Introduction
Distal femur fractures include fractures of the supracondylar and intercondylar region and are relatively common injuries. The goals of treatment follow AO principles of anatomic reduction of the articular surface, restoration of limb alignment, length, and rotation. Despite improvements in implant design, management of distal femur fractures remains a challenge; fractures are often comminuted, intra-articular, and involve osteoporotic bone, making fixation challenging to achieve. In the geriatric trauma population, the incidence of co-morbidities is high and may impact the therapeutic options.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Adult distal femur fractures present in a bimodal distribution.[1] Younger male patients generally present secondary to high-energy mechanisms, such as motor vehicle accidents. Elderly patients present typically after low-energy mechanisms, such as ground level-falls. Elderly patients often present with significant co-morbidities impacting their operability, recovery, and survival. In the pediatric population, the problem can involve the long-term impact of improperly treated intra-articular fractures and early joint damage.[2] As the population ages, the treatment of these complex fractures has correlated with poor outcomes.[3]
Epidemiology
Distal femur fractures account for less than 1% of all fractures and about 3 to 6% of all femoral fractures.[1][4] The incidence of distal femur fractures has been reported to be 37 per 100000 people in the United States.[5] These fractures occur in a bimodal distribution: young males, particularly after high-energy motor trauma and elderly females. One study reported that 80% of patients 35 years of age or older with a distal femur fracture secondary to moderate trauma had evidence of generalized osteopenia.[6] Periprosthetic fractures about the distal femur have also become more common. The incidence of distal femur fractures around a primary total knee arthroplasty has been reported to be from 0.3% to 5.5%, and upwards to 30% after revision knee arthroplasty.[7]
Pathophysiology
The distal femur is defined as the region from the metaphyseal-diaphyseal junction to the articular surface of the knee, involving approximately the distal 15 cm of the femur. The shaft of the femur is a cylindrical shape and extends into two curved condyles at the distal end. When viewed from the axial plane, the shape of the distal femur is trapezoidal. The lateral cortex slopes at approximately 10 degrees, and the medial cortex slopes approximately 25 degrees.[8] The medial condyle of the distal femur extends more distal than the lateral condyle. The posterior portions of both of these condyles extend more posterior than the posterior cortex of the diaphysis of the femur. The femoral shaft, representing the anatomic axis of the femur, averages about 6 to 7 degrees of valgus to the knee joint.
The most common mechanism involves direct trauma to a flexed knee, typically seen in dashboard injuries during motor vehicle accidents. The deforming forces of distal femur fractures depend on the location of the fracture relative to the adductor tubercle. Generally, the hamstrings and extensor mechanism causes the fracture to shorten, and the adductor magnus displaces the fracture into varus. The two heads of the gastrocnemius muscle extend the distal fragment, resulting in an apex posterior angulation of the fracture. With intercondylar split fracture patterns, the two heads may also cause the distal condylar fragments to separate and rotate.
Soft tissue injuries are often associated with distal femur fractures. These may include ligamentous disruptions of the knee joint that are often difficult to diagnosis until the distal femur fracture has undergone stabilization. Controversy remains regarding the timing of treatment with concomitant cruciate ligament injuries. Options, including primary repair, ligament augmentation, and ligament reconstruction, are all made more difficult in the setting of a fracture and internal fixation devices. Polytrauma patients may also present with associated fractures to the tibia. Fractures of the distal femur with associated tibia plateau injury, referred to as a floating knee, often require CT imaging and aggressive treatment.
Distal femur fractures that result from a gunshot injury, high-energy trauma, or open injury present with a high risk for vascular injury. The femoral artery lies within the adductor canal, approximately 10 cm above the knee along the posterior medial cortex. Injuries associated with a knee dislocation increase the risk of injuring the popliteal artery.[9]
The incidence of distal femur fractures following total knee arthroplasty is increasing.[10] The integrity of the prosthesis determines treatment of these complex injuries. If the prosthesis is stable, treatment including open reduction and internal fixation or retrograde nailing are options. If the prosthesis is loose, revision arthroplasty with stemmed prosthesis is the best option.
