Introduction
Entamoeba coli is one of many non-pathogenic protozoa found in humans.[1] It is transmitted through fecal-oral contact, and the mature cyst can be found in contaminated water.[2] Typically, these protozoa inhabit the large intestinal tract and can be identified in diagnostic stool specimens.[3] It is essential to differentiate Entamoeba coli, a nonpathogenic protozoan, from those that cause significant disease. The complete name of the protozoan is usually used to avoid confusion with the bacterium Escherichia coli.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Entamoeba coli is transmitted through fecal-oral contact.[4] Typically, mature cysts are ingested from contaminated water and food sources.[5]
Epidemiology
Entamoeba coli is global in its distribution, with the highest prevalence in regions with inadequate sanitation, typically in rural areas.[5] Older studies from the United States reported a prevalence of 4.2% among all stool samples sent to diagnostic laboratories in 1987.[6][7]
Intestinal parasitic diseases are common in developing countries. In a hospitalized population in Iran, random stool samples showed a prevalence of Entamoeba coli infection in 4.6%.[8] A random non-hospitalized rural community in Iran showed a 2.9% prevalence.[9] In a secluded population in Iran, it is 6.8%.[10] However, other areas have reported a prevalence of 11.4%.[11] Turkey reported a prevalence of 11.5%.[12] Rural areas of India had reported a prevalence of 21.8%.[13] In a hospitalized population in Sudan, the prevalence was 7%.[14]
In a study of 193 children in Malawi, East Africa, Entamoeba coli was found in approximately 10.4% of the sample.[5] In a random school population in Sudan, the prevalence was 7.5%.[15] In some rural school communities in Colombia, the prevalence can be as high as 25.7% to 35%.[16][17] Rural areas in Yucatan, Mexico, had a school children prevalence of 26.5%.[18] Rural communities in Ecuador had a prevalence in schoolchildren of 34.0%.[19] Even in developed countries, the prevalence can be high. In Swiss children, a prevalence of 8% has been reported.[20]
Fresh vegetables can carry parasites and infect a person when consumed unwashed or washed with contaminated water. A study in Tunisia showed that fresh vegetable samples contain helminth eggs and protozoan cysts eggs in 12.5% of the cases; Entamoeba coli was found in 1.6%.[21] In another study in the United Arab Emirates, helminths eggs and protozoa cysts were detected in 15.1% of the samples; Entamoeba coli composed 18.2% of that percentage.[22] This fact demonstrates that safe handling of raw vegetables should be maintained and is recommended.
Pathophysiology
Entamoeba coli, similar to other Entamoeba specifies, has three distinct morphological forms: trophozoite, pre-cystic stage, and cystic stage.[2] The trophozoite form, which measures 20 to 25 μm, is minimally mobile.[23] The core of the trophozoite is slightly oval in shape with a nucleus surrounded by a thick membrane. Within this membrane, chromatin granules surround the large, eccentric, and irregular karyosome. The cytoplasm contains large vacuoles and is typically granular with easily distinguishable ectoplasm and endoplasm. The amoeba produces short, blunt pseudopods, which are projections from the granular cytoplasm, allowing limited mobility. When they surround bacteria and food particles, these pseudopods ingest them and form phagosomes through phagocytosis. In this stage, red blood cells and other bacteria and parasites can be found in the amoeba. Ingestion of red blood cells by Entamoeba coli is rare but may be seen.[24] Entamoeba coli can swallow other organisms, such as Giardia lamblia, which may compete for its food source.[23][25] There have been cases of hyperparasitization with spores of the Sphaerita species fungus.[26] Sphaerita species appear as tightly packed clusters within the cytoplasm, measuring approximately 0.5 to 1.0 μm producing degenerative changes in the host's protoplasm, especially in the nucleus.
