Introduction
Gas gangrene is synonymous with myonecrosis and is a highly lethal infection of deep soft tissue caused by Clostridium species. Clostridium perfringens is the most common (see Image. Gas Gangrene of a Diabetic Foot). Clostridial myonecrosis historically was a common war wound infection with an incidence of 5%. Still, with improvement in wound care, antisepsis, and the use of antibiotics, the incidence has fallen to 0.1% of war-related wound infections since the Vietnam War era. Puncture and surgical wounds, especially GI surgeries done on the biliary tract or intestinal surgeries, are causes of clostridial infections due to inadvertent inoculation of the surgical wound with gut bacteria.[1][2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Clostridial infections usually arise in traumatized tissue but also can arise spontaneously. The infection involves deeper tissue, such as a muscle, which can lead to a rapidly spreading infection along tissue planes, and patients often present with sepsis. The infection may develop hours to weeks after the initial trauma and inoculation. The inoculation of the bacteria does not always cause gas gangrene, and there are host and organism factors that determine the progression to infection. Immunocompromised patients and those with local tissue hypoxia (due to trauma or poor vascular supply) are most at risk. The most common organisms that cause these infections are Clostridium perfringens, Clostridium septicum, and Clostridium histolyticum. C. septicum is the most common cause of spontaneous gas gangrene associated with G.I. abnormalities, such as colon cancer. C. perfringens and C. histolyticum are more commonly associated with post-traumatic infections.[3][4]
More recently, in the literature, Clostridium sordellii, an uncommon pathogen, has been reported to cause fatal shock syndrome and gas gangrene of the uterus after medical abortion with oral mifepristone and vaginal misoprostol. Clostridium sordellii is also on the rise associated with the use of black tar heroin injections, more commonly referred to as “popping.” This organism has also had increased incidence as the cause of deep tissue infections associated with childbirth and infections after gynecologic procedures, including septic abortions, which can cause gas gangrene of the uterus.[1][5][6]
Epidemiology
In the United States, the incidence of myonecrosis is only about 1000 cases per year. The incidence is probably higher in less developed countries with decreased access to healthcare and antibiotics, but the exact number is unknown. With the best of care, including early recognition, surgical care, antibiotic treatment, and hyperbaric oxygen therapy, the overall mortality rate is 20% to 30% and, in some studies, as low as 5% to 10%; however, if not treated, the disease has a 100% fatality. Host factors such as an immunocompromised state, diabetes mellitus, and spontaneous infections can have higher mortality rates of 67% or higher. If the infection involves the abdominal soft tissue or chest wall, the mortality rate can be as high as 60% compared to extremity infections with more favorable mortality of 5% to 30%.[7][8]
Pathophysiology
C. perfringens causes 80% to 90% of gas gangrene cases, but other species can cause infection. In order of prevalence, they are Clostridium novyi (40%), C. septicum (20%), C. histolyticum (10%), Clostridium bifermentans (10%), Clostridium fallax (5%), and C. sordellii. These organisms are in the soil and organic waste, especially if contaminated with fecal material.
