 Anatomy, Head and Neck, Trachea Epiglottic Vallecula
Anatomy, Head and Neck, Trachea Epiglottic Vallecula
Introduction
Vallecula is a term that means depression in something. The epiglottic vallecula consists of a small mucosa-lined depression (vallecula) located at the base of the tongue just between the folds of the throat on either side of the median glossoepiglottic fold. It is usually not seen by the naked eye as it is far back and deep at the root of the tongue. The function of the “depression” is to serve as a trap for saliva and occasionally food. Trapping the saliva in the vallecula prevents the swallowing reflex. At night, when a person is asleep, the vallecula traps the saliva so that the swallowing reflex is not constantly triggered.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Anatomically, the vallecula is situated between the pharynx and larynx and thus helps demark the transition from these to regions. The median glossoepiglottic fold is the separation between the epiglottis and the base of the tongue and gives rise to the two valleculae. Together the valleculae and the pyriform recesses are named the pharyngeal recesses. The anatomic location of the vallecula makes it ideally situated to collect saliva and prevent the swallowing reflex while a person is supine during sleep.[2]
Embryology
The vallecula is an infolding of mucosa to form a pouch. The mucosa is often lined by epithelium, which is the case with the vallecula as well. The vallecula, as well as the rest of the pharynx and larynx, are derived from ectoderm embryologically. The vallecula derives from the third branchial arch along with other structures including the stylopharyngeus, the body of the hyoid bone, and the glossopharyngeal nerve.[3]
Blood Supply and Lymphatics
The facial and lingual arteries are branches of the external carotid artery which run close to the vallecula. The lingual artery runs parallel to the fibers of the geniohyoid and is at the level of the hyoid bone.[4]
Venous drainage of the area follows a similar pattern. The lingual vein and the pharyngeal venous plexus drain to the internal jugular vein.[5]
Lymphatic drainage in the area of the vallecula includes both tonsils and lymph nodes. The palatine tonsil and the lingual tonsils are within a few centimeters of the vallecula. There is also an extensive amount of lymphatic tissue called the lateral bands of the pharynx in this region. Combined, these tonsils and the lateral bands make up Waldeyer's ring, or nasal-associated lymphoid tissue (NALT). The deep cervical lymph nodes are the primary drainage of the vallecular region. These lymph nodes drain to the jugulofacial venous junction, which continues to drain inferiorly to the jugulo-subclavian venous junction bilaterally.[6]
Nerves
The vallecula is a highly innervated region as evidenced by physiological responses such as increases in heart rate and blood pressure with direct laryngoscopy during endotracheal intubation and other procedures like bronchoscopy and upper GI endoscopy. The vallecula receives nerve supply from the ninth cranial nerve (CN IX) or glossopharyngeal nerve.[7] The Vagus nerve (CN X) innervates other portions of the larynx.
Muscles
The vallecula is not a muscular structure but is adjacent to several muscles of the oropharynx as well as the larynx. The vallecula is located just superior to the level of the hyoid bone, and this landmark makes approximating the level of the vallecula easier. The muscles of the tongue including geniohyoid and genioglossus are superior to the vallecula, and the stylopharyngeus is just lateral to the vallecula running vertically.[8]
The pharynx at the level of the vallecula is surrounded by the middle pharyngeal constrictor posteriorly and the hyoglossus laterally.[9]
Physiologic Variants
