nerve V2—pterygoid branches—besides the Vidian nerve. This anatomical arrangement allows cranial nerve VII, the greater petrosal, and deep petrosal nerve to utilize the trigeminal as an expressway for their respective autonomic fibers. The postganglionic sympathetic and parasympathetic fibers that travel alongside the zygomatic nerve of cranial nerve V2 supply the lacrimal glands. Therefore, the greater petrosal nerve enhances the secretomotor function of the nasal-palatal glands and mucosa and mediates reflexive tearing in the lacrimal glands. The greater petrosal nerve also transmits soft palate taste afferents, dura mater, internal carotid artery, and pterygopalatine ganglion sensory fibers toward the geniculate ganglion.[10] The greater petrosal nerve also communicates with the lesser petrosal nerve.[11]
Embryology
After the third week of development, a neural crest cell cluster becomes apparent on the metencephalon rostral to the otic placode. This cluster is the facioacoustic primordium that gives rise to cranial nerves VII and VIII. By week 4, the facial and acoustic portions are better defined, with the facial section terminating at the epibranchial placode on the second branchial arch.[12] The greater petrosal nerve may be first observed during weeks 5 to 6 of embryogenic development rostral to the geniculate ganglion. The nerve becomes well-defined by the eighth week when it joins the deep petrosal nerve near the developing internal carotid artery to form the Vidian nerve.[13] The greater petrosal nerve terminates into a group of neural crest cells that develops into the pterygopalatine ganglion.[14]
Blood Supply and Lymphatics
The greater petrosal nerve receives its blood supply from the superficial petrosal branch of the middle meningeal artery, which anastomoses with the stylomastoid branch of the posterior auricular artery and the pterygoid canal artery.[15] The superior petrosal vein drains the superficial petrosal nerve. The lymphatic vessels of the nerve empty into the skull's glymphatic system, although the details of this relationship remain unknown.
Nerves
According to some authors, the greater petrosal nerve is divided into 4 anatomical areas. The first portion is the intrapetrosal portion. The second comprises the suprapetrosal segment. The third anatomical area traverses the foramen lacerum. The fourth segment courses through the pterygoid canal. About 17.5% of the nerve interconnects with the glossopharyngeal nerve.
Physiologic Variants
The greater petrosal nerve demonstrates some variation in its distance relative to surrounding bony prominences and length as it traverses different segments. The bony coverings of the nerve also exhibit significant variability. The greater petrosal and glossopharyngeal nerves may also form interconnections.
Surgical Considerations
The greater petrosal nerve is a useful landmark for locating the geniculate ganglion, internal auditory canal, and middle cranial fossa. Identifying the greater petrosal nerve in the middle cranial fossa helps delineate the Kawase (posteromedial) and Glasscock (posterolateral) triangles, reducing injury risk to essential structures in these regions. Identifying the Kawase triangle before drilling during an anterior petrosectomy can help avert facial nerve and internal carotid artery damage.[16] Due to its vulnerable location, the greater petrosal nerve is also prone to injury from bone drilling, dural elevation off the middle fossa floor, electrocauterization, or dissection. Hence, bony landmarks and anatomical distances have been published to help identify this nerve during surgery.
