Introduction
Graft-versus-host disease (GVHD) is a systemic disorder occurring when immune cells from transplanted tissue recognize the recipient's body as foreign and attack its cells. In this context, graft refers to transplanted or donated tissue, while host refers to the recipient's tissues. GVHD is a common complication following allogeneic hematopoietic stem cell transplant.[1]
GVHD has traditionally been categorized based on the timing of presentation into acute and chronic, with a cutoff of 100 days post-transplant. These classifications have been further refined based on clinical manifestations accepted by the National Institutes of Health (NIH):
- Acute classic GVHD presents within 100 days of transplantation with typical clinical features of acute GVHD.
- Persistent, recurrent, or late-onset acute GVHD manifests with clinical features of classic acute GVHD but after 100 days of transplantation.
- Classic chronic GVHD presents after 100 days of transplant with classic clinical features of chronic GVHD.
- Overlap syndrome may occur at any time posttransplant with features of both acute and chronic GVHD.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
GVHD arises from a complex interplay of immunological factors during allogeneic transplantation. The etiology of GVHD involves the recognition of recipient tissues as foreign by donor immune cells, leading to an immune-mediated attack on the host. GVHD occurs in the following settings:
- Following allogeneic bone transplantation (most common)
- Following transplantation of solid organs that are rich in lymphoid cells (eg liver)
- Following transfusion of nonirradiated blood
For GVHD to occur, immunologically competent cells should be transplanted into immunodeficient recipients, and these transferred cells should recognize alloantigens in the host. Other important factors that determine the occurrence and severity of GVHD include:
- Donor-host factors: The incidence of GVHD increases with unmatched donor transplants, human leukocyte antigen (HLA) disparity, and sex mismatching.
- Stem-cell source factors: Cryopreservation of marrow before infusion and the use of umbilical cord blood decrease the incidence of GVHD.
- Immune modulation factors: The incidence of GVHD is lower with triple therapy (cyclosporine, methotrexate [MTX], and prednisone) as compared with double therapy (cyclosporine and MTX).[2] In preclinical settings, statins can inhibit antigen-presenting cells (APC) function and reduce the expression of major histocompatibility complex (MHC) class II.[3]
- Chemotherapy and radiation therapy: High-dose chemotherapy causes local tissue damage and increases circulating cytokine levels, leading to a cytokine storm; this increases the ability of immune cells in the graft to recognize host antigens. Regimens, including total body irradiation, are associated with increased incidence and severity of GVHD compared to chemotherapy alone.[4]
Epidemiology
Acute GVHD can occur in up to 50% of patients receiving hematopoietic stem cell transplantation from an HLA-matched sibling.[5][6] The occurrence is typically higher in unmatched donors. The incidence of chronic GVHD ranges from 6% to 80%.[7] GVHD is considered one of the main causes of morbidity and mortality after hematopoietic stem cell transplantation; more than 10% of patients will die from this complication.[8]
Risk factors for acute GVHD include higher degrees of HLA mismatch, prior acute GVHD sex disparity, older age of the donor or recipient, peripheral stem cell recipients, alloimmunization of the donor, cytomegalovirus and Epstein Barr virus seropositivity.[9] These factors collectively contribute to the increased risk of developing acute GVHD following hematopoietic stem cell transplantation.
Pathophysiology
The immune system's cells are trained early to differentiate between self and nonself cells. The ability to recognize nonself cells depends on the histocompatibility genes, which provide instructions for making a group of related proteins known as major histocompatibility complex (MHC) proteins or HLA.
The histocompatibility genes code for MHC class I proteins on all nucleated cells in the body, and MHC class II molecules are expressed only on APC. During transplantation, the donor tissue, usually obtained from a genetically different individual (an allograft), prompts immune cells in the graft to recognize the recipient's MHC proteins as nonself, triggering an immune response between the donor and the recipient.
Donor cytotoxic CD8 T-cells recognize host tissue as foreign and proliferate to cause severe organ damage (type IV cytotoxic T-cell hypersensitivity reaction). Donor allograft T-cells are the primary effector cells for GVHD, and its pathogenesis can be divided into 3 phases (see Image. GVHD Pathogenesis).
- Phase 1 (afferent phase): Radiation or chemotherapy before bone marrow transplantation damages recipient tissue, leading to increased levels of inflammatory cytokines and the expression of MHC antigens; this enhances the APC's ability to present alloantigens to the donor T-cells.
- Phase 2 (efferent phase): This phase is characterized by the interaction of donor T-cells with host APC, leading to their proliferating and differentiation into activated T cells, which release additional inflammatory cytokines.
