Introduction
Fasciocutaneous flaps, also known as axial flaps, comprise skin, subcutaneous tissue, and deep fascia, devoid of muscle components. Aesthetically and functionally, these flaps possess several advantages over both musculocutaneous and muscle-only flaps due to the thin, pliable nature of the transferred tissue. Pontén's pioneering work in 1981 introduced fasciocutaneous flaps for leg reconstruction.[1] His research underscored the significance of incorporating the deep fascia for the survival of leg flaps, challenging the conventional approach of relying solely on random pattern blood supplies from the subdermal plexus. Pontén reported that with fasciocutaneous flap elevation, the length-width ratio could easily be extended from 1:1 to 2-3:1, significantly expanding reconstructive possibilities while minimizing the risk of skin necrosis.[2] Subsequently, fasciocutaneous flaps gained popularity as reliable options to cover bone and tendons in the lower leg and elsewhere.
In the following years, many more authors expanded the clinical applications and indications for fasciocutaneous flap transfer while refining the understanding of their anatomical bases. Haertsch and Barclay et al were the first to recognize that including fascia within these flaps preserves the longitudinal anastomotic vascular networks, especially the suprafascial plexus, thereby increasing flap survivability.[3][4] Cormack and Lamberty further classified fasciocutaneous flaps based on their vascularization patterns.[5] Despite advancements in techniques like perforating vessel-based flaps and microvascular free tissue transfer, fasciocutaneous flaps remain advantageous due to their simplicity and reliability, serving as valuable salvage options when other methods fail.[6]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Perfusion of fasciocutaneous flaps relies on fasciocutaneous perforating vessels, which ascend through the skin from the suprafascial (subcutaneous) plexus alongside a less developed subfascial plexus between the fascia and underlying muscle. Complementing these are subdermal and dermal plexi. These vascular networks are supplied by arteries that enter the deep fascia through underlying muscles (musculocutaneous perforators), through the septa between muscles (septocutaneous perforators), or via direct cutaneous branches (see Image. Fasciocutaneous Flap Perfusion). Dissection of the flap within the subfascial plane is technically more facile than dissection in the suprafascial plane.[7][8]
Anatomical research by Cormack and Lamberty, as well as the work of Pontén and Tolhurst et al, demonstrated that the fasciocutaneous system exhibits regional variability within the body. For example, septocutaneous vessels play a critical role in supplying the suprafascial plexus in the extremities, while musculocutaneous perforators are the main arterial source in the torso.[5][9]
Indications
Fasciocutaneous flaps are commonly employed when a soft tissue defect is too large to permit primary closure, and healing by secondary intention is not feasible. While alternative options like perforator-based or free flaps exist, fasciocutaneous flaps often offer the most expedient surgical solution. These flaps are reliable, thin, and easily mobilized, with numerous potential donor sites that maintain the primary arterial axis of the chosen flap. Unlike bulkier muscle flaps, fasciocutaneous flaps have few functional sequelae at the harvest site.
Although historically perceived as more susceptible to infection due to less vascularization of fat and fascia than muscle flaps, recent research indicates that fasciocutaneous flaps yield outcomes similar to muscle flaps in managing infected wounds, showcasing their efficacy and challenging previous assumptions. Several recent studies have demonstrated that fasciocutaneous flaps offer comparable outcomes to muscle flaps for managing infected wounds.[10][11][12]
Fasciocutaneous flaps are valuable options for soft tissue coverage in revision procedures, reducing the need for skin grafting. Particularly beneficial for thin-skinned areas like the lower leg, dorsum of the hand, nasal lining, and oropharynx, these flaps offer substantial soft tissue reconstruction without needing prior flap delay. (The practice involves elevating a flap and repositioning it into its original harvest site to stimulate the opening of choke vessels between angiosomes, thereby enhancing flap perfusion before its final transfer. Typically performed 2 to 4 weeks after the delay procedure, it optimizes the flap's viability and functionality for subsequent reconstruction.) However, the vascular pedicle limits its rotational arc unless employed as free flaps, introducing additional considerations and risks. While effective for superficial wounds, fasciocutaneous flaps are not recommended for deep wounds, where muscle flaps may offer greater tissue volume and coverage.
Fasciocutaneous Flap Classification
Cormack and Lamberty classified fasciocutaneous flaps into 4 types based on vascular anatomy:
- Type A
- This flap receives perfusion from multiple fasciocutaneous perforators entering its base.
- This type can be based proximally or distally.
- Type B
- A single fasciocutaneous perforator supplies this type of flap.
- This type may be elevated as an island flap or harvested as a free flap.
- Type C
- Several small perforators from the main artery penetrate the skin through a fascial septum, and the main artery is incorporated into the flap.
- This type can have a proximal, distal, or free flap base.
- Type D
- This type is a composite flap, similar to type C, but includes a portion of adjacent muscle and bone.[5]
Fasciocutaneous Flap Harvest
The choice of fasciocutaneous flap harvest configuration depends on factors such as the size and location of the defect, the availability of donor tissue, and the desired aesthetic outcome. Fasciocutaneous flaps can be harvested in 4 different configurations, depending upon the tissue included and the relationship of the flap to its pedicle. They are:
- Peninsular fasciocutaneous flaps
- The adipofasciocutaneous unit is harvested, maintaining a connection to the donor site, the base of the flap, and its contained pedicle. This allows for rotation or transposition of the flap. However, rotation can result in a bulky standing cutaneous "dog-ear" deformity at the base, occasionally necessitating a secondary corrective procedure.
- Island fasciocutaneous flaps with adipofascial pedicles
- This variant requires the dissection of the vascular pedicle separately from the flap itself, although the 2 remain connected. The length of the pedicle then defines the flap's potential arc of rotation and, therefore, how it can be inset into a defect.
- Adipofascial flaps
- These flaps contain subdermal fat and the underlying fascia, with its associated vascular plexus.
- Fascial flaps
- Although labeled as fasciocutaneous, these flaps lack a cutaneous component. They are commonly utilized for tendon coverage to reestablish a gliding layer. However, they can also be used for reconstructing mucosal defects, as the fascial surface can mucosalize when placed in a mucosalized area like the oral cavity or pharynx.
