Introduction
Extubation is removing an endotracheal tube, which is the last step in liberating a patient from the mechanical ventilator. To discuss the actual procedure of extubation, one also needs to understand how to assess readiness for weaning and management before and after extubation. Other terms related to extubation are 'weaning' and 'liberation.' Weaning is a gradual transition from full invasive ventilatory support to spontaneous ventilation with minimal support. Liberation, however, means the complete discontinuation of mechanical ventilation. The current trend is to use the term 'liberation' as opposed to 'weaning' in intensive care unit ventilator management because the goal is to liberate patients from the ventilator as soon as possible rather than weaning over several days to weeks. Weaning is more common in long-term, acute care settings.[1][2]
Indications
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Indications
All patients who are on mechanical ventilation for any reason require liberation as soon as possible. Clinicians should consider the cause of the patient's respiratory failure, prognosis, expected course of the disease, and the absence of any reasons to stay on mechanical ventilation for a longer time. Clinicians should start planning extubation as early as day one of intubation. Any patient who successfully passes the spontaneous breathing trial should be extubated unless there is a change in management plans.
Contraindications
Extubation is contraindicated in patients who are not candidates for initiating ventilator liberation strategy and in those who have failed the spontaneous breathing trial.
Generally, the following groups of patients are not candidates for liberation; however, individual cases vary.
- Acute respiratory failure needing active management: The cause of respiratory failure should be resolved or significantly improved even to consider placing patients on liberation pathways.
- Any patient with a PaO2/FiO2 ratio less than 150, needing FiO2 over 0.40 or positive end-expiratory pressure (PEEP) greater than 10, minute ventilation requirement greater than 15 L per minute, rapid shallow breathing index over 105 (shallow rapid breaths with higher respiratory rate and lower tidal volumes), excessive secretions, worsening chest imaging, are not ready for considering extubation.
- Patients should be able to maintain adequate oxygenation and ventilation with low-level respiratory support, which patients can manage spontaneously or be provided with non-invasive modalities.
- The patient should be able to protect the airway, maintain airway patency, have a strong cough, and have minimal secretions.
- The four most important things to remember are mental status, oxygenation, ventilation, and expectoration (acronym, MOVE).
- Any cardiovascular instability is a contraindication:
- Tachycardia (higher than 140) of any sort needs active management.
- Shock state of any etiology requiring higher doses of vasopressor support - patients can be safely extubated sometimes if they are on small doses of one vasopressor and no other contraindication.
- The patient should not have any active ischemia or pulmonary edema.
- A Glasgow coma scale (GCS) of less than 8 is a contraindication. In rare situations, patients with low GCS can be extubated if they have a good gag and cough and the absence of any other contraindications.
- For most patients considered for extubation, mental status should be alert, awake, and able to follow commands. There should be no other neurologic abnormality impairing the patient's ability to breathe spontaneously.
- Any acute brain injury (including an invasive intracranial pressure measuring device for raised intracranial pressure) where such an injury was the primary reason for intubation.
- Plans to return to the operating room needing general anesthesia in the next 24 hours. Extubation should not be attempted as the patient will be re-intubated for surgery and may remain on the ventilator for a few more days, depending on the outcomes of the surgery.
- Current use of paralytic agents for any reason.
- The presence of an open abdomen is generally a contraindication - if the patient is subject to rigorous SBT, it can jeopardize surgical management.
- Ongoing therapeutic hypothermia is also a contraindication.
Equipment
All equipment needed for intubation should be readily available, including 2 to 3 different sizes of endotracheal tubes, bag-mask with positive end expiratory-pressure valve, airway bougies, tube exchangers, traditional direct laryngoscope, video laryngoscope, flexible bronchoscope, drugs needed for induction, and suction catheters. Ideally, an airway bag should be available in all ICUs. It should include supraglottic airways, video laryngoscopes, and cricothyrotomy kits. Equipment for oxygenation post-extubation should be available, either a nasal cannula, oxygen mask, venturi mask, high-flow oxygen system, or continuous positive airway pressure/bilevel positive airway pressure.
Personnel
A respiratory therapist and bedside nurse should be present with the intensivist for extubation in the intensive care unit. A clinician skilled in airway management should be available in the operating room. An anesthesiologist should be available during the extubation of a difficult airway in either location.
Preparation
The preparation for extubation is a long process, which begins on the day of the patient's intubation and continues through the acute management of the primary problem that caused respiratory failure.
All ventilated patients in the intensive care unit should be assessed daily for readiness to wean. Physicians should determine the benefits of early weaning versus morbidity and mortality associated with failed extubation. A weaning/liberation protocol should be in place to achieve this goal (see Image. Safe Extubation Checklist). It should have the following components:
- The first step involves screening for any exclusion from initiating the liberation pathway. Please refer to the contraindications section to review all those criteria.
- The patient should be evaluated and screened with weaning parameters if there are no exclusions.
- If deemed a good candidate, the patient should start the spontaneous breathing trial (SBT).
