Introduction
Erythema ab igne (EAI) is a cutaneous rash related to chronic long-term heat exposure under the heat required for thermal burns (see Image. Erythema ab Igne, Back).[1] Erythema ab igne additionally carries a risk of malignant transformation; however, this is more likely in specific situations, such as coal-fire-related heat dermatosis.[1] EAI was previously a common entity in its initial discovery, where it was related to exposure to heat stoves and other direct sources of heat, such as coal fires; however, nowadays, it is more strongly associated with chronic exposure to electronics, such as laptops or space heaters, particularly in houses without central heating.[2]
There are many reports of exposure to various other electronics; however, the main uniting feature is that they all imply chronic exposure to a heat source, including virtual headsets and space heaters, which has increased during the COVID-19 pandemic.[3][4][5] Importantly, chronic exposure to heat sources is under the level required for thermal burns, which is reported in situations where the temperature remains below 45C.[1]
Patients often report a history of some external source of contact, which leads to vasodilation that is reticulated, which corresponds to the venous plexus pattern of the disease process.[6] Thus, the morphology of EAI is characterized by a localized reticulated and erythematous patch with some hyperpigmentation and—more rarely—hyperkeratosis.[7] The diagnosis should be clinical, but morphology and distribution provide significant clues. For instance, EAI often appears on the lower back, where people may use a heating pad. Thus, this may indicate that the patient has underlying musculoskeletal issues.[8] Another natural anatomic location is the abdomen, where patients may use a heating pack or even place their laptops in cases of internal pain, such as that from pancreatitis or vomiting.[9][10]
Finally, space heaters often appear on the anterior legs.[11] However, attention should also be paid to other areas, such as the anterior thighs, in laptop use cases.[12] While the rash is most often benign, its presence can indicate chronic inflammation or, less commonly, systemic illness and should prompt further investigation. Furthermore, careful inspection of the rash may yield evidence of possible pre-malignant transformation and should prompt referral for biopsy if indicated.[13] Treatment is often observation, though some studies suggest more intensive treatment, particularly in the case of malignant transformation.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The rash is nearly always associated with an external heating source and is classified as a chronic environmental dermatosis.[2] The presumed etiology has changed with time. Previously, the rash was correlated with open fires, wood-burning stoves, and kerosene lamps; thus, it was associated with a period that preceded central heating.[8] However, etiologic sources have changed to include laptops and other electronics.[14][9] Ultimately, the etiology can be remembered as chronic heat exposure under the temperature required to produce burns.[2]
Although the direct cause of erythema ab igne is external heat exposure, the cause of rashes in unique areas may be more descriptive. For instance, some people have EAI in areas of direct heat exposure from space heaters or heating pads, such as on the anterior legs or the lower back.[15][16][17] Yet, the presence of EAI in other areas may suggest a deeper underlying cause. For example, the presence of EAI on the face or ears may implore the clinician to ask further about electronics, the presence on the abdomen may motivate the clinician to ask about internal abdominal pain that causes the patient to use heat there, and the presence of EAI over other areas should cause an exploration of external heat application, its avoidance, and for what reason heat is being used.[18][19][20][21][22]
Epidemiology
Historically, erythema ab igne affects women more often than men and has been reported to be in a 10:1 distribution; however, this is likely older data representing older causes of EAI, such as coal fires and other household issues exposures that women may have had more exposure to traditionally. Newer data suggests that women are about twice as likely to have erythema ab igne, and it is more likely to appear on the anterior legs.[23]
