
Introduction
Siphonaptera, more commonly known as fleas, are an order of wingless arthropods with more than 2000 species. Fleas live as ectoparasites on warm-blooded species, consuming their blood. They are small, ranging from 1.0 to 3.3 mm in size, and have long hind legs adapted for jumping. Fleas are natural jumpers (relative to body size) that can jump 100 times their length. Fleas are ubiquitous parasites that lack specificity towards their hosts. The cat flea, Ctenocephalides felis, is the most prevalent parasite on dogs. In certain regions, the human flea, Pulex irritans, is prevalent as a dog parasite. The human flea is also detected in wild animals with no human contact. Fleas of the genus Ctenocephalides have 2 ctenidia (combs) that resemble a mane of hair (pronotal comb) and a mustache (genal comb).
Though fleas survive in many environments, they are rare in low-humidity environments and elevations over 1500 ft.[1] Fleas are predominantly a nuisance to their host, causing pruritic local reactions. They can also act as vectors for typhus, rickettsial disease, bubonic plague, protozoan, and helminth infestations. Understanding these features can help direct history-taking, the physical exam, and treatment options. Additionally, exploring eradication techniques within the human environment can help reduce the spread of disease from fleas to humans.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Fleas have large, powerful hind legs, enabling them to jump horizontally or vertically 200 times their body length (equivalent to a 6-foot human jumping 1200 feet) using stored muscle energy in a pad on the hind legs composed of the elastic protein resilin. They feed off various hosts, including humans, pigs, cats, dogs, goats, sheep, cattle, chickens, owls, foxes, rabbits, mice, and feral cats. The flea's mouthparts are highly specialized for piercing the skin and sucking its blood meal via direct capillary cannulation. The adult human flea (P. irritans) is a small, reddish brown, laterally compressed, wingless insect approximately 2 to 3.5 mm long (females, 2.5 to 3.5 mm; males, 2 to 2.5 mm) and enclosed by a rigid cuticle. Compared to the dog flea (Ctenocephalides canis) and cat flea (Ctenocephalides felis), P. irritans has no combs or ctenidia.[3] The sticktight flea, Echidnophaga gallinacea, gets its name from its ability to attach its head to the host's skin via wide and serrated laciniae, allowing it to feed at a single location for 19 days. This flea can be distinguished from dog and cat fleas by its lack of genal and promotal ctenidia and smaller size than a cat flea. The organism possesses 2 pairs of setae behind the antennae and has a head that is flattened towards the front. The sticktight flea, also known as the stickfast or chicken flea, primarily infests poultry but has been discovered in several kinds of birds and mammals, including humans.[4]
Epidemiology
Fleas are prevalent among mammals worldwide. In the developed world, the most influential vectors are household pets, specifically cats and dogs.[5] Fleas significantly cause papular urticaria in the developing world, especially in tropical regions, with a frequency of 2.4% to 16.3% in pediatric patients. While other insects can also cause a similar rash, fleas are among the most frequent causes. In most patients, the rash improves by age 7, though in some cases, it can last into adulthood.[6] Due to diseases such as the bubonic plague, fleas have claimed more victims than all the wars in human history; in the 14th century, the Black Death caused more than 200 million deaths. Tungiasis is a parasitic flea infestation in tropical and subtropical climates, including Africa, South America, and Central America, and is most common in underdeveloped and impoverished regions. Though rare in the United States and Europe despite global travel, it should be considered for patients returning from endemic areas. Peak incidence occurs during the dry season months between August and September.[7]
Pathophysiology
The flea life cycle consists of 4 stages: egg, larva, pupa, and adult. Adult flea species often mate on the host, with the female producing an average of 4 to 8 small white eggs after each blood meal, totaling more than 400 eggs in her lifetime. After being dropped by the host, the eggs hatch into larvae in around 4 to 6 days. The larvae are actively consuming organic material in their surroundings, including their parents' waste and debris, while going through 3 molts over a period ranging from a week to many months. Next, the larva spins a silk cocoon using specialized salivary glands to become a pupa. In ideal settings, the pupa has a short lifespan of a few weeks but can endure for a year or longer in unfavorable circumstances. Factors that cause adult fleas to emerge from the pupa stage include high humidity, warm temperatures, elevated carbon dioxide levels, and vibrations such as sound. An adult P. irritans flea can survive for a few weeks to over 1.5 years in optimal conditions characterized by low air temperatures, high relative humidity, and the availability of a host.