- During the SBT and at the end of the SBT, assess for failure/pass of the SBT.
- If the patient passes the SBT, proceed with extubation without delay.
During the preparation phase of extubation, practitioners should pay attention to the following:
- Nocturnal rest with full ventilatory support before the morning of the trial.
- Ensure adequate nutrition.
- Avoid excessive intravascular volume and consider diuresis if not contraindicated.
- Treat any infections and avoid fever, as it may increase the ventilatory requirement.
- Ensure appropriate body position with head up and propped up if possible.
- Avoid obstipation, urinary retention, gastric distension, musculoskeletal pain, and severe anemia.
- If significant pleural effusion is present, consider tapping before extubation.
- Avoid chemical imbalances.
- Manage secretions aggressively before the SBT and even consider bronchoscopy to inspect airways to clean out inspissated secretions if appropriate.
Assessment of Readiness to Wean
The assessment considers all the contraindications above, including clinical improvement of the cause of respiratory failure, oxygenation and ventilation parameters, mental status, secretions, cardiovascular stability, and specific weaning parameters.
Weaning Parameters
Several weaning parameters have undergone assessment and use in clinical studies, which are helpful when taken into account with the overall clinical picture, but they are not very sensitive or specific when considered individually.[3][4]
- Minute ventilation (tidal volume x respiratory rate) of less than 10 L per minute only correlates with a positive predictive value of 50% and a negative predictive value of 40%.
- Maximum negative inspiratory pressure of greater than 30 cm of water is considered a measure of inspiratory muscle strength and a good predictor of weaning success, but this finding has not been replicated in studies.
- Static compliance (tidal volume/plateau pressure minus PEEP) has low negative and positive predictive values in the range of 50 to 60%.
- Occlusion pressure (P 0.1), which is the pressure at 0.1 seconds after initiation of a spontaneous breath, has shown conflicting results in studies.
- Reduction of venous oxygenation saturation (ScvO2 over 4.5%) after 30 minutes of the SBT in patients who failed their first T-tube SBT is an independent predictor of reintubation with a sensitivity of 88% and specificity of 95%.
- Rapid shallow breathing index (RSBI; respiratory rate/tidal volume) measured over one minute in a spontaneously breathing patient on low-level PEEP only has a higher sensitivity of 97% and moderate specificity of 65% for predicting patients who will subsequently pass the SBT.[5]
- The most common weaning parameters to consider when initiating the SBT are RSBI of less than 105, maximal inspiratory pressure (MIP) of less than -30 cm of water, and minute ventilation of less than 10 liters per minute.
Spontaneous Breathing Trial
Initiation of the weaning trial commences at the time of the first spontaneous breathing trial. The duration of the SBT can be between 30 minutes and 2 hours.[6][7] Several techniques can be used to conduct the SBT:
- T-tube (T-piece) trial
- Pressure support ventilation
- Automatic tube compensation
- Continuous positive airway pressure
- Automated weaning
Several studies have evaluated pressure support ventilation, automated tube compensation, CPAP, and T-piece trials and noted that none is superior to the other.[8][9][10]
T-tube Trial
This approach is a well-established method. It involves attaching the end of the endotracheal tube (ETT) to a short piece of tubing that acts as a reservoir and provides a connection to humidified fresh gas flow. This method is simple, well tested, and imposes a pulmonary workload comparable to that encountered after extubation; this is labor-intensive, and there is no monitoring of flow, pressure, or volume, and there are no alarms. A similar method called "flow by" can also be used when ventilating pressures, rate, and tidal volume are set to zero while the patient is still attached to the ventilator.
Pressure Support Ventilation
It is becoming a more widespread technique for conducting the SBT. Despite theoretical concern that pressure support ventilation may not mimic the true post-extubation workload and difficulty predicting the level of support necessary to compensate for resistive load completely, this does not appear problematic in practice.
Automatic Tube Compensation
In this method, the ventilator compensates for the degree of resistance provided by the ETT. It is available on most modern ventilators.
Continuous Positive Airway Pressure
Continuous positive airway pressure (CPAP) is said to increase functional residual capacity and maintain small airways. It is also beneficial for left ventricular dysfunction and has minimal side effects. Despite the potential risk that a patient may pass the SBT but experience cardiac failure on extubation, most clinicians are comfortable using low CPAP levels with other techniques mentioned earlier.
Automated Weaning
Automated weaning aims to reduce the requirement for clinician input in a weaning process and improve outcomes. These automated systems use closed-loop controls to interpret clinical data in real-time, gradually reduce pressure support, and perform the SBT. At least three different clinical trials and one meta-analysis have shown that the weaning time can be reduced with a computer-driven automated weaning protocol.[11][12][13][14][15][16]
Suitability for Extubation
If the patient has passed the SBT, they should undergo reassessment for the suitability of extubation. Many of these assessments may have been done at the start of the weaning trial or as a part of the daily assessment of the patient's readiness to wean.
The most important part of this assessment is assessing the ability of the patient to protect and maintain a patent airway.