The pre-cyst form begins when the trophozoite starts to slightly change its shape, becoming more spherical and containing two nuclei. The cyst is typically 10 to 35 μm in diameter and is a colorless spherical shape.[23] Their cytoplasm is still granular, but the vacuoles are absent. In the binucleate state, the glycogen vacuole is formed. The most distinguishing feature of the Entamoeba coli is the eight-core nuclei, which develops as the cyst begins to mature. In the octonucleate cystic form, the glycogen vacuole is reabsorbed. Occasionally, the nuclei may replicate until it has 16 nuclei in total. The mature cyst is rich in glycogen with a refractile wall.[27]
Colonization of the host first begins with the ingestion of mature cysts through contaminated food and water sources, typically via fecal-oral contamination. The cyst is hard due to its strong cell wall and can survive up to weeks in an external environment, and this quality allows it to survive the stomach's acidic environment. Cysts release trophozoites in the small intestine forming daughter trophozoites that are minimally motile and migrate to the colon. Entamoeba species, like most of the protozoans, reproduce by binary fission to form two daughter cells. Trophozoites in the colon multiply by undergoing binary fission and slowly reduce in size to first transform into the pre-cyst phase and then to the cyst phase. These cysts undergo mitosis until it becomes octonucleated or occasionally developing 16 nuclei. Host feces release mature octonucleate cysts of Entamoeba coli. Trophozoites found in the stool outside the body are rapidly destroyed, and if ingested, would not survive exposure to the gastric environment.
History and Physical
Most patients with Entamoeba coli infestation remain asymptomatic, and often, the protozoan is discovered incidentally.[27] It is important in those patients with diarrhea symptoms to obtain a thorough history and physical exam. Patients may rarely show gastrointestinal symptoms such as loose stools, colicky abdominal pain, and flatulence.[28] Some patients can complain of gastritis, indigestion, dyspepsia, or hyperacidity if the amoeba is in large amounts in the gastrointestinal tract. Stools are usually non-bloody and without mucus. Symptoms may persist for a long time; however, they are generalized and nonspecific for Entamoeba coli.
Evaluation
Ova and parasite testing can be performed to help distinguish between different amoebae species. Testing via microscopy will show the presence of protozoa; however, it is essential to differentiate between Entamoeba coli and the pathogenic amoeba, Entamoeba histolytica.[23] Stool examination via ova and parasite testing is the most common form of analysis and evaluation.[4][23] Stool examination with ova and parasite testing typically requires three stool specimens for best sensitivity and specificity.[2] Wet smears may result in difficulty in observing the Entamoeba coli cyst due to the refractile wall.[27]
On initial microscopy, the cyst of Entamoeba coli typically has eight nuclei, while Entamoeba histolytica typically has four. The peripheral chromatin is coarse and irregularly clumped for Entamoeba coli and fine, evenly distributed for Entamoeba histolytica. The karyosome of Entamoeba coli is irregular, large, and eccentric, with Entamoeba histolytica having a small, round, and centrally located karyosome.
More advanced tests are available, usually to differentiate between pathogenic and nonpathogenic Entamoeba species. These advanced tests include isoenzyme analysis, antibody detection test, antigen detection test, immunochromatographic assays, and electron microscopy.[23] DNA based methods tests include polymerase chain reaction, microarray, and reverse line hybridization assay; however, they are not always available.[29] Reverse line hybridization assay is the fastest and most specific method of DNA analysis.[29] The test allows for the determination of multiple strains of protozoa and showed intraspecific variation in Entamoeba coli.
Treatment / Management
Treatment is not indicated for Entamoeba coli infection.[27] Supportive care should be provided for patients, and proper hygiene should be maintained. An alternate source should be sought for patients with symptoms.