Most flea bites result in:
- Papular urticaria is a dual Type I and Type IV hypersensitivity reaction. The reactions involve both IgE and cell-mediated responses. This rash appears as small, raised, erythematous, and pruritic lesions. The rash most commonly affects exposed skin, generally the feet and ankles, and appears in clusters and linear patterns known as a "breakfast, lunch, and dinner" pattern.[8][9]
- Tungiasis is an inflammatory skin condition caused by Tunga penetrans, the smallest known flea. Skin irritation occurs when a female flea embeds itself into the skin's epithelium. Fleas typically embed themselves in soft areas of skin, such as the medial foot, under nails, and between toes. The thigh, hands, perianal, and groin may be involved in severe disease. During the first 2 days of infestation, the host may notice itching or discomfort. The abdomen of the flea then swells with eggs, forming a white, pearly lesion. This increased pressure can cause a painful foreign body sensation and irritate surrounding neurovascular structures. Following this, the lesion becomes dark and crusted, and may create a honeycomb pattern in more extensive infections, which is prone to secondary infection and increases the risk of gangrene and tetanus. After healing, scarring can occur.[7][10] The flea has many common names, including chigoe flea, jigger, nigua, pico, sand flea, and bicho de pie (bug of the foot). A white patch with a black dot in the center characterizes the lesions caused by the flea. The tunga flea is native to the West Indies and Caribbean region but has spread to Africa, India, Pakistan, and Latin America. Fleas like the warm, dry soil and sand of beaches, stables, and stock farms. The increase in travelers to endemic areas may cause the disease to appear in other countries.
Fleas can be a vector for several human diseases, including:
- Yersinia pestis is a gram-negative bacteria that causes plague, a highly virulent disease that killed millions during its 3 most significant human pandemics. Initial vectors include the black rat (Rattus rattus) and the oriental rat flea (Xenopsylla cheopis); however, transmission may occur human-to-human with pneumonic plague, while septicemic plague may be spread via Pulex fleas or body lice.
- Lice, ticks, and fleas spread Bartonellosis, caused by different species of gram-negative intracellular bacteria from the genus Bartonella. Bartonella quintana causes trench fever, primarily transmitted by the human body louse Pediculus humanus corporis, and resulted in more than 1 million cases during World War I. Trench fever is characterized by headache, fever, dizziness, and shin pain that lasts 1 to 3 days and recurs in cycles every 4 to 6 days. Other clinical manifestations of B. quintana include chronic bacteremia, endocarditis, lymphadenopathy, and bacillary angiomatosis. Bartonella henslae causes cat scratch fever, which is characterized by lymphadenopathy, fever, headache, joint pain, and lethargy from infected cat scratches or flea bites. Bartonella rochalimae has also been found to cause trench fever-like bacteremia. Bartonella species have been found in P. irritans, and the flea is implicated as a vector of Bartonellosis in humans.
- Rickettsioses are worldwide diseases caused by the gram-negative intracellular bacteria of the genus Rickettsia, transmitted to humans via hematophagous arthropods. Rickettsiae have traditionally been classified into spotted fever or typhus groups. The spotted fever group includes Rocky Mountain spotted fever and Mediterranean spotted fever. Lice transmit the typhus group (epidemic typhus), whereas fleas transmit the endemic or murine typhus. Rickettsia typhi causes murine typhus in warm coastal areas worldwide, where the rat and the rat flea vector Xenopsylla cheopis are the main mammal reservoirs. Clinical signs of infection include an abrupt onset of fever, headaches, myalgia, malaise, chills, and a truncal maculopapular rash that progresses peripherally several days after the initial clinical signs. A rash is present in up to 50% of cases.[3] The cat flea C. felis usually transmits Rickettsia felis, an emerging flea-borne pathogen that causes an acute febrile illness.[11]
- Reports indicate that humans have contracted Dipylidium caninum, a dog tapeworm, after accidentally ingesting cat fleas carrying the parasite. Children may be more susceptible to the infection, which presents as diarrhea or white worms in their feces, possibly due to accidental flea consumption while being licked by the pet.[12]
Histopathology
Histologic sections of tungiasis contain various flea parts that may present a diagnostic dilemma for pathologists unfamiliar with this disease. Skin biopsies show the exoskeleton, hypodermal layer, trachea, digestive tract, and developing eggs. The dermis contains mixed inflammatory cell infiltrates of lymphocytes, plasma cells, and eosinophils (see Image. Tungiasis Histology).[13] The histopathologic pattern in papular urticaria consists of mild subepidermal edema, extravasation of erythrocytes, interstitial eosinophils, and exocytosis of lymphocytes. These findings suggest a pathophysiologic process that is immunologically based.[14]
History and Physical
When evaluating a patient suspected of flea bites, the provider should ask about living conditions, recent exposures, and similar symptoms in co-habitants. The physical exam should include a thorough skin examination, particularly of exposed areas such as the arms, legs, upper back, and scalp. Infested animals that have been handled or groomed may impact other body regions. Patients with flea allergies frequently experience adverse reactions to various flea species. Additionally, the exam should pursue details regarding any rashes, including duration, edema, erythema, and pruritus. Evaluation for local areas of infection, while a rare presentation, should be performed as with all skin breaks.