Healthcare workers should suspect gas gangrene if anaerobic gram-positive bacilli are present in a wound with necrosis of soft tissue and muscle. The organisms produce a gas identifiable on X-ray or CT scans. Only about 5% of the wounds colonized with clostridial organisms develop an infection. Therefore, host factors and the anatomic location of the organism's injection help determine whether the bacteria develop into a clostridial myonecrosis infection. For example, a deep penetrating wound into muscle tissue where the host is immunocompromised is more likely to develop an infection than a host with a healthy immune system and good nutritional status. More open superficial wounds are less likely to become infected, especially if properly cleaned and dressed, compared to deeper penetrating wounds or wounds with crush injury and tissue ischemia.[9]
The clostridial organisms produce alpha and theta toxins that cause extensive tissue damage. The infection can spread quickly, and within a matter of several hours, the patient may develop overwhelming shock, sepsis, and death. A better-oxygenated tissue with 70mmHg oxygen tension inhibits the organism's growth because clostridial species are facultative anaerobes. A facultative anaerobe is an organism that makes ATP by aerobic respiration if oxygen is present but can switch to fermentation if oxygen is absent. If the oxygen tension of the tissue is less than 30 mm Hg, the clostridial organisms grow more quickly. The infection can develop slowly over weeks or rapidly over hours, depending on the oxygen tension of the tissue and the amount of organisms inoculated.[10]
The virulence of the organism depends on the exotoxins produced; Clostridium perfringens is the most pathologic with 17 known toxins, with the most toxic being the alpha-toxin, a lecithinase. Alpha toxin is a phospholipase (lecithinase) that breaks down cell membranes, triggering platelet aggregation, thrombosis, and histamine release. Also present are collagenase, hyaluronidase, hemagglutinins, and hemolysins. Theta toxins cause direct vascular injury and breakdown of leukocytes, causing a blunted host inflammatory response to the infection. Collagenase breaks down connective tissue, allowing the organism to spread rapidly across tissue planes. This is 1 of the main reasons the infection can cross over connective tissue plains, spreading into the deeper muscle tissues.[5][11][12]
Histopathology
Clostridium's Gram stain shows large gram-positive rods with a paucity of leukocytes (as is typical of anaerobic infections).
Toxicokinetics
Common toxins produced by C. perfringens:
- Alpha toxin: Lecithinase (or phospholipase) that breaks down cell membranes, resulting in cell death and tissue necrosis. This toxin is also hemolytic and cardiotoxic.
- Beta toxin: Necrosis of tissue
- Delta toxin: Hemolysin
- Epsilon toxin: Acts to increase cell membrane permeability; permease.
- Iota toxin: Necrosis of tissue
- Kappa toxin: Collagenase, gelatinase, and necrosis of tissue. It especially destroys blood vessels and connective tissue.
- Lambda toxin: Protease
- Mu toxin: Hyaluronidase
- Nu toxin: Deoxyribonuclease, hemolytic and necrosis of tissue
- Phi toxin: Hemolysin, cytolysin[13]
History and Physical
Patients with gas gangrene (myonecrosis) present with signs of infection such as fever, chills, pain, and less superficial inflammation at the site of infection than one would expect, given the deep penetrating nature of these infections. The condition of the patient can rapidly progress to sepsis and death if not treated aggressively. The wound discharge is often dishwater-looking with a musty order. It can involve the vasculature that supplies large areas of infected tissue, leading to subcutaneous fat necrosis down to the fascia and extending into the deeper muscle. If the nerves are damaged, the severity of the pain is less than expected for the extent of infection. The drainage from the necrotic tissue often has a dishwater appearance and musty order. Signs of severe sepsis include septic shock, adult respiratory distress syndrome, disseminated intravascular coagulation, and hemolysis, which may cause hemolytic anemia, which is often how patients present. Any patient with a cellulitis infection who develops additional signs of crepitus secondary to gas in the tissue and necrotic or dusky-looking skin should be evaluated for gas gangrene.[14][15][16]
Evaluation
Immediate workup of a patient with suspected gas gangrene includes CBC, CMP, urinalysis, PT, APTT, blood, and wound cultures. Additional blood tests such as ABG, lactic acid, and pre-calcitonin can be helpful in the evaluation of sepsis, which is often present in gas gangrene. Common imaging studies include X-rays, CT scans of the infected body part, and ultrasound. These can help identify the extent of the infection, abscess, and gas in the tissues. See Image. Gas Gangrene. Extensive lab and imaging should not delay definitive surgical debridement of the necrotic tissue. During the initial surgical debridement, a deep-wound aerobic and anaerobic culture can help determine the causative organism and direct antibiotic therapy.[17]
Treatment / Management