- Phase 3 (effector phase): The third phase is characterized by migrating cytotoxic T lymphocytes and natural killer cells to target organs, causing tissue damage and leading to multiorgan failure.[10]
GVHD is a complication that can occur after a stem cell or bone marrow transplant, where the donor's immune cells attack the recipient's tissues; it is a complex process involving multiple cytokines and immune cells. Some critical cytokines involved in the etiopathogenesis of GVHD include:
- Interleukin-2 (IL-2) plays a crucial role in the activation and proliferation of T cells, central to the immune response involved in GVHD.
- Activated T-cells and macrophages produce tumor necrosis factor-alpha (TNF-α), promoting inflammation and tissue damage in GVHD.
- Interleukin-1 (IL-1), similar to TNF-α, is a proinflammatory cytokine produced by activated immune cells that contribute to tissue damage and inflammation.
- Interleukin-6 (IL-6) is another proinflammatory cytokine involved in the pathogenesis of GVHD. IL-6 promotes B-cell activation and differentiation, as well as inflammatory responses.
- Interleukin-12 (IL-12), produced by APC, stimulates the differentiation of naive T cells into Th1 cells, which are involved in cell-mediated immune responses associated with GVHD.
- Interleukin-17 (IL-17), mainly produced by Th17 cells, promotes inflammation and tissue damage in GVHD, particularly in the gut.
- Interferon-gamma (IFN-γ), secreted by activated T-cells, is involved in the inflammatory response and tissue damage characteristic of GVHD.
- Transforming growth factor-beta (TGF-β) can have both pro- and anti-inflammatory effects; however, it generally has immunosuppressive properties in GVHD, regulating T-cell differentiation and function.
These cytokines are among many not listed, and they interact in a complex network to drive the pathogenesis of GVHD, resulting in tissue damage and systemic inflammation. Therapeutic strategies for GVHD often target these cytokines to modulate the immune response and mitigate disease severity.[11][12]
Histopathology
In the gastrointestinal (GI) tract, apoptosis of epithelial cells is the most important feature. Dilated crypts, crypt destruction, villus atrophy, and neutrophilic infiltration can also be observed in small bowel specimens.[13] A liver biopsy typically shows dysmorphic small bile ducts with portal inflammation. Histopathological damage of the skin ranges from minimal vacuolization to separation of the dermis from the epidermis. Grades of skin GVHD are as follows (see Image. Grades of Skin Graft-Versus-Host Disease):
- Grade I: Minimal vacuolization in the epidermis
- Grade II: Vacuolization and dyskeratotic bodies
- Grade III: Subepidermal cleft formation
- Grade IV: Separation of the dermis from the epidermis [14]
History and Physical
Acute GVHD usually involves the skin, gastrointestinal (GI) tract, and liver; this condition occurs in 70%, 74%, and 44% of cases, respectively. GVHD can also affect the lungs, kidneys, eyes, and hematopoietic system and may decrease responsiveness to active immunization.
The most common skin manifestation is a pruritic or painful maculopapular rash that initially involves the neck's palms, soles, shoulders, and nape. This rash can spread diffusely and become confluent. In severe GVHD, bullous lesions resembling toxic epidermal necrolysis (TEN) can develop.
GI symptoms most commonly include diarrhea and abdominal pain, but mucositis, mucosal ulceration, nausea, and vomiting can also occur. Diarrhea is secretory and continues despite fasting. Initially watery, diarrhea may progress to become bloody, potentially requiring frequent blood transfusions and causing difficulty in maintaining adequate fluid balance.
Liver involvement usually presents together with either cutaneous or GI manifestations; it rarely occurs in isolation. Abnormal liver function tests are characteristic, typically showing elevated bilirubin and alkaline phosphatase levels. Coagulopathy and hyperammonemia are rare but can occur in severe forms. Hepatomegaly, as well as pale urine and stool, may be present.
Chronic GVHD shares many features with collagen vascular disorders and systemic sclerosis.[15] In the oral cavity, this condition may present as lichen planus with a risk of developing into oral squamous cell carcinoma, which differs from classical pathology and appears more aggressive in patients with stem cell transplantation.[16] Recurrent infections can be a cause of death, often complicating immunosuppression.[17][18] Ocular involvement indicates poor prognosis in GVHD, usually affecting the ocular surface and manifesting with dry eye or keratoconjunctivitis sicca.[19]
Evaluation
Diagnosis is usually clinical. Traditionally, the criteria as described by Billingham include the following:
- Immunologically competent cells must be present in the graft.
- The recipient should have transplantation alloantigens that appear foreign to the graft and can, therefore, stimulate it antigenically.