- The patient should have an adequate level of consciousness: A GCS greater than 8 suggests a higher likelihood of successful extubation.
- The patient should have a strong cough:
- Most clinicians objectively determine the presence of a moderate to strong cough before extubation, although there are other objective measures like card moistening and spirometry testing for maximal expiratory pressure (MEP).
- The presence of a weak cough, measured as a cough peak flow of 60 L/min or less, is a strong independent risk factor for extubation failure.
- The patient should be assessed for the volume and thickness of respiratory secretions.
- The most common test for airway patency is the cuff-leak test which is neither sensitive nor specific.
- Providers need to ensure that they know the airway anatomy noted at the time of intubation, potentially difficult airway, and techniques used to intubate the patient - in the case of the known difficult airway, ensure to have all equipment available for difficult airway. If extra personnel is needed, they should be informed beforehand and be available at very short notice.
Technique or Treatment
- After a successful weaning trial/SBT, a decision is made to proceed with extubation.
- All necessary equipment should be available for extubation management, and the rest of the equipment should be available nearby in case extubation does not go as planned.
- The patient should be in an upright sitting position.
- Both the ETT and oral cavity are suctioned: if there is a subglottic suction, it should be utilized to remove all secretions above the ETT cuff. If no subglottic suction is available, use a small-bore catheter to insert on the side of the ETT and suction all secretions above the ETT cuff.
- The ETT is removed from the holder; when ready to be removed, ask the patient to take a deep breath and exhale. During exhalation, deflate the cuff and smoothly take out the ETT.
- If an orogastric tube is present, it is also removed alongside the ETT. This decision should be made before extubation, considering the need for oral medications and nutrition. Some patients may not be ready for oral intake and require a nasogastric tube placement upon removal of the orogastric tube.
- After removing the ETT, suction the oral cavity and ask the patient to take a deep breath and cough out all secretions.
- The patient should be placed on supplemental oxygen afterward.
- The patient should be observed very carefully over the next few hours.
- Frequent airway suction should be considered to prevent re-intubation.
- The timing of extubation (day, evening, night) depends on the institution and individual ICU, but the most critical factor to consider is the availability of adequately experienced personnel.
Strategies for Smooth Extubation and Smooth Emergence
- Deep extubation
- Endotracheal tube exchange to laryngeal mask airway (LMA)
- A “no-touch” extubation technique
- Pre-oxygenation with 100% Fraction of Inspired Oxygen (FiO2)
- Bite Blocks
- Pharmacotherapy: Intravenous or intracuff lidocaine, intravenous remifentanil, and dexmedetomidine [17]
Table. Grades of Recommendations Advocated During the Process of Extubation
| Grade B Recommendations | Grade D Recommendations |
|
|
Post-Extubation Management
The immediate post-extubation phase should be managed as carefully as the ventilated phase because the first 24 hours post-extubation are difficult and tenuous.
- Ensure adequate oxygenation: Consider nasal cannula, oxygen mask, full face mask, and venturi mask as appropriate to ensure good O2 supply.
- In recent times, high-flow oxygen systems have gained popularity in selected patients with hypoxemic respiratory failure, and studies have shown to reduce the re-intubation rate.
- If needed, consider CPAP/BPAP for selected high-risk patients to avoid re-intubation.
- Ensure adequate secretion management, encourage coughing and deep breathing, and maintain airway hydration and the patient's central airway.
- Use adequate bronchodilators as needed.
- Encourage sitting up position and mobility if no other contraindications exist.
- Carefully introduce oral feeding. In at-risk patients, continue enteral feeding with a nasogastric tube until the patient is deemed safe to swallow and tolerate food orally.
Complications
Adverse events relating to the procedure can be dichotomized into 3 categories:
- Respiratory: Exaggerated laryngeal reflexes causing coughing, bucking, or laryngospasm; aspiration, secondary to residual effects of drugs and inadequate relaxation, is the major cause of mortality as well as malpractice claims due to anesthesia-related adverse events
- Traumatic: Injury to the larynx, vocal cords, laryngeal nerves, dental trauma, lingual trauma, and emotional distress
- Hemodynamic: Post-extubation hemodynamic shift and increased intra-thoracic pressure following vigorous coughing [17]
The most feared complications of extubation are the failure and immediate need for re-intubation and post-extubation stridor.