Fasciocutaneous Flaps of the Lower Extremity
Fasciocutaneous flaps gained prominence initially in leg reconstruction, with various flap designs tailored to address soft tissue deficits across different leg regions. These flaps can originate from the leg's posterior, lateral, or medial aspects. They may be based proximally or distally, depending on the location of the pedicle in relation to the flap. Flaps with a distal base pose a higher risk of venous congestion, which can be mitigated by connecting a superficial vein in the flap to 1 in the recipient site during transfer.[13] The leg's proximal third contains numerous musculocutaneous perforating vessels that course through the medial and lateral heads of the gastrocnemius muscle. In the middle and distal thirds, septocutaneous perforators dominate the blood supply, originating from the anterior tibial artery, posterior tibial artery, and peroneal artery.[14] Venous return follows the arterial supply pattern, draining directly into corresponding veins.
The critical factor in flap design is ensuring adequate blood flow to perfuse the tissue. This is achieved by incorporating a preselected vascular pedicle rather than adhering strictly to a fixed length-width ratio. This approach allows for flexibility in narrowing the pedicle at the base, facilitating the harvesting of a true island flap.
Proximally-based fasciocutaneous flaps
- Saphenous flap
- Acland et al were the first to describe the saphenous flap, which relies on the saphenous artery as its vascular supply. This artery initially penetrates the aponeurotic roof of the adductor canal within a short distance of its origin, proceeding inferiorly for approximately 12 to 15 cm between the sartorius and vastus medialis muscles, as well as the adductor tendon.[15] From there, it issues 1 to 4 significant cutaneous branches, providing vascular support to a sizable area of skin medially above the knee. Subsequently, the terminal (distal) saphenous artery courses between the sartorius and gracilis tendons, supplying the skin of the upper and medial segments of the leg below the knee.
- The flap's dimensions can reach up to 8 to 10 cm in width and 30 cm in length, with 10 cm above and 20 cm below the knee. The distal part of the flap may be utilized to cover the proximal third of the tibia. However, if the goal is to address a knee defect, the flap must be harvested more proximally, necessitating the division of the sartorius muscle during flap elevation.
- Medial fasciocutaneous flap
- Perfused by the musculocutaneous perforators of the head of the medial gastrocnemius, this flap's anterior border aligns posterior to the medial edge of the tibia, while its posterior border should follow the posteromedial line of the lower leg. The distal margin of the flap should not surpass a point situated 5 cm proximal to the medial malleolus.
- Frequently employed for coverage, this flap addresses defects in the knee's anterior aspect and the proximal and middle thirds of the leg (see Images. Medial Fasciocutaneous Flap and Medial Fasciocutaneous Flap Follow-Up).
- Lateral fasciocutaneous flap
- Like its medial counterpart, the lateral fasciocutaneous flap is perfused by the musculocutaneous perforators of the head of the lateral gastrocnemius muscle. The flap's anterior limit lies 2 cm posterior to the posterior edge of the fibula, the posterior limit is the medial line of the leg, and the distal limit should not fall beyond a point 10 cm proximal to the lateral malleolus.
- Anterolateral fasciocutaneous flap
- The musculocutaneous perforators of the anterior tibial and peroneal arteries supply this flap. The design should incorporate an anterior limit located 2 cm posterior to the tibial crest, a posterior boundary positioned posterior to the fibula, and a distal endpoint situated 5 cm proximal to the lateral malleolus.
- Posterior fasciocutaneous flap
- The blood supply to the skin of the posterior leg is derived from 2 sources: 1) perforating arteries that arise from the popliteal and posterior tibial arteries and 2) axial arteries originating from the popliteal, sural, and geniculate arteries that course either above or below the deep fascia.[16]
- This flap can be raised from the popliteal fold proximally to the union between the middle and distal third of the leg distally, and the medial and lateral limits may extend to the medial or lateral midlines.
Distally based flaps can be configured in 3 distinct ways:
- Relying on the perforators of the posterior tibial artery, leaving a base width of 3 to 4 cm, the distal dissection stopped no further than 10 cm proximal to the medial malleolus.
- Utilizing the perforators of the peroneal artery, it features a 3- to 4-cm pedicle width and a distal limit not exceeding 13 cm proximal to the lateral malleolus.
- Alternatively, the flap may be raised based on both pedicles, necessitating a broader base to encompass them. Irrespective of the chosen arterial supply, the flap's proximal margin remains in the popliteal fossa.
Distally-based fasciocutaneous flaps
- Groin flap
- Described by McGregor and Jackson in 1972, this flap is based on the superficial circumflex iliac artery, which enters inferomedially.[17] The flap has a fusiform shape, measuring 10 to 15 cm wide by 15 to 20 cm long, centered in the inguinal crease.
- Regarded as a versatile option, this flap can be a reliable choice for various reconstructive purposes, including abdominal or perineal reconstruction, when used as a pedicled flap. Additionally, it can be harvested for free tissue transfer, expanding its utility in surgical procedures. These are increasingly used as an alternative to scrotoplasty for large genital wounds.[18]
- Sural fasciocutaneous flap
- The vascular supply of this flap originates from the sural artery, which runs parallel to the sural nerve. Septocutaneous perforators, deriving from the posterior tibial and peroneal arteries, vascularize these flaps at the medial and lateral edges of the Achilles tendon.
Fasciocutaneous Flaps of the Head, Neck, and Upper Extremity
- Temporoparietal fascia flap
- This flap is commonly employed in both head and neck surgery as a pedicled flap and in hand surgery as a free flap (see Image. Temporoparietal Fascia Flap). Up to 8 x 15 cm of thin, pliable soft tissue can be harvested, although it is typically only fascia without overlying skin.
- In some cases, a composite approach may include parietal bone, temporalis fascia and muscle, or scalp, all reliant on the superficial temporal artery and vein. Flap elevation typically entails a lengthy vertical or zig-zag scalp incision originating just anterior to the root of the helix. However, larger flaps may be procured through smaller, minimally invasive incisions.[19][20]
- When time permits, the available temporoparietal fascia can be expanded via tissue expansion to cover larger defects, as seen in microtia reconstruction cases.[21]
- Alternatively, if the temporoparietal fascia flap is unavailable or inconveniently located, a fascia-only flap may be obtained more posteriorly under the scalp, based on the occipital artery.[22]
- Parascapular flap
- The parascapular flap derives its blood supply from the descending branch of the circumflex scapular artery, providing ample soft tissue spanning up to 15 x 30 cm of skin and fascia situated laterally to the scapula's outer border.[23] Due to the robust vascular network in the axilla, this flap may include a portion of the scapula along with its overlying fascia and skin, latissimus dorsi muscle, and serratus anterior muscle, with or without rib, when harvested.[24]
- When utilized as a free flap, the applications for this flap and its variants are virtually limitless.