- The recipient should not be capable of mounting an effective immunologic reaction against the graft, or there must be enough time for the graft to manifest an immune response.[20]
All patients who undergo hematopoietic cell transplantation are at risk of GVHD, although it usually occurs during the first few months posttransplantation.[21] Skin and GI (usually rectal) biopsies can help confirm the diagnosis. The staging of the disease is based on the extent of symptoms and lab abnormalities.
The use of biomarkers for the diagnosis and prognosis estimation is an area of investigation. No biomarker is ready for clinical application yet.[22][23][24]
Treatment / Management
All patients receiving hematopoietic cell transplantation should undergo prophylactic treatment for GVHD. Treatment protocols differ by institution, but a combination of cyclosporine and MTX is usually continued for several months posttransplantation. Antibacterial, antiviral, and antifungal prophylaxis are typically added posttreatment to mitigate the risk of infections.
Treatment for GVHD depends on the severity of symptoms and the organs involved. Most treatment options focus on immunosuppression of donor T-cells, but they must be balanced to reduce the GVHD symptoms while avoiding decreasing the beneficial graft versus tumor (GVT) response. Corticosteroids remain the most commonly used treatment.
Grade 1 GVHD is usually managed with topical steroids to control local symptoms. Topical tacrolimus is an option for steroid-resistant disease. Grade 2 or higher GVHD requires the addition of systemic steroids, most commonly methylprednisolone 2 mg/kg/day in divided doses. In cases of GI involvement, adding a nonabsorbable corticosteroid (budesonide or beclomethasone) is more effective than systemic treatment alone. Steroids should be avoided if a GI infection is present.
Gradual tapering of the steroid over several months is essential to prevent a GVHD flare. Patients with chronic GVHD will typically require prolonged courses of steroids, generally 2 to 3 years, and some patients may require lifelong treatment. Octreotide can be added in an attempt to decrease the amount of diarrhea.
Other agents that can be added to steroids include mycophenolate, etanercept, pentostatin, monoclonal antibodies, sirolimus, alpha-1-antitrypsin, mesenchymal stromal cells, and extracorporeal photopheresis. However, their efficacy is unclear. Cyclosporine can be added to the treatment regimen for chronic GVHD in an attempt to decrease steroid dosage and duration. This agent is often used in combination with steroids to provide a more comprehensive immunosuppressive effect.
Differential Diagnosis
The differential diagnosis for GVHD depends on the clinical manifestations observed in the patient. These include the following:
- Skin: Drug reactions, viral exanthems, radiation dermatitis
- Hepatic: Infection, especially viral hepatitis, drug-induced liver injury, shock liver, immunotherapy-related hepatotoxicity, sinusoidal obstructive syndrome, malignancy [25]
- Gastrointestinal:
- Diarrhea: Iatrogenic (secondary to chemotherapy, immunosuppressants, antibiotics, or magnesium), infectious (CMV, EBV, adenovirus, rotavirus, Clostridium difficile, Mycobacterium avium complex, Giardia, Cryptosporidium), thrombotic microangiopathy, bile-salt malabsorption
- Nausea and vomiting, anorexia: Iatrogenic (secondary to chemotherapy, immunosuppressants, radiation, antibiotics, or opioids)[26]
Treatment Planning
GVHD occurs when transplanted donor cells recognize the recipient's tissues as foreign and attack them, leading to a range of symptoms affecting the skin, GI tract, liver, and other organs. Treatment typically involves a combination of medications and supportive care measures. An overview of common treatments is as follows:
Immunosuppressive medications are the cornerstone of GVHD treatment, suppressing the immune system to prevent it from attacking the recipient's tissues. Common immunosuppressants include:
- Corticosteroids: Prednisone and methylprednisolone are often used initially to reduce inflammation and suppress immune activity.
- Calcineurin inhibitors: Drugs like cyclosporine and tacrolimus are frequently used in combination with steroids to control GVHD.
- Other immunosuppressants: Mycophenolate mofetil, sirolimus, and azathioprine may also be used alone or in combination with other medications.
Antithymocyte globulin may be used to suppress the immune system in severe cases of GVHD, particularly in patients who do not respond to initial treatments. This medication targets T-cells, reducing their activity and helping to control GVHD symptoms.
Biological therapies can target specific components of the immune system involved in GVHD. Examples include:
- TNF inhibitors: Drugs like infliximab and etanercept may be used to treat severe GI GVHD.
- IL-2 receptor antibodies: Agents like basiliximab and daclizumab can help suppress the immune response in GVHD.
