Introduction
Glaucoma is a collection of diseases where increased intraocular pressure (IOP) adversely impacts the optic nerve and, subsequently, the visual field.[1] However, not all cases of glaucoma are associated with increased IOP. A subset includes similar optic nerve and visual field damage, known as normal pressure glaucoma.[2] The collection of glaucomatous diseases is subdivided into open-angle and closed-angle glaucoma, both of which can have primary or secondary causes and can be of an iatrogenic or non-iatrogenic origin (see Image. Classification of Open-Angle Glaucoma).
Open-angle glaucoma (OAG) is a chronic, progressive, and irreversible multifactorial optic neuropathy characterized by an open angle of the anterior chamber, typical optic nerve head changes, retinal nerve fiber layer thinning, and progressive loss of peripheral vision (see Image. Visual Field and Optical Coherence Tomography, OCT). Central visual field loss and blindness can occur in the advanced stages of glaucoma. IOP is an important risk factor and the target for therapy when treating patients.[3]
The disease is usually bilateral, but asymmetry depends on the etiology. Although increased IOP is a significant risk factor in developing glaucoma, IOP levels greater than 21 mm Hg do not necessarily cause glaucoma and optic nerve damage in all patients.[4] Studies have shown asymptomatic individuals with ocular hypertension who maintain normal visual fields and healthy optic nerves.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Understanding the formation and drainage of aqueous humor is necessary to comprehend the etiology of OAG. The ciliary body continuously produces aqueous humor in the posterior chamber and drains it into the eye's anterior chamber. Most aqueous humor drainage occurs through the trabecular meshwork, and a minority of aqueous outflow is drained through the uveoscleral pathway.
Primary open-angle glaucoma (POAG) is the most common type, characterized by increased resistance to drainage in the trabecular meshwork. However, the drainage angle between the cornea and iris remains open.[6] Due to this blockage, the pressure in the eye gradually increases, resulting in optic nerve damage and progressive visual loss. Secondary OAG can have multiple etiologies but is far less common than POAG.
Genetic
Chromosome 1q24.3, MYOC gene: Myocilin is a cytoskeletal protein product of the MYOC gene, implicated in cases of hereditary juvenile OAG and adult OAG. Myocilin is a cytoskeletal protein expressed in the trabecular meshwork and is also known as trabecular meshwork glucocorticoid-inducible response protein.[7]
Chromosome 5q22.1, WDR36 gene: The WDR36 protein is a member of the WD repeat protein family and is implicated in adult-onset POAG. This protein functions in ribosomal ribonucleic acid processing, p53 stress-pathway response, cell cycle progression, signal transduction, apoptosis, and gene regulation. WDR36 protein is expressed in the lens, iris, sclera, ciliary muscles, ciliary body, trabecular meshwork, retina, and optic nerve in the eye. The protein is also expressed outside the eye in the human heart, placenta, liver, skeletal muscle, kidney, and pancreas. Four mutations in WDR36 at the GLC1G locus (N355S, A449T, R529Q, and D658G) have been identified, with a study implicating the gene in approximately 6% of patients with POAG. However, results from a recent 2017 Chinese study repudiated this claim by showing that the association between WDR36 and POAG is inconsistent across populations and calls for more data supporting the WDR36 protein's role in POAG.[8][9]
Chromosome 7q31, CAV1/CAV2 genes: CAV1 and CAV2 are protein members of the caveolin family that are involved in the formation of caveolae-invaginations of the plasma membrane in areas that are rich in cholesterol during transcytosis. This gene is associated with POAG susceptibility in populations of European and East Asian ancestry. CAV1 and CAV2 are expressed in most human cell types, including tissues such as the scleral spur cells, trabecular meshwork, and retinal ganglion cells. In vitro studies of CAV1 showed consistent upregulation in the trabecular meshwork after one hour of increased IOP.[10][11]
Chromosome 9p21, CDKN2B-AS1 gene: CDKN2B-AS1 is a cyclin-dependent kinase inhibitor 2B antisense noncoding ribonucleic acid that regulates cyclin-dependent kinase inhibitor 2A and 2B in the cell cycle.[12] A United States-based observational case study found that this region modifies optic nerve vulnerability to glaucomatous change. Single nucleotide polymorphism (SNP) in this gene is thought to be implicated in POAG by causing RGCs to undergo apoptosis during their quiescent post-mitotic state.[13][14]
Chromosome 10p13, OPTN gene: Optineurin is the coiled-coil protein product implicated in adult-onset POAG and normal-tension glaucoma. Optineurin is involved in various cellular functions, including apoptosis, cellular morphogenesis, inflammation, vasoconstriction, membrane protein trafficking, vesicular trafficking, and transcription activation.[15]
Chromosome 15q24.1, LOXL1 gene: Lysyl oxidase-like 1 gene codes for an extracellular copper-dependent amine oxidase enzyme that catalyzes the first step in crosslinking collagen and elastin in the extracellular matrix and is implicated in cases of pseudoexfoliation syndrome. SNP in the LOXL1 gene is associated with excessive levels of crosslinked amyloid-like fibrillar glycoproteins that deposit in the anterior segment and are more common in Scandinavian populations.[16][17] SNPs in the LOXL1 gene can present as exfoliation glaucoma as the first signs of a more systemic severe condition that implicates multiple tissues with the expression of this enzyme, including the liver, kidney, and gallbladder.[18][19]
Several study results (based on whole-exome sequencing using gene-based and single-variant analyses) have revealed more than 40 new previously unreported genes associated with glaucoma phenotypes.[20] Understanding this disease's genetic and molecular mechanisms is crucial to developing new drug targets.[21][22]
Epidemiology
Glaucoma affects about 70 million people worldwide and is the second leading cause of blindness globally. Of the 70 million individuals affected by glaucoma, 74% have OAG; in the United States (US), nearly 80% of all glaucoma is OAG. A recent meta-analysis showed that the estimated number of individuals with POAG worldwide is about 68.56 million, with more than 50% from Africa and Asia.[23] Nearly 10% of all patients with glaucoma are blind bilaterally; bilateral blindness due to OAG has been estimated to affect 5.9 million people in 2020. At least 2.7 million people ≥40 years are diagnosed with glaucoma in the US, and the number of patients with all forms of glaucoma worldwide is projected to rise. The highest prevalence of OAG is found in African-American populations. Glaucoma is the leading cause of blindness in African Americans, with prevalence in Latin American and Chinese individuals approaching in older patient populations. Women are disproportionately affected by all forms of glaucoma, comprising approximately 55.4% of all cases of OAG.
Longevity also plays a role because glaucoma primarily affects older populations. The longevity factor should be considered in the epidemiology of glaucoma, as women and individuals in developed countries have greater longevity than men and individuals in non-developed countries. In 2020, OAG was projected to have the highest prevalence rate in Europe, followed by China and India.[24][25]
Risk Factors:
- Older age (African American, 40+ years; Caucasians, 65+ years) [26]
- Race (African-American, Afro-Caribbean, and West African patients have a 4-fold increased risk of developing OAG)[26]
- Family history (eg, the Rotterdam Eye study found a 9.2 times higher risk of developing OAG if first-degree relatives had glaucoma)[27]
- Elevated IOP [28]
- Myopia (eg, results from studies have reported an increased risk of glaucoma of up to 20% for each diopter increase in myopia) [29]
- Increased cup-to-disc ratio [30]
- Disc hemorrhage [31]
- Thin central corneal thickness [32]
- Low ocular perfusion pressure [33]
- Low blood pressure (systolic and diastolic)[34]
- High blood pressure (systemic arterial hypertension has been associated with but is not a confirmed risk factor for OAG)[35]
- Type 2 diabetes mellitus [36]
- High pattern standard deviation on visual fields [37]
- Migraine or vasospasm [38]
- Low intracranial (cerebral spinal fluid) pressure [39]
- Oral contraceptive pill [40]
- Lifestyle risk factors include smoking, obesity, alcohol, anxiety, stress, and sleep apnea [41]
Pathophysiology
Retinal Ganglion Cells
The exact cause of glaucoma is not fully known, but the underlying pathology lies in the apoptosis of retinal ganglion cells.[7] Retinal ganglion cells (RGC) are the third class of photoreceptors recently noted in scientific literature for their intrinsic photosensitivity. RGCs form functional microcircuits with rods, cones, amacrine cells, and bipolar cells that help transmit image-forming and non-image-forming information to the brain. RGC axons target the suprachiasmatic nucleus, intergeniculate leaflet, olivary pretectal nucleus, ventral division of the lateral geniculate nucleus, and the preoptic area.
RGCs play a role in modulating circadian rhythm, releasing melatonin, regulating pupil size, and forming relays in on-off retina centers.[42] RGC axons remain unmyelinated until they have passed through the lamina cribrosa and converged to form the optic nerve.
After passing through the lamina cribrosa, oligodendrocytes myelinate the axons of the RGCs. Iatrogenically induced ocular hypertension in mice, cats, and monkeys has shown blockade of orthograde and retrograde axonal transport, integral in transporting growth factors such as brain-derived neurotrophic factors. Regardless of whether IOP is elevated, normal, or decreased, the death of RGCs underlies glaucoma pathology.[43][44]
Lamina Cribrosa
The lamina cribrosa is a sieve-like fenestration at the back of the sclera that allows for a conglomeration of retinal axons and blood vessels to exit the posterior of the eye. Changes in the three-dimensional structure of the lamina cribrosa have been implicated in the pathogenesis of glaucomatous optic atrophy.[45] The superior and inferior channels of the lamina cribrosa contain larger pores and thinner connective tissue support for the passage of nerve-fiber bundles than the nasal and temporal parts of the lamina. The most common pattern of glaucomatous optic nerve thinning occurs at the inferior and superior portions of the optic nerve. Also, the superior and inferior laminar zones of the lamina cribrosa are where the arcuate area ganglion cell axons travel, and these axons are the most susceptible to glaucomatous damage.
Mechanical damage to axons and the prevention of essential trophic factors, such as the brain-derived neurotrophic factor, being appropriately delivered is conducive to the disease process. Results from studies show that statistically significant depth variability exists among the superior and inferior lamina cribrosa of healthy patients and those with OAG. Patients with OAG have greater depth at the optic cup floor, possibly due to increased IOP pressure. One study examined the lamina cribrosa using Heidelberg retina tomograph and found greater topographic variability and "spikiness" when looking at the lamina cribrosa of patients with OAG; this is most likely a sign of fragility in the lamina, as increased spikiness is inversely related to Humphrey mean deviation (P < 0.05), and cup-disc ratio (P < 0.004) and was directly related to nerve fiber layer thickness (P < 0.005).[46][47]
Elevated Intraocular Pressure
High IOP is an important risk factor for glaucoma progression. Elevated IOP is the most studied and modifiable risk factor that causes OAG. When IOP rises above 21 mm Hg, a significant risk of developing visual field loss exists (with only small increases in IOP), especially if IOP rises above 26 mm Hg to 30 mm Hg. The high fluctuation of IOP may also lead to glaucoma progression. Reduction of IOP leads to less progression or stabilization of the glaucomatous optic nerve and visual field changes. About 40% to 50% of all OAG cases have IOP below 22 mm Hg in a single screening.[35][48]
Aqueous Outflow
The 2 main proposed mechanisms by which an elevated IOP is thought to contribute to glaucomatous damage include vascular dysfunction resulting in ischemia to the optic nerve [49] and mechanical dysfunction due to compression of the axons.[50] When OAG in a patient is attributed to elevated IOP, the cause of this increase in IOP is commonly thought to occur due to dysfunction in aqueous outflow through the trabecular meshwork of the eye.[51] This may occur as a result of partial obstruction due to foreign material (eg, accumulated mucopolysaccharides in the trabecular meshwork), a reduction in the number of trabecular endothelial cells, a decreased density of trabecular pores, number of vacuoles, or size of the inner wall endothelium of the canal of Schlemm, loss of phagocytic activity, or dysfunction in the neurological feedback loop involved in drainage of aqueous humor.
Other proposed mechanisms for obstruction of aqueous humor outflow include oxidative damage to the meshwork, abnormal corticosteroid metabolism, adrenergic dysfunction, or an immunological process. Unlike angle-closure glaucoma, the drainage angle between the iris and cornea remains open in OAG. Specific individuals may have a genetic predisposition [52] to cell death of individual axons in the eye, resulting in the release of potentially cytotoxic substances such as glutamate, calcium, nitric oxide, and free radicals, as well as the apoptosis of neighboring cells.