Extubation Failure
Extubation failure and the need to be re-intubated within 48 hours are noted in 10 to 20% of patients despite passing a spontaneous breathing trial and undergoing planned extubation.[18] Twelve to 14% of planned extubations. Extubation failure increases the length of mandatory ventilation, odds of the need for tracheostomy, medical expenditure, and the risk of mortality.[18][19] Risk factors for reintubation include a weak cough and frequent suctioning. Additional features that may predict reintubation include a rapid shallow breathing index over 58 breaths per minute per liter, a positive fluid balance during the 24 hours preceding extubation, and pneumonia as the reason for the initial intubation. Patients aged 65 and older with severe chronic cardiac or respiratory disease appear to be at particularly high risk for extubation failure. Extubation failure carries a higher risk of intensive care unit mortality.[20][21]. Recently, the use of non-invasive ventilation (NIV), mostly in the form of BPAP, has gained prominence. Current evidence favors prophylactic use of NIV immediately after extubation to prevent reintubation in only selected high-risk patients, like chronic obstructive pulmonary disease and hypercapnia. Otherwise, NIV use for post-extubation respiratory failure has not been shown to reduce reintubation rate or intensive care unit mortality.[22][23] In addition to using NIV, high-flow oxygen systems have gained popularity over the last few years in selected patients with hypoxemic respiratory failure. Studies have shown to reduce the re-intubation rate.[24][25][26][27][28][29]
Various Clinical Parameters to Predict the Outcome Following Extubation
Glasgow coma scale-Glasgow Coma Scale before extubation has been observed to be the most significant variable governing the outcome following extubation.[18][30][31]
- Cough strength, level and consistency of secretion, and status of gag reflex [31]
- Indexes such as heart rate, acidosis, consciousness, oxygenation, and respiratory rate (HACOR) [32]
- Point of care holistic ultrasound- to assess left ventricular function), number of B-lines, and diaphragm thickening fraction; diaphragmatic excursion with a cut-off value of 1.25 cm and diaphragmatic thickening fraction with a cut-off value of 21.5% indexes during the diaphragmatic US have high positive predictive values [33][34][35][36]
- Synchronization between the thoracic and the abdominal wall movement[36]
- Changes in ΔPCO2 (Δ - ΔPCO2) and central venous oxygen saturation (ΔScvO2) during spontaneous breathing trials[36]
Weaning Failure
Weaning failure means that the patient cannot tolerate the SBT, which is different from extubation failure, where the patient can pass the spontaneous breathing trial leading to successful extubation, which later fails. An international consensus conference proposed a classification of patients based on the difficulty and length of the weaning process.[1] Accordingly, patients are categorized into three groups: simple, difficult, and prolonged weaning.[1] The simple weaning group (30% to 58% of patients) is easy to wean and able to be extubated after the first SBT. The difficult weaning group (26 to 40% of patients) requires up to 3 SBTs or up to 7 days to achieve successful weaning. Both of these groups have relatively lower mortality of 0% to 13%. The prolonged weaning group (6% to 30% of patients) requires more than 3 SBTs or more than seven days to achieve successful weaning. The third group has a higher mortality of 13% to 22%. Any weaning failure should prompt physicians to comprehensively assess the patient for all potential problems that can cause weaning failure. Subsequent SBT should only occur when these presumed predisposing factors have been addressed.[37][38]
Unexpected Extubation
A systematic review and meta-analysis have shown the pooled prevalence of unplanned endotracheal extubation at around 7%, with almost 70% occurring despite being preventable.[39] Preventive measures such as restraint and proper fixation of the tracheal tube are paramount to preventing such adverse events.[39]
Post-Extubation Stridor
Post-extubation stridor is uncommon and seen only in less than 10% of unselected critically ill patients and correlates with increased rates of reintubation, prolonged duration of mechanical ventilation, and longer length of intensive care unit stay. Stridor is the result of laryngeal edema.
Several identified risk factors include:
- Prolonged intubation (36 hours to 6 days or more)
- Older adults: 80 years and older
- A large ETT (greater than 8 mm in men and over 7 mm in women)
- A ratio of ETT to the laryngeal diameter of more than 45%
- A GCS score higher than 8 or traumatic intubation
- Female sex
- Medical history of asthma
- Improper fixation of the tube
- Inadequate or lack of sedation
- Aspiration
- The presence of an orogastric or nasogastric tube
The cuff-leak test is used to predict the occurrence of post-extubation stridor.[40] It should be performed if any of the risks mentioned above are identified. Some providers do the cuff-leak test regularly, but there is insufficient evidence to suggest its regular use.
The 2 methods of performing the cuff-leak test are:
- Qualitatively by just listening to the leak of air by a stethoscope over the upper trachea on deflation of the balloon.
- Quantitatively, placing the patient on volume control mode and calculating the difference between inspired and expired air. If the cuff leak is less than 110 mL or less than 25% of the delivered tidal volume, it suggests an increased risk of laryngeal edema.
Management of Post-extubation Stridor
For patients with no cuff leak when tested before extubation, a short course of steroids (methylprednisolone 20 mg every 4 hours for four doses) may be helpful. This course has support from a few studies and meta-analyses.[41][42] For patients who develop post-extubation stridor, nebulized epinephrine, intravenous methylprednisolone, high flow O2, and CPAP are options if clinically stable. Otherwise, prompt reintubation is warranted if significant airway obstruction is suspected. Following reintubation, a short course of steroids is the recommendation, with a re-assessment of the cuff leak. If a leak is present, extubation is generally safe. If cuff leak is reduced or absent, extubation over an airway exchange catheter should be considered, usually in consultation with bedside anesthesiology or an ear, nose, and throat consultant.[43]
Clinical Significance
Intubation and extubation are both critical aspects of the hospital management course for any critically ill patient and require documentation in electronic medical records with dates and times along with the complications and difficulties encountered.