Because the infection is rapidly progressive, it is important to treat patients aggressively with antibiotics, early surgical consultation with debridement, intravenous fluid resuscitation, ICU monitoring, and adjuvant hyperbaric oxygen therapy. Getting early surgical consultation without delay is important as this is a true surgical emergency. Providers should not delay antibiotics to get cultures but begin empiric treatment with antibiotics. Reasonable broad-spectrum coverage includes vancomycin, tazobactam, a carbapenem, or ceftriaxone with metronidazole. If the provider suspects gas gangrene or a necrotizing soft tissue infection, penicillin plus clindamycin should be added, which treats group A streptococcal necrotizing fasciitis. Clindamycin should be strongly considered because it inhibits the synthesis of clostridial exotoxins and lessens the systemic effects of these toxins. Because clindamycin is bacteriostatic and not bactericidal, it should be used with a second anti-microbial, such as penicillin.[18][19][20][21][22](A1)
Fasciotomy may be necessary to relieve compartment pressures. As the infection progresses into deep tissue along and under the fascia, compartment pressures increase, perpetuating further tissue ischemia and necrosis. Surgical debridement should focus on removing all the necrotic tissue and foreign bodies, such as soil, debris, and shrapnel. Irrigating the wounds with copious amounts of sterile normal saline is also important. Hyperbaric oxygen therapy should be added to standard antibiotics and surgical debridement therapy to help improve survival.[22][23] It is important to have coordinated care of these critically ill patients with an intensivist, general surgeon, orthopedic surgeon, urologist (in the setting of Fournier’s gangrene of the testicles and perineal structures), gynecologist (in the setting of uterine gas gangrene), infectious disease specialist, hematologist/oncologist, gastroenterologist (in the setting of spontaneous gas gangrene), and hyperbaric oxygen therapy specialist. The consultation flow usually starts with an emergency department provider and early disease recognition.[24][25][24](B3)
Early IV antibiotics with early surgical debridement followed by hyperbaric oxygen therapy can salvage patients with an otherwise nearly always fatal disease. Intravenous antibiotics and early surgical debridement of the necrotic tissue reduce the fatality rate to about 30%. Hyperbaric oxygen therapy can reduce this to 5 to 10%. Hyperbaric oxygen therapy helps by halting exotoxin production by the bacteria, helps to improve the bactericidal effect of the antibiotic, treats the tissue ischemia, improves reperfusion injury of the tissue, and promotes the activation and migration of stem cells and polymorphonuclear cells. Additionally, hyperbaric oxygen induces vasoconstriction, reducing tissue edema while augmenting oxygenation. The oxygen tension of the tissue increases by a factor of 1000, and this increased oxygen in the tissue helps to resolve hypoxia, improve cellular activity, inhibit bacterial growth, and affect cytokinesis, which increases the migration of neutrophils to the injured tissue. Hyperbaric oxygen also increases the production of growth factors such as vascular epidermal growth factor, which induces neovascularization and tissue repair with capillary budding. This is recognized clinically as increased granulation tissue formation and is usually seen after several hyperbaric oxygen treatments.[26][27][28][27](A1)
Hyperbaric oxygen therapy involves placing the patient in a pressurized chamber, which can be mono-place (single patient) or multi-place (multiple patients treated simultaneously). The mono-place chamber can only treat 1 patient at a time, and the attendant is outside the chamber with specialized equipment and pumps to run IVs and even mechanical ventilation equipment through ports in the chamber door or wall. The disadvantage of this setup is that it limits the therapies available in the chamber. If the patient requires direct contact with the attendant, the chamber has to be depressurized, and the patient is taken out of the chamber. The multi-place chamber has the added benefit of being able to treat multiple patients at the same time, and the attendant is in the chamber with the patients, allowing easier access to the patient for ventilator support, IV therapy, placement of a chest tube, or needle decompression of a pneumothorax. The treatment pressure for gas gangrene is 3 atmospheres absolute. The patient has air brakes every half hour to help reduce the risk of oxygen toxicity. These air brakes are usually 5 to 10 minutes in duration. The treatment at pressure is usually about 90 minutes, with 10 minutes for descent and 10 minutes for the ascent.[24][29][30][24](B3)
When treating gas gangrene, the treatments start twice a day for the first 5 to 10 treatments, reducing to once-daily treatments when stabilized. Continuing hyperbaric oxygen therapy beyond the initial stabilization can speed tissue healing and preparation for eventual tissue grafting, often necessary to close the large defects left after surgical debridement of dead tissue. The risk of hyperbaric oxygen therapy includes oxygen toxicity, which can cause seizures, hypoglycemia, especially in insulin-dependent diabetics, and barotrauma, which can affect the ears, lungs, or any gas-filled structures, such as the stomach, and gas embolism. These complications are rare, except for ear barotrauma, which occurs approximately 43% of the time (84% of these are minor injections of the tympanic membrane).