Histopathology
Early in the disease process, glaucomatous optic nerve atrophy can present with thinning and atrophy of the retinal ganglion cell layer and, thus, thinning of the nerve fiber layer above the ganglion cells.[53] The nerve fiber layer consists of the unmyelinated ganglion cell axons, which shrink concomitantly.[54] In more advanced glaucomatous optic nerve atrophy, cupping of the optic nerve and atrophy of the ganglion cell and nerve fiber layers is prevalent. As the ganglion cells deteriorate, the structural integrity of the nerve is compromised. Increased IOP can push into the optic nerve and cause the visible phenomenon of cupping. Retinal ganglion cell loss also leads to increased space and widening of the subdural optic nerve space (see Image. Glaucomatous Optic Nerve Head With Inferotemporal Retinal Nerve Fiber Layer Defect).[55]
Toxicokinetics
In OAG, particulate matter can lodge into the fine openings in the trabecular meshwork (TM) and increase the passive resistance to aqueous humor drainage. Different substances can disrupt the flow of aqueous across the TM, which include:
- Lens proteins: During cataract surgery, high-molecular-weight lens proteins produced by phacolysis can lodge into the trabecular meshwork and increase drainage resistance.[56][57]
- Red blood cells: In the event of a traumatic injury to the eye, senescent red blood cells are lodged in the trabecular meshwork, a variant of OAG known as "Ghost cell glaucoma."[58]
- Pigment granules: Pigment from the epithelium of the iris can detach and become lodged in the fine trabecular meshwork, as seen in pigmentary glaucoma [59] and pigment dispersion syndrome.[56][60]
- Pseudoexfoliation syndrome: Deposits of white dandruff-like material on the anterior lens surface, iris, and anterior chamber structures.[61]
- Tumor debris: Necrotic tumor debris from necrotic tumors can also clog the trabecular meshwork in a variant known as melanomalytic glaucoma.[62]
- Corticosteroids: Steroid therapy of any kind can contribute to elevated IOP; however, topical eye and periocular steroids are most likely to increase IOP.[26][63]
History and Physical
OAG is often asymptomatic in its early stages; a thorough history and eye exam are instrumental in detecting the disease early (see Image. Glaucoma Field Changes in Left Eye).[64] Early changes in OAG involve a loss of peripheral vision that the patient is usually unaware of until 40% of their nerve fibers are compromised; only then do they start to notice having “tunnel vision.” Visual field defects typically occur after asymptomatic retinal nerve fiber layer thinning and optic nerve cupping (see Image. A Cup-to-Disk Ratio of .75 of the Optic Nerve). Patients do not avert glaucomatous signs and symptoms, unlike maculopathies and cataracts that lead to decreased visual acuity.
Older patients might give clues about their history of losing peripheral vision by admitting to difficulties driving or running into objects around the home more frequently. Primary care patients with the above risk factors should undergo direct ophthalmoscopy to visualize the optic disc.[65] Visualization of the optic disc can provide reliable diagnostic information as it shows changes before the visual field deficits are symptomatic. OAG is often bilateral, and the 2 optic discs can be compared to one another as a useful metric, but the damage can also be asymmetric.
Primary care clinicians should refer patients to an ophthalmologist in the presence of the following risk factors, clinical findings, or symptoms that are suggestive of glaucoma:
- A previous ocular history, such as the history of eye pain or redness, headaches, uveitis, diabetic retinopathy, cataracts, vascular occlusions, or multicolored halos
- African-American race
- Refractive error
- Chronic use of topical or systemic corticosteroids
- Ocular surgery like photocoagulation or refractive procedures, cataract surgery, glaucoma surgery, and systemic surgery/ medications
- Head or ocular trauma
- Certain medications, such as hypertensive medications that may influence IOP or systemic/topical steroids
- Medical history of diabetes mellitus, migraine headaches, hypertension, vasospasm, cardiovascular disease, breathlessness, cardiac arrhythmia
- Family history (eg, first-degree relative with glaucoma, especially significant if this is a sibling) that would place them at a greater risk of developing OAG
- Old medical documentation of IOP, optic disc, visual field, and others
Evaluation
OAG can be clinically evaluated using a variety of diagnostic tools, but the following triad is the cornerstone of diagnosis:
- Optic disc or retinal nerve fiber layer changes
- Visual field changes
- Elevated IOP [66]
Optic Nerve
The optic nerve should be evaluated using a slit lamp and 90D or 78D lens so that the three-dimensional features of the optic nerve are appreciated. The inferior neuroretinal rim (NRR) is the thickest, followed by superior, nasal, and temporal NRR; this is called the ISNT rule.[67] In OAG, the superior and inferior NRR are thinned, breaking the ISNT rule. The optic cup should be determined by its contour and not color. A recent Journal of the Americal Medical Association Rational Clinical Examination systematic review of primary OAG diagnosis found that the risk of glaucoma was highest when an examination revealed an increased cup-disk ratio (CDR), CDR asymmetry, disc hemorrhage, or elevated IOP.[68]
Typical optic nerve head changes in OAG include:
- Diffuse or focal narrowing (notching/shelving) of the NRR precisely at the superior or inferior part of the optic disc
- Symmetrically enlarged cup-to-disc ratios greater than 0.5
- Increased vertical cup-to-disc ratio and thinning of NRR
- Asymmetry of CDR of 0.2 or more
- Hemorrhage at or around the optic disc
- Peripapillary atrophy
- Baring of circumlinear vessels (the gap between the superficial vessels and disc margin)
- Bayonetting of vessels (the vessel first goes back and then climbs along the wall of the deep cup and then angles again on the disc margin)
- Very deep (excavated) cup with bean-pot cupping and laminar dot sign
- Nasalization of optic disc vessels
- Diffuse or focal (arcuate) thinning/defect of the retinal nerve fiber layer contiguous with an area of NRR-notch
- The NRR is typically pink and not pale in OAG. The pallor of the NRR usually denotes an atrophic optic nerve, as seen in primary angle closure glaucoma.
Visual Field
- Perimetry, also known as visual field testing, is an important diagnostic tool that maps out the patient’s visual field on a printout, making it helpful and necessary in diagnosing and managing OAG. The testing provides a baseline visual field for glaucoma suspects and confirmed OAG cases so clinicians can track disease progression. To make a diagnosis of acquired glaucomatous visual field defect, Hoddap–Parrish–Anderson criteria are used:
- Glaucoma hemifield test outside normal limits on at least 2 fields.
- A cluster of 3 or more non-edge points in a location typical for glaucoma, all of which are depressed on the pattern deviation plot at a P <5% and one of which is depressed at a P <1% on 2 consecutive fields.
- A corrected pattern standard deviation that occurs in less than 5% of normal fields on 2 consecutive fields.[69]
Static automated threshold perimetry is used with white stimulus on a white background. Most studies used the Humphrey Field Analyzer, but other perimeters like Octopus have also been used successfully. Non-conventional perimetry like SWAP (short-wavelength automated perimetry using blue stimulus on yellow background),[70] pulsar perimetry,[71][72] rarebit,[73][74] Matrix,[75] and frequency-doubling technology [76] have been proposed in earlier studies for the detection of early glaucoma visual field loss, however, tend not to be used in routine clinical practice.
The visual field must be reliable, and defects should be repeatable on at least 2 fields. When treating patients long-term, it is preferable to use the same machine, the same degree of field, and protocol (eg, 24-2, 30-3, or 10-2) to compare the fields to note for progression or stability. At least 40% to 50% ganglion cell loss is needed to reliably show visual field defects in threshold perimetry.[77][78] Structural changes of the optic nerve and retinal nerve fiber layer (RNFL) tend to occur earlier than functional change (visual field loss) in most patients with OAG;
this is relevant to the concept of preperimetric glaucoma, which is defined as ‘the presence of characteristic glaucomatous changes in the optic disc and increased vulnerability to damage in the RNFL, without the presence of visual field defects detectable with standard automated perimetry.[79] For patients with risk factors, suspect optic discs, and/or ocular hypertension (OHT), periodic visual field and OCT testing are recommended to detect early visual field defects and changes to determine whether therapy is needed.
Typical visual field changes in OAG include:
- Increased variability of responses in an area that later developed field defects
- Asymmetry of the visual field between the eyes
- Paracentral scotoma- commonly superonasal
- Roenne’s nasal step- an area of depression above or below the horizontal meridian on the nasal side
- Temporal wedge
- Sickle-shaped (Seidel) scotoma
- Bjerrum scotoma or arcuate scotoma
- Annular or ring scotoma when arcuate scotoma is present on both above and below the horizontal meridian
- General constriction of peripheral field
- A temporal island of the visual field
Intraocular Pressure
IOP is measured with tonometry;[80] several different tonometers are used.[81] The gold standard remains to be Goldmann applanation tonometry.[82] When determining the IOP of a patient using tonometry, certain variables must be considered. Tonometry measurements can, for example, vary between examiners by approximately 10% per individual, translating to a difference in IOP measurement of 1 mm Hg to 2 mm Hg (see Image. Goldmann Applanation Tonometer [GAT] Procedure).[83]
An individual’s corneal thickness measured with pachymetry or diurnal variations of IOP (eg, higher IOP in early morning hours or other times of the day or variability in the time of day of maximal IOP between patients)[84] can also have a tremendous effect on the accuracy of IOP measurements. Study results have shown that IOP is overestimated in individuals with thick corneas while underestimated in those with thinner corneas.[85] Multiple measurements should be taken and correlated with optic nerve and visual field examinations when a patient is suspected of elevated IOP.
If previous tonometry measurements are available, they should be reviewed and compared to the most recent ones. Also, the IOP may be different on different days, and different instruments may capture different values of IOP. If a difference of 3 mm Hg or more is noted between the 2 eyes, there is an increased suspicion of glaucoma. Clinicians should expect approximately 10% variation between individual and repeat measurements over 2 to 3 occasions before deciding on the treatment.
Elevated IOP is an important and modifiable risk factor; however, it is not a diagnostic factor for OAG. An ophthalmologist should check the patient’s IOP using applanation tonometry, remaining aware that the applanation tonometry test causes patients to squeeze their eyes and elevate their pressure readings. Normal IOP should range between 12 mm Hg and 21 mm Hg. Approximately 75% of patients with elevated IOP never develop glaucomatous optic nerve atrophy or visual field deficits. When a patient has recorded a reliably high IOP reading above 21 mm Hg, they are deemed patients with glaucoma or patients with ocular hypertension.[35][86]
Gonioscopy
OAG is a diagnosis of exclusion, and other ocular emergencies, such as closed-angle glaucoma, must be ruled out.[87] Gonioscopy determines whether the diagnosis is considered “open” or “closed” angle glaucoma. Gonioscopy is an acquired skill that allows the ophthalmologist to visualize the angle between the cornea and iris and determine if it is open. The angle between the iris and cornea should be 20° to 45° to be considered “open” so that aqueous humor can circumvent the posterior chamber to the anterior chamber.[35]
Optical Coherence Tomography
Optical coherence tomography (OCT) is a diagnostic imaging modality that provides high-resolution cross-sectional imaging of the retina, optic nerve, and anterior segment. Low-coherence infrared light is directed toward the back of the eye, and the path of scattered photons helps recreate an image of the retina. OCT is highly reproducible and is widely used as an adjunct in routine glaucoma patient management. Peripapillary RNFL analysis (see Image. Normal Visual Field and Optical Coherence Tomography [OCT] Results) can show thinning in this layer. As the most commonly used scanning protocol for glaucoma diagnosis, it samples RGCs from the entire retina.[88] Some of the drawbacks included variability in ONH morphology from patient to patient. The macular thickness is proposed as a means of glaucoma detection, given that 50% of RGCs are found in the macula, and RGC bodies are thicker than their axons and potentially easier to detect.[89] RNFL, macular thickness measurements, and visual field results are key in managing cases.