Enhancing Healthcare Team Outcomes
The ventilator liberation process is long and involves many factors that require the attention of multiple members of the patient interprofessional care team. This team includes clinicians, nursing, and respiratory technicians. Coordination between different providers is essential. The SBT cannot be conducted without first conducting a spontaneous awakening trial.[44][45] This trial requires close coordination between the bedside nurse and the bedside respiratory therapist. As a part of the daily morning assessments, "sedation vacation" should be included to the point that the patient is alert, awake, and able to follow commands.[46] While the nurse is doing daily sedation vacations or spontaneous awakening trials, the respiratory therapist assesses readiness to wean and initiate the spontaneous breathing trial.
Communication between all team members is crucial so everyone knows their roles and responsibilities. A team-centered, interprofessional approach to care during extubation that includes physicians, nurses, respiratory therapists, and pharmacists is the best approach to achieving a positive patient outcome, irrespective of the events during extubation. Several studies have demonstrated a significant reduction in the intensive care unit length of stay and ventilatory days if the team follows certain protocols and policies, although other studies have argued against using protocolized weaning. In practical terms, protocols save significant time in the decision-making process and facilitate quicker liberation. All patients need to have a respiratory therapy-driven liberation pathway in place, followed by all patients except when ordered by the physician-in-charge not to follow.[47][48][49]
The American Thoracic Society and the American College of Chest Physicians Clinical Practice Guidelines for Liberation from Mechanical Ventilation in Critically Ill Adults
The summary of these clinical practice guidelines applicable to acutely hospitalized adults on mechanical ventilators for more than 24 hours is as follows:
- Management with a ventilator liberation protocol is suggested.
- Protocolized rehabilitation directed towards early mobilization is suggested.
- Performance of the cuff-leak test is suggested in those who meet the criteria for extubation but are deemed a high risk for the complication of post-extubation stridor.
- Administration of systemic steroids for at least 4 hours before extubation is suggested in those who fail the cuff-leak test but are otherwise ready to be extubated.[42]
Although the recommendations suggested by the American Thoracic Society and the American College of Chest Physicians, published in 2017, are conditional and not strong, they certainly will benefit healthcare professionals in decision-making in the ICU setting. The chapter on the approach to extubation from mechanical ventilation by Alistair Nichol and colleagues in the book "Evidence-Based Practice of Critical Care" is an essential reference for healthcare professionals involved in managing critically ill patients.
Media
(Click Image to Enlarge)
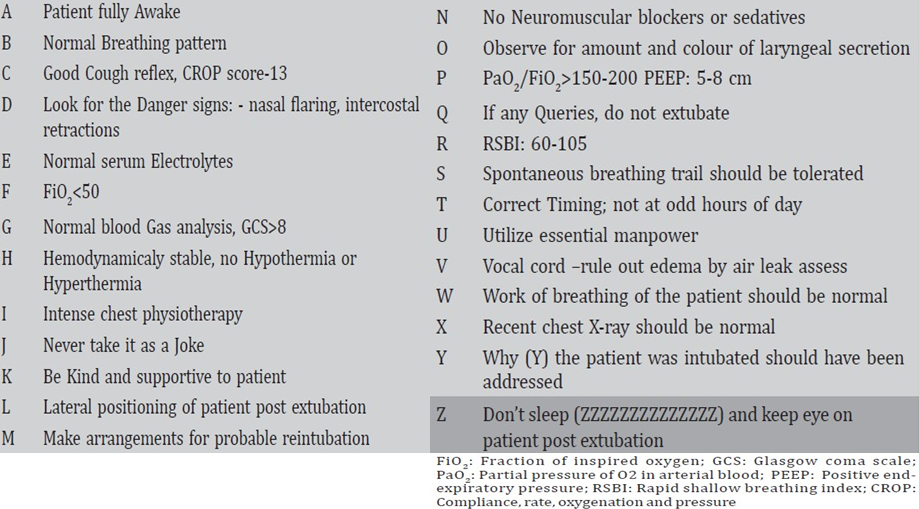
Safe Extubation Checklist
Munakomi S, Tamrakar K. Introducing 'A-Z' algorithm for extubation. Int J Stud Res. 2014;4:56-57.