- Radial forearm
- A versatile option for head, neck, and upper extremity reconstruction, the radial forearm flap relies on the radial artery for its blood supply, with venous drainage typically facilitated by the venae comitantes of the radial artery, often augmented by the cephalic vein.[25] This flap offers a generous supply of thin, pliable skin, spanning up to 15 x 30 cm, and may include the lateral antebrachial cutaneous nerve for sensory restoration if desired. Additionally, it can serve as a source of fascia alone, eliminating the need for skin graft closure at the donor site. In cases requiring bone reconstruction, a 10- to 12-cm segment of partial-thickness radius bone can also be harvested alongside the flap.[26]
- An alternative to the radial forearm flap is 1 based on the ulnar artery, offering similar characteristics but without bone harvest. The ulnar artery is, however, protected by muscle bellies along most of its course, potentially enhancing wound healing and aesthetic outcomes by avoiding direct skin graft application to the paratenon. Venous outflow may be augmented by anastomosing the basilic vein in the recipient site, while sensory function may be provided by incorporating the medial antebrachial cutaneous nerve into the flap.
- The choice between radial and ulnar artery perfusion may be guided by determining which artery is the nondominant supplier of blood to the hand. The Allen test can aid this assessment (see Video. Modified Allen Test).
- Lateral arm flap
- Derived from the posterior radial collateral artery, the lateral arm flap is a fasciocutaneous flap offering fascia with or without skin and subdermal fat. Additionally, it presents the option for harvesting a small quantity of cortical bone from the humerus and muscle from the triceps.
- With a potential size of up to 8 x 20 cm of skin, this flap provides substantial tissue coverage.[27] However, its short pedicle limits its application as either a pedicled or a free flap. Nonetheless, because of its harvest location, the donor site can typically be closed primarily, in contrast to the donor sites of forearm flaps.
Contraindications
An overriding contraindication to fasciocutaneous flap surgery is the absence of suitable tissue for transfer. Several factors can render tissue inadequate for this purpose, including insufficient surface area relative to the size of the defect, scarring or contracture resulting from previous trauma or surgery that disrupted the tissue, inadequate blood supply to the flap (by transecting an artery or causing lymphedema), or underlying vasculopathy.
Smoking, in particular, is known to compromise the microcirculation upon which flaps depend for perfusion and is therefore considered a relative contraindication to fasciocutaneous flap transfer.[28][29][30] While smoking cessation is important for patients' overall health and well-being, even a temporary cessation of smoking for as little as 1 week before flap surgery can significantly improve the likelihood of a successful outcome.[30] If smoking cessation cannot be achieved, a different reconstructive option should be considered, such as a musculocutaneous flap, which will provide a more robust blood supply than a fasciocutaneous flap but at the expense of added bulk.
Diabetes is another prevalent cause of peripheral vasculopathy, which can negatively impact flap perfusion. Before flap surgery, a comprehensive preoperative assessment is mandatory for patients with known or suspected vasculopathy. This evaluation may include conventional angiography, duplex ultrasonography, and computed tomographic or magnetic resonance angiography. These imaging modalities will help determine the planned flap's viability and what other options may be more appropriate.
Fasciocutaneous flaps are typically unsuitable for reconstructing deep, composite defects involving multiple tissue types. In such cases, bulky flaps, like muscle or musculocutaneous flaps, are preferred due to their ability to provide adequate tissue volume.
Defect size is another consideration, as some flaps may not be able to close certain defects fully, and the harvest sites of some flaps may require skin grafting for closure.
Ultimately, patients must be informed about the potential risks before surgery and have the autonomy to make treatment decisions. In some instances, patients may opt for flap transfer without undergoing smoking cessation despite the associated risks.
Equipment
Preoperatively
- Alcohol solution or pad
- Surgical marker
- Local anesthetic (1% lidocaine with 1:100,000 epinephrine in a 10 mL syringe with a 27 gauge 1.5-inch needle or similar)
- Topical antiseptics, such as chlorhexidine or povidone-iodine
- Sterile surgical drape
Intraoperatively
- Scalpel (#15 blade)
- Forceps (Gerald, DeBakey, and Adson)
- Dissecting scissors (Shea or Metzenbaum)
- Suture scissors (Iris or Mayo)
- Gauze
- Monopolar or bipolar electrocautery
- Joseph skin hooks
- Senn retractors
- Needle drivers
- Normal saline
- Suture (2-0 braided polyglactin, 2-0 or 3-0 poliglecaprone, 3-0 polypropylene or nylon)
Postoperatively
- Petrolatum ointment
- Nonadherent gauze
- Gauze roll
- Surgical tape
Personnel
The majority of fasciocutaneous flap transfers are performed by plastic surgeons. However, many orthopedic trauma and hand surgeons are also trained to undertake these procedures.[31] In the head and neck, head and neck surgical oncologists, reconstructive surgeons, and facial plastic surgeons are also typically well-versed in these techniques.[32]
In addition to the surgeon, an assistant is necessary to provide retraction, suture cutting, and manage bleeding. A surgical technician and a circulating nurse are also essential team members. These procedures may be performed under general or regional anesthesia, depending upon patient preferences and the anatomy involved; therefore, an anesthesia provider is also typically required.
Preparation
Patient Counseling
Patient education before surgery is critical. Counseling should emphasize potential complications, primarily vascular compromise leading to tissue loss, and the possibility of cosmetic dissatisfaction at both the flap donor and recipient sites, which may necessitate further procedures. Additionally, patients should be advised on the critical importance of smoking cessation for at least 1 week before surgery to optimize flap perfusion.[30] When necessary, postoperative wound care education should also be provided, particularly if drains are placed or if complications arise and intricate dressings or care regimens are required.
Preoperative Preparation
The flap is designed to match the individual defect precisely. Incorporating excess length in the flap design ensures ample defect coverage and compensates for the inevitable loss of length during pedicle rotation and flap inset. This surplus length also diminishes tension during closure and mitigates the risk of vascular compromise at the flap's distal margin. In cases where the flap is elevated and transferred on an extremity, a tourniquet may be employed, but caution must be exercised to limit tourniquet inflation time to under 2 hours.[33] While the tourniquet aids in reducing blood loss and enhancing visualization in the operative field, it also contributes significantly to procedural efficiency.
Particular attention should be given to positioning the patient so that the surgical team has easy access to the operative site while minimizing pressure points and nerve traction, taking into account the expected duration of the operation. Following proper positioning, the operative site may be infiltrated with a local anesthetic if necessary, and the area should be thoroughly cleansed using an antiseptic solution.