Corneal Photokeratoscopy
Corneal photokeratoscopy, or corneal topography, is a potential biological marker to monitor patients with primary OAG. Preliminary results have shown a forward shift of the posterior and anterior corneal surfaces; this is correlated with more advanced stages of functional damage, indicating a link between corneal structural changes and the duration and intensity of elevated IOP. Further studies are needed to validate this marker in patients with POAG.[57]
Treatment / Management
The goal of OAG treatment is:
- Preventing the progression of optic nerve head changes
- Preventing deterioration of the visual field
The concept of target IOP was introduced to achieve this goal.[90] Below a certain upper limit of IOP, it is estimated that the visual field, the optic nerve head, and RNFL parameters will not deteriorate. This helps to maintain a patient’s quality of life.
Glaucoma Medications
Debate exists over the optimal time to initiate treatment of OAG, with some clinicians initiating treatment of IOP when it reaches above only 21 mm Hg and others reserving treatment either until evidence of optic nerve or RNFL damage or if the patient is at high risk of damage or progression of OAG.
Treatment should be initiated if signs of damage as a result of OAG are evident (eg, disc hemorrhage, nerve fiber layer defects, asymmetric cupping, vertical vocalization, or notching of the cup) or if symptoms of elevated IOP are present (eg, halos, blurred vision, pain, IOP consistently above 28 mm Hg to 30 mm Hg) due to the high risk of optic nerve damage in the setting of elevated IOP. Some clinicians begin a monocular trial with medications only in 1 eye to assess the chosen medications’ effectiveness and side effects before treating both eyes. However, different eyes might respond differently to the same drug, asymmetric IOP fluctuation may occur, and the drug may have a contralateral effect.
A target IOP should be set depending on the severity of structural and functional damage, baseline IOP, age, race, family history, corneal thickness, hysteresis, and other risk factors.[91] Follow-up should also be scheduled based on the level of success in IOP reduction between visits (eg, more frequent follow-up with slower progression in treatment response) and the severity of optic nerve damage or visual field loss. Treatment should be individualized, considering the risk factors, systemic complications of medication use, the patient’s life expectancy, medical history, concomitant conditions, and desire to comply with treatment. The target IOP should be revised based on the behavior of optic nerve head damage and visual function.
If IOP, visual field, or optic nerve inflammation worsens while the patient is on medical therapy, compliance to treatment must be checked.[92] Systemic factors, including diabetes, smoking, and nocturnal hypotension, should be controlled. The managing clinician should confirm with the patient which drops are used and how many times the drops are applied daily. Closing eyelids after administration of drops with nasolacrimal duct occlusion may prevent systemic absorption of the topical medication.
Topical medications
Prostaglandin analogs: Reduces IOP 25% to 33% by increasing the uveoscleral outflow of the aqueous humor (AH).[93] The usual dose is daily. Side effects include lengthening of eyelashes, pigmentation of lids or iris, exacerbation of uveitis or herpetic infection, and cystoid macular edema; it is preferred as initial therapy. The types of prostaglandin analogs used in routine clinics include:
- Latanoprost
- Travoprost
- Bimatoprost
- Tafluprost
- Latanoprostene Bunod: This has nitric oxide-donating properties.
Adrenergic agents: Reduces IOP 20% to 25% by decreasing AH production and increasing uveoscleral outflow.[94] Brimonidine may cause allergic blepharoconjunctivitis and apnea, lethargy, or bradycardia in children. These agents include:(B3)
- Brimonidine
- Apraclonidine
Beta-blockers: Reduces IOP 20% to 25% by decreasing the production of AH.[95] Non-selective beta-blockers should be avoided in chronic obstructive pulmonary disease and asthma. Other contraindications include heart block, hypotension, and bradycardia. These drops include:(A1)
- Non-selective (may have effects on other receptors in the body and thus may have more side effects in some patients)
- Timolol
- Carteolol
- Levobunolol
- Metipranolol
- Selective (show better safety profile about respiratory symptoms)
- Betaxolol
Carbonic anhydrase inhibitor: Reduces IOP by 15% to 20%, decreasing the production of AH.[96](B3)
- Dorzolamide
- Brinzolamide
Cholinergic or parasympathomimetic agents reduce IOP by 20% to 25% by increasing the outflow of AH.[97] These agents are poorly tolerated and normally not considered first-line treatment.
- Pilocarpine
Systemic agents
These are used in the acute rise of IOP and angle-closure glaucoma or when topical medications are not tolerated.
Carbonic anhydrase inhibitor:
- Acetazolamide
Osmotic agents:
- Mannitol
- Glycerol
Laser Therapy for OAG
Laser trabeculoplasty
The indications of laser trabeculoplasty include
- The primary therapy for OAG
- Reduce the number of glaucoma drops
- Non-compliance or intolerance to medical therapy
- Failure of medical therapy as a less invasive alternative therapy compared to surgery
The available methods of laser trabeculoplasty are:
- Argon laser trabeculoplasty: More than 75% of unoperated eyes initially have a good IOP reduction. Within 5 years, 30% to >50% of eyes need additional surgical management.[98]
- Selective laser trabeculoplasty: This uses Q-switched frequency-doubled Nd-YAG and is preferred to argon laser trabeculoplasty (ALT) because it utilizes less laser energy, reducing inflammation and less mechanical injury to the TM. The efficacy of selective laser trabeculoplasty is similar to ALT and possible to repeat over time.[99]
- Micropulse Diode Laser Trabeculoplasty: This laser is based on subthreshold micropulse laser techniques that aim to cause less damage and side effects to angle structures without compromising efficacy.[100] (B3)
Diode laser cyclophotocoagulation
This is a method for ablation of the ciliary processes that secrete aqueous.[101] Indications include:
- Uncontrolled IOP in eyes with ambulatory vision if chances of surgical success are poor
- Management of refractory glaucoma
- Uncontrolled IOP in painful blind eyes or eyes with minimal visual potential
- Uncontrolled IOP with maximal medication after failed glaucoma surgery(ies)
Surgical Management of OAG
Indications for surgical management of glaucoma are:
- IOP above target pressure or progression of visual fields and optic disc changes after compliance and maximally tolerable glaucoma medication
- To avoid excessive glaucoma drops
- Significant barriers to effective and regular medication: cost, compliance, physical disability, inconvenience, side effects, and psychosocial
- Primary therapy for advanced glaucoma requires low target IOP
- Patient preference over other options [102]
Surgical options include:
- Trabeculectomy: The success rate may vary from 31% to 88%, increasing with using mitomycin C or 5-fluorouracil (These agents, however, increase the risk of late-onset bleb leak, hypotony, and bleb-related infection.)[103]
- Glaucoma drainage device and valve: Molteno, Baerveldt, Ahmed [104]
- Non-penetrating glaucoma surgery:
- Deep sclerectomy
- Viscocanalostomy
- Canaloplasty [105]
- Minimally invasive or micro-invasive glaucoma surgery [106] provides a conjunctiva-sparing surgery with an ab-interno approach to reduce IOP in mild to moderate glaucoma. The different approaches include:
- Increasing trabecular outflow (Trabectome, iStent, Hydrus stent, gonioscopy-assisted transluminal trabeculotomy, excimer laser trabeculotomy)
- Suprachoroidal shunts (Cypass micro-stent)
- Reducing aqueous production (endocyclophotocoagulation)
- Subconjunctival filtration (XEN gel stent)[107] (A1)
Cyclocryotherapy
This is another method of cycloablation using cryotherapy, reserved for painful vision loss.[108]
Other options for painful blind eyes from glaucoma
Differential Diagnosis
The differential diagnoses should include:
- Optic nerve head diseases
- Physiological cup: Deep cup with healthy neuroretinal rim is seen with normal retinal nerve fiber layer thickness and no visual field defect; disc size may be large
- Optic disc drusen
- Optic disc coloboma
- Anomalous optic disc
- Tilted disc
- Ischemic optic neuropathy
- Retinal diseases causing similar visual field defects
- Branch retinal vein occlusion
- Branch retinal artery occlusion
- Retinitis pigmentosa
- Panretinal photocoagulation
- Central nervous system diseases
- Pituitary tumor: NRR is typically pale, pallor more than cupping, and bitemporal hemianopia exists, which respects the vertical line passing through the fixation (contrary to glaucoma, whose visual field respects the horizontal meridian)
- Intracranial hypotension due to cerebrospinal fluid shunts or other neurologic pathologies
- Foster Kennedy Syndrome
- Cerebrovascular pathologies or traumas
- Multiple sclerosis
Staging
The Americal Academy of Ophthalmology's preferred practice pattern [35] classifies the severity of glaucomatous damage into different categories:
- Mild: Definite optic disc or RNFL abnormalities consistent with glaucoma as detailed above and a normal visual field tested with standard automated perimetry (SAP) are seen.
- Moderate: Definite optic disc or RNFL abnormalities consistent with glaucoma, as detailed above, are seen, and visual field abnormalities in one hemifield are not within 5° of fixation as tested with SAP.
- Severe: Definite optic disc or RNFL abnormalities consistent with glaucoma as detailed above are seen, and visual field abnormalities in both hemifields or loss within 5° of fixation in at least one hemifield as tested with SAP.
- Indeterminate: Definite optic disc or RNFL abnormalities consistent with glaucoma, as detailed above, are seen, and the patient cannot perform visual field testing, has unreliable or uninterpretable visual field test results, or has not performed visual fields yet.
Several different staging systems are recognized based on visual field damage, [111][112] optic disc cupping,[65][113] and RNFL defects with OCT,[114] some of which are applicable in a routine clinical setting or clinical trials.[115]
Prognosis
Advanced POAG may cause optic atrophy and no perception of light, though most OAG patients will not lose vision in their lifetime. Risk factors for progression of OAG include:
- Old age
- Elevated IOP
- Increased cup-to-disc ratio or small optic rim area
- Beta peripapillary atrophy
- Disc hemorrhage
- Thin central corneal thickness
- Reduced corneal hysteresis
- Low ocular perfusion pressure
- Poor compliance with therapy
- Pseudoexfoliation [35]
In 10 years, the cumulative probability of end-stage glaucoma in at least one eye in untreated cases was shown to be 35% in study results.[116]
Complications
Complications of glaucoma include:
- Blindness: usually painless
- Painful blind eye or absolute glaucoma: OAG predisposes to central retinal venous occlusion, leading to neovascular glaucoma and painful blind eye [117]
Consultations
Screening and management of OAG are typically performed by the following healthcare professionals that deal with:
- Ophthalmology, comprehensive general
- Ophthalmology, glaucoma specialist
- Optometry with special training in ocular hypertension and glaucoma
Deterrence and Patient Education
Glaucoma is a preventable cause of blindness, making patient education crucial in managing and preventing the progression of OAG. Effective and successful treatment of OAG can prevent the evolution of optic nerve atrophy and preserve patient vision.[118] However, patient adherence and compliance with medical therapy are notoriously difficult.[119] Treatment regimens require daily treatment to control IOP, and this can be a challenging task for patients for the rest of their lives.[120]
The nature of medication regimens requiring daily dosage is challenging for many patients, and inconsistent medication administration does not adequately control IOP. Some patients will attempt to use their drops daily but fail to deliver the medications to their eyes. Thus, the medication will not be absorbed, specifically in at-risk older populations. Over a prolonged time frame, failure to adhere to daily drops or oral medication will increase the likelihood of progression to blindness.[121]
Studies have confirmed an inverse relationship between the number and frequency of dosage and patient adherence concerning glaucoma treatment. One study looked into the reasons why patients struggled to adhere to their regimens, and the most commonly cited reasons were forgetfulness (30%), other priorities (11%), lack of information (9%), emotional factors (7%) with 27% of individuals surveyed not providing a reason.
Previous studies have shown that improved patient education regarding disease processes and the rationale behind treatment regimens makes patients consistently more likely to adhere to their prescribed medication regimens. A 2018 study found that physician-centric multifaceted informational and educational mailings were ineffective in improving adherence to IOP-lowering treatment in older patients with glaucoma.[122][123]
Educating patients is crucial for effective glaucoma management, but the best way to provide such education is still unknown. Interestingly, other studies have found no link between medication adherence and side effects and that side effects are unlikely to discourage patients. One of the tricky aspects of glaucoma is that patients often do not experience any symptoms until it is too late. An interprofessional approach is required to tackle this issue, as not all patients visit their ophthalmologist regularly. Therefore, nurses, therapists, social care workers, and primary care clinicians should be the first line of defense.