Photopheresis involves removing white blood cells from the patient's blood, treating them with a photosensitizing agent, exposing them to ultraviolet light, and returning them to the patient. This process can modulate the immune response and is often used in chronic GVHD cases.
Topical treatments may be used for skin involvement in GVHD. Topical corticosteroids, moisturizers, and other supportive measures may relieve symptoms and promote healing.
Supportive care includes managing symptoms and complications associated with GVHD, such as infections, nutritional deficiencies, and electrolyte imbalances.
Stem cell transplant modification (using stem cells from a different donor) may be considered to reduce the risk or severity of GVHD in future transplants.
Treatment decisions depend on various factors, including the severity of GVHD, the organs affected, the patient's overall health, and previous treatments. Close monitoring and collaboration between transplant specialists, oncologists, and other healthcare providers are essential for managing GVHD effectively.
Staging
The 2 most famous systems for acute GVHD staging are the International Cone Marrow Transplant Registry (IBMTR) system (A to D) and Glucksberg grade (1 to 4).[27][28] Staging is based on clinical manifestations and severity of organ involvement.[6]
Skin
- Stage 1: Maculopapular rash <25% of the body
- Stage 2: Maculopapular rash 25% to 50% of the body
- Stage 3: Generalized erythroderma
- Stage 4: Generalized erythroderma with bullae
Liver
- Stage 1: Bilirubin 2 to 3, AST 150 to 750
- Stage 2: Bilirubin 3 to 6
- Stage 3: Bilirubin 6 to 15
- Stage 4: Bilirubin >15
Gastrointestinal System
- Stage 1: Diarrhea >500 cc/day
- Stage 2: Diarrhea >1000 cc/day
- Stage 3: Diarrhea >1500 cc/day
- Stage 4: Diarrhea >2000 cc/day or severe abdominal pain
Glucksberg Grade:
- Mild: No liver or GI involvement, stage 1 to 2 skin involvement
- Moderate: Stage 1 liver or GI involvement, stage 1 to 3 skin involvement
- Severe: Stage 2 to 3 skin, liver, or GI involvement
- Life-threatening: stage 2 to 4 liver or GI involvement, stage 1 to 4 skin involvement [28]
International Cone Marrow Transplant Registry Severity Index:
- Mild: No liver or GI involvement, stage 1 skin involvement
- Moderate: Stage 1 to 2 liver or GI involvement, stage 2 skin involvement
- Severe: Stage 3 skin, liver, or GI involvement
- Life-threatening: Stage 4 skin, liver, or GI involvement [28]
Prognosis
Mortality is generally higher in moderate to severe GVHD compared to mild disease.[8][29] The 5-year survival rate for grade C is 25%, and 5% for grade 4.[30] There is a strong correlation between the response to first-line treatment and survival.[6] Extensive skin involvement, diarrhea, thrombocytopenia, elevated liver enzymes, and lung or liver involvement are poor prognostic factors for acute or chronic GVHD.[1][31] Early recognition and aggressive management of these factors are crucial for improving patient outcomes.
Complications
GVHD is a complication of allogeneic hematopoietic stem cell transplant that can lead to other complications, including bronchiolitis obliterans syndrome, interstitial lung disease, obliterative bronchiolitis, organizing pneumonia, and pleuroparenchymal fibroelastosis.[32] These additional complications further contribute to morbidity and mortality in transplant recipients.
Reported complications include GI involvement, resulting in fibrosis, motility abnormalities, and malabsorption. Lung problems may cause bronchiectasis, while infections are common and can be fatal. Liver complications include endothelialitis, bile duct destruction, and pericholangitis, but a liver biopsy is not routinely performed due to associated thrombocytopenia.[5] Instead, liver function tests and imaging studies are often used to assess liver involvement in GVHD.
Consultations
Nutritionists should evaluate patients with GI involvement due to a higher risk of malnutrition and abnormalities in zinc, magnesium, vitamin B12, and vitamin D.[33] Nutritional support and supplementation are often necessary to address these deficiencies and optimize patient outcomes.
Deterrence and Patient Education
Along with timely, appropriate treatment and prophylactic measures, patients can receive counseling and education about remedial measures to improve the management of GVHD.
- Skincare: The use of moisturizer, application of sunscreen lotion with an appropriate sun protection factor, avoidance of scratching on the sutured area or other regions, and wearing long sleeves and pants to protect the skin are emphasized.
- Mouth care: Dental hygiene with topical fluorides is suggested.[34]
- Diet: Avoiding substances that can cause loose stools, such as spicy food, is important. Patients should be cautious of the foods they choose to ingest.