If the patient is symptomatic and no other organism or causes are found, treatment may be indicated. For those with persistent symptoms and no other infection source, treatment can be initiated. In one study, patients with gastrointestinal symptoms for many years with no other diagnosis were found to consistently had Entamoeba coli in the stool and were treated with diloxanide furoate 500 milligrams three times daily for ten days.[28] After treatment, symptoms were resolved, and the stool was tested again with no signs of Entamoeba coli infection. Metronidazole 400 mg orally three times a day is also effective. Patients typically stop developing symptoms within five days.(B3)
Differential Diagnosis
Patients with only Entamoeba coli in stool are typically asymptomatic.[27] Differential diagnosis of diarrheal disease is vast but can include:
- Bacterial pathogens: Escherichia coli, Shigella, Salmonella, Campylobacter, and Clostridium difficile
- Inflammatory bowel disease
- Ischemic bowel disease
The differential diagnosis for cyst or protozoa in the stool can include:[2][23]
- Entamoeba histolytica
- Chilomastix mesnili
- Endolimax nana
- Entamoeba dispar
- Entamoeba hartmanni
- Entamoeba polecki
- Iodamoeba buetschlii
Prognosis
The prognosis of patients with Entamoeba coli is excellent, as most patients are asymptomatic.[27]
Complications
Complications from Entamoeba coli infection are limited as patients are usually asymptomatic.[27] There are no long-term complications documented. The presence of nonpathogenic protozoa suggests contaminated food or water sources or poor fecal-oral hygiene.[2][23]
Consultations
The following consultations are required:
- Internal medicine
- Epidemiology
- Microbiology laboratory
- Pharmacy
- Social worker
Deterrence and Patient Education
If Entamoeba coli are found in stool samples, it may persist for days to years. Treatment is typically not needed. Patients can reduce the chances of getting parasitic infections such as Entamoeba coli by maintaining proper hand hygiene and avoiding contaminated food and water. Entamoeba coli is found globally and more prevalent in areas with poor sanitation.[4][5] Hygiene promotion lowers the risk of reinfection more than medication treatment alone.[30]
When traveling to areas with a high prevalence of low sanitation:
- Avoid drinking tap or well water. Avoid ice cubes, which are commonly made from tap water.
- Avoid eating raw fruits and vegetables that are cleaned with tap or well water.
- Avoid street vendors.
- Drink bottled beverages and use bottled water to brush your teeth.
- Wash hands with soap and water frequently, particularly after touching animals, before eating, and after using the restroom.
- Boil water before drinking.
- Use gloves if you need to touch feces.
Pearls and Other Issues
- Entamoeba coli is one of many non-pathogenic protozoa found in humans.
- It is transmitted through fecal-oral contact.
- Typically, mature cysts are ingested from contaminated water and food sources.
- The highest prevalence occurs in areas with inadequate sanitation, typically in rural areas.
- Entamoeba coli has three distinct morphological forms: trophozoite, pre-cystic stage, and cystic stage.
- The most distinguishing feature is the eight-core nuclei, which develops as the cyst begins to mature.
- The cyst is hard due to its strong cell wall and can survive up to weeks in an external environment.
- Trophozoites found in the stool outside the body are rapidly destroyed, and if ingested, would not survive the gastric environment.
- Most patients with Entamoeba coli infestation remain asymptomatic, and often protozoan is discovered incidentally.
- Patients may rarely show gastrointestinal symptoms such as loose stools, colicky abdominal pain, and flatulence.
- Ova and parasite testing can be completed to help distinguish between different amoebae species.
- It is essential to distinguish between Entamoeba coli and the pathogenic amoeba, Entamoeba histolytica.
- Stool samples should be taken at different times to ensure adequate specimens for testing.
- Reverse line hybridization assay is the fastest and most specific method of DNA analysis.
- Treatment is not indicated for Entamoeba coli infection.
- If the patient is symptomatic and no other organism or causes are found, treatment may be indicated.
- Patients can reduce the chances of getting parasitic infections such as Entamoeba coli by maintaining proper hand hygiene.
Enhancing Healthcare Team Outcomes
Entamoeba coli is a common protozoan found in stool worldwide. It is essential to identify and differentiate this non-pathologic protozoan from those causing significant disease. Infection with Entamoeba coli is a sign of fecal-oral contamination. Prevention through proper hand hygiene and avoidance of contaminated food and water. Patient education through multiple medical professionals, such as nursing staff, pharmacists, and physicians, is essential so patients can reduce infection chances. Patients should be advised to see physicians for further workup if gastrointestinal symptoms develop.
