Introduction
Fetal movements felt by pregnant women are a sign that the fetus is growing in size and strength. The pregnant woman is usually the first to feel these movements, which can later be perceived by others. Women are often taught by their healthcare provider to monitor or be aware of the movements of the fetus. This can be a general awareness of fetal movements, or the women can be taught to count the number of kicks they feel in a set amount of time. Reduced fetal movement can be worrisome for both the mother and the attending healthcare provider. Decreased fetal movement can be a warning sign of potential fetal impairment or risk, and therefore, warrants further evaluation by the healthcare provider.[1][2]
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The first fetal movements, which are felt by the mother, are called quickening. One function of these movements is to alert the pregnant woman that she has a fetus growing in her uterus. Quickening often occurs between the 16th to the 22nd week of pregnancy. This is called a presumptive sign of pregnancy as the other movements of the woman's body can mimic early fetal movements such as flatus, peristalsis, and abdominal muscle contractions. A multiparous woman will usually first notice these fluttering movements of the fetus at an earlier gestation than a primiparous woman. A multiparous woman might feel movements as early as 16 weeks, whereas a primiparous woman may not feel anything until 20 to 22 weeks. At around 20 weeks of gestation, the trained healthcare provider can feel fetal movement externally through the abdomen. This is considered a positive sign of pregnancy.[3]
Most providers recommend that pregnant women monitor fetal movements, especially by the third trimester. This can be accomplished by simply instructing the woman to have a general awareness of the fetus and determine if the fetus is moving less than normal on any given day or about the same as other days. Alternatively, healthcare providers might recommend a more formal fetal movement count (FMC), sometimes called a kick count. Clinicians often recommend starting this surveillance around 28 weeks gestation and continuing throughout the remainder of the pregnancy. The "count to 10" method includes the instructions for the woman to count fetal movements at the same time each day. If the woman experiences less than 10 movements in a 2 to 3-hour period, she is instructed to contact her healthcare provider. One study noted that having women count fetal movements can improve maternal-child bonding during pregnancy as the mother starts to get to know her unborn child.[3]
Issues of Concern
The issues of concern would include perceived or actual decreased fetal movement. Historically, cases of a compromised fetus or infant have usually been preceded by decreased fetal movement. Therefore, the assumption is that if a woman notices a decrease in fetal movement and has it evaluated, then a possible adverse event with the fetus might be avoided by the use of interventions. Many studies have attempted to verify a correlation between decreased fetal movement and placental functioning, abnormalities of the uterus, fetal growth restriction, twin-to-twin transfusion, and tight nuchal cords or to demonstrate that kick counts can prevent intrauterine fetal demise. Although this type of monitoring is often recommended, tracking does not always prevent complications. However, due to the low cost and potential benefit, it is recommended. Decreased fetal movement can indicate a need for more evaluation and has the potential to save lives. There is a worse outcome in pregnancies with reduced fetal movement, with one study demonstrating the highest incidence of poor outcomes in small for gestational age fetuses.[4]
One potential side effect of routine monitoring of fetal movement could be an increase in prenatal visits, either outpatient or inpatient. However, most research has not found this type of increase to be true. Usually, the fetal movement count (FMC) is reassuring to pregnant women and prevents unnecessary visits. The healthcare provider should remember that some women are more vigilant at fetal movement monitoring than others. Therefore other methods of surveillance might be needed if the mother of the baby is less likely to comply with the fetal movement count. Numerous studies are trying to determine various new methods to track fetal movements while the pregnant woman is at home or work. Some methods could allow a more consistent and objective method of measuring frequency and possible strength of movements. The advance of three-dimensional ultrasound has allowed researchers to study normal movements of the fetus throughout pregnancy. This includes facial expressions and rapid eye movement (REM) during sleep. The arm movements of twins compared to singleton births are being studied and evaluated. Researchers find that fetal movement changes throughout pregnancy and can indicate normal or abnormal development (see Image. Development of the Fetal Membranes and Placenta). It is of note that studies have shown that obese women can feel fetal movement as well as women with normal body mass index (BMI). However, due to more common maternal and fetal complications, obese women will likely notice decreased fetal movement more often than their lower BMI counterparts.[5][6]