- Hygiene: Avoiding infective sources, wearing a face and nose mask when going out, and keeping the hands and feet clean are essential for minimizing the risk of infections.
All patients and caregivers should receive vaccines against influenza and pneumococcus to reduce the risk of infection.[5] These vaccines are crucial for protecting against serious respiratory illnesses.
Pearls and Other Issues
Key facts to keep in mind about GVHD include the following:
- GVHD is when donor immune cells attack the recipient's tissues, often occurring after an allogeneic hematopoietic stem cell transplant.
- The typical clinical manifestations of acute and chronic GVHD include skin rash, GI symptoms (such as diarrhea and abdominal pain), liver dysfunction, and involvement of other organs like the lungs.
- Staging and grading systems used for GVHD include the IBMTR system and Glucksberg grade.
- Diagnostic criteria for GVHD are primarily through clinical assessment.
- The principles of GVHD treatment include immunosuppressive medications, such as corticosteroids and calcineurin inhibitors, and agents, such as mycophenolate mofetil and sirolimus.
- Complications of GVHD are infections, hepatic dysfunction, GI complications, and pulmonary complications like bronchiolitis obliterans syndrome.
- The prognosis of GVHD varies based on severity and response to treatment.
Enhancing Healthcare Team Outcomes
Enhancing healthcare team outcomes for patients with GVHD involves several vital strategies. First, promoting interdisciplinary collaboration among healthcare professionals, including transplant specialists, hematologists, primary care providers, nurses, nutritionists, and pharmacists, ensures comprehensive care and holistic management of GVHD. Regular communication and information sharing among team members are crucial to ensure continuity of care and prompt response to patient needs. Ongoing education and training for healthcare professionals involved in GVHD care keep them updated on the latest treatment guidelines and best practices.
Patient education is also essential. Educating patients and their families about GVHD, its symptoms, treatment options, and self-care strategies actively involve them in their care and promotes adherence to treatment plans. Care coordination strategies streamline care delivery, including scheduling appointments, coordinating treatments, and managing transitions between care settings. Establishing multidisciplinary clinics where patients receive integrated care from specialists in a single visit improves convenience and efficiency.
Additionally, facilitating support groups for patients with GVHD and their caregivers provides emotional support, allows for sharing experiences, and promotes learning of coping strategies from one another. Participation in clinical trials and research studies is encouraged to advance the understanding and treatment of GVHD, promoting innovation in care delivery. By implementing these strategies, healthcare teams can optimize outcomes for patients with GVHD, improving quality of life and reducing the burden of this challenging condition.
Media
(Click Image to Enlarge)
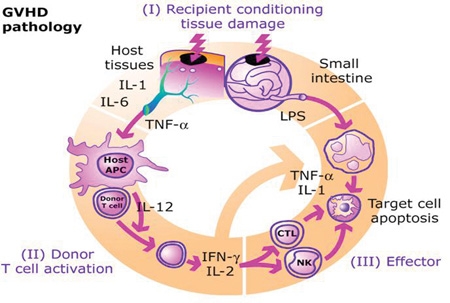
GVHD Pathogenesis
Reddy P, Ferrara JLM. Mouse models of graft-versus-host disease. Stembook Web site. https://www.stembook.org/node/54. Published February 28, 2009. Accessed March 12, 2024.