Enhancing Healthcare Team Outcomes
Open-angle glaucoma is a chronic eye condition characterized by increased intraocular pressure, potentially leading to optic nerve damage and vision loss. As the most common type of glaucoma, it often develops gradually without noticeable symptoms until advanced stages. Regular eye exams, including measuring intraocular pressure and assessing optic nerve health, are crucial for early detection. Treatment aims to lower intraocular pressure through medications, laser therapy, or surgery. Clinicians should emphasize the importance of adherence to prescribed treatments and routine follow-up appointments. Given its asymptomatic nature, raising awareness among at-risk populations, such as individuals older than 40 or those with a family history, is essential for early intervention and optimal management of open-angle glaucoma.
If untreated, OAG leads to progressive loss of peripheral vision followed by central visual field loss. Due to its chronicity, the condition is best managed by an interprofessional team that provides patient education and ensures that daily dosing is maintained. The best outcomes occur when the clinician, ophthalmic specialty-trained nurse, and pharmacist work together to educate and support the patient.
Media
(Click Image to Enlarge)
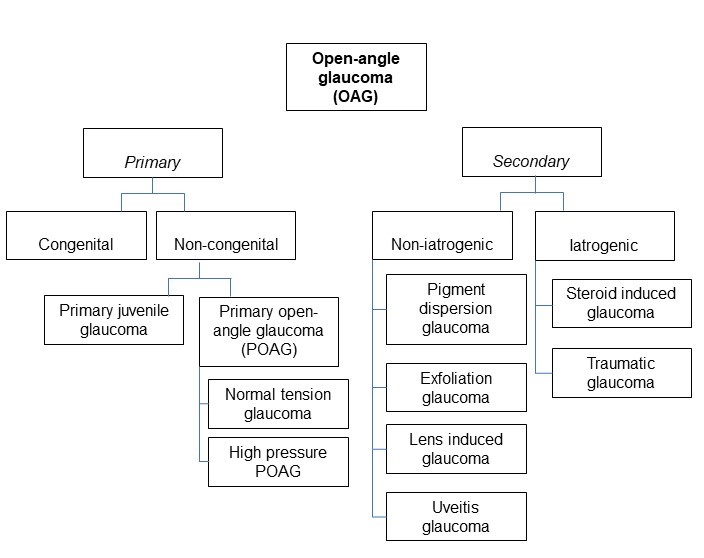
Classification of open-angle glaucoma. Contributed by Marco Zeppieri, MD, PhD.
(Click Image to Enlarge)
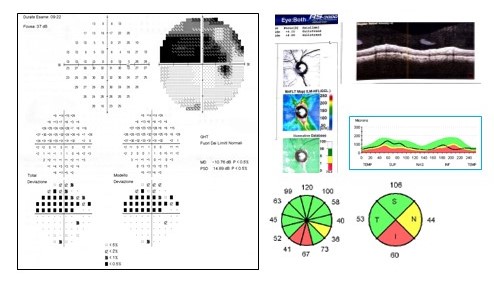
Visual field and Optical Coherence Tomography (OCT) results in a patients with open-angle glaucoma. Superior visual field defects correspond to inferior retinal nerve fiber layer thinning with OCT. Contributed by Marco Zeppieri, MD, PhD.
(Click Image to Enlarge)
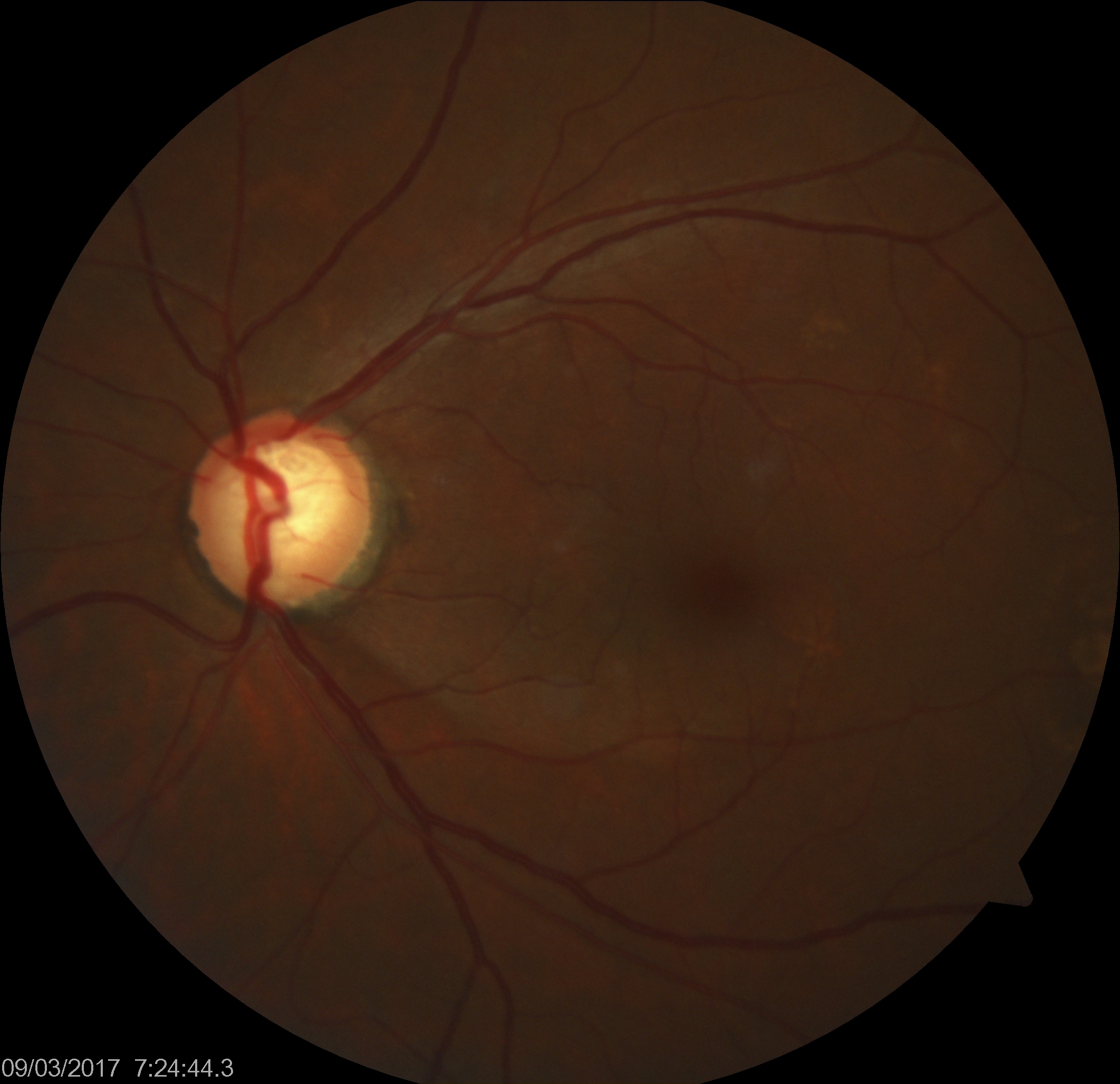
Glaucomatous Optic Nerve Head Showing Inferotemporal Retinal Nerve Fiber Layer Defect. Increased intraocular pressure can result in reduced blood supply to the optic nerve fibers, resulting in subtle ischemic injury.
Contributed by K Tripathy, MD
(Click Image to Enlarge)
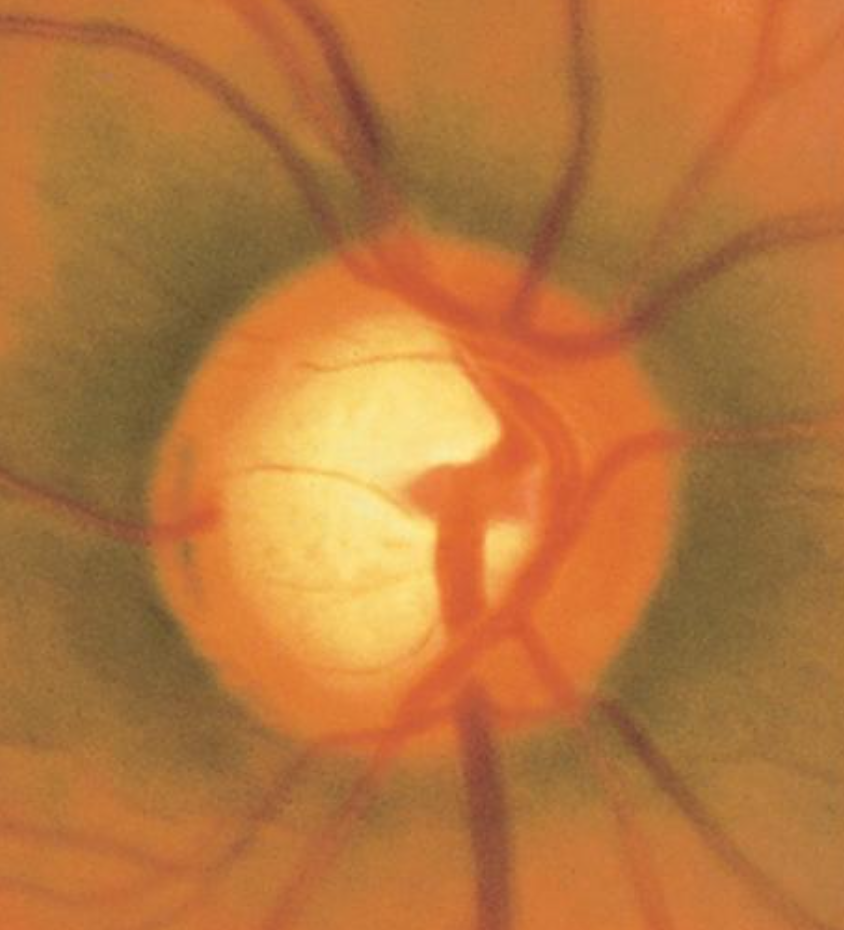
Optic Nerve Cup-to-Disc Ratio of 0.75. A cup-to-disc ratio greater than 0.5 is often associated with glaucoma, and initial loss is typically observed in the inferotemporal and superotemporal poles of the optic disc.
Contributed by AS Huang, MD
(Click Image to Enlarge)
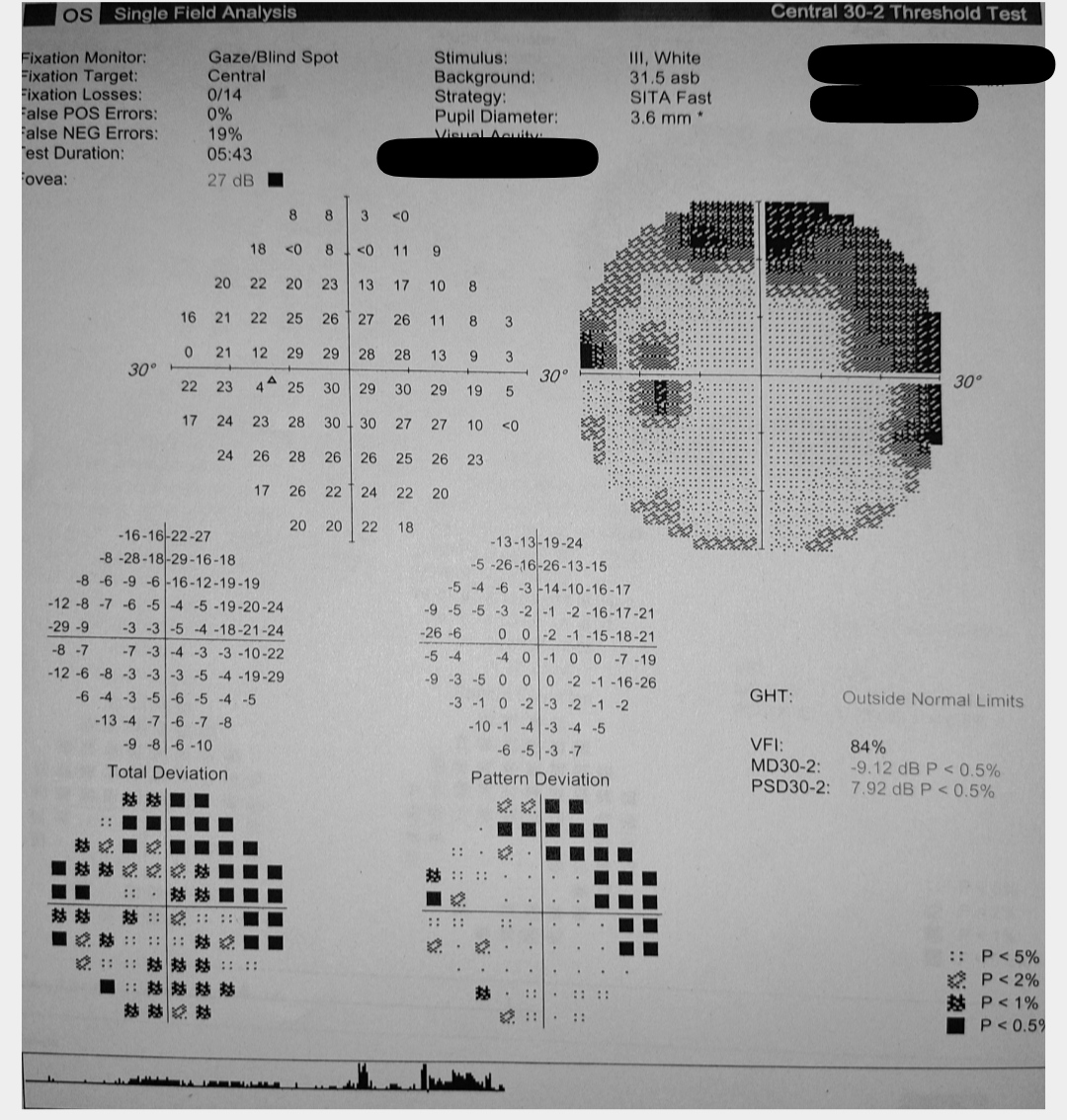
Left Eye Glaucomatous Visual Field Changes. This image displays the results of a visual field test indicating characteristic changes associated with glaucoma in the left eye, as observed on perimetry.