Although it can appear at any age, a previous study noted that the average age was 28.6 +/- 10.4 years.[23] Most lesions are localized and related to heater exposure, stove exposure, laptop exposure, tandoor oven exposure, or hot water bag.[23] Notably, the age distribution may be indicative of etiology; for instance, use in older adults for chronic back or abdominal pain may indicate underlying systemic or internal issues, including malignancy.[16]
Pathophysiology
Erythema ab igne occurs from repeated exposure to direct heat or infrared radiation, usually developing over weeks to years at insufficient temperatures to cause significant thermal burns.[1] This chronic heat exposure is proposed to cause damage to superficial blood vessels, such as the venous plexus, that thus corresponds to a reticulated pattern on the skin related to thermoregulatory mechanisms in the integumentary blood vessels.[24]
The deposition of hemosiderin and melanin may be a reaction pattern from blood vessels, where some capillaries have shown endothelial cell changes.[25][26] Continued exposure may eventually lead to hyperkeratosis and hyperelastosis of the affected skin.[27][28]
Histopathology
Changes in the skin at the microscopic level typically occur from cumulative and prolonged exposure to infrared radiation. Initial changes may show epidermal atrophy, vasodilation, and deposition of hemosiderin/melanin in the dermal layer. The presence of melanin may be related to melanocyte activation. Additionally, there may be dermal capillaries with enlarged endothelial cells. Later changes may also show focal hyperkeratosis or dyskeratosis with squamous atypia, consistent with changes in actinic keratosis or other pre-malignant lesions.[1] Given this, biopsies are most useful for excluding more serious conditions such as Merkel and squamous cell carcinoma, which may present with similar skin findings or be masked by erythema ab igne.[28][29][30][16] Further, erythema ab igne may mimic or mask other skin cancers, such as basal cell carcinoma; it may even mask cutaneous metastases of internal malignancy, like colonic adenocarcinoma.[31][13][32]
History and Physical
Patients may seek medical care for this dermatosis, but it often occurs as an incidental finding on a physical exam. Patients are usually asymptomatic, but some may complain that the affected area burns, itches, or stings.[27][33] Patients typically present with a chronic history of using a heating source, such as a pad. This may be associated with pain in the area, such as in the abdomen, lower back, or joints.[34][20][18]
Historical findings should focus on contact with any heat source in the rash area. On physical exam, the skin initially presents as easily blanching macular erythema broadly in 1 area. This ultimately evolves into the classic reticulated (net-like) dusky hyperpigmentation that is non-blanching.[35][36][37] There may be associated epidermal atrophy on the reticulated hyperpigmentation and focal hyperkeratosis.[7][38]
Evaluation
Erythema ab igne is a clinical diagnosis that raises suspicion, given the relevant history and characteristic skin manifestations. Long-standing disease in the presence of ulcerations, hyperkeratosis, or bullae should prompt further evaluation by a dermatologist, as this finding can be associated with the malignant transformation of squamous cell carcinoma.[39][1][13][1] As patients often apply heat to areas of chronic pain, further history should also be obtained from the patient to investigate the cause of the patient's chronic pain, as they may need a further referral for this as well.[40][41]
In ambiguous cases, a biopsy should be considered, particularly as this may mimic or mask underlying skin cancer, such as basal cell carcinoma or squamous cell carcinoma; it may even mask cutaneous metastases of internal malignancy, like colonic adenocarcinoma.[31][13][32][31] Usually, other laboratory and imaging are unnecessary, except as they are related to the causes of chronic pain. For instance, evaluating the patient for pancreatitis or conducting imaging of the abdomen for abdominal EAI may be indicated to evaluate underlying pathology.[42][19]
Treatment / Management
The primary treatment of this disease entity is removing the offending heat source.[6] The resulting abnormal pigmentation of affected areas may resolve over months to years; however, permanent hyperpigmentation or scarring may persist. Treatments for hyperpigmentation, such as topical tretinoin or hydroquinone, can be useful in treating persistent hyperpigmentation.[43] Scars can be monitored or treated if they become hypertrophic or disfiguring.[44] (A1)