Clinical Significance
Any decrease in perceived fetal movement should be followed up by the healthcare provider with a nonstress test (see Image. Nonstress Test). This non-invasive test can evaluate fetal movement and fetal heart rate accelerations. A reactive nonstress test must have accelerations of the fetal heart of a specific size, duration, and frequency. This includes at least three fetal heart tone (FHT) accelerations, which are at least 15 beats per minute above the baseline and last at least 15 seconds, all within a 20-minute window. A non-reactive nonstress test, one that does not have the three accelerations, could indicate fetal sleep or fetal compromise, and further testing should be done. Usually, the nonstress test is first extended for a longer time to determine if the lack of accelerations was just due to fetal sleep. If the non-stress test continues to be non-reactive, then a BPP (biophysical profile) is often completed. This is an ultrasound of the fetus to assess fetal breathing movement, fetal movement of the body or limbs, fetal tone, and amniotic fluid volume. If this test does not reassure the healthcare provider, then the delivery of the fetus should be considered.[7] One study found that increased fetal movements may be used to predict adverse neonatal outcomes such as large for gestational age.[8] One study found that instructing women on fetal counting compared to not instructing them was not associated with a clear improvement of pregnancy outcomes.[9] Fetal movement count monitoring is a low-cost and low-tech method that has the potential to prevent worsening problems with unborn babies and merits the attention of providers and pregnant women.
Enhancing Healthcare Team Outcomes
The care of pregnant patients is best undertaken with an interprofessional team approach. Healthcare providers of women during pregnancy have the responsibility to screen and monitor the fetus to identify potential problems. This allows the practitioner to provide patient-centered, targeted treatment, and follow-up. Patients should be educated about the importance of self-monitoring of fetal movements. When decreased fetal movement is perceived, the team should work together to evaluate the fetus further. Many techniques for monitoring fetal movement are controversial and lack sufficient study to document their efficacy. In theory, detecting risk factors and complications during pregnancy could lower neonatal morbidity and mortality.[10] More study is needed to evaluate current methods and their effectiveness in both detection and long-term effects. Monitoring and then subsequent response with interventions have the potential to improve patient outcomes.
Nursing, Allied Health, and Interprofessional Team Interventions
Nurses participate in the evaluation of neonates after maternal reports of decreased fetal movement. Interventions may include applying an external fetal heart monitor, monitoring for contractions, assessing maternal vital signs, and assessing for rupture of maternal membranes. The nurse may also be involved in the care of the woman during further ultrasound assessment of the fetus (biophysical profile) and in communicating the assessments to the patient and her family as well as the primary care clinician.
The nurse in labor and delivery may need to assist in the induction of labor of the patient or cesarean delivery of a compromised fetus if the evaluation is not favorable or reassuring. Communication with all parties is a very important role of the nurse as well as providing empathy and assistance to the patient and family when the pregnancy/birth are not as planned or expected. This can help improve patient outcomes for both mother and baby.
Nursing, Allied Health, and Interprofessional Team Monitoring
Ongoing monitoring by nurses employed in medical offices that care for pregnant women should include education of women about fetal movements and prompt response to reports of decreased fetal movements. All office personnel that are in contact with a pregnant woman either during phone triage or prenatal assessments need to understand the importance of fetal movement monitoring and the need to listen to patient reports. Communication of concerns to the primary care clinician is critical in obtaining further evaluation, which has the potential of improving patient outcomes, especially with prompt assessment and intervention.