Contributed by S Shah, MBBS
(Click Image to Enlarge)
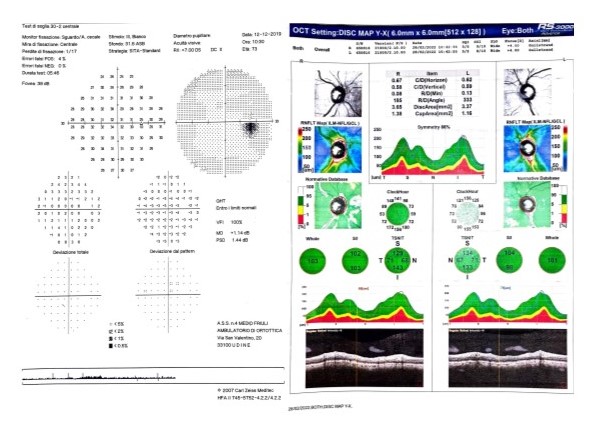
Normal visual field and Optical Coherence Tomography (OCT) results in a patients with ocular hypertension (OHT). Contributed by Marco Zeppieri, MD, PhD
(Click Image to Enlarge)
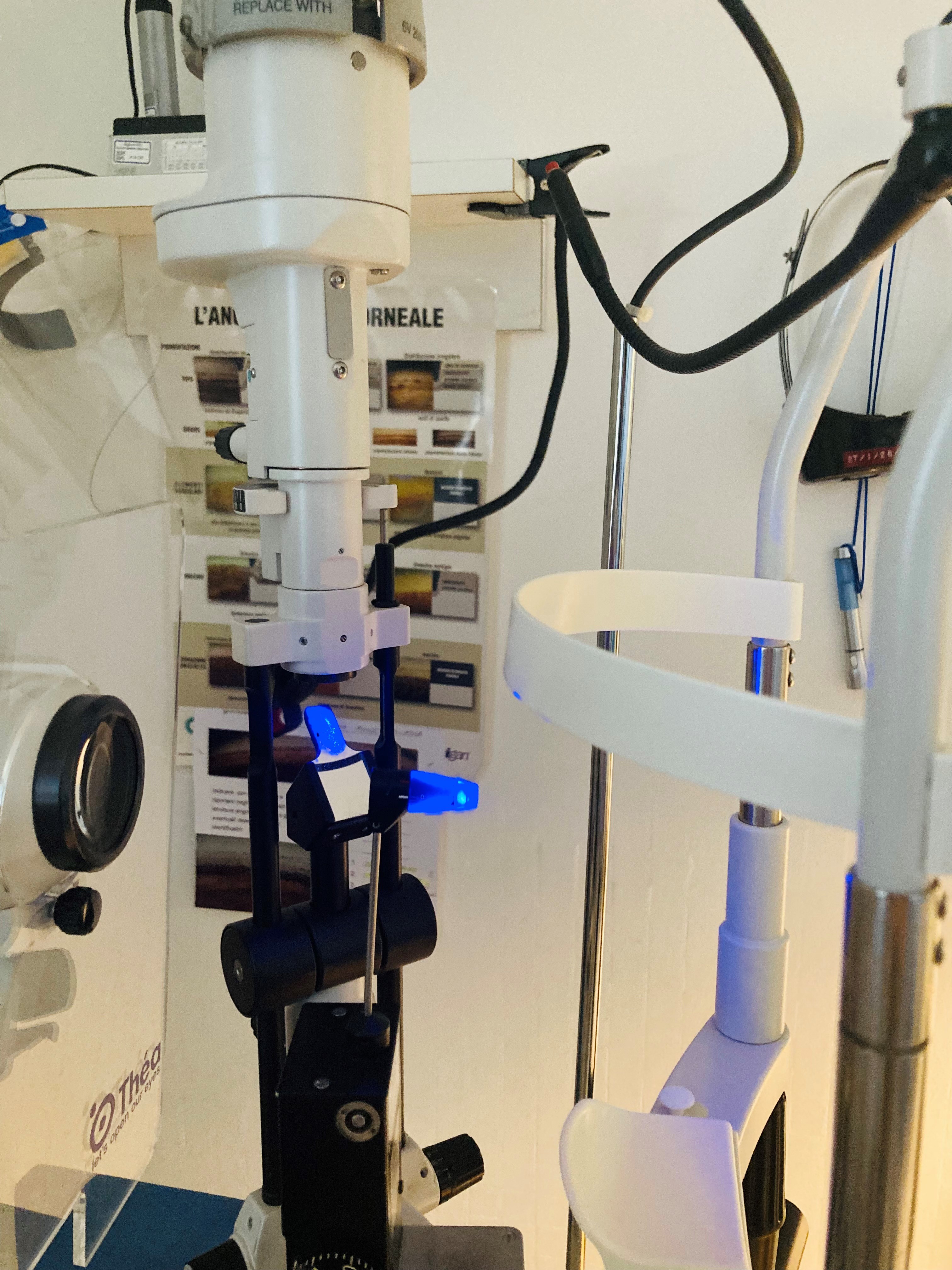
Goldmann Applanation Tonometer (GAT) mounted on a slit-lamp. Contributed by Marco Zeppieri, MD, PhD.
(Click Image to Enlarge)
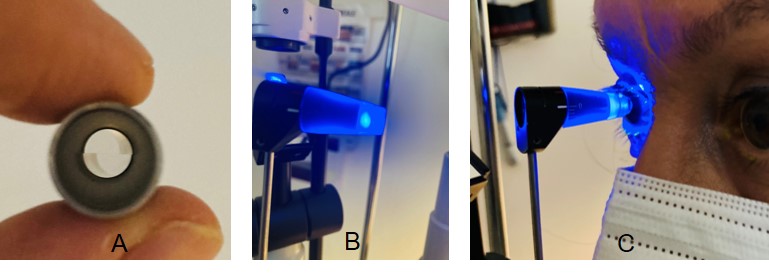
A tip with a split-image prism (A) is used with the Goldmann Applanation Tonometer (GAT), which is mounted on a slit-lamp (B). Filtered cobalt blue light is used during the measurement. The tip is positioned on the center of the eye to gently flatten the cornea (C). Contributed by Marco Zeppieri, MD, PhD.
References
Gupta D, Chen PP. Glaucoma. American family physician. 2016 Apr 15:93(8):668-74 [PubMed PMID: 27175839]
Leung DYL, Tham CC. Normal-tension glaucoma: Current concepts and approaches-A review. Clinical & experimental ophthalmology. 2022 Mar:50(2):247-259. doi: 10.1111/ceo.14043. Epub 2022 Feb 7 [PubMed PMID: 35040248]
Kastner A, King AJ. Advanced glaucoma at diagnosis: current perspectives. Eye (London, England). 2020 Jan:34(1):116-128. doi: 10.1038/s41433-019-0637-2. Epub 2019 Nov 18 [PubMed PMID: 31740802]
Level 3 (low-level) evidenceParajuli S, Shrestha P, Sharma S, Shrestha JK. Prevalence of Ocular Hypertension in Patients Above 40 Years of Age. Nepalese journal of ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2022 Jan:14(27):140-143. doi: 10.3126/nepjoph.v14i1.29740. Epub [PubMed PMID: 35996922]
Gordon MO, Kass MA. What We Have Learned From the Ocular Hypertension Treatment Study. American journal of ophthalmology. 2018 May:189():xxiv-xxvii. doi: 10.1016/j.ajo.2018.02.016. Epub 2018 Mar 1 [PubMed PMID: 29501371]
Veeraraghavan N. Adult Eye Conditions: Primary Open-Angle Glaucoma and Cataract. FP essentials. 2022 Aug:519():19-23 [PubMed PMID: 35947132]
Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014 May 14:311(18):1901-11. doi: 10.1001/jama.2014.3192. Epub [PubMed PMID: 24825645]
Liu K, He W, Zhao J, Zeng Y, Cheng H. Association of WDR36 polymorphisms with primary open angle glaucoma: A systematic review and meta-analysis. Medicine. 2017 Jun:96(26):e7291. doi: 10.1097/MD.0000000000007291. Epub [PubMed PMID: 28658128]
Level 1 (high-level) evidenceMonemi S, Spaeth G, DaSilva A, Popinchalk S, Ilitchev E, Liebmann J, Ritch R, Héon E, Crick RP, Child A, Sarfarazi M. Identification of a novel adult-onset primary open-angle glaucoma (POAG) gene on 5q22.1. Human molecular genetics. 2005 Mar 15:14(6):725-33 [PubMed PMID: 15677485]
Level 3 (low-level) evidenceThorleifsson G, Walters GB, Hewitt AW, Masson G, Helgason A, DeWan A, Sigurdsson A, Jonasdottir A, Gudjonsson SA, Magnusson KP, Stefansson H, Lam DS, Tam PO, Gudmundsdottir GJ, Southgate L, Burdon KP, Gottfredsdottir MS, Aldred MA, Mitchell P, St Clair D, Collier DA, Tang N, Sveinsson O, Macgregor S, Martin NG, Cree AJ, Gibson J, Macleod A, Jacob A, Ennis S, Young TL, Chan JC, Karwatowski WS, Hammond CJ, Thordarson K, Zhang M, Wadelius C, Lotery AJ, Trembath RC, Pang CP, Hoh J, Craig JE, Kong A, Mackey DA, Jonasson F, Thorsteinsdottir U, Stefansson K. Common variants near CAV1 and CAV2 are associated with primary open-angle glaucoma. Nature genetics. 2010 Oct:42(10):906-9. doi: 10.1038/ng.661. Epub 2010 Sep 12 [PubMed PMID: 20835238]
Level 2 (mid-level) evidenceBorrás T. Gene expression in the trabecular meshwork and the influence of intraocular pressure. Progress in retinal and eye research. 2003 Jul:22(4):435-63 [PubMed PMID: 12742391]
Pasquale LR, Loomis SJ, Kang JH, Yaspan BL, Abdrabou W, Budenz DL, Chen TC, Delbono E, Friedman DS, Gaasterland D, Gaasterland T, Grosskreutz CL, Lee RK, Lichter PR, Liu Y, McCarty CA, Moroi SE, Olson LM, Realini T, Rhee DJ, Schuman JS, Singh K, Vollrath D, Wollstein G, Zack DJ, Allingham RR, Pericak-Vance MA, Weinreb RN, Zhang K, Hauser MA, Richards JE, Haines JL, Wiggs JL. CDKN2B-AS1 genotype-glaucoma feature correlations in primary open-angle glaucoma patients from the United States. American journal of ophthalmology. 2013 Feb:155(2):342-353.e5. doi: 10.1016/j.ajo.2012.07.023. Epub 2012 Oct 27 [PubMed PMID: 23111177]
Level 2 (mid-level) evidenceNunes HF, Ananina G, Costa VP, Zanchin NIT, de Vasconcellos JPC, de Melo MB. Investigation of CAV1/CAV2 rs4236601 and CDKN2B-AS1 rs2157719 in primary open-angle glaucoma patients from Brazil. Ophthalmic genetics. 2018 Apr:39(2):194-199. doi: 10.1080/13816810.2017.1393830. Epub 2017 Nov 7 [PubMed PMID: 29111846]
Burdon KP, Macgregor S, Hewitt AW, Sharma S, Chidlow G, Mills RA, Danoy P, Casson R, Viswanathan AC, Liu JZ, Landers J, Henders AK, Wood J, Souzeau E, Crawford A, Leo P, Wang JJ, Rochtchina E, Nyholt DR, Martin NG, Montgomery GW, Mitchell P, Brown MA, Mackey DA, Craig JE. Genome-wide association study identifies susceptibility loci for open angle glaucoma at TMCO1 and CDKN2B-AS1. Nature genetics. 2011 Jun:43(6):574-8. doi: 10.1038/ng.824. Epub 2011 May 1 [PubMed PMID: 21532571]
Level 3 (low-level) evidenceShim MS, Kim KY, Noh M, Ko JY, Ahn S, An MA, Iwata T, Perkins GA, Weinreb RN, Ju WK. Optineurin E50K triggers BDNF deficiency-mediated mitochondrial dysfunction in retinal photoreceptor cell line. Biochemical and biophysical research communications. 2018 Sep 18:503(4):2690-2697. doi: 10.1016/j.bbrc.2018.08.025. Epub 2018 Aug 9 [PubMed PMID: 30100066]
Ma L, Zeng Y, Wei J, Yang D, Ding G, Liu J, Shang J, Kang Y, Ji X. Knockdown of LOXL1 inhibits TGF-β1-induced proliferation and fibrogenesis of hepatic stellate cells by inhibition of Smad2/3 phosphorylation. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie. 2018 Nov:107():1728-1735. doi: 10.1016/j.biopha.2018.08.156. Epub 2018 Sep 10 [PubMed PMID: 30257391]
Berner D, Zenkel M, Pasutto F, Hoja U, Liravi P, Gusek-Schneider GC, Kruse FE, Schödel J, Reis A, Schlötzer-Schrehardt U. Posttranscriptional Regulation of LOXL1 Expression Via Alternative Splicing and Nonsense-Mediated mRNA Decay as an Adaptive Stress Response. Investigative ophthalmology & visual science. 2017 Nov 1:58(13):5930-5940. doi: 10.1167/iovs.17-22963. Epub [PubMed PMID: 29164236]
Guven Yilmaz S, Palamar M, Onay H, Ilim O, Aykut A, Ozkinay FF, Yagci A. Association of Lysyl Oxidase-like 1 Gene Polymorphism in Turkish Patients With Pseudoexfoliation Syndrome and Pseudoexfoliation Glaucoma. Journal of glaucoma. 2017 Jul:26(7):684-685. doi: 10.1097/IJG.0000000000000672. Epub [PubMed PMID: 28369001]
Sharma S, Martin S, Sykes MJ, Dave A, Hewitt AW, Burdon KP, Ronci M, Voelcker NH, Craig JE. Biological effect of LOXL1 coding variants associated with pseudoexfoliation syndrome. Experimental eye research. 2016 May:146():212-223. doi: 10.1016/j.exer.2016.03.013. Epub 2016 Mar 18 [PubMed PMID: 26997634]
Gao XR, Chiariglione M, Arch AJ. Whole-exome sequencing study identifies rare variants and genes associated with intraocular pressure and glaucoma. Nature communications. 2022 Nov 30:13(1):7376. doi: 10.1038/s41467-022-35188-3. Epub 2022 Nov 30 [PubMed PMID: 36450729]
Mabuchi F, Mabuchi N, Sakurada Y, Yoneyama S, Kashiwagi K, Yamagata Z, Takamoto M, Aihara M, Iwata T, Hashimoto K, Sato K, Shiga Y, Nakazawa T, Akiyama M, Kawase K, Ozaki M, Araie M. Genetic variants associated with glaucomatous visual field loss in primary open-angle glaucoma. Scientific reports. 2022 Dec 1:12(1):20744. doi: 10.1038/s41598-022-24915-x. Epub 2022 Dec 1 [PubMed PMID: 36456827]
Zukerman R, Harris A, Oddone F, Siesky B, Verticchio Vercellin A, Ciulla TA. Glaucoma Heritability: Molecular Mechanisms of Disease. Genes. 2021 Jul 27:12(8):. doi: 10.3390/genes12081135. Epub 2021 Jul 27 [PubMed PMID: 34440309]
Zhang N, Wang J, Li Y, Jiang B. Prevalence of primary open angle glaucoma in the last 20 years: a meta-analysis and systematic review. Scientific reports. 2021 Jul 2:11(1):13762. doi: 10.1038/s41598-021-92971-w. Epub 2021 Jul 2 [PubMed PMID: 34215769]
Level 1 (high-level) evidenceMalihi M, Moura Filho ER, Hodge DO, Sit AJ. Long-term trends in glaucoma-related blindness in Olmsted County, Minnesota. Ophthalmology. 2014 Jan:121(1):134-141. doi: 10.1016/j.ophtha.2013.09.003. Epub 2013 Oct 25 [PubMed PMID: 24823760]