Clinical Significance
Injuries to the greater petrosal nerve resulting from surgical procedures, tumors, or skull fractures can lead to ipsilateral xerotic keratitis. Reduced lacrimation can promote corneal dryness, xerophthalmia, corneal ulceration, or infection. Degeneration of the greater petrosal nerve due to lesions occurring along the path of cranial nerve VII toward the geniculate ganglion promotes the development of parasympathetic collaterals from the lesser petrosal nerve to the lacrimal glands. The lesser petrosal nerve contributes parasympathetic fibers to the parotid gland to aid in salivation. Interconnections between the greater and lesser petrosal nerves may lead to simultaneous lacrimation on salivation. Cluster headaches with parasympathetic dysfunction involving the greater petrosal nerve have been described. These conditions include Horton headaches and Sluder neuralgia, which present with rhinorrhea, mucosal congestion, and hyperlacrimation. Surgical nerve sectioning has been used to treat these headaches in the past. Sphenopalatine ganglion blockade by local anesthetic injection and radiofrequency ablation has been investigated recently for cluster headaches, with promising results.[17] Although rare, tumors of the greater petrosal nerve have also been reported. Schwannomas of this nerve may present with xerophthalmia, facial paralysis, and conductive hearing loss.[18]
Other Issues
The greater petrosal nerve innervates the taste receptors of the palate. Animal studies have shown the nerve's role in differentiating flavors and detecting the presence of substances such as salt, quinine, and sucrose. Greater petrosal nerve information reaches the solitary tract nucleus to help regulate energy and electrolyte homeostasis.[19]
Media
(Click Image to Enlarge)
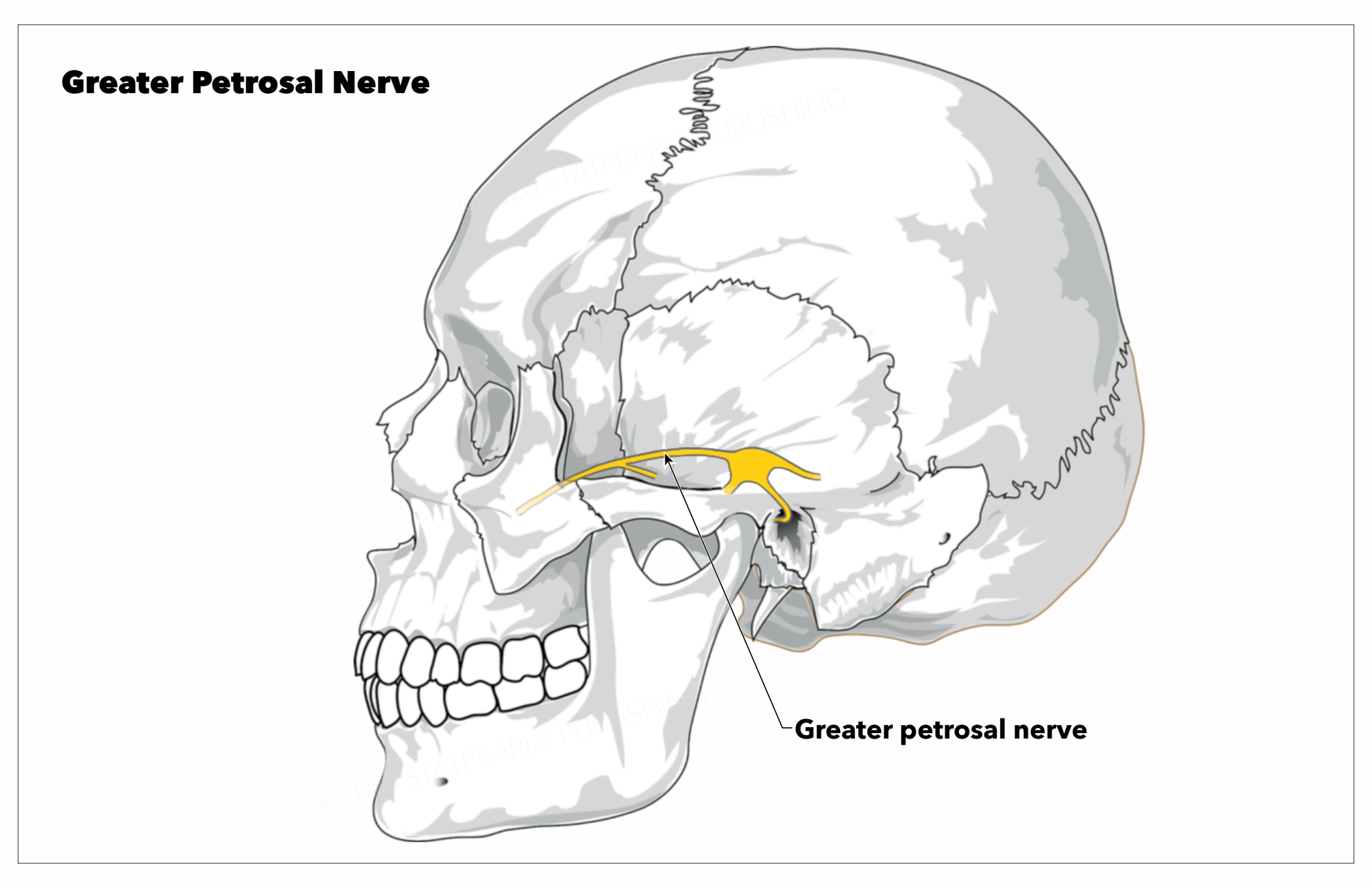
Greater Petrosal Nerve. This image shows the greater petrosal nerve's course within the craniofacial region.