While there is potential for physiological variants of the vallecula, there is little documentation of such findings; this might be because any variants or malformations in this region are potentially incompatible with life. Malformations of the third branchial arch are exceedingly rare, and branchial arch malformations most commonly occur in arch two and commonly manifest as fistulas or cysts.[10]
While variants of the epiglottic vallecula are uncommon, variations in the location of blood supply and nerves are rather common in the human body.[5]
Surgical Considerations
The mucosa lining the vallecula has the potential to develop a squamous carcinoma, although rarely. While also concerning for metastasis, these tumors are especially concerning due to their potential to obstruct the airway. These tumors can present a difficult challenge for both the airway team and the otolaryngologist who must resect the tumor.[11]
Vallecular cysts are also potential manifestations in this region. The incidence of these cysts is unknown due to the rare nature of this pathology. These are most common in pediatric patients, although they can potentially occur in adulthood. These cysts are most commonly present in infants and they affect both genders equally. They can arise after obstruction of the mucosal ducts.[12] There are also potential origins for these cysts from malformations of the third branchial arch, or a thyroglossal duct cyst. Thyroglossal duct cysts develop from a remnant of the thyroid gland that failed to obliterate during migration of the thyroid away from the base of the tongue.[13]
Infants classically will present with difficulty with feeding, failure to thrive, and potentially respiratory distress. For adults with this condition, difficulty swallowing is the most common presenting complaint. As the cyst or tumor enlarges shortness of breath on exertion can be the primary presenting complaint. Diagnosis of these cysts often includes nasopharyngeal laryngoscopy or bronchoscopy. Treatment requires excision of these cysts is necessary as these cysts will often recur if only drained. Treatment may include marsupialization, excision with a carbon dioxide laser, or coblation. Marsupialization is a procedure where the cyst is opened, and a permanent pouch is formed to allow continuous drainage of the cyst.[14]
Clinical Significance
Knowledge of the location of the vallecula is crucial for anesthesiologists and all healthcare workers who perform intubation. The vallecula serves as an important anatomical landmark during oral intubation of the trachea. For direct laryngoscopy, an anesthesiology provider may use different blade options.[15] One difference in these devices is that the Macintosh blade is placed in the vallecula, while the Miller blade is placed over the superior tip of the epiglottis. The end goal with either tool is to depress enhance the view of the vocal cords by drawing the epiglottis anterior and opening the larynx. Neither laryngoscopy blade is superior and choosing the right one for a specific patient is up to the provider's discretion. Miller blade is longer and can be used if the patients neck is longer, has floppy epiglottis, and has anterior airway. If proper visualization of the vallecula with a blade is not achieved during intubation, the risk of failed intubation attempt is very high, hypoxia and hypercarbia can lead to potential cardiac arrest. One should be trained to intubate using newer techniques like using glidescope in which the larynx is directly visible on a screen, and the endotracheal tube can be passed through the vocal cords easily. While using Macintosh and Miller blades, one has to pull the base of the tongue forward to lift the epiglottis forward to visualize the vocal cords, and this technique can be operator-dependent. But while using glideslope, the person performing intubation does not have to lift the base of the tongue as much.[16]
Media
(Click Image to Enlarge)
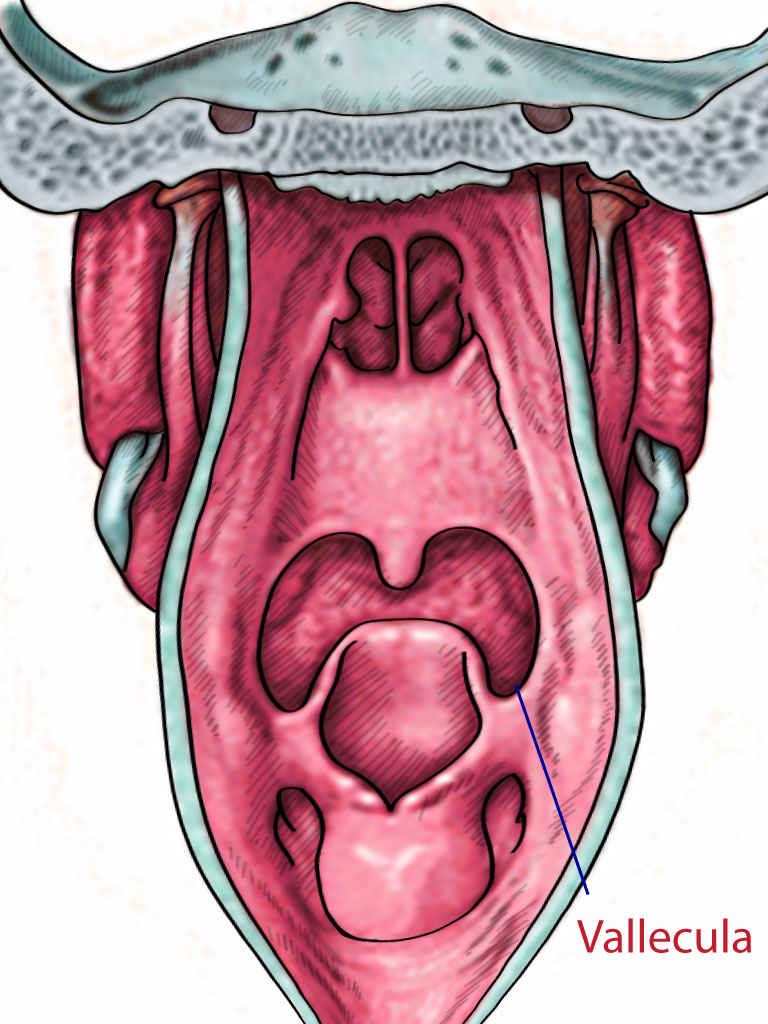
Vallecula