Level 2 (mid-level) evidenceQuigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. The British journal of ophthalmology. 2006 Mar:90(3):262-7 [PubMed PMID: 16488940]
Distelhorst JS, Hughes GM. Open-angle glaucoma. American family physician. 2003 May 1:67(9):1937-44 [PubMed PMID: 12751655]
Wolfs RC, Klaver CC, Ramrattan RS, van Duijn CM, Hofman A, de Jong PT. Genetic risk of primary open-angle glaucoma. Population-based familial aggregation study. Archives of ophthalmology (Chicago, Ill. : 1960). 1998 Dec:116(12):1640-5 [PubMed PMID: 9869795]
Birhanu G, Tegegne AS. Predictors for elevation of Intraocular Pressure (IOP) on glaucoma patients; a retrospective cohort study design. BMC ophthalmology. 2022 Jun 7:22(1):254. doi: 10.1186/s12886-022-02431-w. Epub 2022 Jun 7 [PubMed PMID: 35672680]
Level 2 (mid-level) evidenceHa A, Kim CY, Shim SR, Chang IB, Kim YK. Degree of Myopia and Glaucoma Risk: A Dose-Response Meta-analysis. American journal of ophthalmology. 2022 Apr:236():107-119. doi: 10.1016/j.ajo.2021.10.007. Epub 2021 Oct 11 [PubMed PMID: 34648776]
Level 1 (high-level) evidenceIkeda Y, Mori K, Maruyama Y, Ueno M, Yoshii K, Yamamoto Y, Imai K, Omi N, Sato R, Sato F, Nakano M, Hamuro J, Tashiro K, Sotozono C, Kinoshita S. Novel Vertical Cup-to-Disc Classification to Identify Normal Eyes That Maintain Non-Glaucoma Status: A 10-Year Longitudinal Study. Journal of glaucoma. 2023 Feb 1:32(2):127-132. doi: 10.1097/IJG.0000000000002109. Epub 2022 Aug 25 [PubMed PMID: 36001508]
Lee EJ, Kee HJ, Han JC, Kee C. Evidence-based understanding of disc hemorrhage in glaucoma. Survey of ophthalmology. 2021 May-Jun:66(3):412-422. doi: 10.1016/j.survophthal.2020.09.001. Epub 2020 Sep 17 [PubMed PMID: 32949554]
Level 3 (low-level) evidenceZeppieri M, Brusini P, Miglior S. Corneal thickness and functional damage in patients with ocular hypertension. European journal of ophthalmology. 2005 Mar-Apr:15(2):196-201 [PubMed PMID: 15812759]
Kim KE, Oh S, Baek SU, Ahn SJ, Park KH, Jeoung JW. Ocular Perfusion Pressure and the Risk of Open-Angle Glaucoma: Systematic Review and Meta-analysis. Scientific reports. 2020 Jun 22:10(1):10056. doi: 10.1038/s41598-020-66914-w. Epub 2020 Jun 22 [PubMed PMID: 32572072]
Level 1 (high-level) evidenceLeske MC, Wu SY, Hennis A, Honkanen R, Nemesure B, BESs Study Group. Risk factors for incident open-angle glaucoma: the Barbados Eye Studies. Ophthalmology. 2008 Jan:115(1):85-93 [PubMed PMID: 17629563]
Level 2 (mid-level) evidencePrum BE Jr, Rosenberg LF, Gedde SJ, Mansberger SL, Stein JD, Moroi SE, Herndon LW Jr, Lim MC, Williams RD. Primary Open-Angle Glaucoma Preferred Practice Pattern(®) Guidelines. Ophthalmology. 2016 Jan:123(1):P41-P111. doi: 10.1016/j.ophtha.2015.10.053. Epub 2015 Nov 12 [PubMed PMID: 26581556]
Li Y, Mitchell W, Elze T, Zebardast N. Association Between Diabetes, Diabetic Retinopathy, and Glaucoma. Current diabetes reports. 2021 Sep 8:21(10):38. doi: 10.1007/s11892-021-01404-5. Epub 2021 Sep 8 [PubMed PMID: 34495413]
Matsuda A, Hara T, Miyata K, Matsuo H, Murata H, Mayama C, Asaoka R. Do pattern deviation values accurately estimate glaucomatous visual field damage in eyes with glaucoma and cataract? The British journal of ophthalmology. 2015 Sep:99(9):1240-4. doi: 10.1136/bjophthalmol-2014-306019. Epub 2015 Mar 20 [PubMed PMID: 25795915]
Level 2 (mid-level) evidenceGramer G, Weber BH, Gramer E. Migraine and Vasospasm in Glaucoma: Age-Related Evaluation of 2027 Patients With Glaucoma or Ocular Hypertension. Investigative ophthalmology & visual science. 2015 Dec:56(13):7999-8007. doi: 10.1167/iovs.15-17274. Epub [PubMed PMID: 26720447]
Baneke AJ, Aubry J, Viswanathan AC, Plant GT. The role of intracranial pressure in glaucoma and therapeutic implications. Eye (London, England). 2020 Jan:34(1):178-191. doi: 10.1038/s41433-019-0681-y. Epub 2019 Nov 27 [PubMed PMID: 31776450]
Hogden K, Mikelberg F, Sodhi M, Khosrow-Khavar F, Mansournia MA, Kezouh A, Etminan M. The association between hormonal contraceptive use and glaucoma in women of reproductive age. British journal of clinical pharmacology. 2021 Dec:87(12):4780-4785. doi: 10.1111/bcp.14920. Epub 2021 Jun 22 [PubMed PMID: 34159623]
Moreno-Montañés J, Gándara E, Gutierrez-Ruiz I, Moreno-Galarraga L, Ruiz-Canela M, Bes-Rastrollo M, Martínez-González MÁ, Fernandez-Montero A. Healthy Lifestyle Score and Incidence of Glaucoma: The Sun Project. Nutrients. 2022 Feb 12:14(4):. doi: 10.3390/nu14040779. Epub 2022 Feb 12 [PubMed PMID: 35215429]
Quigley HA, McKinnon SJ, Zack DJ, Pease ME, Kerrigan-Baumrind LA, Kerrigan DF, Mitchell RS. Retrograde axonal transport of BDNF in retinal ganglion cells is blocked by acute IOP elevation in rats. Investigative ophthalmology & visual science. 2000 Oct:41(11):3460-6 [PubMed PMID: 11006239]
Level 3 (low-level) evidenceBerson DM. Phototransduction in ganglion-cell photoreceptors. Pflugers Archiv : European journal of physiology. 2007 Aug:454(5):849-55 [PubMed PMID: 17351786]
Level 3 (low-level) evidenceHattar S, Kumar M, Park A, Tong P, Tung J, Yau KW, Berson DM. Central projections of melanopsin-expressing retinal ganglion cells in the mouse. The Journal of comparative neurology. 2006 Jul 20:497(3):326-49 [PubMed PMID: 16736474]
Level 3 (low-level) evidenceMorgan-Davies J, Taylor N, Hill AR, Aspinall P, O'Brien CJ, Azuara-Blanco A. Three dimensional analysis of the lamina cribrosa in glaucoma. The British journal of ophthalmology. 2004 Oct:88(10):1299-304 [PubMed PMID: 15377555]
Quigley HA, Addicks EM. Regional differences in the structure of the lamina cribrosa and their relation to glaucomatous optic nerve damage. Archives of ophthalmology (Chicago, Ill. : 1960). 1981 Jan:99(1):137-43 [PubMed PMID: 7458737]
Morgan-Davies J, King AJ, Aspinall P, O'Brien CJ. Measurement of a novel optic disc topographic parameter, "spikiness", in glaucoma. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2000 Aug:238(8):669-76 [PubMed PMID: 11011687]
Dielemans I, Vingerling JR, Wolfs RC, Hofman A, Grobbee DE, de Jong PT. The prevalence of primary open-angle glaucoma in a population-based study in The Netherlands. The Rotterdam Study. Ophthalmology. 1994 Nov:101(11):1851-5 [PubMed PMID: 7800368]
Level 2 (mid-level) evidenceZhang SH, Zhao JL, Wu C. [Microcirculation of optic nerve head and glaucoma]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2016 Jun 11:52(6):466-70. doi: 10.3760/cma.j.issn.0412-4081.2016.06.018. Epub [PubMed PMID: 27373574]
Fortune B, Reynaud J, Hardin C, Wang L, Sigal IA, Burgoyne CF. Experimental Glaucoma Causes Optic Nerve Head Neural Rim Tissue Compression: A Potentially Important Mechanism of Axon Injury. Investigative ophthalmology & visual science. 2016 Aug 1:57(10):4403-11. doi: 10.1167/iovs.16-20000. Epub [PubMed PMID: 27564522]
Buffault J, Labbé A, Hamard P, Brignole-Baudouin F, Baudouin C. The trabecular meshwork: Structure, function and clinical implications. A review of the literature. Journal francais d'ophtalmologie. 2020 Sep:43(7):e217-e230. doi: 10.1016/j.jfo.2020.05.002. Epub 2020 Jun 16 [PubMed PMID: 32561029]
Zukerman R, Harris A, Vercellin AV, Siesky B, Pasquale LR, Ciulla TA. Molecular Genetics of Glaucoma: Subtype and Ethnicity Considerations. Genes. 2020 Dec 31:12(1):. doi: 10.3390/genes12010055. Epub 2020 Dec 31 [PubMed PMID: 33396423]
Nishida T, Moghimi S, Chang AC, Walker E, Liebmann JM, Fazio MA, Girkin CA, Zangwill LM, Weinreb RN. Association of Intraocular Pressure With Retinal Nerve Fiber Layer Thinning in Patients With Glaucoma. JAMA ophthalmology. 2022 Dec 1:140(12):1209-1216. doi: 10.1001/jamaophthalmol.2022.4462. Epub [PubMed PMID: 36301523]
Rao HL, Dasari S, Puttaiah NK, Pradhan ZS, Moghimi S, Mansouri K, Webers CAB, Weinreb RN. Optical Microangiography and Progressive Retinal Nerve Fiber Layer Loss in Primary Open Angle Glaucoma. American journal of ophthalmology. 2022 Jan:233():171-179. doi: 10.1016/j.ajo.2021.07.023. Epub 2021 Jul 25 [PubMed PMID: 34320375]
Quigley HA, Addicks EM, Green WR, Maumenee AE. Optic nerve damage in human glaucoma. II. The site of injury and susceptibility to damage. Archives of ophthalmology (Chicago, Ill. : 1960). 1981 Apr:99(4):635-49 [PubMed PMID: 6164357]
Level 3 (low-level) evidenceCălugăru D, Mang A, Călugăru M. Secondary open-angle pigmentary glaucoma resulting from pseudophakia. Case report. Romanian journal of ophthalmology. 2016 Apr-Jun:60(2):125-130 [PubMed PMID: 29450335]