Bites by these arthropods are common and are usually associated with acute prurigo, and they are especially allergenic in atopic individuals, in whom they lead to papular urticaria. Unlike bites by other bloodsucking arthropods, flea and bedbug bites frequently display a pattern that identifies the offending agent, unlike other bloodsucking arthropods. The diagnosis is based on clinical observation, which shows 3 or more bites with pruritic, erythematous-edematous papules in a linear array or triangular, a few centimeters apart. This pattern is known as the "breakfast, lunch, and dinner" sign (see Image. Flea Bites Pattern).[15] There are 2 explanations (not mutually exclusive) for the lesions' pattern: prior mapping of the skin areas by the parasites and successive blood meals. Before feeding, the fleas and bedbugs mark the most favorable skin area using salivary apyrase, an anticoagulant enzyme. The enzyme's action itself can already induce local hypersensitivity. Once they have attached themselves to the human's skin, the arthropods begin their blood meal, which can be interrupted by the host's sudden movement or clothing friction. When interrupted, arthropods quickly locate another nearby site to feed, potentially promoting sequential biting.[16]
Evaluation
The diagnosis is typically based on the history and physical exam. No laboratory tests can confirm fleas as the causal agent of a rash. Confirmation of the diagnosis can be obtained by examining debris from vacuuming and bedding.[17]
Treatment / Management
Flea bites are present as intense, pruritic, urticarial, or vesicular papules that are usually located on the lower extremities but can also be present on exposed areas of the upper extremities and hands. Human fleas infect clothing, and bites can be widespread. Actions to combat fleas include:
- Identifying the flea host in areas such as the home, school, farm, work, or local environment.
- Veterinarians should examine and treat house pets. The pet's bedding should be washed and dried at high temperatures, and carpets and floors should be routinely vacuumed or cleaned to remove eggs, larvae, flea feces, or pupae.
- Killing adult fleas with insecticidal products (eg, imidacloprid, fipronil, spinosad, selamectin, lufenuron, and ivermectin) is the primary method of flea control. Using insect growth regulators such as pyriproxyfen inhibits adult reproduction and blocks the organogenesis of immature larval stages via hormonal or enzymatic actions. Combining an insecticide and an insect growth regulator appears to be most effective in synergistic actions against adult fleas and larvae. There have been reports of insecticidal resistance in the flea population, especially with pyrethroids. A professional exterminator and veterinarian should be consulted. In recalcitrant cases, evaluation for other wild mammals or birds should be performed in unoccupied areas of the home, such as the attic, crawl spaces, basements, and inside walls.[3]
Medical interventions for flea bites include the following:
- With soap and water, washing the skin exposed to flea bites.
- The bites cause a hypersensitivity reaction that results in local edema, erythema, and pruritus, which can be treated with cold packs and topical creams.
- Calamine- or pramoxine-containing lotions and topical corticosteroids effectively reduce local inflammation and pruritus.
- Oral antihistamines such as cetirizine or loratadine may also combat pruritus. When using oral H1 antihistamines, avoid applying topical antihistamines to large areas of skin to prevent systemic anticholinergic toxicity.
- Oral steroids may be an option for severe swelling.