Technique or Treatment
With experience, the elevation and transfer of fasciocutaneous flaps become rapid and straightforward. The design of the flap and the placement of incisions are contingent on the location of the tissue defect and the selected donor site. Before completing the incisions, it is crucial to identify the pivot point and determine the required length of the pedicle. Flaps with long arcs of rotation may require additional length in their design to compensate for the inevitable loss during rotation into the wound and to prevent excessive tension during closure, which could lead to subsequent distal margin necrosis. The degree of rotation directly impacts the length lost: a 45° angle results in a 5% reduction in length, a 90º angle leads to a 15% reduction, and a 180º angle results in a 40% loss. Additionally, the size of the standing cutaneous deformity at the base of the flap correlates with the degree of rotation, with larger angles resulting in larger deformities.
Generally, the incision is extended through the skin, subcutaneous tissue, and fascia. Subsequently, flap elevation typically advances through dissection within a subfascial plane to safeguard the fasciocutaneous perforating vessels supplying the skin. While raising the flap, individually identifying these vessels isn't essential, but attention should be given to identifying and safeguarding the pedicle vessels. Usually, the pedicle is dissected retrogradely following the circumferential incision of the flap, with its length determined by the extent of flap mobility needed for the inset.[34]
The skin encompassing the defect is excised, and the wound edges are undermined. Following this, the fasciocutaneous flap is either rotated or advanced into place, and the fascia is sutured to ensure stability. Only a few tacking sutures are required to secure the flap. Subsequently, the skin is closed around the margin of the flap. In the case of rotating large flaps, the standing cutaneous deformity should be deferred for correction later, as excising it during flap transfer could jeopardize blood flow through the base of the flap. The secondary defect at the flap harvest site can be promptly closed with a split-thickness skin graft; however, since the surface is typically irregular, it might be preferable to wait for granulation tissue to develop before applying the graft. The area is then bandaged with moderate pressure, and if necessary, continuous suction drainage may be employed for 24 hours or longer. Continuous suction drainage may be applied for 24 hours or more if bleeding persists.[1]
Complications
The most concerning complication after transferring a fasciocutaneous flap is vascular compromise, which may lead to complete or partial necrosis of the flap. Arterial or venous factors can cause vascular compromise. Arterial insufficiency may arise from suboptimal microvasculature quality, seen in smokers or diabetic patients, or from excessive tension on the flap, constricting arterioles and capillaries, especially at the flap's distal end. Hypotension can also reduce perfusion, as can clot formation within the arterial or venous systems, causing arterial stasis due to insufficient outflow. Venous insufficiency, more prevalent than arterial issues, may occur if the flap is inadvertently raised without adequate venous drainage or if the venous outflow is obstructed, such as by a hematoma exerting pressure on the vein or by the vein becoming twisted during flap manipulation before inset. Microsurgical anastomosis of a superficial vein within the flap to a recipient vein in the wound bed can significantly enhance venous outflow and diminish the risk of flap failure.
Additional risks associated with fasciocutaneous flap transfer include cosmetic dissatisfaction arising from inadequate color, texture, or hair growth matching with surrounding tissue and potential scarring and distortion at the donor site, particularly evident with larger flaps. While normal pilosebaceous function typically returns to the flap posttransfer, long-term sensation may remain diminished. Moreover, standard surgical risks such as pain, bleeding, infection, and damage to adjacent structures (depending on the flap elevation site) persist, potentially necessitating further procedures.[35]
Clinical Significance
Fasciocutaneous flaps are integral in reconstructing soft tissue defects exceeding primary closure capabilities. By encompassing the deep fascia and perifascial vascular network during elevation, they offer superior soft tissue coverage compared to local advancement and rotation flaps, especially in the lower extremities. Renowned for their thin and pliable nature, these flaps are swiftly and easily elevated and transferred. They prove versatile in addressing various wounds, with a particular aptitude for covering exposed tendons, bones, and joints.
Despite advancements in flap techniques, fasciocutaneous flaps remain pivotal in reconstructive surgery due to their reliability and straightforward application. They often become the go-to option when alternatives like perforator-based or free flaps have failed.[6]
Enhancing Healthcare Team Outcomes
Successful treatment of patients undergoing fasciocutaneous flap procedures requires collaboration among various healthcare professionals. Physicians, including surgeons and specialists, are responsible for accurately assessing the patient's condition, determining the need for flap reconstruction, and planning the surgical procedure. Advanced practitioners are crucial in assisting with preoperative assessments, providing perioperative care, and monitoring patients postoperatively. Nurses are essential for patient education, wound care management, and monitoring for any signs of complications during recovery. Pharmacists contribute by ensuring appropriate medication management, including pain control and prevention against infection.
Interprofessional communication among team members ensures seamless care transitions and optimal patient outcomes. Regular communication facilitates the exchange of critical information regarding the patient and allows for the early identification and mitigation of potential complications, ensuring patient safety throughout the surgical and recovery process. Care coordination involves organizing the various aspects of patient care, including scheduling appointments, arranging diagnostic tests, and facilitating consultations with other specialists. By working together as a cohesive team, healthcare professionals can provide patient-centered care, enhance outcomes, promote patient safety, and optimize team performance in caring for patients undergoing fasciocutaneous flap procedures.