If epidermal atypia is suspected, regular skin examinations are recommended, particularly as EAI may be associated with squamous atypia and malignant transformation to squamous cell carcinoma.[1] Indeed, pathologic evidence shows that erythema ab igne shows histopathologic changes that align with those seen in pre-malignant states, like actinic keratosis.[13] Therefore, topical 5-fluorouracil has also been shown to treat epithelial atypia if present.[45](B3)
Differential Diagnosis
Erythema ab igne should be considered in the differential diagnosis of dyspigmented reticular dermatoses.[46] Other diagnoses for this pattern of rash include:
- Livedo reticularis
- Livedoid vasculitis
- Poikiloderma atrophicans vascular
- Cutaneous T-cell lymphoma
- Dermatomyositis
- Cutis marmorata telangiectatica congenita
- Genodermatoses
- Angiosarcoma[47]
- Vasculitis[48]
- Bullous disease[17]
A key feature that can distinguish erythema ab igne from other reticular rashes is its presentation in the setting of chronic heat exposure, as livedo reticularis and cutis marmorata are often present with exposure to cold and other rashes present without a history of heat exposure altogether.[28] Patients with pancreatitis may have livedo reticularis on the abdomen, chest, or thighs. This is believed to be because of trypsin-induced damage to the subcutaneous venous network. This is called Walzels sign.[49]
Prognosis
Erythema ab igne holds a favorable prognosis by removing the offending heat source, and repeated exposures are limited. If prolonged exposure continues, there is a risk of permanent dyschromia of the skin and the potential for transformation into pre-malignant or malignant skin lesions [50]. There are multiple case reports of either malignant transformation of erythema ab igne into squamous cell carcinoma as well as multiple case reports demonstrating the mimicking or masking of cutaneous malignancy by erythema ab igne; therefore, there remains some chance of malignant transformation that should be considered in areas affected.[31][13][32]
Complications
Complications are rare; however, malignant transformation to squamous cell carcinoma has been reported in the literature, with signs of hyperkeratosis or ulceration occurring as secondary, premalignant changes.[1]
Deterrence and Patient Education
Patient education on heat as a cause of this disease is essential for the treatment and to prevent a recurrence. Patients diagnosed with this disease due to occupational exposure need specific guidance on preventing exposure and optimizing outcomes. In patients with chronic pain, alternative therapies for pain relief should be advised to avoid repetitive exposures.
Enhancing Healthcare Team Outcomes
An interprofessional team approach to erythema ab igne that includes clinicians, specialists (particularly dermatologists), and nursing staff is recommended. Erythema ab igne is a preventable skin dermatosis, and patient education is critical in preventing disease progression. Most patients present to the primary care provider. Clinicians can counsel the patient on preventative measures and coordinate with pharmacy consult when medication is necessary. Accurate record-keeping by all interprofessional care team members ensures that everyone on the case has the same accurate patient data; this is another aspect of communication between team members. The interprofessional approach yields the best results with the fewest adverse events.
Heating pads and water bottles are commonly used to manage chronic pain and can potentially lead to the development of erythema ab igne. Clinicians should be aware of the presentation of erythema ab igne and other mimicking conditions such as livedo reticularis, cutis marmorata, and physical abuse. Providers should be aware of the risks for malignant transformation in areas of repeated heat exposure. Furthermore, a careful history should be obtained to rule out other systemic symptoms that could be indicative of other more serious pathologies causing the patient’s chronic pain. Long-standing erythema ab igne in the presence of other secondary changes such as ulceration or hyperkeratosis should prompt a dermatologist referral for biopsy and further management.