StatPearls Publishing Illustration
(Click Image to Enlarge)
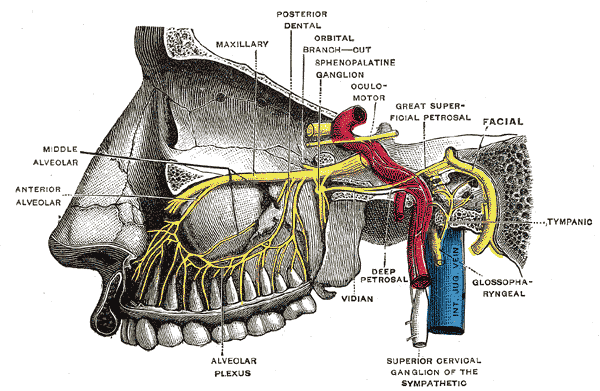
Pterygopalatine Fossa Nerves. Depiction of the pterygopalatine ganglion and the deep petrosal and Vidian nerves.
Henry Vandyke Carter, (plate 779), Public Domain, via Wikimedia Commons
References
Tayebi Meybodi A, Mignucci-Jiménez G, Lawton MT, Liu JK, Preul MC, Sun H. Comprehensive microsurgical anatomy of the middle cranial fossa: Part II-neurovascular anatomy. Frontiers in surgery. 2023:10():1132784. doi: 10.3389/fsurg.2023.1132784. Epub 2023 Mar 24 [PubMed PMID: 37035563]
Prasad S, Lee TC, Chiocca EA, Klein JP. Superficial greater petrosal neuropathy. Neurology. Clinical practice. 2014 Dec:4(6):505-507. doi: 10.1212/CPJ.0000000000000066. Epub [PubMed PMID: 29443140]
Tubbs RS, Menendez J, Loukas M, Shoja MM, Shokouhi G, Salter EG, Cohen-Gadol A. The petrosal nerves: anatomy, pathology, and surgical considerations. Clinical anatomy (New York, N.Y.). 2009 Jul:22(5):537-44. doi: 10.1002/ca.20814. Epub [PubMed PMID: 19544297]
Ginsberg LE, De Monte F, Gillenwater AM. Greater superficial petrosal nerve: anatomy and MR findings in perineural tumor spread. AJNR. American journal of neuroradiology. 1996 Feb:17(2):389-93 [PubMed PMID: 8938317]
Level 3 (low-level) evidenceVidić B, Young PA. Gross and microscopic observations on the communicating branch of the facial nerve to the lesser petrosal nerve. The Anatomical record. 1967 Jul:158(3):257-61 [PubMed PMID: 6055071]
Tubbs RS, Custis JW, Salter EG, Sheetz J, Zehren SJ, Oakes WJ. Landmarks for the greater petrosal nerve. Clinical anatomy (New York, N.Y.). 2005 Apr:18(3):210-4 [PubMed PMID: 15768412]
Shao YX, Xie X, Liang HS, Zhou J, Jing M, Liu EZ. Microsurgical anatomy of the greater superficial petrosal nerve. World neurosurgery. 2012 Jan:77(1):172-82. doi: 10.1016/j.wneu.2011.06.035. Epub 2011 Nov 1 [PubMed PMID: 22120573]
Goosmann MM, Dalvin M. Anatomy, Head and Neck, Deep Petrosal Nerve. StatPearls. 2024 Jan:(): [PubMed PMID: 30521238]
Khonsary SA, Ma Q, Villablanca P, Emerson J, Malkasian D. Clinical functional anatomy of the pterygopalatine ganglion, cephalgia and related dysautonomias: A review. Surgical neurology international. 2013:4(Suppl 6):S422-8. doi: 10.4103/2152-7806.121628. Epub 2013 Nov 20 [PubMed PMID: 24349865]