Contributed by T Silappathikaram
References
Kitagawa J, Nakagawa K, Hasegawa M, Iwakami T, Shingai T, Yamada Y, Iwata K. Facilitation of reflex swallowing from the pharynx and larynx. Journal of oral science. 2009 Jun:51(2):167-71 [PubMed PMID: 19550082]
Level 3 (low-level) evidenceThexton AJ. Mastication and swallowing: an overview. British dental journal. 1992 Oct 10:173(6):197-206 [PubMed PMID: 1389633]
Level 3 (low-level) evidenceSakamoto Y. Classification of pharyngeal muscles based on innervations from glossopharyngeal and vagus nerves in human. Surgical and radiologic anatomy : SRA. 2009 Dec:31(10):755-61. doi: 10.1007/s00276-009-0516-9. Epub 2009 May 29 [PubMed PMID: 19479181]
Seki S, Sumida K, Yamashita K, Baba O, Kitamura S. Gross anatomical classification of the courses of the human lingual artery. Surgical and radiologic anatomy : SRA. 2017 Feb:39(2):195-203. doi: 10.1007/s00276-016-1696-8. Epub 2016 May 17 [PubMed PMID: 27189234]
Wang C, Kundaria S, Fernandez-Miranda J, Duvvuri U. A description of arterial variants in the transoral approach to the parapharyngeal space. Clinical anatomy (New York, N.Y.). 2014 Oct:27(7):1016-22. doi: 10.1002/ca.22273. Epub 2014 Feb 7 [PubMed PMID: 24510490]
Hellings P, Jorissen M, Ceuppens JL. The Waldeyer's ring. Acta oto-rhino-laryngologica Belgica. 2000:54(3):237-41 [PubMed PMID: 11082757]
Sakamoto Y. Morphological Features of the Glossopharyngeal Nerve in the Peripharyngeal Space, the Oropharynx, and the Tongue. Anatomical record (Hoboken, N.J. : 2007). 2019 Apr:302(4):630-638. doi: 10.1002/ar.23924. Epub 2018 Nov 1 [PubMed PMID: 30383337]
Gervasio A, D'Orta G, Mujahed I, Biasio A. Sonographic anatomy of the neck: The suprahyoid region. Journal of ultrasound. 2011 Sep:14(3):130-5. doi: 10.1016/j.jus.2011.06.001. Epub 2011 Jun 29 [PubMed PMID: 23396801]
Choi DY, Bae JH, Youn KH, Kim HJ, Hu KS. Anatomical considerations of the longitudinal pharyngeal muscles in relation to their function on the internal surface of pharynx. Dysphagia. 2014 Dec:29(6):722-30. doi: 10.1007/s00455-014-9568-z. Epub 2014 Aug 21 [PubMed PMID: 25142243]
Patoulias I, Rachmani E, Farmakis K, Rafailidis V, Kalogirou M, Patoulias D. A Bilateral, Non-syndromic, Type III Second Branchial Arch Sinus in a Neonate: a Case Report. Acta medica (Hradec Kralove). 2018:61(1):33-36. doi: 10.14712/18059694.2018.21. Epub [PubMed PMID: 30012248]
Level 3 (low-level) evidenceLaccourreye L, Garcia D, Ménard M, Brasnu D, Laccourreye O, Holsinger FC. Horizontal supraglottic partial laryngectomy for selected squamous carcinoma of the vallecula. Head & neck. 2008 Jun:30(6):756-64. doi: 10.1002/hed.20780. Epub [PubMed PMID: 18286490]
Level 2 (mid-level) evidenceLee DH, Yoon TM, Lee JK, Lim SC. Clinical characteristics and surgical treatment outcomes of vallecular cysts in adults. Acta oto-laryngologica. 2015:135(11):1185-8. doi: 10.3109/00016489.2015.1062549. Epub 2015 Jul 3 [PubMed PMID: 26139619]
Zamfir-Chiru-Anton A, Gheorghe DC. Vallecular cysts in clinical practice: report of two cases. Journal of medicine and life. 2016 Jul-Sep:9(3):288-290 [PubMed PMID: 27974936]
Level 3 (low-level) evidenceZalvan CH, Reilly E. Symptomatic vallecular cysts: diagnosis and management with the KTP laser. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2016 Aug:273(8):2111-6. doi: 10.1007/s00405-016-4026-1. Epub 2016 Apr 7 [PubMed PMID: 27056198]
Nishikawa K, Yamada K, Sakamoto A. A new curved laryngoscope blade for routine and difficult tracheal intubation. Anesthesia and analgesia. 2008 Oct:107(4):1248-52. doi: 10.1213/ane.0b013e318185cecb. Epub [PubMed PMID: 18806035]
Seto A, Takenaka I, Aoyama K, Iwagaki T, Ishimura H, Takenaka Y, Kadoya T. [Efficacy of bougie in difficult intubation with the Airway Scope caused by inability to lift the epiglottis directly]. Masui. The Japanese journal of anesthesiology. 2010 Apr:59(4):525-30 [PubMed PMID: 20420153]
Level 1 (high-level) evidence