Media
(Click Image to Enlarge)
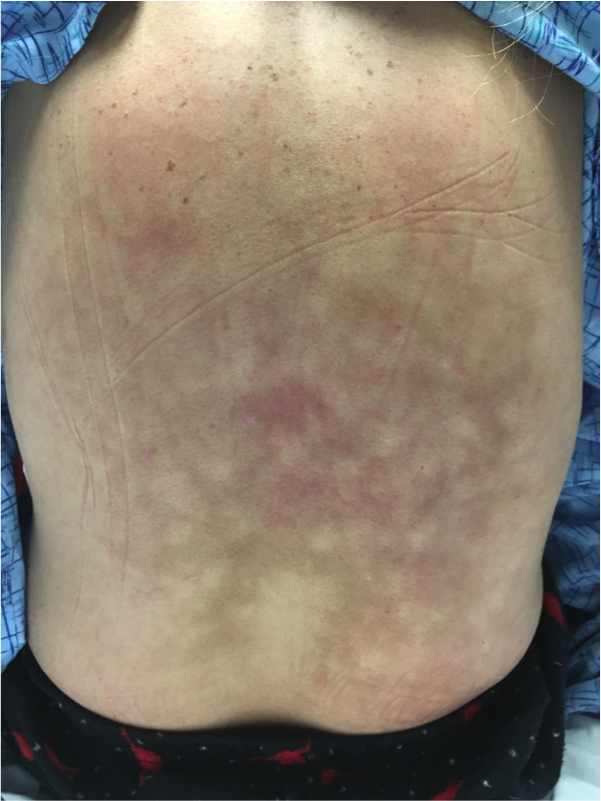
Erythema ab Igne, Back
Contributed by D Smith, DO; J McIntosh, DO; J Roach, DO; J Traylor, DO
References
Wipf AJ, Brown MR. Malignant transformation of erythema ab igne. JAAD case reports. 2022 Aug:26():85-87. doi: 10.1016/j.jdcr.2022.06.018. Epub 2022 Jul 5 [PubMed PMID: 35942353]
Level 3 (low-level) evidenceKhaitan BK, Ahuja R. Erythema Ab Igne. The New England journal of medicine. 2022 Oct 6:387(14):e33. doi: 10.1056/NEJMicm2203401. Epub [PubMed PMID: 36198181]
Moreau T, Benzaquen M, Gueissaz F. Erythema ab igne after using a virtual reality headset: a new phenomenon to know. Journal of the European Academy of Dermatology and Venereology : JEADV. 2022 Nov:36(11):e932-e933. doi: 10.1111/jdv.18371. Epub 2022 Jul 7 [PubMed PMID: 35753063]
Haleem Z,Philip J,Muhammad S, Erythema Ab Igne: A Rare Presentation of Toasted Skin Syndrome With the Use of a Space Heater. Cureus. 2021 Feb 17; [PubMed PMID: 33754117]
Duan GY, Stein SL. Erythema ab igne in pediatric patients remote schooling during the COVID-19 pandemic: A case series. Pediatric dermatology. 2021 Sep:38(5):1361-1362. doi: 10.1111/pde.14791. Epub 2021 Aug 31 [PubMed PMID: 34463374]
Level 2 (mid-level) evidenceForouzan P, Riahi RR, Cohen PR. Heater-Associated Erythema Ab Igne: Case Report and Review of Thermal-Related Skin Conditions. Cureus. 2020 May 11:12(5):e8057. doi: 10.7759/cureus.8057. Epub 2020 May 11 [PubMed PMID: 32537275]
Level 3 (low-level) evidenceWells A, Desai A, Rudnick EW, Motaparthi K. Erythema ab igne with features resembling keratosis lichenoides chronica. Journal of cutaneous pathology. 2021 Jan:48(1):151-153. doi: 10.1111/cup.13885. Epub 2020 Nov 5 [PubMed PMID: 32990396]
LeVault KM, Sapra A, Bhandari P, O'Malley M, Ranjit E. Erythema Ab Igne: A Mottled Rash on the Torso. Cureus. 2020 Jan 11:12(1):e6628. doi: 10.7759/cureus.6628. Epub 2020 Jan 11 [PubMed PMID: 32064204]
Mirgh SP, Shah VD, Sorabjee JS. Perils of Technology - Laptop Induced Erythema Ab Igne (Toasted Skin Syndrome) on Abdomen. Indian journal of occupational and environmental medicine. 2020 May-Aug:24(2):131-132. doi: 10.4103/ijoem.IJOEM_12_19. Epub 2020 Aug 19 [PubMed PMID: 33281387]
Sahu KK, Mishra A, Naraghi L. Erythema ab igne as a complication of cannabinoid hyperemesis syndrome. BMJ case reports. 2019 Jan 29:12(1):. doi: 10.1136/bcr-2018-227836. Epub 2019 Jan 29 [PubMed PMID: 30700469]
Level 3 (low-level) evidenceGoorland J, Edens MA, Baudoin TD. An Emergency Department Presentation of Erythema Ab Igne Caused by Repeated Heater Exposure. The Journal of the Louisiana State Medical Society : official organ of the Louisiana State Medical Society. 2016 Mar-Apr:168(2):33-4 [PubMed PMID: 27383852]
Yehudina Y, Trypilka S. A clinical case of laptop-generated Erythema ab igne. European journal of rheumatology. 2021 Apr:8(2):117-118. doi: 10.5152/eurjrheum.2020.20175. Epub [PubMed PMID: 33687829]