References
Boles JM,Bion J,Connors A,Herridge M,Marsh B,Melot C,Pearl R,Silverman H,Stanchina M,Vieillard-Baron A,Welte T, Weaning from mechanical ventilation. The European respiratory journal. 2007 May; [PubMed PMID: 17470624]
Peñuelas Ó,Thille AW,Esteban A, Discontinuation of ventilatory support: new solutions to old dilemmas. Current opinion in critical care. 2015 Feb [PubMed PMID: 25546535]
Level 3 (low-level) evidenceYang KL,Tobin MJ, A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. The New England journal of medicine. 1991 May 23; [PubMed PMID: 2023603]
Level 1 (high-level) evidenceSahn SA,Lakshminarayan S, Bedside criteria for discontinuation of mechanical ventilation. Chest. 1973 Jun; [PubMed PMID: 4514488]
Tanios MA,Nevins ML,Hendra KP,Cardinal P,Allan JE,Naumova EN,Epstein SK, A randomized, controlled trial of the role of weaning predictors in clinical decision making. Critical care medicine. 2006 Oct [PubMed PMID: 16878032]
Level 1 (high-level) evidenceEsteban A,Alía I,Tobin MJ,Gil A,Gordo F,Vallverdú I,Blanch L,Bonet A,Vázquez A,de Pablo R,Torres A,de La Cal MA,Macías S, Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. American journal of respiratory and critical care medicine. 1999 Feb [PubMed PMID: 9927366]
Level 1 (high-level) evidenceVallverdú I,Calaf N,Subirana M,Net A,Benito S,Mancebo J, Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. American journal of respiratory and critical care medicine. 1998 Dec [PubMed PMID: 9847278]
Brochard L,Rauss A,Benito S,Conti G,Mancebo J,Rekik N,Gasparetto A,Lemaire F, Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. American journal of respiratory and critical care medicine. 1994 Oct; [PubMed PMID: 7921460]
Level 1 (high-level) evidenceEsteban A,Frutos F,Tobin MJ,Alía I,Solsona JF,Valverdú I,Fernández R,de la Cal MA,Benito S,Tomás R, A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. The New England journal of medicine. 1995 Feb 9; [PubMed PMID: 7823995]
Level 1 (high-level) evidenceMolina-Saldarriaga FJ,Fonseca-Ruiz NJ,Cuesta-Castro DP,Esteban A,Frutos-Vivar F, [Spontaneous breathing trial in chronic obstructive pulmonary disease: continuous positive airway pressure (CPAP) versus T-piece]. Medicina intensiva. 2010 Oct [PubMed PMID: 20452705]
Level 1 (high-level) evidenceClavieras N,Wysocki M,Coisel Y,Galia F,Conseil M,Chanques G,Jung B,Arnal JM,Matecki S,Molinari N,Jaber S, Prospective randomized crossover study of a new closed-loop control system versus pressure support during weaning from mechanical ventilation. Anesthesiology. 2013 Sep [PubMed PMID: 23619172]
Level 1 (high-level) evidenceLellouche F,Mancebo J,Jolliet P,Roeseler J,Schortgen F,Dojat M,Cabello B,Bouadma L,Rodriguez P,Maggiore S,Reynaert M,Mersmann S,Brochard L, A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. American journal of respiratory and critical care medicine. 2006 Oct 15 [PubMed PMID: 16840741]
Level 2 (mid-level) evidenceRose L,Presneill JJ,Johnston L,Cade JF, A randomised, controlled trial of conventional versus automated weaning from mechanical ventilation using SmartCare/PS. Intensive care medicine. 2008 Oct [PubMed PMID: 18575843]
Level 3 (low-level) evidenceBurns KE,Meade MO,Lessard MR,Hand L,Zhou Q,Keenan SP,Lellouche F, Wean earlier and automatically with new technology (the WEAN study). A multicenter, pilot randomized controlled trial. American journal of respiratory and critical care medicine. 2013 Jun 1 [PubMed PMID: 23525929]
Level 3 (low-level) evidenceSchädler D,Engel C,Elke G,Pulletz S,Haake N,Frerichs I,Zick G,Scholz J,Weiler N, Automatic control of pressure support for ventilator weaning in surgical intensive care patients. American journal of respiratory and critical care medicine. 2012 Mar 15 [PubMed PMID: 22268137]
Level 1 (high-level) evidenceRose L,Schultz MJ,Cardwell CR,Jouvet P,McAuley DF,Blackwood B, Automated versus non-automated weaning for reducing the duration of mechanical ventilation for critically ill adults and children: a cochrane systematic review and meta-analysis. Critical care (London, England). 2015 Feb 24 [PubMed PMID: 25887887]
Level 1 (high-level) evidenceWong TH,Weber G,Abramowicz AE, Smooth Extubation and Smooth Emergence Techniques: A Narrative Review. Anesthesiology research and practice. 2021; [PubMed PMID: 33510786]