Media
(Click Image to Enlarge)
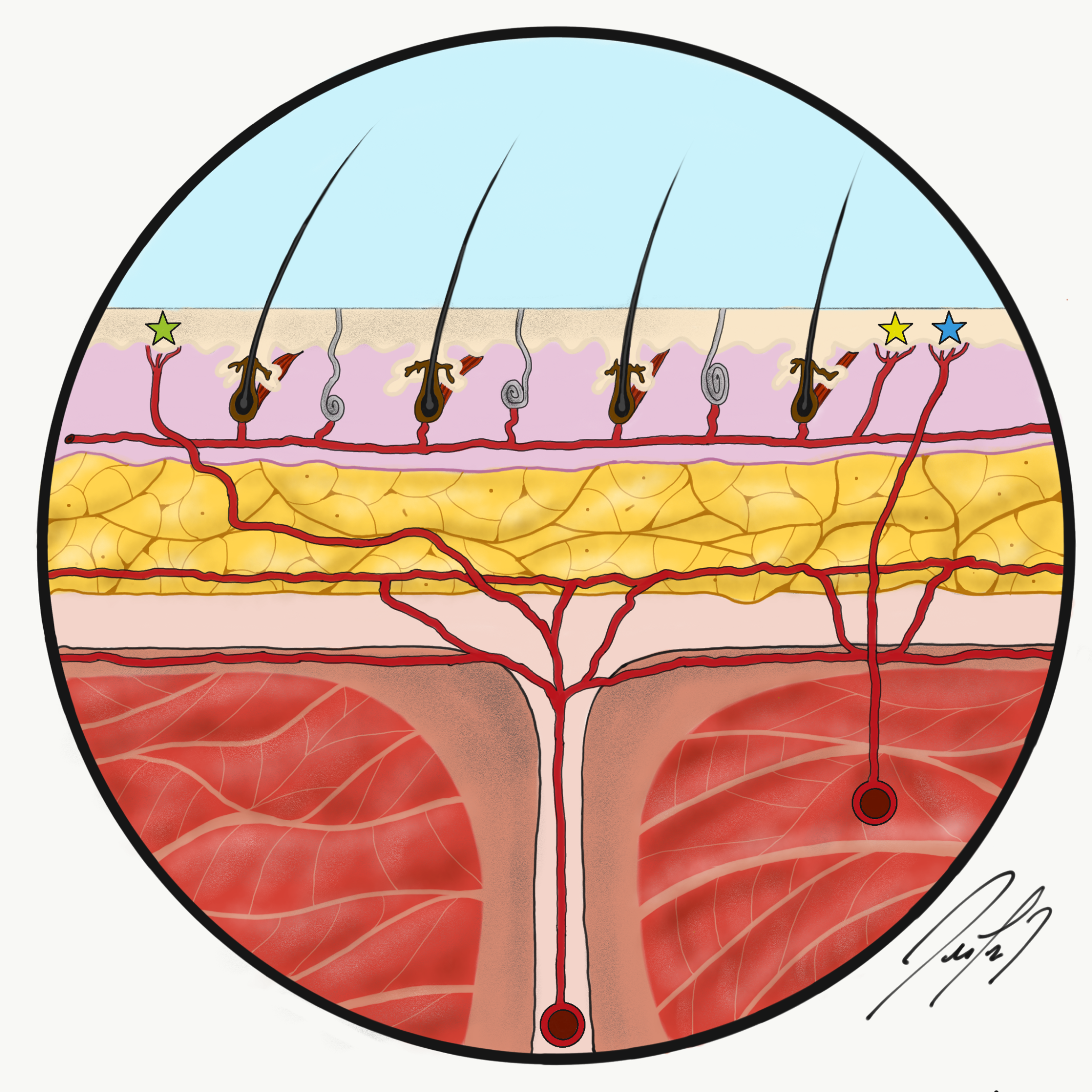
Fasciocutaneous Flap Perfusion. The green star indicates a septocutaneous perforator, the yellow star is a direct cutaneous perforator, and the blue star is a musculocutaneous perforator.
Contributed by FL De Cicco, MD
(Click Image to Enlarge)
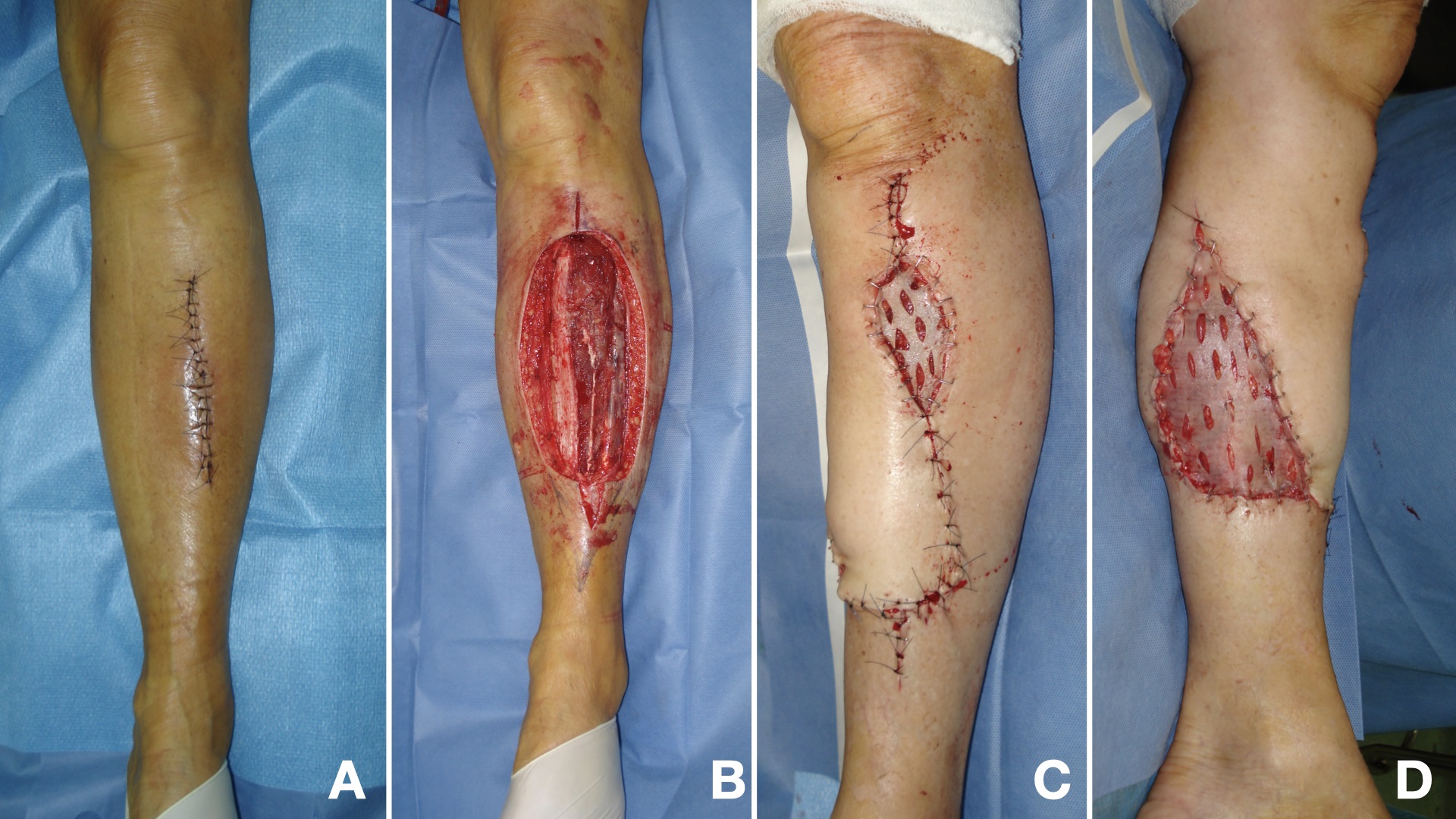
Medial Fasciocutaneous Flap. A) A 65-year-old woman with an unplanned incomplete sarcoma excision of the leg. B) Wide resection of the sarcoma. C and D) A medial fasciocutaneous flap, with associated skin graft, has been placed to cover the proximal and middle third of the exposed tibia.