Level 3 (low-level) evidenceWilder EG, Frieder JH, Menter MA. Erythema Ab Igne and Malignant Transformation to Squamous Cell Carcinoma. Cutis. 2021 Jan:107(1):51-53. doi: 10.12788/cutis.0145. Epub [PubMed PMID: 33651859]
Riahi RR, Cohen PR. Laptop-induced erythema ab igne: Report and review of literature. Dermatology online journal. 2012 Jun 15:18(6):5 [PubMed PMID: 22747929]
Level 3 (low-level) evidenceDvoretzky I, Silverman NR. Reticular erythema of the lower back. Erythema ab igne. Archives of dermatology. 1991 Mar:127(3):405-6, 408-9 [PubMed PMID: 1998373]
Level 3 (low-level) evidenceSalgado F, Handler MZ, Schwartz RA. Erythema ab igne: new technology rebounding upon its users? International journal of dermatology. 2018 Apr:57(4):393-396. doi: 10.1111/ijd.13609. Epub 2017 Mar 30 [PubMed PMID: 28369761]
Redding KS, Watts AN, Lee J, Kennedy KR, Shimek CM, Skinner RB. Space heater-induced bullous erythema ab igne. Cutis. 2017 Aug:100(2):E9-E10 [PubMed PMID: 28961297]
Marie I. Erythema Ab Igne. Arthritis & rheumatology (Hoboken, N.J.). 2018 Nov:70(11):1896. doi: 10.1002/art.40561. Epub 2018 Sep 3 [PubMed PMID: 29781584]
Harsch IA. Abdominal erythema ab igne-An "old" finding revisited. Clinical case reports. 2020 Jul:8(7):1315-1316. doi: 10.1002/ccr3.2834. Epub 2020 Apr 16 [PubMed PMID: 32695386]
Samaan CB, Valentin MN, Jamison MO, Ellison K, Marathe KS, Norton SA, Kirkorian AY. Erythema ab igne in patients with sickle cell disease. Pediatric hematology and oncology. 2018 Apr:35(3):225-230. doi: 10.1080/08880018.2018.1516838. Epub 2018 Oct 25 [PubMed PMID: 30359159]
Gmuca S, Yu J, Weiss PF, Treat JR, Sherry DD. Erythema Ab Igne in an Adolescent With Chronic Pain: An Alarming Cutaneous Eruption From Heat Exposure. Pediatric emergency care. 2020 Apr:36(4):e236-e238. doi: 10.1097/PEC.0000000000001460. Epub [PubMed PMID: 29538269]
Ravindran R. Erythema ab igne in an individual with diabetes and gastroparesis. BMJ case reports. 2017 Oct 4:2017():. pii: bcr-2014-203856. doi: 10.1136/bcr-2014-203856. Epub 2017 Oct 4 [PubMed PMID: 28978571]
Level 3 (low-level) evidenceOzturk M, An I. Clinical features and etiology of patients with erythema ab igne: A retrospective multicenter study. Journal of cosmetic dermatology. 2020 Jul:19(7):1774-1779. doi: 10.1111/jocd.13210. Epub 2019 Nov 7 [PubMed PMID: 31696628]
Level 2 (mid-level) evidencePage EH, Shear NH. Temperature-dependent skin disorders. Journal of the American Academy of Dermatology. 1988 May:18(5 Pt 1):1003-19 [PubMed PMID: 3290279]
Level 3 (low-level) evidencePincelli T, Keeling J, Sokumbi O. Bullous Erythema ab Igne Unexpected Biopsy: Challenge. The American Journal of dermatopathology. 2022 Aug 1:44(8):e86-e87. doi: 10.1097/DAD.0000000000002243. Epub [PubMed PMID: 35830705]