History and Physical
Advanced trauma life support protocol, including a full trauma evaluation, is required for the assessment of any high energy mechanism injury. The clinical evaluation usually manifests as severe pain about the thigh and knee. Patients typically present with an inability to weight bear on the affected extremity. There may be noticeable deformity about the distal thigh and knee. A thorough evaluation of skin is mandatory to rule out the possibility of an open fracture, which may present in 5 to 10 percent of supracondylar fractures.[11] Tetanus prophylaxis and intravenous antibiotics should be administered immediately following an open fracture.[12] Early irrigation and debridement of the open fracture are necessary to prevent infection. Neurovascular examination of the affected extremity before and after reduction is essential. If there are differences in pulses between the injured and noninjured sides, or any suspicion for vascular compromise, ankle-brachial indices (ABI) should be obtained. CT angiography with vascular surgery consultation is necessary if vascular compromise is suspected (ABI less than 0.90, absent palpable pulses, or Doppler signals).[13] Elderly patients who suffered a trivial fall may receive non-emergent treatment. Conversely, in younger adults, distal femur fractures are often associated with other injuries as a result of the high-energy injury. Finally, the non-displaced distal femur fracture of the adolescent athlete can easily be missed and may present with other knee injuries.[14]
Evaluation
Imaging
Radiographs of the entire extremity, including the joints proximal and distal to the suspected injury, should be obtained when patients are hemodynamically stable to characterize the injury. Femur fractures are rarely a life or death emergency despite their associated impressive deformities. Traction views can help with characterizing the fracture pattern; however, this is very painful for the patient, and pain control is necessary before any manipulation. Contralateral femur films may be considered for pre-operative planning and templating.
At the time of planning for treatment, CT with coronal and sagittal reconstruction is recommended for complex fractures, fractures with intra-articular extension, and assessment for osteochondral fragments in the intercondylar notch. CT is a strong recommendation to asses for the Hoffa fracture, which is an intra-articular distal femoral fracture in the coronal plane that most commonly involves the lateral condyle with an incidence of 38.1%.[15] If choosing an external fixation construct for fixation, a CT scan should take place afterward.
CT angiography is indicated in the setting of decreased ipsilateral distal pulses despite re-alignment or distal pulses present with ABI below 0.90.[13] This imaging also merits consideration if there is an associated knee dislocation. Multi-slice helical CT angiography is a highly specific and sensitive study for the evaluation and management of lower extremity injuries.[16]
Classification
Classification of distal femur fractures may be descriptive, including extra-articular, intra-articular unicondylar, intra-condylar bicondylar, and pattern of fracture, including the degree of comminution.
The most commonly used fracture classification system used is the Orthopaedic Trauma Association classification.
The Orthopaedic Trauma Association Classification
33A - Extra-articular
- A1 - simple
- A2 - metaphyseal wedge
- A3 - metaphyseal complex
33B - Partial articular (a portion of the articular surface remains attached to the proximal shaft)
- B1 - lateral condyle
- B2 - medial condyle
- B3 - coronal plane (Hoffa fragment)
33C - Complete articular (articular fragment separated from the shaft)
- C1 – simple articular, simple metaphyseal
- C2 – simple articular, metaphyseal comminution
- C3 - metaphyseal and intra-articular comminution
Treatment / Management
Nonoperative
Indications for nonoperative management is reserved for stable, minimally displaced, and non-articular fractures. Management consists of a hinged kneed brace with emphasis on immediate range of motion to prevent stiffness and non-weight bearing for six weeks.[17] Other indications include non-ambulatory patients with significant comorbidities presenting with significant anesthesia/surgical risk. Management consists of splinting, bracing, or skeletal traction to prevent shortening. Complications include decubitus ulcers, venous thromboembolism, and considerable loss of knee function. Due to these devasting complications, studies support surgical intervention even for the non-ambulatory patient.[18](B2)
Chemical prophylaxis should be offered for all eligible patients to diminish the risk of venous thromboembolism, as early as permitted. The elderly population, especially, is at risk for high mortality and poor quality of life. An early conversation with patients, in non-equivocal terms about death and loss of autonomy, should be initiated immediately. Surgical treatments with the role in pain control is not a contraindication to palliation. Practitioners who are not educated or not comfortable should seek assistance to support patients, family, and team members.
External Fixation
External fixation is a temporizing measure for prompt restoration and stabilization of limb length, alignment, and rotation until the soft tissue can tolerate internal fixation.[19] Indications for external fixation include open wounds, poor skin healing potential, and patients too unstable to tolerate internal surgical fixation. Complications include pin-tract infection, deep infection, loss of reduction, malunion, and knee stiffness. Clinicians should avoid pin placement in the area of planned internal fixation if possible.(B2)
Open Reduction Internal Fixation
Options for open reduction internal fixation include fixed angled blade plate, sliding barrel condylar plate, condylar buttress plate, and locking plate. Indications for open reduction internal fixation include fracture displacement, intra-articular fractures, and fractures that have gone on to nonunion. Goals include anatomic reduction of the articular surface, restoration of limb alignment, length, and rotation with preservation of vascularity. The usual determination of surgical exposure and implant of choice are by fracture configuration and surgeon preference.