It is crucial to get early surgical consultation without delay in the case of gas gangrene, as this is an immediate emergency. Broad-spectrum antibiotics should be initiated without any delay in getting cultures. Reasonable coverage should include vancomycin, tazobactam, or a carbapenem, or a third-generation cephalosporin (ceftriaxone) with metronidazole. Moreover, in case of any suspicion of gas gangrene or necrotizing fascitis, penicillin plus clindamycin should be added to cover group A streptococcal necrotizing fasciitis. Clindamycin is strongly recommended. Adjunctive measures in the treatment of gas gangrene include hyperbaric oxygen (HBO) therapy. The function of the existing toxin is not affected by hyperbaric oxygen therapy; thus, debridement is of paramount importance. Hemodynamically unstable patients may not be candidates for HBO therapy. Moreover, animal experimental studies in animals failed to document the therapeutic efficacy of HBO.[31][32][23] Providers should consider using negative pressure wound dressing therapy once adequate surgical debridement has resolved ongoing tissue necrosis.(B3)
Differential Diagnosis
The differential for gas gangrene includes the following:
- Abdominal abscess
- Abdominal trauma
- Bacteria sepsis
- Elective abortion
- Emphysematous cholecystitis
- Group A streptococcal infections
- Septic shock
- Toxic shock syndrome
- Vibrio infection[33]
Postoperative and Rehabilitation Care
Patients with gas gangrene need daily or repeated surgical debridement until the necrotizing infection is controlled and receive twice-daily hyperbaric oxygen therapy until tissue necrosis stops and signs of tissue recovery with granulation tissue formation occur. The patient also needs ongoing intensive care and may require hemodialysis for renal failure and extracorporeal membrane oxygenation for patients with severe adult respiratory distress syndrome. Once the infection resolves, many patients require further wound care, often with negative pressure wound therapy, advanced tissue regeneration techniques, and plastic surgical therapies such as skin grafting and flap procedures to close the surgical wounds. Many patients with gas gangrene required prolonged ICU stays, followed by long rehab to improve survival and restore function. Many patients require transfer to a long-term care facility for ongoing wound care, sometimes hyperbaric oxygen therapy, and therapeutic rehab programs with physical therapy and occupational therapy.[34][35]
Pearls and Other Issues
To enhance patient survival and reduce morbidity in gas gangrene, this diagnosis should be high on the differential if the patient presents with infection with signs of necrotic tissue, sepsis, or if gas is present in the tissue. It is important to diagnose early, consult surgery for emergent debridement, and transfer patients with gas gangrene to facilities that have the capability of taking care of such ill patients. They require coordinated care between surgery, intensive care, and hyperbaric oxygen/wound care.[36][37]
Enhancing Healthcare Team Outcomes
Best outcomes are achieved with coordinated care between multiple specialties and intensive care in a facility with personnel competent in caring for critically ill patients. Care has to be coordinated between the surgeons doing the debridements, the wound care/hyperbaric oxygen providers, and the intensivist. Photo documentation in the electronic health record helps improve coordination of care. The surgical team can take pictures in the operating room, and the wound care team can also take pictures when doing dressing changes. This helps nurses and other specialties, such as plastic surgery and infectious disease, know the progress and helps guide decisions. Rehabilitation should start as soon as the patient can, reducing the risk of blood clots and muscle atrophy. The care team effort must be coordinated so that everyone is on the same page regarding expectations of outcomes. There needs to be peer review and evaluation of team performance for the improvement of patient care in a non-hostile and supportive manner so that all team members are able and willing to contribute to improved patient care.[14][38][39]
Media
(Click Image to Enlarge)

Gas Gangrene of a Diabetic Foot. Gas-producing gram-negative organisms are also common in diabetic foot infections.