- The rash can take several weeks to resolve. Eliminating fleas from the patient's surroundings is also imperative to stop the continuation of the rash.[17]
- Taking all precautions to prevent secondary infections like cellulitis, bacteremia, tetanus, and gangrene.
- Tungarisis is typically benign and self-limiting, particularly in returning travelers. Tungiasis will often heal independently, as the burrowed flea dies within 2 weeks and naturally sloughs off as the skin sheds. Over the next 1 to 2 weeks, while it feeds on the host's blood, the flea will lay more than 100 eggs that fall to the ground through the opening of the lesion. However, patients with extensive infestations may have complications, including loss of nails, toe deformities, and difficulty ambulating. Patients with a high risk of secondary infection and patients with extensive infections should receive treatment with prophylactic antibiotics. Unvaccinated patients face an increased risk of tetanus, so the practitioner should ask all patients about their tetanus status. Conventional therapy is the surgical extraction of the parasite under sterile conditions. No oral or topical therapy is entirely effective; however, in mild infections, even without treatment, the flea will die within 5 weeks and will be sloughed off with the skin. Basic hygiene, as well as paving roads and floors, can prevent infestations.[6][18][5]
- Treating sticktight fleas can be tricky, as they embed tightly into the host's skin. A qualified veterinarian should treat animals. Removal of attached fleas in humans requires grasping the flea firmly with tweezers and pulling it from the skin. Malathion 5% liquid or gel can be applied if the infestation is considerable.[4]
- For treating lymphadenitis caused by B. henselae, current recommendations suggest a 5-day course of oral azithromycin.
- A study of 392 strains from 17 countries in 2012 showed that the antibiotics used to treat Y. pestis were still effective. These antibiotics include doxycycline, streptomycin, gentamicin, tetracycline, trimethoprim-sulfamethoxazole, and ciprofloxacin.[19] (B3)
Differential Diagnosis
The differential diagnosis of pruritic urticaria should focus on inciting factors such as recent changes in detergents and body products and recent exposures to animals and insects. While fleas and mosquitoes are the most frequent insects associated with rashes (see Image. Flea Bite), other insects can cause similar rashes.[6][18] Additionally, consideration should be given to the possibility of anaphylaxis by exploring the involvement of other organ systems, including the gastrointestinal tract, as evidenced by vomiting or diarrhea, and the pulmonary system, as evidenced by wheezing or difficulty breathing. Anaphylaxis to insect bites, especially fleas, is very rare.
Prognosis
Flea bites typically have a benign clinical course. Most patients only experience a mild local reaction called papular urticaria. This rash resolves spontaneously and is manageable with antihistamines and anti-inflammatory medications. Secondary infections such as cellulitis and abscesses are possible and should be treated per current clinical guidelines. Fleas can be vectors for secondary infections such as Yersinia pestis, murine typhus, and parasitic infections. Secondary infection, not the flea bite, determines the prognosis for these patients.
Complications
Flea bites may appear simple, but they can be complicated by the following:
- Fleas are a critical factor in the epidemiologic cycles of several diseases, including plague and typhus. As carriers of these diseases, they can spread them to humans through their bites.[20] While there are numerous routes of transmission of the plague to humans, flea bites remain the most common. Various mammalian species are carriers of the plague, including cats, dogs, squirrels, mice, and rats.[21] Yersinia pestis, a gram-negative coccobacillus, initially manifests as regional lymphadenopathy after an invasion of the lymphatic system. These diseases are transmitted to humans through their bites. Subsequent disease progression presents itself as pneumonia, hemorrhagic lesions, purpuric skin lesions, and sepsis secondary to bacteremia.