Accurate fracture reduction is critical for successful outcomes; this is achievable through direct or indirect methods. Indirect reduction of the fracture offers some advantages through minimal soft tissue stripping that improves fracture biology. Examples of indirect reduction methods include manual traction, pointed reduction forceps, universal femoral distractor, and using the periarticular plate to reduce the bone to the anatomically contoured plate with screws. The latter may be achieved by first using cortical screws to aid in reducing the bone to the plate, followed by locking screws to create a fixed angled device to increase stability. A combination of direct and indirect methods is also an option. For OTA 33 type B and C fractures with intraarticular displacement, a lateral arthrotomy may be used for direct anatomic joint reduction and restoration of the joint surface, followed by indirect reduction of the articular block to the femoral shaft. The use of fluoroscopy to reference Blumensaat's line can aid in plate placement on the distal femur. When placing the most distal and posterior screws, if the plate is too dorsal to Blumensaat's line, the screw has a high risk of violating the intercondylar notch.
Blade plate and Sliding barrel condylar plate
The 95-degree blade plate is a useful implant for fracture fixation of OTA 33 type A patterns, as well as for the stabilization of malunions and nonunions. The placement of the blade plate is often a technically demanding procedure because three planes must simultaneously be corrected. Condylar malalignment may result if the chisel and plate are incorrectly inserted. Sliding barrel condylar plates are devices based on the compression screw used for hip fractures. These devices allow for the ability to apply compression across the femoral condyles. They allow better purchase in osteoporotic bone and only need two planes of correction when compared to the blade plate. Potential disadvantages with this construct include its bulky size and the requirement to remove a large amount of bone from the lateral femoral condyle. Due to its bulky size, the plate may cause symptomatic hardware and knee symptoms. Clinical studies have generally shown good results with fixed angled blade plate and sliding barrel condylar plate devices with 82% reporting satisfactory to excellent results at 9.5 years for condylar plate and 81% good or excellent results for the dynamic condylar screw.[20][21] A recent study comparing the less invasive stabilization system (LISS) with minimally invasive sliding barrel condylar plates in the treatment of OTA 33 type A1 to C2 concluded that there was no advantage for locking plate designs.[22](A1)
Condylar Buttress Plating
A condylar buttress plate utilizes multiple lags screws for the treatment of condylar fractures. Advantages to these plates allow for the treatment of OTA 33 type B fractures. Disadvantages to these plates include not being a fixed-angle device and thereby relying on the friction of the bone-plate interface. Due to the eccentric mechanical axis of the femur, screw loosening can occur, causing the typical varus deformity.
Locking Plates
Locking plates have more recently become the workhorse for open reduction internal fixation. Modern plate designs have various screw fixation options, including unicortical or bicortical screws, cannulated locking and nonlocking screws, solid locking screws, and attachments of radiolucent targeting devices that allow for percutaneous fixation. Locking screws offer advantages because each screw is a fixed-angle device, thus augmenting the stability of the construct by securing the plate at multiple points and eliminating motion at the plate-bone interface. Studies have shown locking plates to be biomechanically superior to blade plates in both cyclic loading and ultimate strength.[23] Recent studies demonstrate acceptable failure rates of 9.3% for lateral compression plates.[24] Current surgical techniques recommend using a longer plate when possible, with a balanced spread of screws in the proximal segment.[25] No more than 50% of the available holes in the proximal segment should be filled when utilizing bridge mode. Risk factors for fixation failure include high-energy fracture with metaphyseal comminution, poor reduction of the fracture, poor plate position, and early weight-bearing before radiographic union.[26](B2)
Intramedullary Nailing
Intramedullary nail fixation has the benefit of providing a stable construct with minimal soft tissue and periosteum disruption. Antegrade and retrograde options are available depending on fracture characteristics. Pearls to successful intramedullary nailing include obtaining an optimal starting point to pass the reamer and maintaining reduction throughout the procedure. Blocking screws may be placed in the proximal or distal fragment to guide the trajectory of the nail and obtain satisfactory reduction.