Contributed by H Murphy-Lavoie, MD
(Click Image to Enlarge)
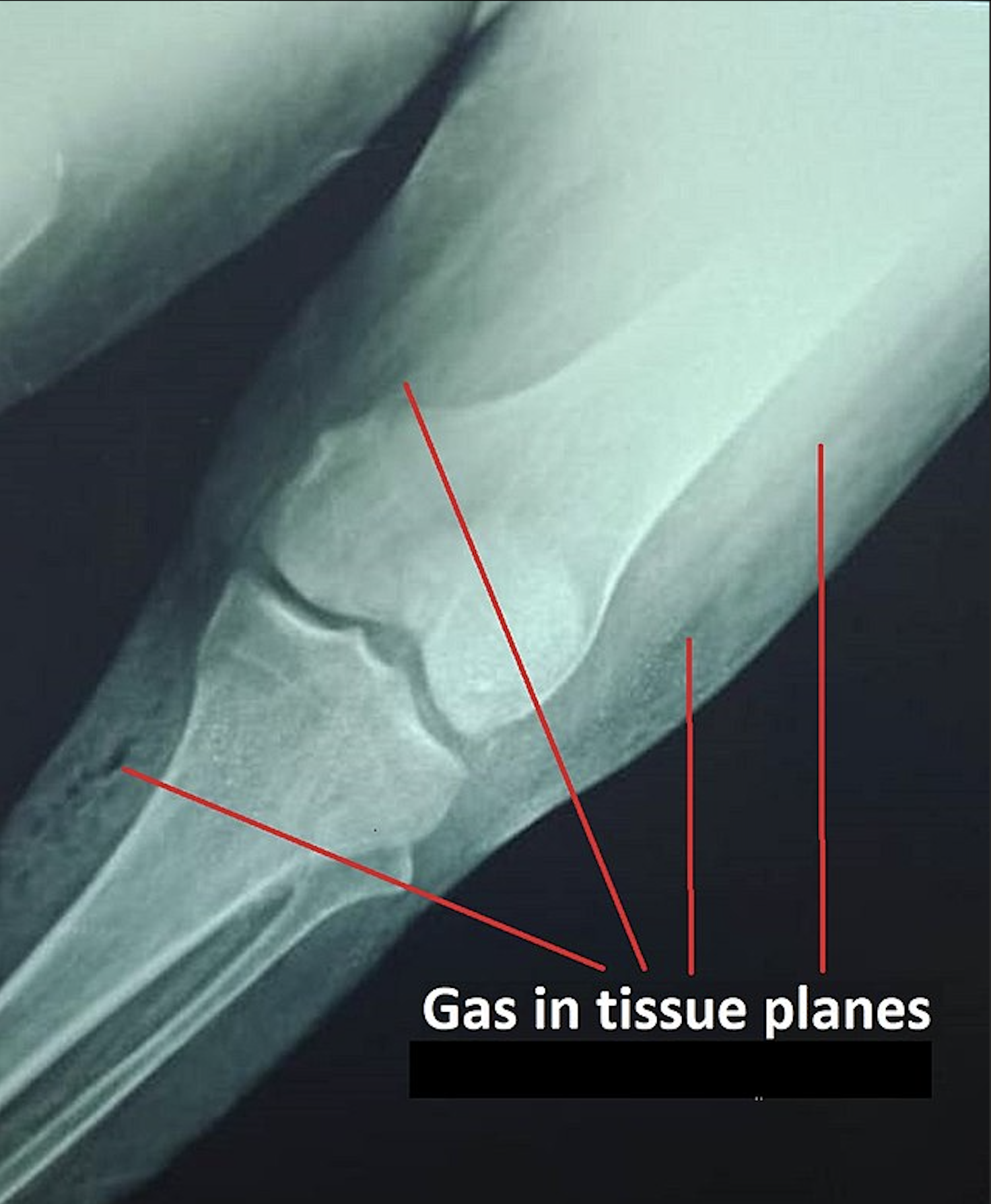
Gas Gangrene. Plain x-ray showing gas in the tissue planes in a patient with gas gangrene.