GARDNER WJ, STOWELL A, DUTLINGER R. Resection of the greater superficial petrosal nerve in the treatment of unilateral headache. Journal of neurosurgery. 1947 Mar:4(2):105-14 [PubMed PMID: 20293608]
Vidić B. The origin and the course of the communicating branch of the facial nerve to the lesser petrosal nerve in man. The Anatomical record. 1968 Dec:162(4):511-6 [PubMed PMID: 5705481]
Sataloff RT. Embryology of the facial nerve and its clinical applications. The Laryngoscope. 1990 Sep:100(9):969-84 [PubMed PMID: 2395407]
Sataloff RT, Selber JC. Phylogeny and embryology of the facial nerve and related structures. Part II: Embryology. Ear, nose, & throat journal. 2003 Oct:82(10):764-6, 769-72, 774 passim [PubMed PMID: 14606174]
Espinosa-Medina I, Outin E, Picard CA, Chettouh Z, Dymecki S, Consalez GG, Coppola E, Brunet JF. Neurodevelopment. Parasympathetic ganglia derive from Schwann cell precursors. Science (New York, N.Y.). 2014 Jul 4:345(6192):87-90. doi: 10.1126/science.1253286. Epub 2014 Jun 12 [PubMed PMID: 24925912]
Level 3 (low-level) evidenceBhatia KD, Kortman H, Lee H, Waelchli T, Radovanovic I, Schaafsma JD, Pereira VM, Krings T. Facial Nerve Arterial Arcade Supply in Dural Arteriovenous Fistulas: Anatomy and Treatment Strategies. AJNR. American journal of neuroradiology. 2020 Apr:41(4):687-692. doi: 10.3174/ajnr.A6449. Epub 2020 Mar 19 [PubMed PMID: 32193191]
Tomio R, Akiyama T, Ohira T, Horikoshi T, Yoshida K. Usefulness of facial nerve monitoring for confirmation of greater superficial petrosal nerve in anterior transpetrosal approach. Acta neurochirurgica. 2014 Oct:156(10):1847-52. doi: 10.1007/s00701-014-2162-1. Epub 2014 Jun 27 [PubMed PMID: 24969175]
Tolba R, Weiss AL, Denis DJ. Sphenopalatine Ganglion Block and Radiofrequency Ablation: Technical Notes and Efficacy. Ochsner journal. 2019 Spring:19(1):32-37. doi: 10.31486/toj.18.0163. Epub [PubMed PMID: 30983899]
Wang Z, Zhang S, Qi Y, Cao L, Li P, Zhang Q. Excision of Greater Superficial Petrosal Nerve Schwannoma Via a Pure Endoscopic Endonasal Approach. Ear, nose, & throat journal. 2024 Jan:103(1):13-18. doi: 10.1177/01455613211026397. Epub 2021 Jul 19 [PubMed PMID: 34281408]
Level 2 (mid-level) evidenceSollars SI, Hill DL. In vivo recordings from rat geniculate ganglia: taste response properties of individual greater superficial petrosal and chorda tympani neurones. The Journal of physiology. 2005 May 1:564(Pt 3):877-93 [PubMed PMID: 15746166]
Level 3 (low-level) evidence