Antegrade Nailing
Antegrade nailing is a good option for extraarticular OTA 33 type A fractures and some type C1 and C2 fractures.[27] The advantages of antegrade nailing include the ability to treat ipsilateral femoral shaft fractures with associated supracondylar femoral fractures with one device. Relative contraindications to antegrade nailing include OTA 33 type B3 and C3 fractures.[28](B2)
Retrograde Nailing
Retrograde nailing is a viable option for the treatment of distal femur fractures. The advantages of retrograde nailing include: the intramedullary nail is a load-sharing device compared to plate fixation, the nail may be inserted through smaller incisions causing less soft tissue disruption, and it allows for the treatment of ipsilateral hip and ipsilateral tibia fractures in the polytrauma patient. Retrograde nails of standard-length should extend to the level of the lesser trochanter to prevent a stress riser in the subtrochanteric region. Newer implants with options for multiple distal screw fixation allow for the restoration of the articular surface for simple intra-articular fractures. Biomechanical studies demonstrate that the number, orientation of the distal locking screws, and quality of distal screw purchase are essential components in determining the strength of a nail.[29] A recent study concluded that intramedullary nails might have superior outcomes compared to anatomic locking plate devices for fractures of the distal femur.[30] Potential disadvantages to retrograde nailing include knee sepsis, patellofemoral pain, and synovial metallosis from the nail or screw breakage. OTA 33 type C3 fractures with severe comminution may not be optimal for stabilization with a nail.
Bone Cement and Bone Grafts
Bone cement may serve as a useful adjunct for stable internal fixation of supracondylar distal femur fractures with severe osteoporosis.[31] There have been studies that have demonstrated good results with bone cement for distal femoral fractures in osteoporotic patients presenting with intraarticular extension.[32] Bone grafts are reasonable reconstructive options for patients who present with massive bone loss.[33] Bone grafts are also options for the treatment of aseptic nonunions. (B3)
Differential Diagnosis
The differential diagnosis of a distal femur fracture is rarely a problem. The identification of an acute deformity on a plain radiograph in the setting of trauma is rarely a challenge. In the context of chronic knee pain in a young athlete, a patient with limited verbal communication, or the setting of severe trauma, the timing of diagnosis may be the challenge. Similarly, the clinician should systematically approach repeated surveys of trauma patients after the stabilization of life-challenging issues.
Pertinent Studies and Ongoing Trials
The role of physical therapy in the elderly population is still a debate. At least one clinical - ClinicalTrials.gov Identifier: NCT02475941- is studying this topic: "Early Weight Bearing on Supracondylar Distal Femur Fractures in Elderly Patients."
From the surgical treatment properly speaking, several studies are on-going comparing the management of locked compression plating to retrograde intramedullary nailing in patients with distal femur fractures or distal peri-prosthetic femur fractures. One study focuses on the comparison between distal femur fixation to replacement in the geriatric population - ClinicalTrials.gov Identifier: NCT04076735.
Prognosis
The 1-year mortality rate for distal femur fractures in the elderly who undergo operative treatment has been reported to be from 13.4 to 35%.[34][35] Recovery for geriatric patients is often slow. This patient population is often frail and have other comorbidities which hamper healing. In terms of constructs, both intramedullary nailing and distal locking plates have shown good outcomes for distal femur fractures.[36][37]
Complications
Patients may complain of pain secondary to hardware presence; this may occur over the plate on the lateral femoral condyle where the iliotibial band may rub. Hardware pain can also result from medial screw irritation secondary to excessively long screws in contact with medial soft tissues.[38] Malunion is a common complication. Malunion of greater than 5 to 10 degrees affects knee mechanics, which may lead to arthritis of the medial and lateral compartments. While locking plates have proven to be successful at preventing varus collapse, fractures with significant metaphyseal comminution are at particularly high risk for failing and producing a varus malunion.[39] Fixation of the distal fragment into excessive extension or flexion may also result with ORIF. Correction of malunion is possible with supracondylar osteotomy. Nonunion is a substantial complication, with rates up to 20%.[25][26] Risk factors have been reported to include obesity, open fracture, infection, and the use of stainless steel. Treatment often consists of revision ORIF with bone autograft or changing fixation technique.[40] Infection can occur in up to 3 to 16% for closed fractures.[41][19] Infection should be treated with debridement, culture-specific antibiotics, and hardware removal if the fracture is stable. Range of motion loss is a common complication after distal femur fractures. Younger patients who had sustained high-energy trauma are at particularly high risk for this complication.[42]
Deterrence and Patient Education
Postoperatively, patients should begin gentle range of motion of the knee to prevent stiffness. Depending on the intraoperative stability, the affected extremity may be made non-weight bearing, touchdown weight-bearing, or partial weight-bearing for 10 to 12 weeks. Progressive weight-bearing as tolerated may begin after 12 weeks with the assistance of ambulatory devices if needed.