Media
(Click Image to Enlarge)
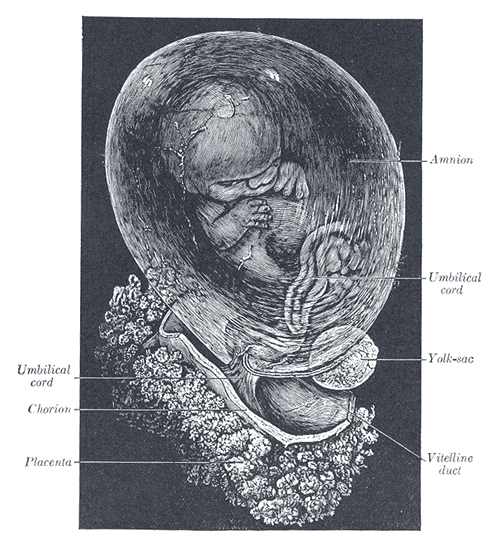
Development of the Fetal Membranes and Placenta. The fetus is approximately 8 weeks enclosed in the amnion.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
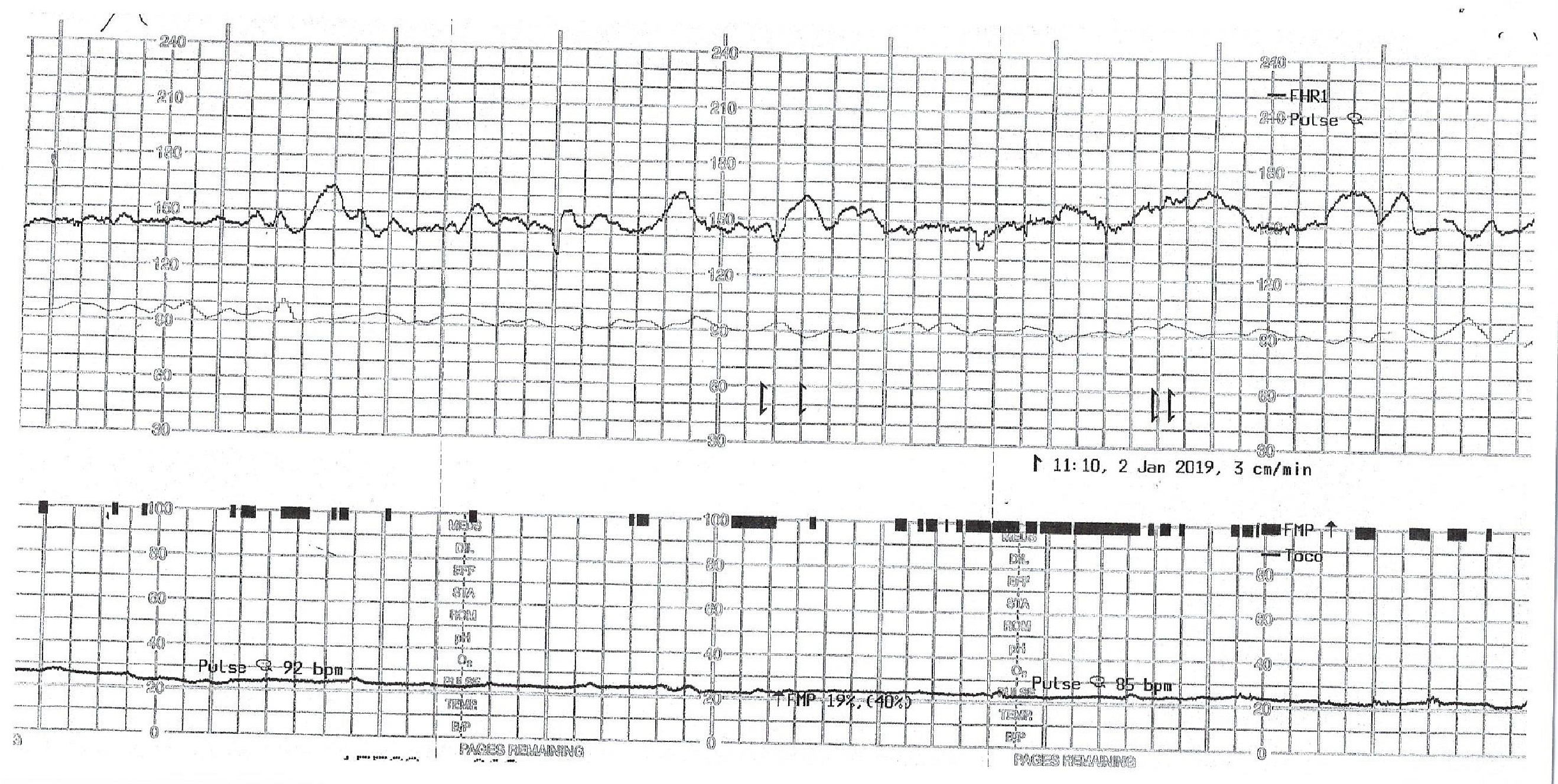
Nonstress Test. Results of a nonstress test reveal fetal heart rate tracing, fetal movement, and contraction tracing.