(Click Image to Enlarge)
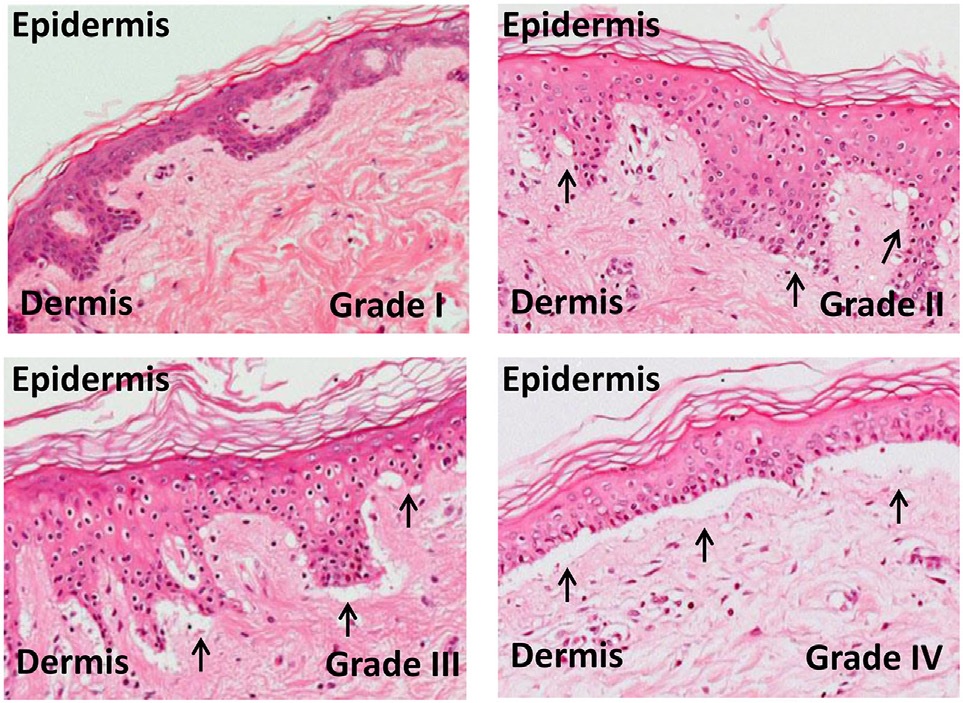
Grades of Skin Graft-Versus-Host Disease
Ghimire S, Weber D, Mavin E, Wang XN, Dickinson AM, Ernst Holler E. Pathophysiology of GvHD and other HSCT-related major complications. Front Immunol. 2017;8:79. doi: 10.3389/fimmu.2017.00079.
References
Socié G, Ritz J. Current issues in chronic graft-versus-host disease. Blood. 2014 Jul 17:124(3):374-84. doi: 10.1182/blood-2014-01-514752. Epub 2014 Jun 9 [PubMed PMID: 24914139]
Antin JH, Kim HT, Cutler C, Ho VT, Lee SJ, Miklos DB, Hochberg EP, Wu CJ, Alyea EP, Soiffer RJ. Sirolimus, tacrolimus, and low-dose methotrexate for graft-versus-host disease prophylaxis in mismatched related donor or unrelated donor transplantation. Blood. 2003 Sep 1:102(5):1601-5 [PubMed PMID: 12730113]
Shimabukuro-Vornhagen A, Liebig T, von Bergwelt-Baildon M. Statins inhibit human APC function: implications for the treatment of GVHD. Blood. 2008 Aug 15:112(4):1544-5. doi: 10.1182/blood-2008-04-149609. Epub [PubMed PMID: 18684883]
Level 3 (low-level) evidenceMielcarek M, Martin PJ, Leisenring W, Flowers ME, Maloney DG, Sandmaier BM, Maris MB, Storb R. Graft-versus-host disease after nonmyeloablative versus conventional hematopoietic stem cell transplantation. Blood. 2003 Jul 15:102(2):756-62 [PubMed PMID: 12663454]
Level 2 (mid-level) evidenceFerrara JL, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet (London, England). 2009 May 2:373(9674):1550-61. doi: 10.1016/S0140-6736(09)60237-3. Epub 2009 Mar 11 [PubMed PMID: 19282026]
Jamil MO, Mineishi S. State-of-the-art acute and chronic GVHD treatment. International journal of hematology. 2015 May:101(5):452-66. doi: 10.1007/s12185-015-1785-1. Epub 2015 Apr 12 [PubMed PMID: 25864189]
Atkinson K, Horowitz MM, Gale RP, van Bekkum DW, Gluckman E, Good RA, Jacobsen N, Kolb HJ, Rimm AA, Ringdén O. Risk factors for chronic graft-versus-host disease after HLA-identical sibling bone marrow transplantation. Blood. 1990 Jun 15:75(12):2459-64 [PubMed PMID: 2350582]
MacMillan ML, Robin M, Harris AC, DeFor TE, Martin PJ, Alousi A, Ho VT, Bolaños-Meade J, Ferrara JL, Jones R, Arora M, Blazar BR, Holtan SG, Jacobsohn D, Pasquini M, Socie G, Antin JH, Levine JE, Weisdorf DJ. A refined risk score for acute graft-versus-host disease that predicts response to initial therapy, survival, and transplant-related mortality. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2015 Apr:21(4):761-7. doi: 10.1016/j.bbmt.2015.01.001. Epub 2015 Jan 10 [PubMed PMID: 25585275]
Gale RP, Bortin MM, van Bekkum DW, Biggs JC, Dicke KA, Gluckman E, Good RA, Hoffmann RG, Kay HE, Kersey JH. Risk factors for acute graft-versus-host disease. British journal of haematology. 1987 Dec:67(4):397-406 [PubMed PMID: 3322360]
Nassereddine S, Rafei H, Elbahesh E, Tabbara I. Acute Graft Versus Host Disease: A Comprehensive Review. Anticancer research. 2017 Apr:37(4):1547-1555 [PubMed PMID: 28373413]
Level 3 (low-level) evidenceElhage A, Sligar C, Cuthbertson P, Watson D, Sluyter R. Insights into mechanisms of graft-versus-host disease through humanised mouse models. Bioscience reports. 2022 Sep 30:42(9):. doi: 10.1042/BSR20211986. Epub [PubMed PMID: 35993192]
Várady G, Cserepes J, Németh A, Szabó E, Sarkadi B. Cell surface membrane proteins as personalized biomarkers: where we stand and where we are headed. Biomarkers in medicine. 2013 Oct:7(5):803-19. doi: 10.2217/bmm.13.90. Epub [PubMed PMID: 24044572]