Enhancing Healthcare Team Outcomes
Distal femur fractures are best managed by an interprofessional team that includes the emergency department physician, orthopedic surgeon, internist, orthopedic nurses, and physical therapist. The majority of distal femur fractures require surgical intervention; thus, consultation of the orthopedic surgeon is essential. Vascular surgery requires a consult if there is any suspicion for vascular compromise to the limb. The management of the elderly patient requires advanced training and education in the handling of patients with co-morbidities and a significant change in their life trajectory. After surgery, patients need nursing care with prophylaxis against pressure sores and deep vein thrombosis. Nursing can also serve as a bridge between rehabilitative care and the treating clinician, as physical therapy is a vital part of rehabilitation. A social worker should be involved to ensure that the patient's home environment is safe and that the patient has support services. The recovery is often slow, and many patients need pain control; hence, a pharmacist may be helpful to educate the patient on modes of pain management. Open communication between the team members is vital to improving patient outcomes. These interprofessional team dynamics can improve patient outcomes. [Level 5]
Media
(Click Image to Enlarge)
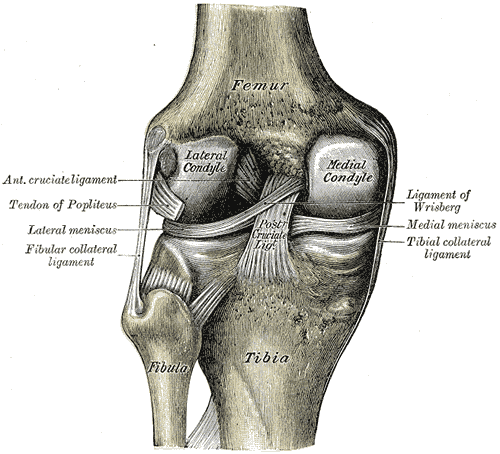
Interior Ligaments of the Left Knee. Anatomy includes anterior cruciate ligament, tendon of popliteus, lateral meniscus, fibular collateral ligament, ligament of Wrisberg, medial meniscus, tibial collateral ligament, posterior cruciate ligament, femur, tibia, and fibula.
Gray's Anatomy
(Click Image to Enlarge)

Distal femur fracture Image courtesy S Bhimji
(Click Image to Enlarge)
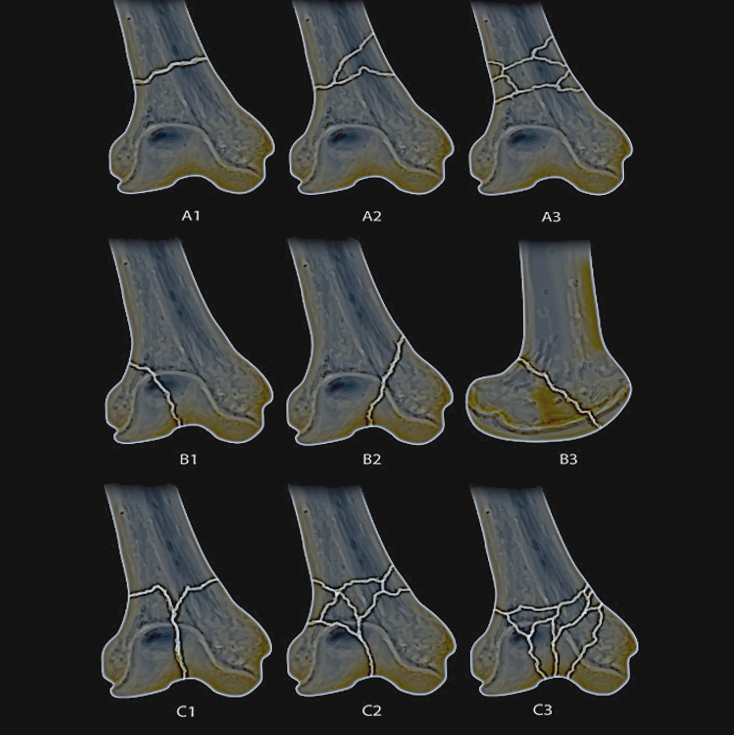
Distal femur fx classification Image courtesy S Bhimji MD
(Click Image to Enlarge)

Lateral view of a periprosthetic distal femur fracture about a cemented cruciate retaining total knee arthroplasty Contributed by Wesley Mesko, MD
(Click Image to Enlarge)

Retrograde femoral nail of periprosthetic distal femur fracture Contributed by Daniel R Mesko DO
References
Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE. The epidemiology of fractures of the distal femur. Injury. 2000 Sep:31 Suppl 3():C62-3 [PubMed PMID: 11052383]
Adams AJ, Mahmoud MAH, Wells L, Flynn JM, Arkader A. Physeal fractures of the distal femur: does a lower threshold for surgery lead to better outcomes? Journal of pediatric orthopedics. Part B. 2020 Jan:29(1):40-46. doi: 10.1097/BPB.0000000000000664. Epub [PubMed PMID: 31425335]
Shields E, Behrend C, Bair J, Cram P, Kates S. Mortality and Financial Burden of Periprosthetic Fractures of the Femur. Geriatric orthopaedic surgery & rehabilitation. 2014 Dec:5(4):147-53. doi: 10.1177/2151458514542281. Epub [PubMed PMID: 26246936]
Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006 Aug:37(8):691-7 [PubMed PMID: 16814787]
Level 2 (mid-level) evidenceZlowodzki M, Bhandari M, Marek DJ, Cole PA, Kregor PJ. Operative treatment of acute distal femur fractures: systematic review of 2 comparative studies and 45 case series (1989 to 2005). Journal of orthopaedic trauma. 2006 May:20(5):366-71 [PubMed PMID: 16766943]