Level 3 (low-level) evidenceTorrini F,Gendreau S,Morel J,Carteaux G,Thille AW,Antonelli M,Mekontso Dessap A, Prediction of extubation outcome in critically ill patients: a systematic review and meta-analysis. Critical care (London, England). 2021 Nov 15; [PubMed PMID: 34782003]
Level 1 (high-level) evidenceCinotti R,Mijangos JC,Pelosi P,Haenggi M,Gurjar M,Schultz MJ,Kaye C,Godoy DA,Alvarez P,Ioakeimidou A,Ueno Y,Badenes R,Suei Elbuzidi AA,Piagnerelli M,Elhadi M,Reza ST,Azab MA,McCredie V,Stevens RD,Digitale JC,Fong N,Asehnoune K,ENIO Study Group, the PROtective VENTilation network, the European Society of Intensive Care Medicine, the Colegio Mexicano de Medicina Critica, the Atlanréa group and the Société Française d’Anesthésie-Réanimation–SFAR research network., Extubation in neurocritical care patients: the ENIO international prospective study. Intensive care medicine. 2022 Aug 29; [PubMed PMID: 36038713]
Epstein SK,Ciubotaru RL,Wong JB, Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997 Jul [PubMed PMID: 9228375]
Level 2 (mid-level) evidenceThille AW,Harrois A,Schortgen F,Brun-Buisson C,Brochard L, Outcomes of extubation failure in medical intensive care unit patients. Critical care medicine. 2011 Dec [PubMed PMID: 21765357]
Agarwal R,Aggarwal AN,Gupta D,Jindal SK, Role of noninvasive positive-pressure ventilation in postextubation respiratory failure: a meta-analysis. Respiratory care. 2007 Nov [PubMed PMID: 17971250]
Level 1 (high-level) evidenceGirault C,Bubenheim M,Abroug F,Diehl JL,Elatrous S,Beuret P,Richecoeur J,L'Her E,Hilbert G,Capellier G,Rabbat A,Besbes M,Guérin C,Guiot P,Bénichou J,Bonmarchand G, Noninvasive ventilation and weaning in patients with chronic hypercapnic respiratory failure: a randomized multicenter trial. American journal of respiratory and critical care medicine. 2011 Sep 15 [PubMed PMID: 21680944]
Level 1 (high-level) evidenceMaggiore SM,Idone FA,Vaschetto R,Festa R,Cataldo A,Antonicelli F,Montini L,De Gaetano A,Navalesi P,Antonelli M, Nasal high-flow versus Venturi mask oxygen therapy after extubation. Effects on oxygenation, comfort, and clinical outcome. American journal of respiratory and critical care medicine. 2014 Aug 1 [PubMed PMID: 25003980]
Level 1 (high-level) evidenceXu Z,Li Y,Zhou J,Li X,Huang Y,Liu X,Burns KEA,Zhong N,Zhang H, High-flow nasal cannula in adults with acute respiratory failure and after extubation: a systematic review and meta-analysis. Respiratory research. 2018 Oct 16 [PubMed PMID: 30326893]
Level 1 (high-level) evidenceMaggiore SM,Battilana M,Serano L,Petrini F, Ventilatory support after extubation in critically ill patients. The Lancet. Respiratory medicine. 2018 Dec [PubMed PMID: 30629933]
Thille AW,Muller G,Gacouin A,Coudroy R,Demoule A,Sonneville R,Beloncle F,Girault C,Dangers L,Lautrette A,Cabasson S,Rouzé A,Vivier E,Le Meur A,Ricard JD,Razazi K,Barberet G,Lebert C,Ehrmann S,Picard W,Bourenne J,Pradel G,Bailly P,Terzi N,Buscot M,Lacave G,Danin PE,Nanadoumgar H,Gibelin A,Zanre L,Deye N,Ragot S,Frat JP, High-flow nasal cannula oxygen therapy alone or with non-invasive ventilation during the weaning period after extubation in ICU: the prospective randomised controlled HIGH-WEAN protocol. BMJ open. 2018 Sep 5 [PubMed PMID: 30185583]
Level 1 (high-level) evidenceNi YN,Luo J,Yu H,Liu D,Liang BM,Yao R,Liang ZA, Can high-flow nasal cannula reduce the rate of reintubation in adult patients after extubation? A meta-analysis. BMC pulmonary medicine. 2017 Nov 17 [PubMed PMID: 29149868]
Level 1 (high-level) evidenceFernando SM,Tran A,Sadeghirad B,Burns KEA,Fan E,Brodie D,Munshi L,Goligher EC,Cook DJ,Fowler RA,Herridge MS,Cardinal P,Jaber S,Møller MH,Thille AW,Ferguson ND,Slutsky AS,Brochard LJ,Seely AJE,Rochwerg B, Noninvasive respiratory support following extubation in critically ill adults: a systematic review and network meta-analysis. Intensive care medicine. 2022 Feb; [PubMed PMID: 34825256]
Level 1 (high-level) evidenceIgarashi Y,Ogawa K,Nishimura K,Osawa S,Ohwada H,Yokobori S, Machine learning for predicting successful extubation in patients receiving mechanical ventilation. Frontiers in medicine. 2022; [PubMed PMID: 36035403]
Mogase LG,Koto MZ, Failed extubation in a tertiary-level hospital intensive care unit, Pretoria, South Africa. The Southern African journal of critical care : the official journal of the Critical Care Society. 2021; [PubMed PMID: 35517852]