Contributed by JG. Boretto, MD
(Click Image to Enlarge)
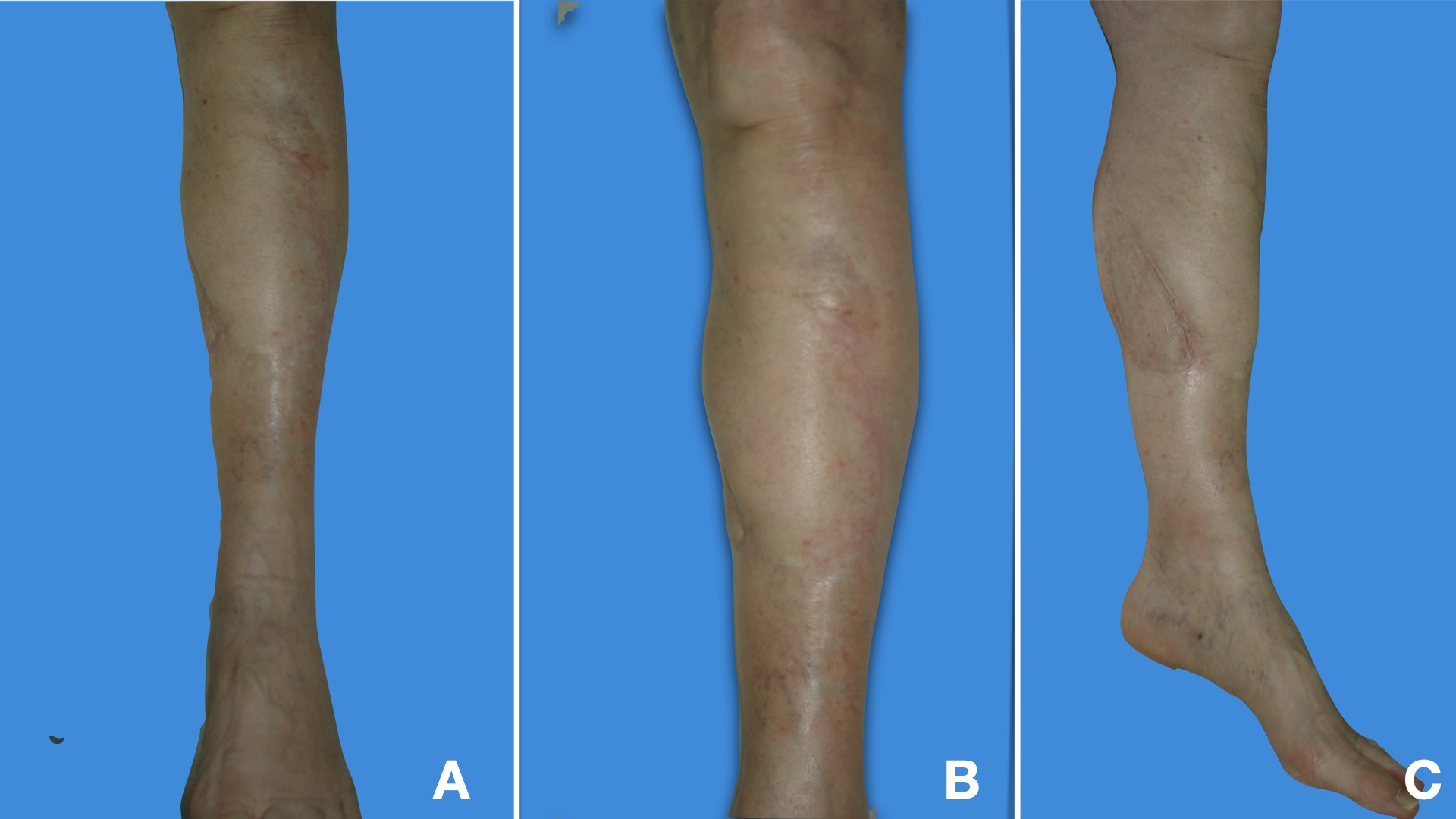
Medial Fasciocutaneous Flap Follow-Up. Images A, B, and C show the flap at a 2-year follow-up.