شہاب, Public Domain, via Wikimedia Commons
References
Takehara M. [Host Defense against Bacterial Infection and Bacterial Toxin-induced Impairment of Innate Immunity]. Yakugaku zasshi : Journal of the Pharmaceutical Society of Japan. 2018:138(10):1249-1253. doi: 10.1248/yakushi.18-00102. Epub [PubMed PMID: 30270267]
Stevens DL, Aldape MJ, Bryant AE. Life-threatening clostridial infections. Anaerobe. 2012 Apr:18(2):254-9. doi: 10.1016/j.anaerobe.2011.11.001. Epub 2011 Nov 20 [PubMed PMID: 22120198]
Huang YY, Lin CW, Yang HM, Hung SY, Chen IW. Survival and associated risk factors in patients with diabetes and amputations caused by infectious foot gangrene. Journal of foot and ankle research. 2018:11():1. doi: 10.1186/s13047-017-0243-0. Epub 2018 Jan 4 [PubMed PMID: 29312468]
Perkins TA, Bieniek JM, Sumfest JM. Solitary Candida albicans Infection Causing Fournier Gangrene and Review of Fungal Etiologies. Reviews in urology. 2014:16(2):95-8 [PubMed PMID: 25009452]
Dempsey A. Serious infection associated with induced abortion in the United States. Clinical obstetrics and gynecology. 2012 Dec:55(4):888-92. doi: 10.1097/GRF.0b013e31826fd8f8. Epub [PubMed PMID: 23090457]
Stevens DL, Bryant AE. Necrotizing Soft-Tissue Infections. The New England journal of medicine. 2017 Dec 7:377(23):2253-2265. doi: 10.1056/NEJMra1600673. Epub [PubMed PMID: 29211672]
Shindo Y, Dobashi Y, Sakai T, Monma C, Miyatani H, Yoshida Y. Epidemiological and pathobiological profiles of Clostridium perfringens infections: review of consecutive series of 33 cases over a 13-year period. International journal of clinical and experimental pathology. 2015:8(1):569-77 [PubMed PMID: 25755747]
Level 2 (mid-level) evidenceLehnhardt M, Homann HH, Daigeler A, Hauser J, Palka P, Steinau HU. Major and lethal complications of liposuction: a review of 72 cases in Germany between 1998 and 2002. Plastic and reconstructive surgery. 2008 Jun:121(6):396e-403e. doi: 10.1097/PRS.0b013e318170817a. Epub [PubMed PMID: 18520866]
Level 2 (mid-level) evidenceTakazawa K, Otsuka H, Nakagawa Y, Inokuchi S. Clinical Features of Non-clostridial Gas Gangrene and Risk Factors for In-hospital Mortality. The Tokai journal of experimental and clinical medicine. 2015 Sep 20:40(3):124-9 [PubMed PMID: 26369267]
Janik E, Ceremuga M, Saluk-Bijak J, Bijak M. Biological Toxins as the Potential Tools for Bioterrorism. International journal of molecular sciences. 2019 Mar 8:20(5):. doi: 10.3390/ijms20051181. Epub 2019 Mar 8 [PubMed PMID: 30857127]
Srivastava I, Aldape MJ, Bryant AE, Stevens DL. Spontaneous C. septicum gas gangrene: A literature review. Anaerobe. 2017 Dec:48():165-171. doi: 10.1016/j.anaerobe.2017.07.008. Epub 2017 Aug 2 [PubMed PMID: 28780428]
Crum-Cianflone NF. Infection and musculoskeletal conditions: Infectious myositis. Best practice & research. Clinical rheumatology. 2006 Dec:20(6):1083-97 [PubMed PMID: 17127198]
Carter GP, Cheung JK, Larcombe S, Lyras D. Regulation of toxin production in the pathogenic clostridia. Molecular microbiology. 2014 Jan:91(2):221-31 [PubMed PMID: 24563915]