Level 3 (low-level) evidenceGil P, Pires J, Matos R, Cardoso MS, Lopes N, Matias J, Mariano M. Corneal Elevation Topography in Primary Open Angle Glaucoma. Journal of glaucoma. 2017 Feb:26(2):e41-e45. doi: 10.1097/IJG.0000000000000535. Epub [PubMed PMID: 27599178]
Alamri A, Alkatan H, Aljadaan I. Traumatic Ghost Cell Glaucoma with Successful Resolution of Corneal Blood Staining Following Pars Plana Vitrectomy. Middle East African journal of ophthalmology. 2016 Jul-Sep:23(3):271-3. doi: 10.4103/0974-9233.180778. Epub [PubMed PMID: 27555716]
Zeppieri M, Tripathy K. Pigment Dispersion Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 35593820]
Zeppieri M. Pigment dispersion syndrome: A brief overview. Journal of clinical and translational research. 2022 Oct 31:8(5):344-350 [PubMed PMID: 36518550]
Level 3 (low-level) evidencePadhy B, Alone DP. Is pseudoexfoliation glaucoma a neurodegenerative disorder? Journal of biosciences. 2021:46():. pii: 97. Epub [PubMed PMID: 34785624]
McMenamin PG, Lee WR. Ultrastructural pathology of melanomalytic glaucoma. The British journal of ophthalmology. 1986 Dec:70(12):895-906 [PubMed PMID: 3801367]
Level 3 (low-level) evidenceFeroze KB, Zeppieri M, Khazaeni L. Steroid-Induced Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 28613653]
Stein JD, Khawaja AP, Weizer JS. Glaucoma in Adults-Screening, Diagnosis, and Management: A Review. JAMA. 2021 Jan 12:325(2):164-174. doi: 10.1001/jama.2020.21899. Epub [PubMed PMID: 33433580]
Brusini P, Zeppieri M, Tosoni C, Parisi L, Salvetat ML. Optic disc damage staging system. Journal of glaucoma. 2010 Sep:19(7):442-9. doi: 10.1097/IJG.0b013e3181ca7303. Epub [PubMed PMID: 20051883]
Level 2 (mid-level) evidenceTripathy K, Sharma YR, Chawla R, Basu K, Vohra R, Venkatesh P. Triads in Ophthalmology: A Comprehensive Review. Seminars in ophthalmology. 2017:32(2):237-250. doi: 10.3109/08820538.2015.1045150. Epub 2015 Jul 6 [PubMed PMID: 26148300]
Maupin E, Baudin F, Arnould L, Seydou A, Binquet C, Bron AM, Creuzot-Garcher CP. Accuracy of the ISNT rule and its variants for differentiating glaucomatous from normal eyes in a population-based study. The British journal of ophthalmology. 2020 Oct:104(10):1412-1417. doi: 10.1136/bjophthalmol-2019-315554. Epub 2020 Jan 20 [PubMed PMID: 31959590]
Hollands H, Johnson D, Hollands S, Simel DL, Jinapriya D, Sharma S. Do findings on routine examination identify patients at risk for primary open-angle glaucoma? The rational clinical examination systematic review. JAMA. 2013 May 15:309(19):2035-42. doi: 10.1001/jama.2013.5099. Epub [PubMed PMID: 23677315]
Level 1 (high-level) evidenceSusanna R Jr, Vessani RM. Staging glaucoma patient: why and how? The open ophthalmology journal. 2009 Sep 17:3():59-64. doi: 10.2174/1874364100903020059. Epub 2009 Sep 17 [PubMed PMID: 19834563]
Kalyani VK, Bharucha KM, Goyal N, Deshpande MM. Comparison of diagnostic ability of standard automated perimetry, short wavelength automated perimetry, retinal nerve fiber layer thickness analysis and ganglion cell layer thickness analysis in early detection of glaucoma. Indian journal of ophthalmology. 2021 May:69(5):1108-1112. doi: 10.4103/ijo.IJO_2409_20. Epub [PubMed PMID: 33913843]
Zeppieri M, Brusini P, Parisi L, Johnson CA, Sampaolesi R, Salvetat ML. Pulsar perimetry in the diagnosis of early glaucoma. American journal of ophthalmology. 2010 Jan:149(1):102-12. doi: 10.1016/j.ajo.2009.07.020. Epub 2009 Oct 2 [PubMed PMID: 19800607]
Level 2 (mid-level) evidenceSalvetat ML, Zeppieri M, Parisi L, Johnson CA, Sampaolesi R, Brusini P. Learning effect and test-retest variability of pulsar perimetry. Journal of glaucoma. 2013 Mar:22(3):230-7. doi: 10.1097/IJG.0b013e318237bfe7. Epub [PubMed PMID: 22027935]
Level 2 (mid-level) evidenceSalvetat ML, Zeppieri M, Parisi L, Brusini P. Rarebit perimetry in normal subjects: test-retest variability, learning effect, normative range, influence of optical defocus, and cataract extraction. Investigative ophthalmology & visual science. 2007 Nov:48(11):5320-31 [PubMed PMID: 17962489]
Brusini P, Salvetat ML, Parisi L, Zeppieri M. Probing glaucoma visual damage by rarebit perimetry. The British journal of ophthalmology. 2005 Feb:89(2):180-4 [PubMed PMID: 15665349]
Brusini P, Salvetat ML, Zeppieri M, Tosoni C, Parisi L, Felletti M. Visual field testing with the new Humphrey Matrix: a comparison between the FDT N-30 and Matrix N-30-F tests. Acta ophthalmologica Scandinavica. 2006 Jun:84(3):351-6 [PubMed PMID: 16704697]
Mastropasqua L, Brusini P, Carpineto P, Ciancaglini M, Di Antonio L, Zeppieri MW, Parisi L. Humphrey matrix frequency doubling technology perimetry and optical coherence tomography measurement of the retinal nerve fiber layer thickness in both normal and ocular hypertensive subjects. Journal of glaucoma. 2006 Aug:15(4):328-35 [PubMed PMID: 16865011]
Harwerth RS, Quigley HA. Visual field defects and retinal ganglion cell losses in patients with glaucoma. Archives of ophthalmology (Chicago, Ill. : 1960). 2006 Jun:124(6):853-9 [PubMed PMID: 16769839]
Level 3 (low-level) evidenceHarwerth RS, Carter-Dawson L, Shen F, Smith EL 3rd, Crawford ML. Ganglion cell losses underlying visual field defects from experimental glaucoma. Investigative ophthalmology & visual science. 1999 Sep:40(10):2242-50 [PubMed PMID: 10476789]
Level 3 (low-level) evidenceShiga Y, Aizawa N, Tsuda S, Yokoyama Y, Omodaka K, Kunikata H, Yasui T, Kato K, Kurashima H, Miyamoto E, Hashimoto M, Nakazawa T. Preperimetric Glaucoma Prospective Study (PPGPS): Predicting Visual Field Progression With Basal Optic Nerve Head Blood Flow in Normotensive PPG Eyes. Translational vision science & technology. 2018 Jan:7(1):11. doi: 10.1167/tvst.7.1.11. Epub 2018 Jan 23 [PubMed PMID: 29372113]
Bader J, Zeppieri M, Havens SJ. Tonometry. StatPearls. 2024 Jan:(): [PubMed PMID: 29630277]
Brusini P, Salvetat ML, Zeppieri M. How to Measure Intraocular Pressure: An Updated Review of Various Tonometers. Journal of clinical medicine. 2021 Aug 27:10(17):. doi: 10.3390/jcm10173860. Epub 2021 Aug 27 [PubMed PMID: 34501306]
Zeppieri M, Gurnani B. Applanation Tonometry. StatPearls. 2024 Jan:(): [PubMed PMID: 35881737]
Campbell P, Edgar DF, Shah R. Inter-optometrist variability of IOP measurement for modern tonometers and their agreement with Goldmann Applanation Tonometry. Clinical & experimental optometry. 2021 Jul:104(5):602-610. doi: 10.1080/08164622.2021.1878831. Epub 2021 Feb 28 [PubMed PMID: 33689641]
Biswas S, Biswas P. Relationship between Diurnal Variation in Intraocular Pressure and Central Corneal Power. Optometry and vision science : official publication of the American Academy of Optometry. 2023 Jan 1:100(1):96-104. doi: 10.1097/OPX.0000000000001974. Epub 2022 Dec 13 [PubMed PMID: 36705719]
Belovay GW, Goldberg I. The thick and thin of the central corneal thickness in glaucoma. Eye (London, England). 2018 May:32(5):915-923. doi: 10.1038/s41433-018-0033-3. Epub 2018 Feb 15 [PubMed PMID: 29445115]
Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. The British journal of ophthalmology. 2002 Feb:86(2):238-42 [PubMed PMID: 11815354]
Level 2 (mid-level) evidenceKhazaeni B, Zeppieri M, Khazaeni L. Acute Angle-Closure Glaucoma. StatPearls. 2024 Jan:(): [PubMed PMID: 28613607]
Bhat KS, Reddy MV, Pai V. Correlation of retinal nerve fiber layer thickness with perimetric staging in primary open-angle glaucoma - A cross-sectional study. Oman journal of ophthalmology. 2022 Jan-Apr:15(1):36-42. doi: 10.4103/ojo.ojo_345_20. Epub 2022 Mar 2 [PubMed PMID: 35388245]
Level 2 (mid-level) evidenceKansal V, Armstrong JJ, Pintwala R, Hutnik C. Optical coherence tomography for glaucoma diagnosis: An evidence based meta-analysis. PloS one. 2018:13(1):e0190621. doi: 10.1371/journal.pone.0190621. Epub 2018 Jan 4 [PubMed PMID: 29300765]
Level 1 (high-level) evidenceSihota R, Angmo D, Ramaswamy D, Dada T. Simplifying "target" intraocular pressure for different stages of primary open-angle glaucoma and primary angle-closure glaucoma. Indian journal of ophthalmology. 2018 Apr:66(4):495-505. doi: 10.4103/ijo.IJO_1130_17. Epub [PubMed PMID: 29582808]