Media
(Click Image to Enlarge)
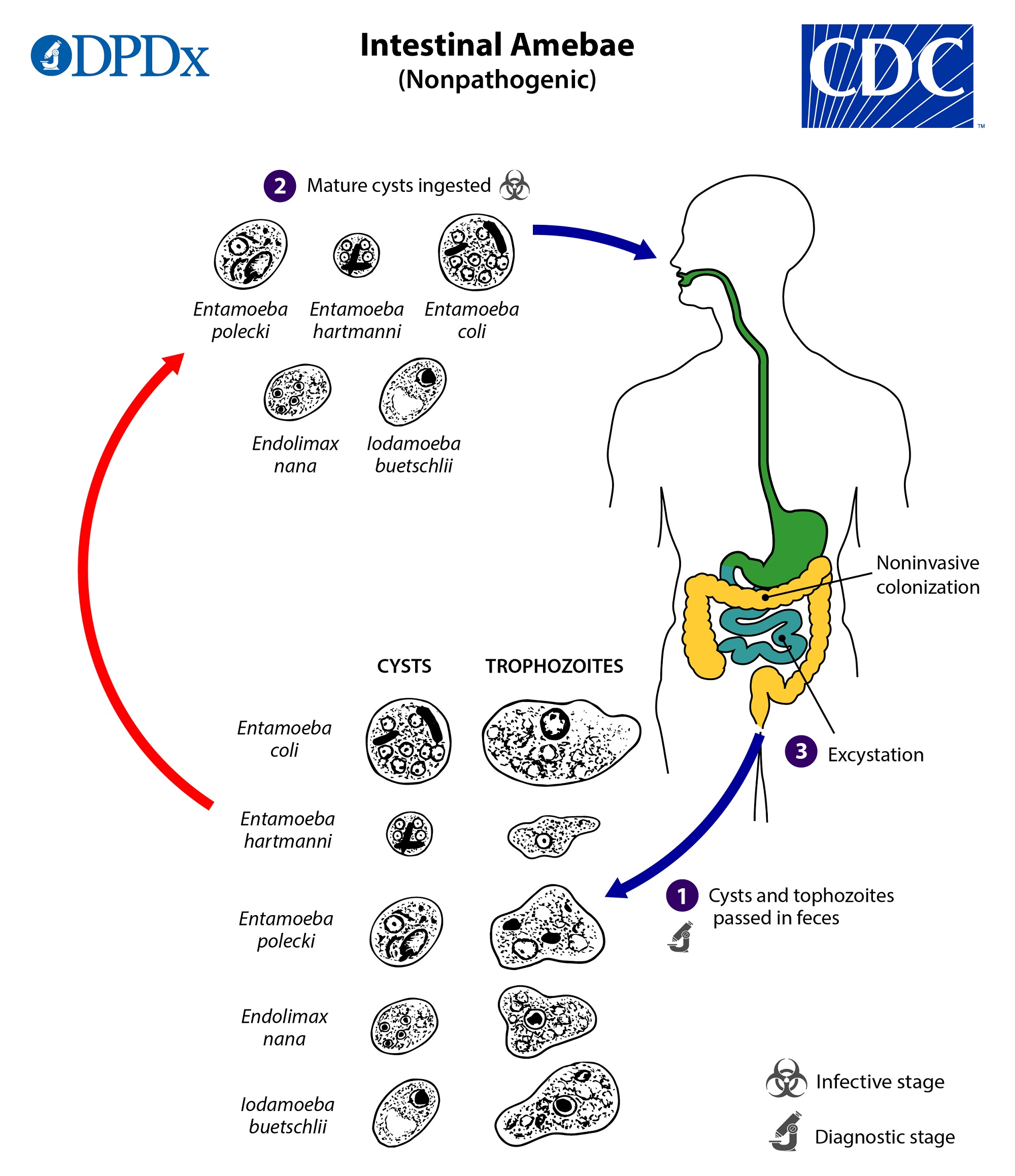
Life Cycle of Nonpathogenic Intestinal Amebae. Life cycle of nonpathogenic intestinal amebaeinclude several Entamoeba species (Entamoeba coli, Entamoeba hartmanni, and Entamoeba polecki), Endolimax nana, and Iodamoeba buetschlii (=I. bütschlii).