Level 3 (low-level) evidenceArneson TJ, Melton LJ 3rd, Lewallen DG, O'Fallon WM. Epidemiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clinical orthopaedics and related research. 1988 Sep:(234):188-94 [PubMed PMID: 3409576]
Della Rocca GJ, Leung KS, Pape HC. Periprosthetic fractures: epidemiology and future projections. Journal of orthopaedic trauma. 2011 Jun:25 Suppl 2():S66-70. doi: 10.1097/BOT.0b013e31821b8c28. Epub [PubMed PMID: 21566478]
Butt WP, Samuel E. Radiologic anatomy of the proximal end of the femur. Journal of the Canadian Association of Radiologists. 1966 Jun:17(2):103-6 [PubMed PMID: 5945612]
Green NE, Allen BL. Vascular injuries associated with dislocation of the knee. The Journal of bone and joint surgery. American volume. 1977 Mar:59(2):236-9 [PubMed PMID: 845209]
Morwood MP, Gebhart SS, Zamith N, Mir HR. Outcomes of fixation for periprosthetic tibia fractures around and below total knee arthroplasty. Injury. 2019 Apr:50(4):978-982. doi: 10.1016/j.injury.2019.03.014. Epub 2019 Mar 15 [PubMed PMID: 30929804]
Dugan TR, Hubert MG, Siska PA, Pape HC, Tarkin IS. Open supracondylar femur fractures with bone loss in the polytraumatized patient - Timing is everything! Injury. 2013 Dec:44(12):1826-31. doi: 10.1016/j.injury.2013.03.018. Epub 2013 Apr 16 [PubMed PMID: 23601115]
Level 2 (mid-level) evidenceZalavras CG, Patzakis MJ. Open fractures: evaluation and management. The Journal of the American Academy of Orthopaedic Surgeons. 2003 May-Jun:11(3):212-9 [PubMed PMID: 12828451]
Boyce RH, Singh K, Obremskey WT. Acute Management of Traumatic Knee Dislocations for the Generalist. The Journal of the American Academy of Orthopaedic Surgeons. 2015 Dec:23(12):761-8. doi: 10.5435/JAAOS-D-14-00349. Epub 2015 Oct 22 [PubMed PMID: 26493970]
Pennock AT, Ellis HB, Willimon SC, Wyatt C, Broida SE, Dennis MM, Bastrom T. Intra-articular Physeal Fractures of the Distal Femur: A Frequently Missed Diagnosis in Adolescent Athletes. Orthopaedic journal of sports medicine. 2017 Oct:5(10):2325967117731567. doi: 10.1177/2325967117731567. Epub 2017 Oct 10 [PubMed PMID: 29051906]
Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, Benirschke SK. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. The Journal of bone and joint surgery. American volume. 2005 Mar:87(3):564-9 [PubMed PMID: 15741623]
Level 2 (mid-level) evidenceInaba K, Potzman J, Munera F, McKenney M, Munoz R, Rivas L, Dunham M, DuBose J. Multi-slice CT angiography for arterial evaluation in the injured lower extremity. The Journal of trauma. 2006 Mar:60(3):502-6; discussion 506-7 [PubMed PMID: 16531846]
Gwathmey FW Jr, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q. Distal femoral fractures: current concepts. The Journal of the American Academy of Orthopaedic Surgeons. 2010 Oct:18(10):597-607 [PubMed PMID: 20889949]
Cass J, Sems SA. Operative versus nonoperative management of distal femur fracture in myelopathic, nonambulatory patients. Orthopedics. 2008 Nov:31(11):1091 [PubMed PMID: 19226094]