Salomao M, Dorritie K, Mapara MY, Sepulveda A. Histopathology of Graft-vs-Host Disease of Gastrointestinal Tract and Liver: An Update. American journal of clinical pathology. 2016 May:145(5):591-603. doi: 10.1093/ajcp/aqw050. Epub [PubMed PMID: 27247365]
Ghimire S, Weber D, Mavin E, Wang XN, Dickinson AM, Holler E. Pathophysiology of GvHD and Other HSCT-Related Major Complications. Frontiers in immunology. 2017:8():79. doi: 10.3389/fimmu.2017.00079. Epub 2017 Mar 20 [PubMed PMID: 28373870]
Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host disease. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2003 Apr:9(4):215-33 [PubMed PMID: 12720215]
Elad S, Zadik Y, Zeevi I, Miyazaki A, de Figueiredo MA, Or R. Oral cancer in patients after hematopoietic stem-cell transplantation: long-term follow-up suggests an increased risk for recurrence. Transplantation. 2010 Dec 15:90(11):1243-4. doi: 10.1097/TP.0b013e3181f9caaa. Epub [PubMed PMID: 21119507]
Level 3 (low-level) evidenceGálvez K, Muñoz P, Vera V, Arce C. Vitiligo type cutaneous manifestation of chronic graft-versus-host disease. Case report. Revista chilena de pediatria. 2018 Feb:89(1):113-117. doi: 10.4067/S0370-41062018000100113. Epub [PubMed PMID: 29664513]
Level 3 (low-level) evidenceGandelman JS, Zic J, Dewan AK, Lee SJ, Flowers M, Cutler C, Pidala J, Chen H, Jagasia MH, Tkaczyk ER. The Anatomic Distribution of Skin Involvement in Patients with Incident Chronic Graft-versus-Host Disease. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2019 Feb:25(2):279-286. doi: 10.1016/j.bbmt.2018.09.007. Epub 2018 Sep 13 [PubMed PMID: 30219700]
Munir SZ, Aylward J. A Review of Ocular Graft-Versus-Host Disease. Optometry and vision science : official publication of the American Academy of Optometry. 2017 May:94(5):545-555. doi: 10.1097/OPX.0000000000001071. Epub [PubMed PMID: 28422804]
Billingham RE. The biology of graft-versus-host reactions. Harvey lectures. 1966-1967:62():21-78 [PubMed PMID: 4875305]
Level 3 (low-level) evidenceFiroz BF, Lee SJ, Nghiem P, Qureshi AA. Role of skin biopsy to confirm suspected acute graft-vs-host disease: results of decision analysis. Archives of dermatology. 2006 Feb:142(2):175-82 [PubMed PMID: 16490845]
Vander Lugt MT, Braun TM, Hanash S, Ritz J, Ho VT, Antin JH, Zhang Q, Wong CH, Wang H, Chin A, Gomez A, Harris AC, Levine JE, Choi SW, Couriel D, Reddy P, Ferrara JL, Paczesny S. ST2 as a marker for risk of therapy-resistant graft-versus-host disease and death. The New England journal of medicine. 2013 Aug 8:369(6):529-39. doi: 10.1056/NEJMoa1213299. Epub [PubMed PMID: 23924003]
Ferrara JL, Harris AC, Greenson JK, Braun TM, Holler E, Teshima T, Levine JE, Choi SW, Huber E, Landfried K, Akashi K, Vander Lugt M, Reddy P, Chin A, Zhang Q, Hanash S, Paczesny S. Regenerating islet-derived 3-alpha is a biomarker of gastrointestinal graft-versus-host disease. Blood. 2011 Dec 15:118(25):6702-8. doi: 10.1182/blood-2011-08-375006. Epub 2011 Oct 6 [PubMed PMID: 21979939]
Korngold R, Marini JC, de Baca ME, Murphy GF, Giles-Komar J. Role of tumor necrosis factor-alpha in graft-versus-host disease and graft-versus-leukemia responses. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2003 May:9(5):292-303 [PubMed PMID: 12766879]