Garcia NM, Cai J. Aggressive Soft Tissue Infections. The Surgical clinics of North America. 2018 Oct:98(5):1097-1108. doi: 10.1016/j.suc.2018.05.001. Epub 2018 Jul 29 [PubMed PMID: 30243450]
Roberts EJ, Martucci JA, Wu D. The Unusual Presence of Gas From a Puncture Wound: A Case Report. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2018 Jul-Aug:57(4):785-789. doi: 10.1053/j.jfas.2017.11.003. Epub 2018 Mar 21 [PubMed PMID: 29571810]
Level 3 (low-level) evidenceCristoferi G, Fabris G, Ronconi AM, Bozza F, Gallassi GC, Bucca D, Caria GM, Duodeci S. [Gas gangrene. Clinical considerations, prognosis and therapeutic prospects in our experience]. Journal de chirurgie. 1991 May:128(5):243-6 [PubMed PMID: 1880179]
Sarvari KP, Vasas B, Kiss I, Lazar A, Horvath I, Simon M, Peto Z, Urban E. Fatal Clostridium perfringens sepsis due to emphysematous gastritis and literature review. Anaerobe. 2016 Aug:40():31-4. doi: 10.1016/j.anaerobe.2016.03.011. Epub 2016 Mar 30 [PubMed PMID: 27036998]
Finsterer J, Hess B. Neuromuscular and central nervous system manifestations of Clostridium perfringens infections. Infection. 2007 Dec:35(6):396-405 [PubMed PMID: 18034207]
Nichols RL, Smith JW. Anaerobes from a surgical perspective. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1994 May:18 Suppl 4():S280-6 [PubMed PMID: 8086576]
Level 3 (low-level) evidenceShin SH, Park IK, Kang JW, Lee YS, Chung YG. Vacuum-Assisted Closure (VAC) Using Multiple Foam Pieces for Hidden Space Drainage through Less Exposure in Musculoskeletal Infections. The journal of hand surgery Asian-Pacific volume. 2018 Sep:23(3):369-376. doi: 10.1142/S242483551850039X. Epub [PubMed PMID: 30282543]
Yang Z, Hu J, Qu Y, Sun F, Leng X, Li H, Zhan S. Interventions for treating gas gangrene. The Cochrane database of systematic reviews. 2015 Dec 3:2015(12):CD010577. doi: 10.1002/14651858.CD010577.pub2. Epub 2015 Dec 3 [PubMed PMID: 26631369]
Level 1 (high-level) evidenceDevaney B, Frawley G, Frawley L, Pilcher DV. Necrotising soft tissue infections: the effect of hyperbaric oxygen on mortality. Anaesthesia and intensive care. 2015 Nov:43(6):685-92 [PubMed PMID: 26603791]
Bakker DJ. Clostridial myonecrosis (gas gangrene). Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2012 May-Jun:39(3):731-7 [PubMed PMID: 22670554]
Level 3 (low-level) evidenceMathieu D, Marroni A, Kot J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving and hyperbaric medicine. 2017 Mar:47(1):24-32. doi: 10.28920/dhm47.1.24-32. Epub [PubMed PMID: 28357821]
Level 3 (low-level) evidenceGacto-Sanchez P. Surgical treatment and management of the severely burn patient: Review and update. Medicina intensiva. 2017 Aug-Sep:41(6):356-364. doi: 10.1016/j.medin.2017.02.008. Epub 2017 Apr 26 [PubMed PMID: 28456441]
Pruskowski KA. Pharmacokinetics and Pharmacodynamics of Antimicrobial Agents in Burn Patients. Surgical infections. 2021 Feb:22(1):77-82. doi: 10.1089/sur.2020.375. Epub 2020 Nov 6 [PubMed PMID: 33164665]
Ramos G, Cornistein W, Cerino GT, Nacif G. Systemic antimicrobial prophylaxis in burn patients: systematic review. The Journal of hospital infection. 2017 Oct:97(2):105-114. doi: 10.1016/j.jhin.2017.06.015. Epub 2017 Jun 16 [PubMed PMID: 28629932]