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
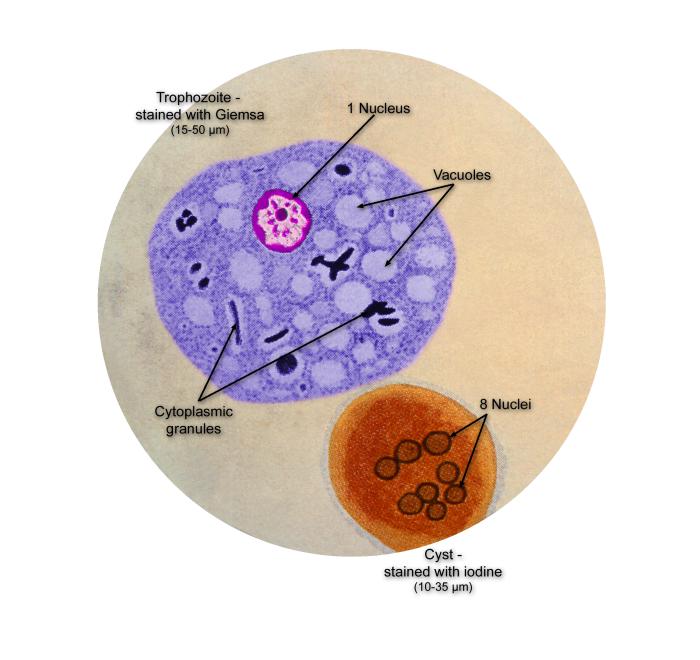
Life Cycle of the Parasite Entamoeba coli. This illustration of a composite photomicrograph reveals the ultrastructural details seen in two stages of the life cycle of the parasite, Entamoeba coli, including its cystic stage in the lower right, which was stained with iodine, and its Giemsa-stained, vegetative, trophozoite stage at center left.
Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
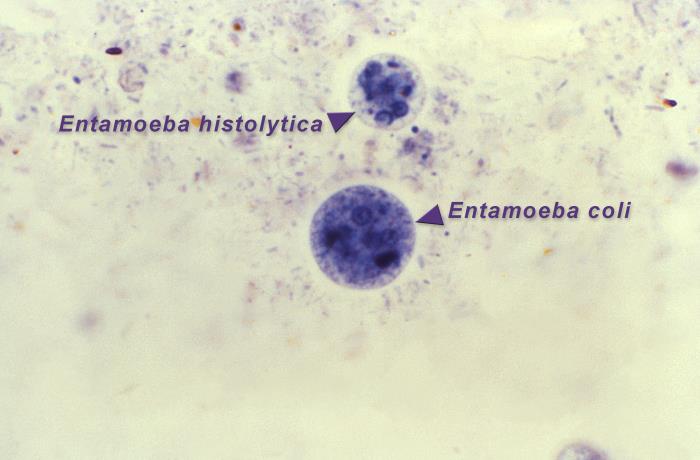
Amoebic Organisms in the Cystic Stages of Development. This photomicrograph of an iron hematoxylin-stained specimen revealed the presence of two amoebic organisms in the cystic stages of their development. In this focal plane, the smaller Entamoeba histolytica cyst (top), contained four nuclei, and two bluntly tipped chromatoid bodies, while six nuclei could be detected in the larger Entamoeba coli cyst (bottom), which also contained two chromatoid bodies.