Pincelli T, Keeling J, Sokumbi O. Bullous Erythema ab Igne Unexpected Biopsy: Answer. The American Journal of dermatopathology. 2022 Aug 1:44(8):615. doi: 10.1097/DAD.0000000000002242. Epub [PubMed PMID: 35830702]
Milchak M, Smucker J, Chung CG, Seiverling EV. Erythema Ab Igne due to Heating Pad Use: A Case Report and Review of Clinical Presentation, Prevention, and Complications. Case reports in medicine. 2016:2016():1862480. doi: 10.1155/2016/1862480. Epub 2016 Jan 3 [PubMed PMID: 26880929]
Level 3 (low-level) evidenceAria AB, Chen L, Silapunt S. Erythema Ab Igne from Heating Pad Use: A Report of Three Clinical Cases and a Differential Diagnosis. Cureus. 2018 May 16:10(5):e2635. doi: 10.7759/cureus.2635. Epub 2018 May 16 [PubMed PMID: 30034957]
Level 3 (low-level) evidenceJohnson WC, Butterworth T. Erythema ab Igne elastosis. Archives of dermatology. 1971 Aug:104(2):128-31 [PubMed PMID: 5093167]
Iacocca MV, Abernethy JL, Stefanato CM, Allan AE, Bhawan J. Mixed Merkel cell carcinoma and squamous cell carcinoma of the skin. Journal of the American Academy of Dermatology. 1998 Nov:39(5 Pt 2):882-7 [PubMed PMID: 9810922]
Level 3 (low-level) evidenceDaneshvar E, Seraji S, Kamyab-Hesari K, Ehsani AH, Hanifnia AR, Razavi Z. Basal cell carcinoma associated with erythema ab igne. Dermatology online journal. 2020 Apr 15:26(4):. pii: 13030/qt3kz985b4. Epub 2020 Apr 15 [PubMed PMID: 32621693]
Alhuzimi AM, Alfawzan AI, Alajlan A, Aljasser MI. Erythema ab igne masking cutaneous metastasis of colorectal adenocarcinoma. Dermatology reports. 2021 Mar 18:13(1):9079. doi: 10.4081/dr.2021.9079. Epub 2021 Mar 18 [PubMed PMID: 33824711]
Salvio AG, Nunes AJ, Angarita DP. Laptop computer induced erythema ab igne: a new presentation of an old disease. Anais brasileiros de dermatologia. 2016 Sep-Oct:91(5 suppl 1):79-80. doi: 10.1590/abd1806-4841.20165139. Epub [PubMed PMID: 28300902]
Stollery N. Photo quiz. Case 10. Erythema ab igne. The Practitioner. 2007 Dec:251(1701):34 [PubMed PMID: 18193513]
Level 3 (low-level) evidenceKokturk A, Kaya TI, Baz K, Yazici AC, Apa DD, Ikizoglu G. Bullous erythema ab igne. Dermatology online journal. 2003 Aug:9(3):18 [PubMed PMID: 12952765]
Level 3 (low-level) evidenceNield TR, Brunner NE, Zinn Z. Erythema Ab Igne in a 12-Year-Old Boy Diagnosed via Telemedicine. Cureus. 2020 Nov 19:12(11):e11577. doi: 10.7759/cureus.11577. Epub 2020 Nov 19 [PubMed PMID: 33364102]
Bourseau S, Bastens B, Leclercq P. Umbilical spider's web. Acta gastro-enterologica Belgica. 2022 Jul-Sep:85(3):542. doi: 10.51821/85.3.10418. Epub [PubMed PMID: 36198302]
Prohic A, Poparic S, Cemerlic A, Kapetanovic A. Erythema Ab Igne with Histological Features of Keratosis Lichenoides Chronica. Case reports in dermatology. 2021 Jan-Apr:13(1):184-189. doi: 10.1159/000515259. Epub 2021 Mar 29 [PubMed PMID: 34703425]