Level 1 (high-level) evidenceBarone M, Grani G, Ramundo V, Garritano T, Durante C, Falcone R. Fournier's gangrene during lenvatinib treatment: A case report. Molecular and clinical oncology. 2020 Jun:12(6):588-591. doi: 10.3892/mco.2020.2031. Epub 2020 Apr 10 [PubMed PMID: 32337042]
Level 3 (low-level) evidenceChantre C, Foucher S, Le Hot H, Lefort H, Blatteau JÉ. [Hyperbaric oxygen therapy, a little-known discipline]. Revue de l'infirmiere. 2018 Jun-Jul:67(242):14-15. doi: 10.1016/j.revinf.2018.03.012. Epub [PubMed PMID: 29907169]
Burman F. Low-pressure fabric hyperbaric chambers. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 2019 Mar 29:109(4):12574. doi: 10.7196/SAMJ.2019.v109i4.13524. Epub 2019 Mar 29 [PubMed PMID: 31084683]
Heyboer M 3rd. Hyperbaric Oxygen Therapy Side Effects - Where Do We Stand? The journal of the American College of Clinical Wound Specialists. 2016:8(1-3):2-3. doi: 10.1016/j.jccw.2018.01.005. Epub 2018 Feb 5 [PubMed PMID: 30276115]
Clark LA, Moon RE. Hyperbaric oxygen in the treatment of life-threatening soft-tissue infections. Respiratory care clinics of North America. 1999 Jun:5(2):203-19 [PubMed PMID: 10333449]
Chernyadyev SA, Ufimtseva MA, Vishnevskaya IF, Bochkarev YM, Ushakov AA, Beresneva TA, Galimzyanov FV, Khodakov VV. Fournier's Gangrene: Literature Review and Clinical Cases. Urologia internationalis. 2018:101(1):91-97. doi: 10.1159/000490108. Epub 2018 Jun 27 [PubMed PMID: 29949811]
Level 3 (low-level) evidenceChen SY, Fu JP, Wang CH, Lee TP, Chen SG. Fournier gangrene: a review of 41 patients and strategies for reconstruction. Annals of plastic surgery. 2010 Jun:64(6):765-9. doi: 10.1097/SAP.0b013e3181ba5485. Epub [PubMed PMID: 20407363]
Level 2 (mid-level) evidenceMcGinness K, Kurtz Phelan DH. Use of Viable Cryopreserved Umbilical Tissue for Soft Tissue Defects in Patients With Gas Gangrene: A Case Series. Wounds : a compendium of clinical research and practice. 2018 Apr:30(4):90-95 [PubMed PMID: 29718818]
Level 2 (mid-level) evidenceIngraham AM, Jung HS, Liepert AE, Warner-Hillard C, Greenberg CC, Scarborough JE. Effect of transfer status on outcomes for necrotizing soft tissue infections. The Journal of surgical research. 2017 Dec:220():372-378. doi: 10.1016/j.jss.2017.06.006. Epub 2017 Sep 1 [PubMed PMID: 29180205]
Mills MK, Faraklas I, Davis C, Stoddard GJ, Saffle J. Outcomes from treatment of necrotizing soft-tissue infections: results from the National Surgical Quality Improvement Program database. American journal of surgery. 2010 Dec:200(6):790-6; discussion 796-7. doi: 10.1016/j.amjsurg.2010.06.008. Epub [PubMed PMID: 21146022]
Level 2 (mid-level) evidenceRoloff D. [Prerequisites for the transfer of patients with gas gangrene to a specialized facility]. Anaesthesiologie und Reanimation. 1991:16(1):49-58 [PubMed PMID: 2043237]
Sison-Martinez J, Hendriksen S, Cooper JS. Hyperbaric Treatment of Clostridial Myositis and Myonecrosis. StatPearls. 2025 Jan:(): [PubMed PMID: 29763178]