Contributed by M Melvin, MD; via Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
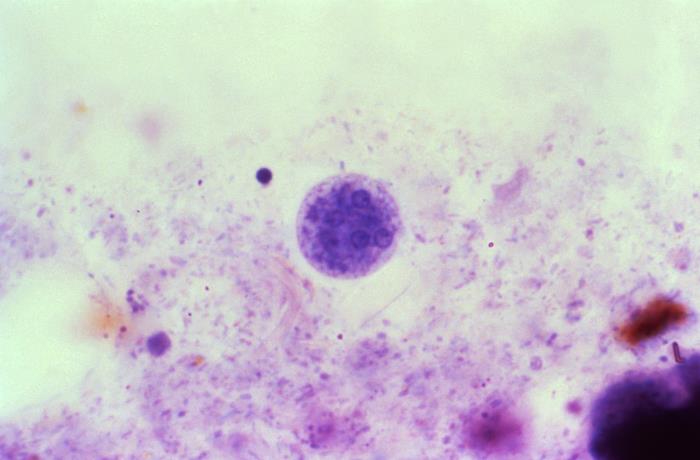
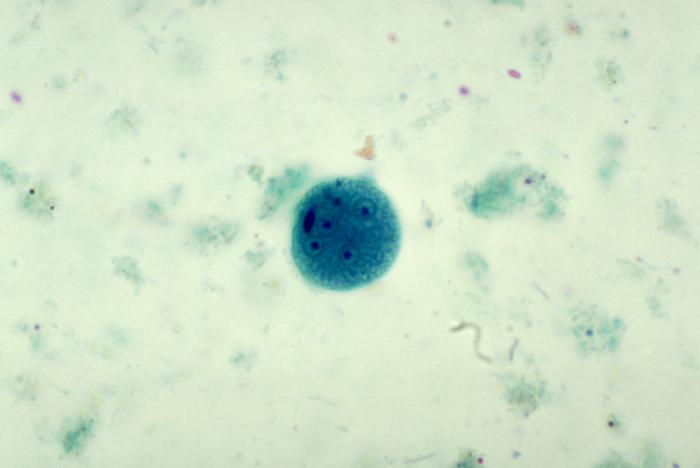
Mature Entamoeba coli Cyst. This photomicrograph of an iron-hematoxylin-stained specimen revealed the presence of a mature Entamoeba coli cyst, which contained five visible nuclei, each with its eccentrically located karyosome and peripherally located chromatin.
Contributed by M Melvin, MD; via Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
(Click Image to Enlarge)
Mature Entamoeba coli Cyst. This trichrome-stained photomicrograph depicts a mature Entamoeba coli cyst containing five clearly visible nuclei and what may have been a sixth nucleus, which was outside the focal plane and, therefore, out of focus. The cyst also contained a visible chromatoid body.
Contributed by M Melvin, MD; via Public Health Image Library, Public Domain, Centers for Disease Control and Prevention
References
Feng M, Pandey K, Yanagi T, Wang T, Putaporntip C, Jongwutiwes S, Cheng X, Sherchand JB, Pandey BD, Tachibana H. Prevalence and genotypic diversity of Entamoeba species in inhabitants in Kathmandu, Nepal. Parasitology research. 2018 Aug:117(8):2467-2472. doi: 10.1007/s00436-018-5935-2. Epub 2018 May 28 [PubMed PMID: 29808233]
Tanyuksel M, Petri WA Jr. Laboratory diagnosis of amebiasis. Clinical microbiology reviews. 2003 Oct:16(4):713-29 [PubMed PMID: 14557296]
Level 3 (low-level) evidencePinilla AE, López MC, Viasus DF. [History of the Entamoeba histolytica protozoan]. Revista medica de Chile. 2008 Jan:136(1):118-24 [PubMed PMID: 18483662]
Level 3 (low-level) evidencePritt BS,Clark CG, Amebiasis. Mayo Clinic proceedings. 2008 Oct; [PubMed PMID: 18828976]
Level 3 (low-level) evidenceJones TPW, Hart JD, Kalua K, Bailey RL. A prevalence survey of enteral parasites in preschool children in the Mangochi District of Malawi. BMC infectious diseases. 2019 Oct 11:19(1):838. doi: 10.1186/s12879-019-4439-8. Epub 2019 Oct 11 [PubMed PMID: 31604429]
Level 3 (low-level) evidenceKappus KK, Juranek DD, Roberts JM. Results of testing for intestinal parasites by state diagnostic laboratories, United States, 1987. MMWR. CDC surveillance summaries : Morbidity and mortality weekly report. CDC surveillance summaries. 1991 Dec:40(4):25-45 [PubMed PMID: 1779956]
Kappus KD, Lundgren RG Jr, Juranek DD, Roberts JM, Spencer HC. Intestinal parasitism in the United States: update on a continuing problem. The American journal of tropical medicine and hygiene. 1994 Jun:50(6):705-13 [PubMed PMID: 8024063]
Level 3 (low-level) evidenceNorouzi P, Mohaghegh MA, Ghorbani M, Mirzaii M, Abolhassani M, Mirbadie SR. Investigating the prevalence of intestinal parasites with an emphasis on Strongyloides stercoralis infection in hospitalized patients: a regional report from Iran. Annals of parasitology. 2020:66(3):365-371. doi: 10.17420/ap6603.275. Epub [PubMed PMID: 33128862]