Level 3 (low-level) evidenceMatsukuma KE, Wei D, Sun K, Ramsamooj R, Chen M. Diagnosis and differential diagnosis of hepatic graft versus host disease (GVHD). Journal of gastrointestinal oncology. 2016 Apr:7(Suppl 1):S21-31. doi: 10.3978/j.issn.2078-6891.2015.036. Epub [PubMed PMID: 27034810]
Naymagon S, Naymagon L, Wong SY, Ko HM, Renteria A, Levine J, Colombel JF, Ferrara J. Acute graft-versus-host disease of the gut: considerations for the gastroenterologist. Nature reviews. Gastroenterology & hepatology. 2017 Dec:14(12):711-726. doi: 10.1038/nrgastro.2017.126. Epub 2017 Sep 27 [PubMed PMID: 28951581]
Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA, Lerner KG, Thomas ED. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974 Oct:18(4):295-304 [PubMed PMID: 4153799]
Rowlings PA, Przepiorka D, Klein JP, Gale RP, Passweg JR, Henslee-Downey PJ, Cahn JY, Calderwood S, Gratwohl A, Socié G, Abecasis MM, Sobocinski KA, Zhang MJ, Horowitz MM. IBMTR Severity Index for grading acute graft-versus-host disease: retrospective comparison with Glucksberg grade. British journal of haematology. 1997 Jun:97(4):855-64 [PubMed PMID: 9217189]
Level 2 (mid-level) evidenceCho C, Hsu M, Barba P, Maloy MA, Avecilla ST, Barker JN, Castro-Malaspina H, Giralt SA, Jakubowski AA, Koehne G, Meagher RC, O'Reilly RJ, Papadopoulos EB, Ponce DM, Tamari R, van den Brink MRM, Young JW, Devlin SM, Perales MA. Long-term prognosis for 1-year relapse-free survivors of CD34+ cell-selected allogeneic hematopoietic stem cell transplantation: a landmark analysis. Bone marrow transplantation. 2017 Dec:52(12):1629-1636. doi: 10.1038/bmt.2017.197. Epub 2017 Oct 9 [PubMed PMID: 28991247]
Cahn JY, Klein JP, Lee SJ, Milpied N, Blaise D, Antin JH, Leblond V, Ifrah N, Jouet JP, Loberiza F, Ringden O, Barrett AJ, Horowitz MM, Socié G, Société Française de Greffe de Moëlle et Thérapie Cellulaire, Dana Farber Cancer Institute, International Bone Marrow Transplant Registry. Prospective evaluation of 2 acute graft-versus-host (GVHD) grading systems: a joint Société Française de Greffe de Moëlle et Thérapie Cellulaire (SFGM-TC), Dana Farber Cancer Institute (DFCI), and International Bone Marrow Transplant Registry (IBMTR) prospective study. Blood. 2005 Aug 15:106(4):1495-500 [PubMed PMID: 15878974]
Müller JA, Zirafi O, Roan NR, Lee SJ, Münch J. Evaluation of EPI-X4 as a urinary peptide biomarker for diagnosis and prognosis of late acute GvHD. Bone marrow transplantation. 2016 Aug:51(8):1137-9. doi: 10.1038/bmt.2016.65. Epub 2016 Apr 4 [PubMed PMID: 27042833]
Bergeron A, Cheng GS. Bronchiolitis Obliterans Syndrome and Other Late Pulmonary Complications After Allogeneic Hematopoietic Stem Cell Transplantation. Clinics in chest medicine. 2017 Dec:38(4):607-621. doi: 10.1016/j.ccm.2017.07.003. Epub 2017 Sep 19 [PubMed PMID: 29128013]
van der Meij BS, de Graaf P, Wierdsma NJ, Langius JA, Janssen JJ, van Leeuwen PA, Visser OJ. Nutritional support in patients with GVHD of the digestive tract: state of the art. Bone marrow transplantation. 2013 Apr:48(4):474-82. doi: 10.1038/bmt.2012.124. Epub 2012 Jul 9 [PubMed PMID: 22773121]
Mays JW, Fassil H, Edwards DA, Pavletic SZ, Bassim CW. Oral chronic graft-versus-host disease: current pathogenesis, therapy, and research. Oral diseases. 2013 May:19(4):327-46. doi: 10.1111/odi.12028. Epub 2012 Oct 28 [PubMed PMID: 23107104]