Contributed by O Umana, MD
References
Das R, Jana N, Arora N, Sengupta S. Ultrasound assessment of fetal hearing response to vibroacoustic stimulation. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2020 Jul:33(14):2326-2332. doi: 10.1080/14767058.2018.1548600. Epub 2019 Jan 8 [PubMed PMID: 30618302]
Kapaya H, Almeida J, Karouni F, Anumba D. Management of reduced fetal movement: A comparative analysis of two audits at a tertiary care clinical service. European journal of obstetrics, gynecology, and reproductive biology. 2020 May:248():128-132. doi: 10.1016/j.ejogrb.2020.03.040. Epub 2020 Mar 18 [PubMed PMID: 32203823]
Level 2 (mid-level) evidenceFlenady V, Ellwood D, Bradford B, Coory M, Middleton P, Gardener G, Radestad I, Homer C, Davies-Tuck M, Forster D, Gordon A, Groom K, Crowther C, Walker S, Foord C, Warland J, Murphy M, Said J, Boyle F, O'Donoghue K, Cronin R, Sexton J, Weller M, McCowan L. Beyond the headlines: Fetal movement awareness is an important stillbirth prevention strategy. Women and birth : journal of the Australian College of Midwives. 2019 Feb:32(1):1-2. doi: 10.1016/j.wombi.2018.12.001. Epub 2018 Dec 15 [PubMed PMID: 30563769]
Sterpu I, Pilo C, Koistinen IS, Lindqvist PG, Gemzell-Danielsson K, Itzel EW. Risk factors for poor neonatal outcome in pregnancies with decreased fetal movements. Acta obstetricia et gynecologica Scandinavica. 2020 Aug:99(8):1014-1021. doi: 10.1111/aogs.13827. Epub 2020 Mar 12 [PubMed PMID: 32072616]
Daly LM, Boyle FM, Gibbons K, Le H, Roberts J, Flenady V. Mobile applications providing guidance about decreased fetal movement: Review and content analysis. Women and birth : journal of the Australian College of Midwives. 2019 Jun:32(3):e289-e296. doi: 10.1016/j.wombi.2018.07.020. Epub 2018 Aug 20 [PubMed PMID: 30139669]
Bradford B, Cronin R, McKinlay C, Thompson J, McCowan L. Maternally perceived fetal movement patterns: The influence of body mass index. Early human development. 2020 Jan:140():104922. doi: 10.1016/j.earlhumdev.2019.104922. Epub 2019 Nov 15 [PubMed PMID: 31739267]
Heazell AEP, Budd J, Li M, Cronin R, Bradford B, McCowan LME, Mitchell EA, Stacey T, Martin B, Roberts D, Thompson JMD. Alterations in maternally perceived fetal movement and their association with late stillbirth: findings from the Midland and North of England stillbirth case-control study. BMJ open. 2018 Jul 6:8(7):e020031. doi: 10.1136/bmjopen-2017-020031. Epub 2018 Jul 6 [PubMed PMID: 29982198]
Level 2 (mid-level) evidenceHuang C, Han W, Fan Y. Correlation study between increased fetal movement during the third trimester and neonatal outcome. BMC pregnancy and childbirth. 2019 Dec 4:19(1):467. doi: 10.1186/s12884-019-2637-4. Epub 2019 Dec 4 [PubMed PMID: 31801506]
Bellussi F, Po' G, Livi A, Saccone G, De Vivo V, Oliver EA, Berghella V. Fetal Movement Counting and Perinatal Mortality: A Systematic Review and Meta-analysis. Obstetrics and gynecology. 2020 Feb:135(2):453-462. doi: 10.1097/AOG.0000000000003645. Epub [PubMed PMID: 31923063]
Level 1 (high-level) evidenceHaws RA, Yakoob MY, Soomro T, Menezes EV, Darmstadt GL, Bhutta ZA. Reducing stillbirths: screening and monitoring during pregnancy and labour. BMC pregnancy and childbirth. 2009 May 7:9 Suppl 1(Suppl 1):S5. doi: 10.1186/1471-2393-9-S1-S5. Epub 2009 May 7 [PubMed PMID: 19426468]
Level 1 (high-level) evidence