Level 2 (mid-level) evidenceParekh AA, Smith WR, Silva S, Agudelo JF, Williams AE, Hak D, Morgan SJ. Treatment of distal femur and proximal tibia fractures with external fixation followed by planned conversion to internal fixation. The Journal of trauma. 2008 Mar:64(3):736-9. doi: 10.1097/TA.0b013e31804d492b. Epub [PubMed PMID: 18332816]
Level 2 (mid-level) evidenceKolb K, Grützner P, Koller H, Windisch C, Marx F, Kolb W. The condylar plate for treatment of distal femoral fractures: a long-term follow-up study. Injury. 2009 Apr:40(4):440-8. doi: 10.1016/j.injury.2008.08.046. Epub 2009 Mar 13 [PubMed PMID: 19285670]
Level 2 (mid-level) evidenceHuang HT, Huang PJ, Su JY, Lin SY. Indirect reduction and bridge plating of supracondylar fractures of the femur. Injury. 2003 Feb:34(2):135-40 [PubMed PMID: 12565021]
Level 2 (mid-level) evidenceCanadian Orthopaedic Trauma Society. Are Locking Constructs in Distal Femoral Fractures Always Best? A Prospective Multicenter Randomized Controlled Trial Comparing the Less Invasive Stabilization System With the Minimally Invasive Dynamic Condylar Screw System. Journal of orthopaedic trauma. 2016 Jan:30(1):e1-6. doi: 10.1097/BOT.0000000000000450. Epub [PubMed PMID: 26429408]
Level 1 (high-level) evidenceHiggins TF, Pittman G, Hines J, Bachus KN. Biomechanical analysis of distal femur fracture fixation: fixed-angle screw-plate construct versus condylar blade plate. Journal of orthopaedic trauma. 2007 Jan:21(1):43-6 [PubMed PMID: 17211268]
McDonald TC, Lambert JJ, Hulick RM, Graves ML, Russell GV, Spitler CA, Bergin PF. Treatment of Distal Femur Fractures With the DePuy-Synthes Variable Angle Locking Compression Plate. Journal of orthopaedic trauma. 2019 Sep:33(9):432-437. doi: 10.1097/BOT.0000000000001510. Epub [PubMed PMID: 31259799]
Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk factors for failure of locked plate fixation of distal femur fractures: an analysis of 335 cases. Journal of orthopaedic trauma. 2014 Feb:28(2):83-9. doi: 10.1097/BOT.0b013e31829e6dd0. Epub [PubMed PMID: 23760176]
Level 2 (mid-level) evidenceVallier HA, Hennessey TA, Sontich JK, Patterson BM. Failure of LCP condylar plate fixation in the distal part of the femur. A report of six cases. The Journal of bone and joint surgery. American volume. 2006 Apr:88(4):846-53 [PubMed PMID: 16595476]
Level 3 (low-level) evidenceLeung KS, Shen WY, So WS, Mui LT, Grosse A. Interlocking intramedullary nailing for supracondylar and intercondylar fractures of the distal part of the femur. The Journal of bone and joint surgery. American volume. 1991 Mar:73(3):332-40 [PubMed PMID: 2002070]
Level 2 (mid-level) evidenceButler MS, Brumback RJ, Ellison TS, Poka A, Bathon GH, Burgess AR. Interlocking intramedullary nailing for ipsilateral fractures of the femoral shaft and distal part of the femur. The Journal of bone and joint surgery. American volume. 1991 Dec:73(10):1492-502 [PubMed PMID: 1748698]
Wähnert D, Hoffmeier KL, von Oldenburg G, Fröber R, Hofmann GO, Mückley T. Internal fixation of type-C distal femoral fractures in osteoporotic bone. The Journal of bone and joint surgery. American volume. 2010 Jun:92(6):1442-52. doi: 10.2106/JBJS.H.01722. Epub [PubMed PMID: 20516320]