Histochemical and histopathologic studies of alveolar mucosa under complete dentures., Razek MK,Shaaban NA,, The Journal of prosthetic dentistry, 1978 Jan [PubMed PMID: 32099570]
Sobati H. Epidemiological Study of Parasitic Infections in BuMusa Island, Hormozgan. Iranian journal of parasitology. 2020 Jul-Sep:15(3):425-434. doi: 10.18502/ijpa.v15i3.4208. Epub [PubMed PMID: 33082808]
Abbaszadeh Afshar MJ, Barkhori Mehni M, Rezaeian M, Mohebali M, Baigi V, Amiri S, Amirshekari MB, Hamidinia R, Samimi M. Prevalence and associated risk factors of human intestinal parasitic infections: a population-based study in the southeast of Kerman province, southeastern Iran. BMC infectious diseases. 2020 Jan 6:20(1):12. doi: 10.1186/s12879-019-4730-8. Epub 2020 Jan 6 [PubMed PMID: 31906872]
Tanyuksel M, Yilmaz H, Ulukanligil M, Araz E, Cicek M, Koru O, Tas Z, Petri WA Jr. Comparison of two methods (microscopy and enzyme-linked immunosorbent assay) for the diagnosis of amebiasis. Experimental parasitology. 2005 Jul:110(3):322-6 [PubMed PMID: 15955332]
Level 3 (low-level) evidenceDhanabal J, Selvadoss PP, Muthuswamy K. Comparative study of the prevalence of intestinal parasites in low socioeconomic areas from South chennai, India. Journal of parasitology research. 2014:2014():630968. doi: 10.1155/2014/630968. Epub 2014 Jan 21 [PubMed PMID: 24587897]
Level 2 (mid-level) evidenceYousif Abd Elbagi Y, Abd Alla AB, Saad MBE. The relationship between Helicobacter pylori infection and intestinal parasites in individuals from Khartoum state, Sudan: a case-control study. F1000Research. 2019:8():2094. doi: 10.12688/f1000research.21397.2. Epub 2019 Dec 12 [PubMed PMID: 32765829]
Level 2 (mid-level) evidenceAbdalazim Hassan H, Abd Alla AB, Elfaki TEM, Saad MBEA. Frequencies of gastrointestinal parasites among students of primary school in Al Kalakla Locality, Khartoum State, Sudan: a cross-sectional study. F1000Research. 2019:8():1719. doi: 10.12688/f1000research.20610.3. Epub 2019 Oct 4 [PubMed PMID: 32913632]
Peña-Quistial MG, Benavides-Montaño JA, Duque NJR, Benavides-Montaño GA. Prevalence and associated risk factors of Intestinal parasites in rural high-mountain communities of the Valle del Cauca-Colombia. PLoS neglected tropical diseases. 2020 Oct:14(10):e0008734. doi: 10.1371/journal.pntd.0008734. Epub 2020 Oct 9 [PubMed PMID: 33035233]
Hernández PC, Morales L, Chaparro-Olaya J, Sarmiento D, Jaramillo JF, Ordoñez GA, Cortés F, Sánchez LK. Intestinal parasitic infections and associated factors in children of three rural schools in Colombia. A cross-sectional study. PloS one. 2019:14(7):e0218681. doi: 10.1371/journal.pone.0218681. Epub 2019 Jul 10 [PubMed PMID: 31291262]