Sit AJ, Pruet CM. Personalizing Intraocular Pressure: Target Intraocular Pressure in the Setting of 24-Hour Intraocular Pressure Monitoring. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2016 Jan-Feb:5(1):17-22. doi: 10.1097/APO.0000000000000178. Epub [PubMed PMID: 26886115]
Zaharia AC, Dumitrescu OM, Radu M, Rogoz RE. Adherence to Therapy in Glaucoma Treatment-A Review. Journal of personalized medicine. 2022 Mar 22:12(4):. doi: 10.3390/jpm12040514. Epub 2022 Mar 22 [PubMed PMID: 35455630]
Holló G, Katsanos A, Boboridis KG, Irkec M, Konstas AGP. Preservative-Free Prostaglandin Analogs and Prostaglandin/Timolol Fixed Combinations in the Treatment of Glaucoma: Efficacy, Safety and Potential Advantages. Drugs. 2018 Jan:78(1):39-64. doi: 10.1007/s40265-017-0843-9. Epub [PubMed PMID: 29196953]
Oh DJ, Chen JL, Vajaranant TS, Dikopf MS. Brimonidine tartrate for the treatment of glaucoma. Expert opinion on pharmacotherapy. 2019 Jan:20(1):115-122. doi: 10.1080/14656566.2018.1544241. Epub 2018 Nov 8 [PubMed PMID: 30407890]
Level 3 (low-level) evidenceSkov AG, Rives AS, Freiberg J, Virgili G, Azuara-Blanco A, Kolko M. Comparative efficacy and safety of preserved versus preservative-free beta-blockers in patients with glaucoma or ocular hypertension: a systematic review. Acta ophthalmologica. 2022 May:100(3):253-261. doi: 10.1111/aos.14926. Epub 2021 Jun 14 [PubMed PMID: 34128326]
Level 1 (high-level) evidenceSupuran CT, Altamimi ASA, Carta F. Carbonic anhydrase inhibition and the management of glaucoma: a literature and patent review 2013-2019. Expert opinion on therapeutic patents. 2019 Oct:29(10):781-792. doi: 10.1080/13543776.2019.1679117. Epub 2019 Oct 15 [PubMed PMID: 31596641]
Level 3 (low-level) evidencePanarese V, Moshirfar M. Pilocarpine. StatPearls. 2024 Jan:(): [PubMed PMID: 32310588]
Greslechner R, Spiegel D. [Laser Trabeculoplasty in Modern Glaucoma Therapy - a Review]. Klinische Monatsblatter fur Augenheilkunde. 2019 Oct:236(10):1192-1200. doi: 10.1055/a-0577-7925. Epub 2018 Apr 11 [PubMed PMID: 29642265]
Landers J. Selective laser trabeculoplasty: A review. Clinical & experimental ophthalmology. 2021 Dec:49(9):1102-1110. doi: 10.1111/ceo.13979. Epub 2021 Aug 16 [PubMed PMID: 34331388]
Ma A, Yu SWY, Wong JKW. Micropulse laser for the treatment of glaucoma: A literature review. Survey of ophthalmology. 2019 Jul-Aug:64(4):486-497. doi: 10.1016/j.survophthal.2019.01.001. Epub 2019 Jan 11 [PubMed PMID: 30639207]
Level 3 (low-level) evidenceSouissi S, Le Mer Y, Metge F, Portmann A, Baudouin C, Labbé A, Hamard P. An update on continuous-wave cyclophotocoagulation (CW-CPC) and micropulse transscleral laser treatment (MP-TLT) for adult and paediatric refractory glaucoma. Acta ophthalmologica. 2021 Aug:99(5):e621-e653. doi: 10.1111/aos.14661. Epub 2020 Nov 22 [PubMed PMID: 33222409]
Lim R. The surgical management of glaucoma: A review. Clinical & experimental ophthalmology. 2022 Mar:50(2):213-231. doi: 10.1111/ceo.14028. Epub 2022 Jan 17 [PubMed PMID: 35037376]
King AJ, Hudson J, Fernie G, Kernohan A, Azuara-Blanco A, Burr J, Homer T, Shabaninejad H, Sparrow JM, Garway-Heath D, Barton K, Norrie J, McDonald A, Vale L, MacLennan G, TAGS Study Group. Primary trabeculectomy for advanced glaucoma: pragmatic multicentre randomised controlled trial (TAGS). BMJ (Clinical research ed.). 2021 May 12:373():n1014. doi: 10.1136/bmj.n1014. Epub 2021 May 12 [PubMed PMID: 33980505]
Level 1 (high-level) evidenceMuralidharan S, Kumar S, Ichhpujani P, Dhillon HK. Quality of life in glaucoma patients: Comparison of medical therapy, trabeculectomy, and glaucoma drainage device surgery. Indian journal of ophthalmology. 2022 Dec:70(12):4206-4211. doi: 10.4103/ijo.IJO_667_22. Epub [PubMed PMID: 36453315]
Level 2 (mid-level) evidenceWong D. Non-penetrating glaucoma surgery for advanced open-angle glaucoma. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2018 Aug:256(8):1479. doi: 10.1007/s00417-018-4026-5. Epub 2018 Jun 18 [PubMed PMID: 29911272]
Richter GM, Coleman AL. Minimally invasive glaucoma surgery: current status and future prospects. Clinical ophthalmology (Auckland, N.Z.). 2016:10():189-206. doi: 10.2147/OPTH.S80490. Epub 2016 Jan 28 [PubMed PMID: 26869753]
Pereira ICF, van de Wijdeven R, Wyss HM, Beckers HJM, den Toonder JMJ. Conventional glaucoma implants and the new MIGS devices: a comprehensive review of current options and future directions. Eye (London, England). 2021 Dec:35(12):3202-3221. doi: 10.1038/s41433-021-01595-x. Epub 2021 Jun 14 [PubMed PMID: 34127842]
Level 3 (low-level) evidenceMiljković A, Babić N, Čanadanović V, Davidović S, Ljikar J, Vasin M. EFFICACY OF CYCLOCRYOTHERAPY AND TRANSSCLERAL DIODE LASER CYCLOPHOTOCOAGULATION IN THE MANAGEMENT OF REFRACTORY GLAUCOMA. Acta clinica Croatica. 2021 Jun:60(2):171-177. doi: 10.20471/acc.2021.60.02.01. Epub [PubMed PMID: 34744265]
Kowanz DH, Wawer Matos PA, Gordon E, Doulis A, Simon M, Rokohl AC, Heindl LM. [Evisceration, enucleation and exenteration-Indications, techniques, and postoperative care]. Die Ophthalmologie. 2023 Feb:120(2):126-138. doi: 10.1007/s00347-022-01791-4. Epub 2023 Jan 12 [PubMed PMID: 36635593]
Galindo-Ferreiro A, Akaishi P, Cruz A, Khandekar R, Al Dosairi S, Dufaileej M, Al Salem A, Galvez-Ruiz A, Craven ER. Retrobulbar Injections for Blind Painful Eyes: A Comparative Study of Retrobulbar Alcohol Versus Chlorpromazine. Journal of glaucoma. 2016 Nov:25(11):886-890 [PubMed PMID: 27814327]
Level 2 (mid-level) evidenceSpaeth GL, Shields MB. The stages of glaucoma. American journal of ophthalmology. 2006 Jan:141(1):147-8 [PubMed PMID: 16386990]
Brusini P. Estimating glaucomatous anatomical damage by computerized automated perimetry. Acta ophthalmologica Scandinavica. Supplement. 1997:(224):28-9 [PubMed PMID: 9589720]
Spaeth GL, Lopes JF, Junk AK, Grigorian AP, Henderer J. Systems for staging the amount of optic nerve damage in glaucoma: a critical review and new material. Survey of ophthalmology. 2006 Jul-Aug:51(4):293-315 [PubMed PMID: 16818081]
Level 3 (low-level) evidenceBrusini P. OCT Glaucoma Staging System: a new method for retinal nerve fiber layer damage classification using spectral-domain OCT. Eye (London, England). 2018 Jan:32(1):113-119. doi: 10.1038/eye.2017.159. Epub 2017 Aug 4 [PubMed PMID: 28776589]
Ng M, Sample PA, Pascual JP, Zangwill LM, Girkin CA, Liebmann JM, Weinreb RN, Racette L. Comparison of visual field severity classification systems for glaucoma. Journal of glaucoma. 2012 Oct-Nov:21(8):551-61. doi: 10.1097/IJG.0b013e31821dac66. Epub [PubMed PMID: 21878817]
Level 2 (mid-level) evidenceWilson MR. Progression of visual field loss in untreated glaucoma patients and suspects in St Lucia, West Indies. Transactions of the American Ophthalmological Society. 2002:100():365-410 [PubMed PMID: 12545702]
Mokhles P, Schouten JS, Beckers HJ, Azuara-Blanco A, Tuulonen A, Webers CA. Glaucoma blindness at the end of life. Acta ophthalmologica. 2017 Feb:95(1):10-11. doi: 10.1111/aos.12933. Epub [PubMed PMID: 28102642]
Fiscella R, Caplan E, Kamble P, Bunniran S, Uribe C, Chandwani H. The Effect of an Educational Intervention on Adherence to Intraocular Pressure-Lowering Medications in a Large Cohort of Older Adults with Glaucoma. Journal of managed care & specialty pharmacy. 2018 Dec:24(12):1284-1294. doi: 10.18553/jmcp.2018.17465. Epub 2018 May 31 [PubMed PMID: 29848186]
Robin A, Grover DS. Compliance and adherence in glaucoma management. Indian journal of ophthalmology. 2011 Jan:59 Suppl(Suppl1):S93-6. doi: 10.4103/0301-4738.73693. Epub [PubMed PMID: 21150041]
Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009 Nov:116(11 Suppl):S30-6. doi: 10.1016/j.ophtha.2009.06.024. Epub [PubMed PMID: 19837258]
Level 3 (low-level) evidenceFriedman DS, Quigley HA, Gelb L, Tan J, Margolis J, Shah SN, Kim EE, Zimmerman T, Hahn SR. Using pharmacy claims data to study adherence to glaucoma medications: methodology and findings of the Glaucoma Adherence and Persistency Study (GAPS). Investigative ophthalmology & visual science. 2007 Nov:48(11):5052-7 [PubMed PMID: 17962457]
Level 2 (mid-level) evidenceOlthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005 Jun:112(6):953-61 [PubMed PMID: 15885795]
Osterberg L, Blaschke T. Adherence to medication. The New England journal of medicine. 2005 Aug 4:353(5):487-97 [PubMed PMID: 16079372]