Hoskins W, Sheehy R, Edwards ER, Hau RC, Bucknill A, Parsons N, Griffin XL. Nails or plates for fracture of the distal femur? data from the Victoria Orthopaedic Trauma Outcomes Registry. The bone & joint journal. 2016 Jun:98-B(6):846-50. doi: 10.1302/0301-620X.98B6.36826. Epub [PubMed PMID: 27235531]
Benum P. The use of bone cement as an adjunct to internal fixation of supracondylar fractures of osteoporotic femurs. Acta orthopaedica Scandinavica. 1977 May:48(1):52-6 [PubMed PMID: 868487]
Struhl S, Szporn MN, Cobelli NJ, Sadler AH. Cemented internal fixation for supracondylar femur fractures in osteoporotic patients. Journal of orthopaedic trauma. 1990:4(2):151-7 [PubMed PMID: 2358929]
Nizegorodcew T, Palmieri G, Peruzzi M, Galli M. Allograft for the treatment of traumatic severe bone loss in the lateral femoral condyle: A case report. Injury. 2018 Dec:49 Suppl 4():S16-S20. doi: 10.1016/j.injury.2018.11.037. Epub 2018 Dec 3 [PubMed PMID: 30526946]
Level 3 (low-level) evidenceLoosen A, Fritz Y, Dietrich M. Surgical Treatment of Distal Femur Fractures in Geriatric Patients. Geriatric orthopaedic surgery & rehabilitation. 2019:10():2151459319860723. doi: 10.1177/2151459319860723. Epub 2019 Jul 2 [PubMed PMID: 31308992]
Myers P, Laboe P, Johnson KJ, Fredericks PD, Crichlow RJ, Maar DC, Weber TG. Patient Mortality in Geriatric Distal Femur Fractures. Journal of orthopaedic trauma. 2018 Mar:32(3):111-115. doi: 10.1097/BOT.0000000000001078. Epub [PubMed PMID: 29462121]
Thomson AB, Driver R, Kregor PJ, Obremskey WT. Long-term functional outcomes after intra-articular distal femur fractures: ORIF versus retrograde intramedullary nailing. Orthopedics. 2008 Aug:31(8):748-50 [PubMed PMID: 18714768]
Level 2 (mid-level) evidenceHartin NL, Harris I, Hazratwala K. Retrograde nailing versus fixed-angle blade plating for supracondylar femoral fractures: a randomized controlled trial. ANZ journal of surgery. 2006 May:76(5):290-4 [PubMed PMID: 16768683]
Level 1 (high-level) evidenceCollinge CA, Gardner MJ, Crist BD. Pitfalls in the application of distal femur plates for fractures. Journal of orthopaedic trauma. 2011 Nov:25(11):695-706. doi: 10.1097/BOT.0b013e31821d7a56. Epub [PubMed PMID: 21857537]
Sanders R, Swiontkowski M, Rosen H, Helfet D. Double-plating of comminuted, unstable fractures of the distal part of the femur. The Journal of bone and joint surgery. American volume. 1991 Mar:73(3):341-6 [PubMed PMID: 2002071]
Bellabarba C, Ricci WM, Bolhofner BR. Indirect reduction and plating of distal femoral nonunions. Journal of orthopaedic trauma. 2002 May:16(5):287-96 [PubMed PMID: 11972070]
Kregor PJ, Stannard JA, Zlowodzki M, Cole PA. Treatment of distal femur fractures using the less invasive stabilization system: surgical experience and early clinical results in 103 fractures. Journal of orthopaedic trauma. 2004 Sep:18(8):509-20 [PubMed PMID: 15475846]
Level 2 (mid-level) evidenceMoore TJ, Watson T, Green SA, Garland DE, Chandler RW. Complications of surgically treated supracondylar fractures of the femur. The Journal of trauma. 1987 Apr:27(4):402-6 [PubMed PMID: 3553608]
Level 2 (mid-level) evidence