[22] Fleas, particularly the rat flea Xenopsylla cheopis, transmit murine typhus, but it also spreads through the mouse flea, Leptopsyllia segnis, and the cat flea, Ctenocephalides. Human inoculation occurs when bite wounds are contaminated with infected flea feces. In the United States, R. typhi is strongly associated with areas with large rat populations.[23] While Rickettsia felis does not cause murine typhus, the presentation of its infection is clinically indistinguishable from that of murine typhus. Manifestations include fever, headache, chills, myalgias, and other non-specific symptoms. A faint, maculopapular rash may also occur, spreading centrifugally but sparring the palms and soles.[24] Complications may occur in those with severe comorbidities, including hepatic, cardiac, pulmonary, renal, and neurologic dysfunction.[24][25][26] Patients with uncomplicated typhus may receive treatment with doxycycline, which is more effective than azithromycin.[27] Chloramphenicol may be an option as a third-line agent.[28]
- Adult female hard ticks feed on a single host for several days, whereas adult female cat fleas collect the blood required for laying eggs by multiple short-term bites on single or multiple hosts ("breakfast, lunch, and dinner sign" in humans). According to this hypothesis, cat fleas can transfer traces of α-gal-carrying glycoprotein from a previous blood meal on a cat during a further bite to an accidental human host. This can result in persistent itching, local inflammation around the bite area, and increased serum IgE to α-gal in susceptible individuals. Stenger and his colleagues presented the first case of a significant increase in α-gal serum IgE titers in the context of cat flea bites.[29]
- Secondary infections such as cellulitis and abscesses are possible. Orbital inflammatory syndrome has been reported as secondary to flea bites around the left lateral canthus.[30]
Deterrence and Patient Education
To prevent flea bites, one must avoid exposure. Using insecticidal sprays in living conditions can eliminate fleas. Flea eggs drop onto floors after being laid in animal fur, making vacuuming and cleaning paramount. Removing flea eggs from the environment halts the continuation of the flea's life cycle. Household pets, mostly cats and dogs, are common flea carriers. Flea preventatives are obtained from a veterinarian. These agents can be either topical or oral. If household pets are suspected to be the source of the infestation, consult a veterinarian.[31][32] In an environment where flea eradication is difficult or unfeasible, repellants are an option. Both DEET and thymol-containing essential oils have demonstrated effectiveness against both human (Pulex irritans) and cat (Ctenocephalides felis) fleas.
Pearls and Other Issues
Flea bites cause severe, pruritic papules mainly on the lower limbs in a characteristic breakfast, lunch, and dinner pattern. Fleas infect garments and cause widespread bites. Anti-flea measures include finding the flea host at home, school, farm, or work. Veterinarians should treat household pets. To remove eggs, larvae, flea excrement, and pupae, regularly wash and dry pet bedding at high temperatures and vacuum carpets and floors. Synergistic insecticide-insect growth regulator combinations work best against adult fleas and larvae. Evaluating additional wild creatures or birds in vacant locations such as attics, crawl spaces, basements, and walls is necessary in stubborn instances.
Enhancing Healthcare Team Outcomes
Open provider-patient communication can enhance healthcare outcomes. An interprofessional team must ask about the patient’s living environment, including animal contact, and provide tips on managing fleas and other insect infestations. Assistance may be required from extermination services and veterinarians to rid the environment of infestations. By counseling patients, the team members can help prevent discomfort from bites and spreading disease. Healthcare providers, including nurse practitioners, nurses with specialty training in dermatology, pharmacists, and the primary care provider, should provide a judgment-free space that offers a healthy exchange to educate the patient and family to facilitate the best patient care and produce the best outcomes.
Media
(Click Image to Enlarge)

Flea Bite. A flea bite with a hemorrhagic center and surrounding erythema are present.