Level 3 (low-level) evidenceSigmon JR, Cantrell J, Teague D, Sangueza O, Sheehan DJ. Poorly differentiated carcinoma arising in the setting of erythema ab igne. The American Journal of dermatopathology. 2013 Aug:35(6):676-8. doi: 10.1097/DAD.0b013e3182871648. Epub [PubMed PMID: 23872874]
Level 3 (low-level) evidenceJones CS, Tyring SK, Lee PC, Fine JD. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Archives of dermatology. 1988 Jan:124(1):110-3 [PubMed PMID: 3337533]
Level 3 (low-level) evidenceBunick CG, King BA, Ibrahim O. When erythema ab igne warrants an evaluation for internal malignancy. International journal of dermatology. 2014 Jul:53(7):e353-5. doi: 10.1111/ijd.12329. Epub 2014 Mar 6 [PubMed PMID: 24601874]
Level 3 (low-level) evidenceParker R, Gordon FH. A different cause of erythema ab igne in chronic pancreatitis. Pancreatology : official journal of the International Association of Pancreatology (IAP) ... [et al.]. 2008:8(4-5):532. doi: 10.1159/000152002. Epub 2008 Sep 3 [PubMed PMID: 18765958]
Level 3 (low-level) evidencePennitz A, Kinberger M, Avila Valle G, Passeron T, Nast A, Werner RN. Self-applied topical interventions for melasma: a systematic review and meta-analysis of data from randomized, investigator-blinded clinical trials. The British journal of dermatology. 2022 Sep:187(3):309-317. doi: 10.1111/bjd.21244. Epub 2022 May 18 [PubMed PMID: 35290681]
Level 1 (high-level) evidenceChua S, Chen Q, Lee HY. Erythema ab igne and dermal scarring caused by cupping and moxibustion treatment. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2015 Apr:13(4):337-8. doi: 10.1111/ddg.12581. Epub [PubMed PMID: 25819248]
Sahl WJ Jr, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. Journal of the American Academy of Dermatology. 1992 Jul:27(1):109-10 [PubMed PMID: 1619057]
Level 3 (low-level) evidenceKozera EK, Sebaratnam DF. Erythema ab igne. The Medical journal of Australia. 2021 Nov 1:215(9):405. doi: 10.5694/mja2.51292. Epub 2021 Oct 1 [PubMed PMID: 34599511]
Johnson NM, Shvygina A, Luyimbazi DT, Grider DJ. Rare mimic of angiosarcoma: Erythema ab igne with reactive angiomatosis. Journal of cutaneous pathology. 2021 Oct:48(10):1298-1302. doi: 10.1111/cup.14072. Epub 2021 Jun 24 [PubMed PMID: 34086363]
Çakan M, Demirsoy EO. Vasculitic Rash or Something Simpler: Erythema Ab Igne. Journal of clinical rheumatology : practical reports on rheumatic & musculoskeletal diseases. 2021 Aug 1:27(5):e193. doi: 10.1097/RHU.0000000000001362. Epub [PubMed PMID: 32149928]
Lankisch PG, Weber-Dany B, Maisonneuve P, Lowenfels AB. Skin signs in acute pancreatitis: frequency and implications for prognosis. Journal of internal medicine. 2009 Feb:265(2):299-301. doi: 10.1111/j.1365-2796.2008.02004.x. Epub [PubMed PMID: 19192040]
Level 3 (low-level) evidenceTan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2000 Jan 11:162(1):77-8 [PubMed PMID: 11216204]
Level 3 (low-level) evidence