Pande RK,Sharma J, Heart Rate, Acidosis, Consciousness, Oxygenation, and Respiratory Rate: A Perfect Weaning Index or Just a New Kid on the Block. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2022 Aug; [PubMed PMID: 36042771]
Kundu R,Baidya D,Anand R,Maitra S,Soni K,Subramanium R, Integrated ultrasound protocol in predicting weaning success and extubation failure: a prospective observational study. Anaesthesiology intensive therapy. 2022; [PubMed PMID: 35413786]
Level 2 (mid-level) evidenceArslan G,Besci T,Duman M, Point of care diaphragm ultrasound in mechanically ventilated children: A predictive tool to detect extubation failure. Pediatric pulmonology. 2022 Jun; [PubMed PMID: 35362674]
Elshazly MI,Kamel KM,Elkorashy RI,Ismail MS,Ismail JH,Assal HH, Role of Bedside Ultrasonography in Assessment of Diaphragm Function as a Predictor of Success of Weaning in Mechanically Ventilated Patients. Tuberculosis and respiratory diseases. 2020 Oct; [PubMed PMID: 32871066]
Alam MJ,Roy S,Iktidar MA,Padma FK,Nipun KI,Chowdhury S,Nath RK,Rashid HO, Diaphragm ultrasound as a better predictor of successful extubation from mechanical ventilation than rapid shallow breathing index. Acute and critical care. 2022 Feb; [PubMed PMID: 35081706]
Routsi C,Stanopoulos I,Kokkoris S,Sideris A,Zakynthinos S, Weaning failure of cardiovascular origin: how to suspect, detect and treat-a review of the literature. Annals of intensive care. 2019 Jan 9 [PubMed PMID: 30627804]
Fadila M,Regunath H, Ventilator Weaning . 2019 Jan [PubMed PMID: 28613464]
Wu J,Liu Z,Shen D,Luo Z,Xiao Z,Liu Y,Huang H, Prevention of unplanned endotracheal extubation in intensive care unit: An overview of systematic reviews. Nursing open. 2022 Aug 15; [PubMed PMID: 35971250]
Level 3 (low-level) evidencePrinianakis G,Alexopoulou C,Mamidakis E,Kondili E,Georgopoulos D, Determinants of the cuff-leak test: a physiological study. Critical care (London, England). 2005 Feb [PubMed PMID: 15693963]
Kuriyama A, Umakoshi N, Sun R. Prophylactic Corticosteroids for Prevention of Postextubation Stridor and Reintubation in Adults: A Systematic Review and Meta-analysis. Chest. 2017 May:151(5):1002-1010. doi: 10.1016/j.chest.2017.02.017. Epub 2017 Feb 21 [PubMed PMID: 28232056]
Level 1 (high-level) evidenceGirard TD,Alhazzani W,Kress JP,Ouellette DR,Schmidt GA,Truwit JD,Burns SM,Epstein SK,Esteban A,Fan E,Ferrer M,Fraser GL,Gong MN,Hough CL,Mehta S,Nanchal R,Patel S,Pawlik AJ,Schweickert WD,Sessler CN,Strøm T,Wilson KC,Morris PE, An Official American Thoracic Society/American College of Chest Physicians Clinical Practice Guideline: Liberation from Mechanical Ventilation in Critically Ill Adults. Rehabilitation Protocols, Ventilator Liberation Protocols, and Cuff Leak Tests. American journal of respiratory and critical care medicine. 2017 Jan 1; [PubMed PMID: 27762595]
Level 1 (high-level) evidenceMort TC, Continuous airway access for the difficult extubation: the efficacy of the airway exchange catheter. Anesthesia and analgesia. 2007 Nov [PubMed PMID: 17959966]
Kress JP, Pohlman AS, O'Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. The New England journal of medicine. 2000 May 18:342(20):1471-7 [PubMed PMID: 10816184]
Level 1 (high-level) evidenceKress JP,Gehlbach B,Lacy M,Pliskin N,Pohlman AS,Hall JB, The long-term psychological effects of daily sedative interruption on critically ill patients. American journal of respiratory and critical care medicine. 2003 Dec 15 [PubMed PMID: 14525802]
Sharma S,Valentino III DJ, Sedation Vacation in the ICU . 2019 Jan [PubMed PMID: 30020699]
Blackwood B,Burns KE,Cardwell CR,O'Halloran P, Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. The Cochrane database of systematic reviews. 2014 Nov 6 [PubMed PMID: 25375085]
Level 1 (high-level) evidenceBlackwood B,Alderdice F,Burns K,Cardwell C,Lavery G,O'Halloran P, Use of weaning protocols for reducing duration of mechanical ventilation in critically ill adult patients: Cochrane systematic review and meta-analysis. BMJ (Clinical research ed.). 2011 Jan 13 [PubMed PMID: 21233157]
Level 1 (high-level) evidenceKollef MH,Shapiro SD,Silver P,St John RE,Prentice D,Sauer S,Ahrens TS,Shannon W,Baker-Clinkscale D, A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Critical care medicine. 1997 Apr; [PubMed PMID: 9142019]
Level 1 (high-level) evidence