Public Domain via Wikimedia Commons
(Click Image to Enlarge)
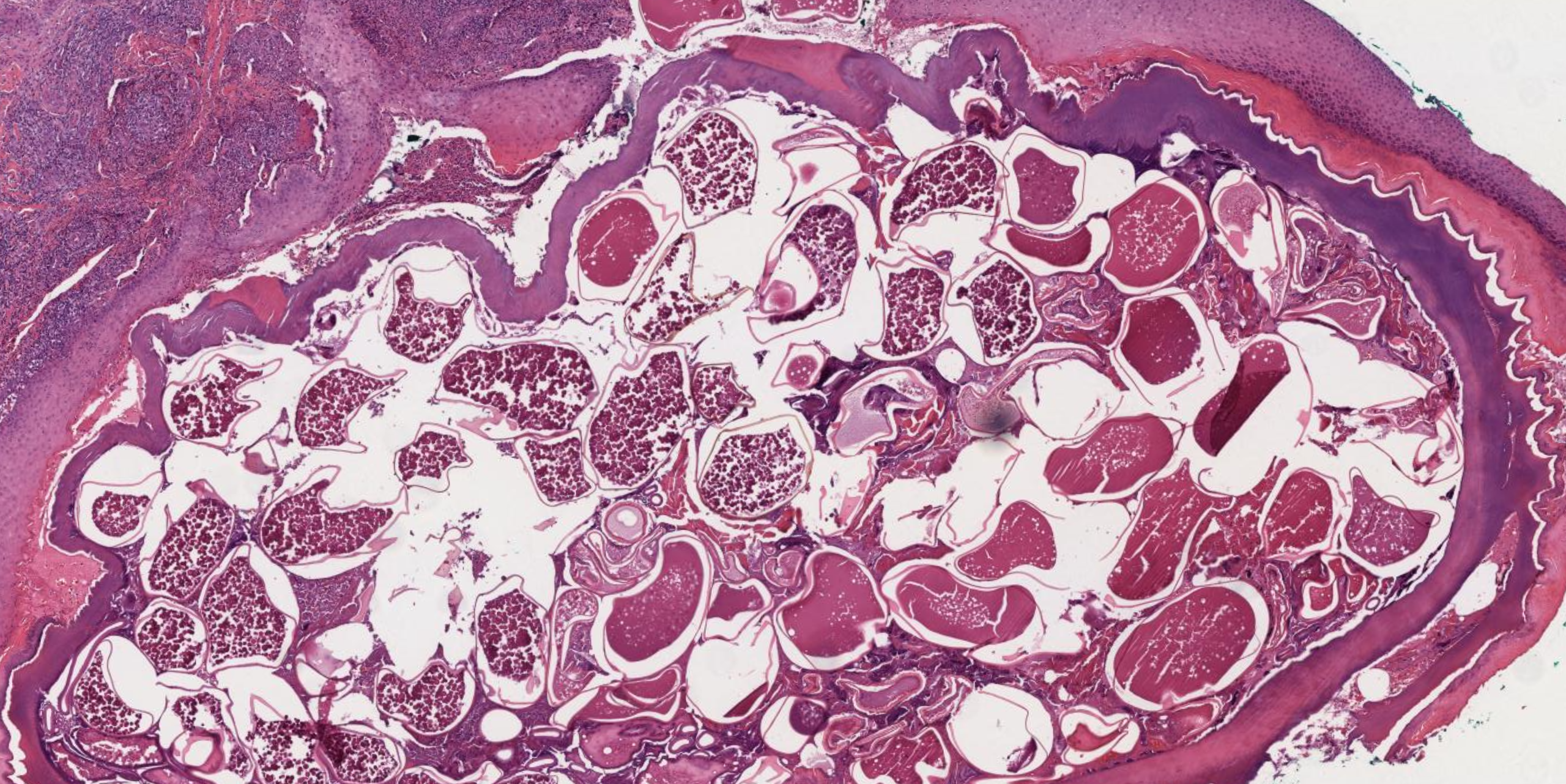
Tungiasis Histology
Contributed by N Sathe, MD
(Click Image to Enlarge)

Flea Bites Pattern. This image shows a flea bite's classic "breakfast, lunch, and dinner" pattern.