Contributed by JG Boretto, MD
(Click Image to Enlarge)
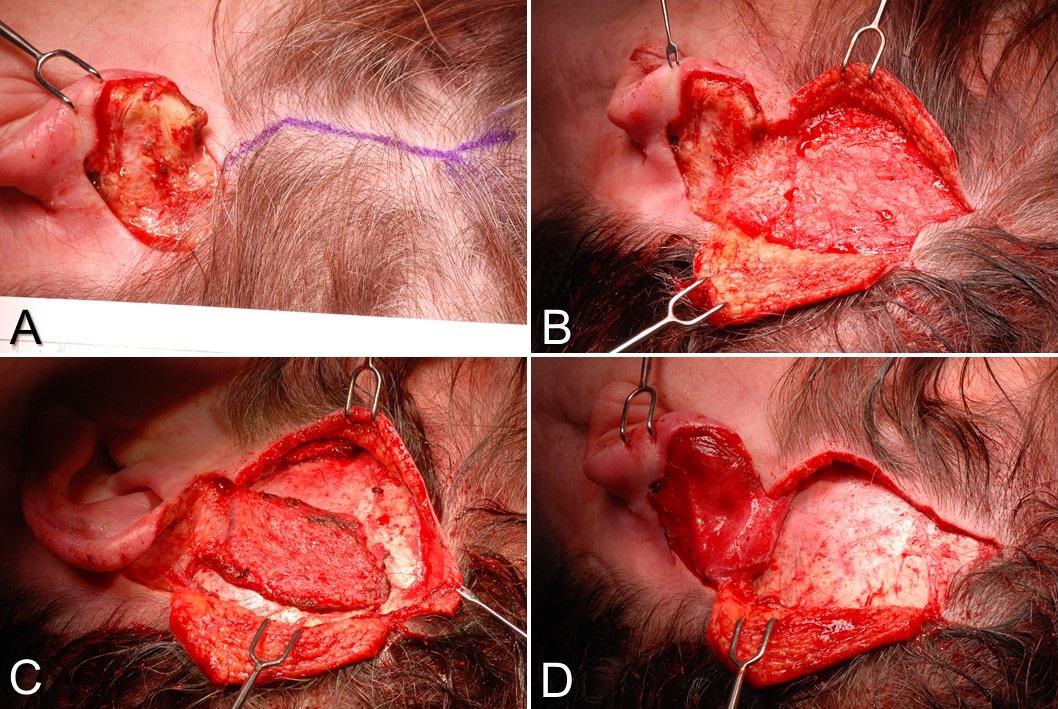
Temporoparietal Fascia Flap. A) This is a postauricular defect from Mohs surgery with too much bare cartilage for a skin graft alone to survive. A Y-shaped incision is planned, paralleling the course of the superficial temporal artery. B) The scalp flaps are elevated in a subdermal plane, exposing the temporoparietal fascia. C) The temporoparietal fascia flap is incised on 3 sides, with the pedicle intact inferiorly. D) The temporoparietal fascia flap is transferred into the defect, after which the scalp will be closed in layers, and a skin graft will be applied to the flap.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
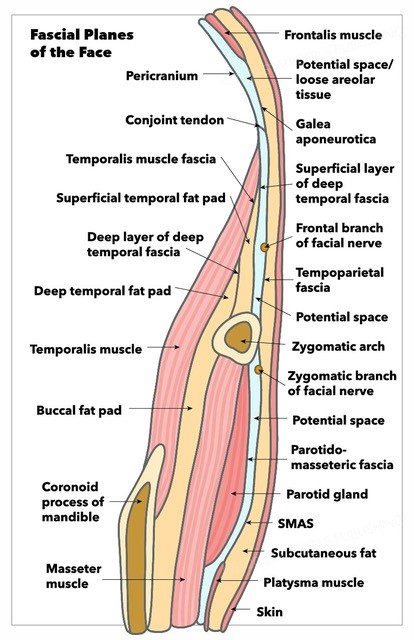
Fascial Planes of the Face and Musculature. This illustration depicts the fascial planes of the face, highlighting the continuity of the frontalis muscle, galea aponeurotica, temporoparietal fascia, superficial musculoaponeurotic system, platysma, and the location of the facial nerve.
Contributed by K Humphreys and MH Hohman, MD, FACS
(Click Video to Play)
Modified Allen Test. The modified Allen test evaluates whether the ulnar artery can adequately supply blood to the hand if the radial artery is ligated, such as during a radial forearm flap harvest.
Contributed by MH Hohman, MD, FACS
References
Pontén B. The fasciocutaneous flap: its use in soft tissue defects of the lower leg. British journal of plastic surgery. 1981 Apr:34(2):215-20 [PubMed PMID: 7236984]
Hashimoto I, Abe Y, Ishida S, Kashiwagi K, Mineda K, Yamashita Y, Yamato R, Toda A, Fukunaga Y, Yoshimoto S, Tsuda T, Nagasaka S, Keyama T. Development of Skin Flaps for Reconstructive Surgery: Random Pattern Flap to Perforator Flap. The journal of medical investigation : JMI. 2016:63(3-4):159-62. doi: 10.2152/jmi.63.159. Epub [PubMed PMID: 27644551]
Haertsch P. The surgical plane in the leg. British journal of plastic surgery. 1981 Oct:34(4):464-9 [PubMed PMID: 7296153]
Barclay TL, Cardoso E, Sharpe DT, Crockett DJ. Repair of lower leg injuries with fascio-cutaneous flaps. British journal of plastic surgery. 1982 Apr:35(2):127-32 [PubMed PMID: 7044458]
Cormack GC, Lamberty BG. A classification of fascio-cutaneous flaps according to their patterns of vascularisation. British journal of plastic surgery. 1984 Jan:37(1):80-7 [PubMed PMID: 6692066]
Kim JT, Kim SW. Perforator Flap versus Conventional Flap. Journal of Korean medical science. 2015 May:30(5):514-22. doi: 10.3346/jkms.2015.30.5.514. Epub 2015 Apr 15 [PubMed PMID: 25931780]
Taylor GI, Palmer JH. The vascular territories (angiosomes) of the body: experimental study and clinical applications. British journal of plastic surgery. 1987 Mar:40(2):113-41 [PubMed PMID: 3567445]
Batchelor JS, Moss AL. The relationship between fasciocutaneous perforators and their fascial branches: an anatomical study in human cadaver lower legs. Plastic and reconstructive surgery. 1995 Apr:95(4):629-33 [PubMed PMID: 7892305]
Tolhurst DE, Haeseker B, Zeeman RJ. The development of the fasciocutaneous flap and its clinical applications. Plastic and reconstructive surgery. 1983 May:71(5):597-606 [PubMed PMID: 6836058]
Level 3 (low-level) evidenceSalgado CJ, Mardini S, Jamali AA, Ortiz J, Gonzales R, Chen HC. Muscle versus nonmuscle flaps in the reconstruction of chronic osteomyelitis defects. Plastic and reconstructive surgery. 2006 Nov:118(6):1401-1411. doi: 10.1097/01.prs.0000239579.37760.92. Epub [PubMed PMID: 17051111]
Level 3 (low-level) evidenceCho EH, Shammas RL, Carney MJ, Weissler JM, Bauder AR, Glener AD, Kovach SJ, Hollenbeck ST, Levin LS. Muscle versus Fasciocutaneous Free Flaps in Lower Extremity Traumatic Reconstruction: A Multicenter Outcomes Analysis. Plastic and reconstructive surgery. 2018 Jan:141(1):191-199. doi: 10.1097/PRS.0000000000003927. Epub [PubMed PMID: 28938362]
Kovar A, Colakoglu S, Iorio ML. Choosing between Muscle and Fasciocutaneous Free Flap Reconstruction in the Treatment of Lower Extremity Osteomyelitis: Available Evidence for a Function-Specific Approach. Journal of reconstructive microsurgery. 2020 Mar:36(3):197-203. doi: 10.1055/s-0039-1698469. Epub 2019 Oct 7 [PubMed PMID: 31590192]
Herlin C, Bekara F, Bertheuil N, Carloni R, Dast S, Sinna R, Chaput B. Venous Supercharging Reduces Complications and Improves Outcomes of Distally Based Sural Flaps. Journal of reconstructive microsurgery. 2017 Jun:33(5):343-351. doi: 10.1055/s-0037-1598620. Epub 2017 Feb 24 [PubMed PMID: 28235215]
Kumar S, Kumar S, Tiwari V, Nathani N, Pal L. Various Modalities of the Resurfacing of the Lower Limb and Its Outcome. Cureus. 2023 Oct:15(10):e46421. doi: 10.7759/cureus.46421. Epub 2023 Oct 3 [PubMed PMID: 37927660]