Level 2 (mid-level) evidencePanti-May JA,Zonta ML,Cociancic P,Barrientos-Medina RC,Machain-Williams C,Robles MR,Hernández-Betancourt SF, Occurrence of intestinal parasites in Mayan children from Yucatán, Mexico. Acta tropica. 2019 Jul [PubMed PMID: 31022382]
Jacobsen KH, Ribeiro PS, Quist BK, Rydbeck BV. Prevalence of intestinal parasites in young Quichua children in the highlands of rural Ecuador. Journal of health, population, and nutrition. 2007 Dec:25(4):399-405 [PubMed PMID: 18402182]
Légeret C, Rüttimann C, Furlano RI, Ruf T, Poppert S, Fankhauser H, Köhler H. Blastocystis in Swiss children: a practical approach. European journal of pediatrics. 2020 Jun:179(6):979-984. doi: 10.1007/s00431-020-03599-3. Epub 2020 Feb 5 [PubMed PMID: 32020333]
M'rad S, Chaabane-Banaoues R, Lahmar I, Oumaima H, Mezhoud H, Babba H, Oudni-M'rad M. Parasitological Contamination of Vegetables Sold in Tunisian Retail Markets with Helminth Eggs and Protozoan Cysts. Journal of food protection. 2020 Jul 1:83(7):1104-1109. doi: 10.4315/JFP-19-559. Epub [PubMed PMID: 32074629]
El Bakri A,Hussein NM,Ibrahim ZA,Hasan H,AbuOdeh R, Intestinal Parasite Detection in Assorted Vegetables in the United Arab Emirates. Oman medical journal. 2020 May [PubMed PMID: 32550016]
Fotedar R, Stark D, Beebe N, Marriott D, Ellis J, Harkness J. Laboratory diagnostic techniques for Entamoeba species. Clinical microbiology reviews. 2007 Jul:20(3):511-32, table of contents [PubMed PMID: 17630338]
Level 3 (low-level) evidenceTrissl D, Martínez-Palomo A, de la Torre M, de la Hoz R, Pérez de Suárez E. Surface properties of Entamoeba: increased rates of human erythrocyte phagocytosis in pathogenic strains. The Journal of experimental medicine. 1978 Nov 1:148(5):1137-43 [PubMed PMID: 722237]
Level 3 (low-level) evidenceMarkell EK, Kuritsubo R. The food of Entamoeba coli. The Journal of parasitology. 1967 Oct:53(5):1108 [PubMed PMID: 6062066]
Level 3 (low-level) evidenceVOGE M,KESSEL JF, Sphaerita in cysts of Entamoeba coli. The Journal of parasitology. 1958 Aug; [PubMed PMID: 13564367]
Craig CF. The Classification of the Parasitic Amebae of Man. The Journal of medical research. 1917 Jan:35(3):425-42 [PubMed PMID: 19972346]
Wahlgren M. Entamoeba coli as cause of diarrhoea? Lancet (London, England). 1991 Mar 16:337(8742):675 [PubMed PMID: 1672011]
Level 3 (low-level) evidenceVerweij JJ, Laeijendecker D, Brienen EA, van Lieshout L, Polderman AM. Detection and identification of entamoeba species in stool samples by a reverse line hybridization assay. Journal of clinical microbiology. 2003 Nov:41(11):5041-5 [PubMed PMID: 14605136]
Level 3 (low-level) evidenceGungoren B, Latipov R, Regallet G, Musabaev E. Effect of hygiene promotion on the risk of reinfection rate of intestinal parasites in children in rural Uzbekistan. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2007 Jun:101(6):564-9 [PubMed PMID: 17418321]
Level 1 (high-level) evidence