Contributed by H Saleh, MSc
References
Lam A, Yu A. Overview of flea allergy dermatitis. Compendium (Yardley, PA). 2009 May:31(5):E1-10 [PubMed PMID: 19517416]
Level 3 (low-level) evidenceJuckett G. Arthropod bites. American family physician. 2013 Dec 15:88(12):841-7 [PubMed PMID: 24364549]
Level 3 (low-level) evidenceO'Donnell M, Elston DM. What's eating you? human flea (Pulex irritans). Cutis. 2020 Nov:106(5):233-235. doi: 10.12788/cutis.0107. Epub [PubMed PMID: 33465194]
Salgado F, Elston DM. What's eating you? sticktight flea revisited. Cutis. 2017 Jul:100(1):40;49 [PubMed PMID: 28873107]
Iannino F, Sulli N, Maitino A, Pascucci I, Pampiglione G, Salucci S. Fleas of dog and cat: species, biology and flea-borne diseases. Veterinaria italiana. 2017 Dec 29:53(4):277-288. doi: 10.12834/VetIt.109.303.3. Epub [PubMed PMID: 29307121]
Halpert E, Borrero E, Ibañez-Pinilla M, Chaparro P, Molina J, Torres M, García E. Prevalence of papular urticaria caused by flea bites and associated factors in children 1-6 years of age in Bogotá, D.C. The World Allergy Organization journal. 2017:10(1):36. doi: 10.1186/s40413-017-0167-y. Epub 2017 Nov 7 [PubMed PMID: 29158868]
Sanusi ID, Brown EB, Shepard TG, Grafton WD. Tungiasis: report of one case and review of the 14 reported cases in the United States. Journal of the American Academy of Dermatology. 1989 May:20(5 Pt 2):941-4 [PubMed PMID: 2654224]
Level 3 (low-level) evidenceYoussefi MR, Ebrahimpour S, Rezaei M, Ahmadpour E, Rakhshanpour A, Rahimi MT. Dermatitis caused by Ctenocephalides felis (cat flea) in human. Caspian journal of internal medicine. 2014 Fall:5(4):248-50 [PubMed PMID: 25489439]
Level 3 (low-level) evidenceYoussefi MR, Rahimi MT. Extreme human annoyance caused by Ctenocephalides felis felis (cat flea). Asian Pacific journal of tropical biomedicine. 2014 Apr:4(4):334-6. doi: 10.12980/APJTB.4.2014C795. Epub [PubMed PMID: 25182561]
Cestari TF, Pessato S, Ramos-e-Silva M. Tungiasis and myiasis. Clinics in dermatology. 2007 Mar-Apr:25(2):158-64 [PubMed PMID: 17350494]
Brown LD, Macaluso KR. Rickettsia felis, an Emerging Flea-Borne Rickettsiosis. Current tropical medicine reports. 2016:3():27-39 [PubMed PMID: 27340613]
Jiang P, Zhang X, Liu RD, Wang ZQ, Cui J. A Human Case of Zoonotic Dog Tapeworm, Dipylidium caninum (Eucestoda: Dilepidiidae), in China. The Korean journal of parasitology. 2017 Feb:55(1):61-64. doi: 10.3347/kjp.2017.55.1.61. Epub 2017 Feb 28 [PubMed PMID: 28285500]
Level 3 (low-level) evidenceSmith MD, Procop GW. Typical histologic features of Tunga penetrans in skin biopsies. Archives of pathology & laboratory medicine. 2002 Jun:126(6):714-6 [PubMed PMID: 12033962]
Stibich AS, Schwartz RA. Papular urticaria. Cutis. 2001 Aug:68(2):89-91 [PubMed PMID: 11534921]
Peres G, Yugar LBT, Haddad Junior V. Breakfast, lunch, and dinner sign: a hallmark of flea and bedbug bites. Anais brasileiros de dermatologia. 2018 Sep-Oct:93(5):759-760. doi: 10.1590/abd1806-4841.20187384. Epub [PubMed PMID: 30156636]
Haddad Junior V, Amorim PC, Haddad Junior WT, Cardoso JL. Venomous and poisonous arthropods: identification, clinical manifestations of envenomation, and treatments used in human injuries. Revista da Sociedade Brasileira de Medicina Tropical. 2015 Nov-Dec:48(6):650-7. doi: 10.1590/0037-8682-0242-2015. Epub [PubMed PMID: 26676488]
Singh S, Mann BK. Insect bite reactions. Indian journal of dermatology, venereology and leprology. 2013 Mar-Apr:79(2):151-64. doi: 10.4103/0378-6323.107629. Epub [PubMed PMID: 23442453]
Level 3 (low-level) evidenceSteen CJ, Carbonaro PA, Schwartz RA. Arthropods in dermatology. Journal of the American Academy of Dermatology. 2004 Jun:50(6):819-42, quiz 842-4 [PubMed PMID: 15153881]