Acland RD, Schusterman M, Godina M, Eder E, Taylor GI, Carlisle I. The saphenous neurovascular free flap. Plastic and reconstructive surgery. 1981 Jun:67(6):763-74 [PubMed PMID: 7243977]
Level 3 (low-level) evidenceWalton RL, Bunkis J. The posterior calf fasciocutaneous free flap. Plastic and reconstructive surgery. 1984 Jul:74(1):76-85 [PubMed PMID: 6377344]
Level 3 (low-level) evidenceMcGregor IA, Jackson IT. The groin flap. British journal of plastic surgery. 1972 Jan:25(1):3-16 [PubMed PMID: 4550433]
Staniorski C, Myrga J, Hayden C, Sterling J, Rusilko P. Fasciocutaneous Flap Perineal Closure with Testicular Thigh Pouch for Scrotal Defects: Surgical Technique and Initial Experience. Urology. 2023 Dec:182():231-238. doi: 10.1016/j.urology.2023.07.039. Epub 2023 Sep 13 [PubMed PMID: 37708982]
Jawad BA, Raggio BS. Temporoparietal Fascia Flaps. StatPearls. 2024 Jan:(): [PubMed PMID: 32310365]
Reinisch J, Tahiri Y. Polyethylene Ear Reconstruction: A State-of-the-Art Surgical Journey. Plastic and reconstructive surgery. 2018 Feb:141(2):461-470. doi: 10.1097/PRS.0000000000004088. Epub [PubMed PMID: 29370000]
Kerem M, Orbay H, Şensöz Ö. Use of an expanded temporoparietal fascial flap technique for total auricular reconstruction. Plastic and reconstructive surgery. 2007 Jun:119(7):2320-2321. doi: 10.1097/01.prs.0000261075.10453.1d. Epub [PubMed PMID: 17519745]
Level 3 (low-level) evidenceReinisch JF, van Hövell Tot Westerflier CVA, Tahiri Y, Yao CA. The Occipital Artery-Based Fascial Flap for Ear Reconstruction. Plastic and reconstructive surgery. 2019 Mar:143(3):592e-601e. doi: 10.1097/PRS.0000000000005263. Epub [PubMed PMID: 30531625]
Chen D, Jupiter JB, Lipton HA, Li SQ. The parascapular flap for treatment of lower extremity disorders. Plastic and reconstructive surgery. 1989 Jul:84(1):108-16 [PubMed PMID: 2734386]
Vincent A, Hohman MH. Latissimus Dorsi Myocutaneous Flap. StatPearls. 2024 Jan:(): [PubMed PMID: 33232047]
Rengifo D, Lian TT. Radial Forearm Tissue Transfer. StatPearls. 2024 Jan:(): [PubMed PMID: 32809631]
Bigcas JLM, Bond J. Osteocutaneous Radial Forearm Flap. StatPearls. 2024 Jan:(): [PubMed PMID: 33232054]
Sauerbier M, Germann G, Giessler GA, Sedigh Salakdeh M, Döll M. The free lateral arm flap-a reliable option for reconstruction of the forearm and hand. Hand (New York, N.Y.). 2012 Jun:7(2):163-71. doi: 10.1007/s11552-012-9395-3. Epub [PubMed PMID: 23730235]
Reece EM, Bonelli MA, Livingston T, Mulligan PS, Rockwood J, Wilson JR, Zoldos J, Champagne L. Factors in Free Fasciocutaneous Flap Complications: A Logistic Regression Analysis. Plastic and reconstructive surgery. 2015 Jul:136(1):54e-58e. doi: 10.1097/PRS.0000000000001377. Epub [PubMed PMID: 26111332]
Goldminz D, Bennett RG. Cigarette smoking and flap and full-thickness graft necrosis. Archives of dermatology. 1991 Jul:127(7):1012-5 [PubMed PMID: 2064398]
Level 2 (mid-level) evidenceHwang K, Son JS, Ryu WK. Smoking and Flap Survival. Plastic surgery (Oakville, Ont.). 2018 Nov:26(4):280-285. doi: 10.1177/2292550317749509. Epub 2018 Jan 9 [PubMed PMID: 30450347]
Challa S, Conway D, Wu HH, Bisht R, Sherchan B, Lamichhane A, Shearer DW, Terry M, Gillenwater J. Can a 2-Day Course Teach Orthopaedic Surgeons Rotational Flap Procedures? An Evaluation of Data From the Nepal SMART Course Over 2 years. Journal of orthopaedic trauma. 2018 Oct:32 Suppl 7():S38-S42. doi: 10.1097/BOT.0000000000001298. Epub [PubMed PMID: 30247399]
Sahni M, Patel P, Lakhera KK, Singh S, Sharma R. Use of Temporalis Muscle and Temporoparietal Fasciocutaneous Flap (TPPF) for Orbital Exentration Defects: Our Experience of 10 Cases. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2023 Dec:75(4):3657-3662. doi: 10.1007/s12070-023-04054-z. Epub 2023 Jul 14 [PubMed PMID: 37974706]
Level 3 (low-level) evidenceOstman B, Michaelsson K, Rahme H, Hillered L. Tourniquet-induced ischemia and reperfusion in human skeletal muscle. Clinical orthopaedics and related research. 2004 Jan:(418):260-5 [PubMed PMID: 15043128]
Wei FC, Jain V, Suominen S, Chen HC. Confusion among perforator flaps: what is a true perforator flap? Plastic and reconstructive surgery. 2001 Mar:107(3):874-6 [PubMed PMID: 11304620]
Chiu YJ, Liao WC, Wang TH, Shih YC, Ma H, Lin CH, Wu SH, Perng CK. A retrospective study: Multivariate logistic regression analysis of the outcomes after pressure sores reconstruction with fasciocutaneous, myocutaneous, and perforator flaps. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2017 Aug:70(8):1038-1043. doi: 10.1016/j.bjps.2017.04.004. Epub 2017 Apr 23 [PubMed PMID: 28552279]
Level 2 (mid-level) evidence