Level 3 (low-level) evidenceUrich SK, Chalcraft L, Schriefer ME, Yockey BM, Petersen JM. Lack of antimicrobial resistance in Yersinia pestis isolates from 17 countries in the Americas, Africa, and Asia. Antimicrobial agents and chemotherapy. 2012 Jan:56(1):555-8. doi: 10.1128/AAC.05043-11. Epub 2011 Oct 24 [PubMed PMID: 22024826]
Kwit N, Nelson C, Kugeler K, Petersen J, Plante L, Yaglom H, Kramer V, Schwartz B, House J, Colton L, Feldpausch A, Drenzek C, Baumbach J, DiMenna M, Fisher E, Debess E, Buttke D, Weinburke M, Percy C, Schriefer M, Gage K, Mead P. Human Plague - United States, 2015. MMWR. Morbidity and mortality weekly report. 2015 Aug 28:64(33):918-9 [PubMed PMID: 26313475]
Perry RD, Fetherston JD. Yersinia pestis--etiologic agent of plague. Clinical microbiology reviews. 1997 Jan:10(1):35-66 [PubMed PMID: 8993858]
Level 3 (low-level) evidencePrentice MB, Rahalison L. Plague. Lancet (London, England). 2007 Apr 7:369(9568):1196-207 [PubMed PMID: 17416264]
Level 3 (low-level) evidenceCiven R, Ngo V. Murine typhus: an unrecognized suburban vectorborne disease. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2008 Mar 15:46(6):913-8. doi: 10.1086/527443. Epub [PubMed PMID: 18260783]
Level 3 (low-level) evidenceTsioutis C, Zafeiri M, Avramopoulos A, Prousali E, Miligkos M, Karageorgos SA. Clinical and laboratory characteristics, epidemiology, and outcomes of murine typhus: A systematic review. Acta tropica. 2017 Feb:166():16-24. doi: 10.1016/j.actatropica.2016.10.018. Epub 2016 Oct 29 [PubMed PMID: 27983969]
Level 1 (high-level) evidenceDumler JS, Taylor JP, Walker DH. Clinical and laboratory features of murine typhus in south Texas, 1980 through 1987. JAMA. 1991 Sep 11:266(10):1365-70 [PubMed PMID: 1880866]
Vander T, Medvedovsky M, Valdman S, Herishanu Y. Facial paralysis and meningitis caused by Rickettsia typhi infection. Scandinavian journal of infectious diseases. 2003:35(11-12):886-7 [PubMed PMID: 14723370]
Level 3 (low-level) evidenceNewton PN, Keolouangkhot V, Lee SJ, Choumlivong K, Sisouphone S, Choumlivong K, Vongsouvath M, Mayxay M, Chansamouth V, Davong V, Phommasone K, Sirisouk J, Blacksell SD, Nawtaisong P, Moore CE, Castonguay-Vanier J, Dittrich S, Rattanavong S, Chang K, Darasavath C, Rattanavong O, Paris DH, Phetsouvanh R. A Prospective, Open-label, Randomized Trial of Doxycycline Versus Azithromycin for the Treatment of Uncomplicated Murine Typhus. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019 Feb 15:68(5):738-747. doi: 10.1093/cid/ciy563. Epub [PubMed PMID: 30020447]
Level 1 (high-level) evidenceShaked Y, Samra Y, Maier MK, Rubinstein E. Relapse of rickettsial Mediterranean spotted fever and murine typhus after treatment with chloramphenicol. The Journal of infection. 1989 Jan:18(1):35-7 [PubMed PMID: 2915129]
Level 2 (mid-level) evidenceStenger F, Seidel P, Schricker T, Volc S, Fischer J. Could Cat Flea Bites Contribute to a-Gal Serum IgE Levels in Humans? Journal of investigational allergology & clinical immunology. 2022 Dec 15:32(6):494-495. doi: 10.18176/jiaci.0784. Epub 2022 Jan 28 [PubMed PMID: 35088764]
Prospero Ponce CM, Malik AI, Vickers A, Chevez-Barrios P, Lee AG. Orbital Inflammatory Syndrome Secondary to Flea Bite. Ophthalmic plastic and reconstructive surgery. 2018 Jul/Aug:34(4):e115-e118. doi: 10.1097/IOP.0000000000001115. Epub [PubMed PMID: 29659432]
Rust MK. Advances in the control of Ctenocephalides felis (cat flea) on cats and dogs. Trends in parasitology. 2005 May:21(5):232-6 [PubMed PMID: 15837612]
Level 3 (low-level) evidenceRust MK. The Biology and Ecology of Cat Fleas and Advancements in Their Pest Management: A Review. Insects. 2017 Oct 27:8(4):. doi: 10.3390/insects8040118. Epub 2017 Oct 27 [PubMed PMID: 29077073]