Introduction
The ductus arteriosus is a short vessel that connects the fetal pulmonary artery to the aorta and involutes it following birth. During development, the ductus arteriosus allows oxygenated blood to bypass the pulmonary circulation and provides nutritional and oxygen-rich blood directly into the systemic circulation. After birth, the ductus arteriosus closes, and its remnant is referred to as the ligamentum arteriosum. A failure of the closure of the ductus arteriosus leads to a patent ductus arteriosus (PDA) which may cause a left-to-right shunt post-birth. A PDA may be repaired either medically using non-steroidal anti-inflammatory agents (NSAIDs) or surgically.[1][2][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
During fetal development, the ductus arteriosus serves as a shunt between the pulmonary artery and the aorta. In the fetus, blood is oxygenated in the placenta and ultimately pumped to the body systems. The fetal lungs are filled with amniotic fluid and, therefore, cannot be used to oxygenate the blood. The arterioles in the lungs are constricted, which restricts the volume of blood that can pass through the pulmonary system. Since fetal blood leaving the placenta is already oxygen-rich, and the lungs are non-functional, the ductus arteriosus allows some of this blood to bypass the pulmonary circulation to enter directly into the systemic circulation. The ductus arteriosus is maintained in its open conformation by being exposed to the E series prostaglandins, which are in relatively high concentrations before birth. These prostaglandins are produced by the ductus and placenta.
Shortly after birth and the first breath, the lungs fill with oxygen, and the pulmonary arterioles dilate. This change in pulmonary-arteriole resistance allows for a significant increase in pulmonary blood flow. Around the same time, the placenta is removed from circulation by the contraction or clamping of the umbilical cord, resulting in a drop in prostaglandin levels. The ductus arteriosus responds to these changes by contracting and closing, ultimately forming the ligamentum arteriosum. The closure of the ductus arteriosus prevents oxygenated blood from returning to the pulmonary circulation and reducing cardiac efficiency. The closure of the ductus arteriosus typically occurs within the first three months of life. However, there are times when the ductus fails to close, resulting in a condition known as a patent ductus arteriosus (PDA). In certain heart conditions, a patent ductus arteriosus can be kept open by the administration of prostaglandin E1.
Embryology
The ductus arteriosus derives from the 6th aortic arch. During embryonic development, this connection forms between the first portion of the pulmonary artery and the isthmus of the aorta. This provides a path through which fetal blood can be shunted away from the pulmonary circuit and delivered directly into the systemic circulation.[4]
Surgical Considerations
The ductus arteriosus can be of surgical importance when treating certain congenital heart defects. One such example is when a child is born with transposition of the great arteries. In this condition, the ascending aorta and the pulmonary trunk are switched in their locations; this leads to an inability for oxygenated blood to leave the pulmonary circulation and enter the systemic circulation. If left untreated, this condition is incompatible with life.[5] In these situations, an arterial switch is the only definitive treatment.[6] In these situations, prostaglandin E1 is often administered prophylactically to maintain the patency of the ductus arteriosus until a surgical correction can be made. This allows for blood to mix between the two distinct circulatory circuits.
Another important surgical consideration is in cases where a patent ductus arteriosus is resistant to medical treatment. In these cases, the ductus arteriosus can be closed manually in surgery. There are two different approaches used to accomplish this. A more traditional surgical approach requires the surgeon to open the thoracic cavity and ligate the vessel directly. The other is much less invasive and is done percutaneously. This version of the procedure involves the intravenous delivery of an occlusion device that plugs up the shunt from within.[7][8]
Clinical Significance
Patent Ductus Arteriosus
Patent ductus arteriosus (PDA) is a condition in which the ductus arteriosus fails to close after birth. A PDA is one of the most common cardiac defects associated with congenital rubella syndrome and may severely impact an infant's quality of life.[9] The PDA leads to the generation of a left-to-right shunt since the blood pressures in the aorta are much higher than in the pulmonary artery. If allowed to remain patent, the pressure inside the pulmonary circuit will rise, leading to pulmonary hypertension. Failure to adequately address this pulmonary hypertension may lead to cyanosis and shunt reversal (Eisenmenger syndrome). Late complications of Eisenmenger syndrome include arrhythmias and sudden cardiac death. The development of this syndrome indicates irreversible changes to the cardiac and pulmonary vasculature, and lung/cardiac transplants are the only viable treatment option.[10]
During fetal development, prostaglandins (E1 and E2) are responsible for maintaining the patency of the ductus arteriosus. Prostaglandin E2 has the most potent effect and is produced both by the placenta and the ductus arteriosus itself.[11] A patent ductus arteriosus can also be induced by the direct administration of prostaglandin E1. This is often done to maintain circulation in children born with life-threatening congenital heart defects. One such example is when a child is born with transposition of the great vessels, a condition where the aorta and pulmonary trunk are switched in location. Ordinarily, this condition would exclude oxygenated blood from entering the systemic circulation. However, a patent ductus arteriosus allows oxygenated blood to cross over and buys the surgeon time to prepare for surgery.
Patent ductus arteriosus is often treated medically with non-steroidal anti-inflammatory drugs (NSAIDs) such as indomethacin.[12] These medications work by inhibiting the synthesis of prostaglandins and, therefore, decreasing their concentration in the blood. Studies have shown that premature infants born to non-Caucasian mothers are more responsive to indomethacin treatment for PDA than Caucasian infants. It has been suggested that this may be associated with the expression of genes involved with nitric oxide production.[4] In refractory cases, however, surgery can be done to close the shunt manually.
It should also be noted that NSAIDs taken during pregnancy can increase the risk of early closure of the ductus arteriosus. For this reason, it is often advised that pregnant mothers avoid these medications after 30 weeks of gestation.
Aortic Transection
An aortic transection is a condition where the aorta is torn or ruptured due to some trauma. This condition is most often fatal shortly after its onset since the aorta is the largest vessel in the body and supplies blood directly from the heart to the rest of the vessels. The most frequent site of aortic transection is at the location where the ligamentum arteriosum, the remnant of the ductus arteriosus, attaches to the aorta. The ligamentum arteriosum acts as a tether that holds the aorta and pulmonary artery close to each other. When the body experiences a rapid deceleration (such as in a car crash), a large shearing force is applied to these great vessels due to the rigidity of this tether. This sheering force is responsible for the subsequent rupture of the aorta.[13]
Media
(Click Image to Enlarge)
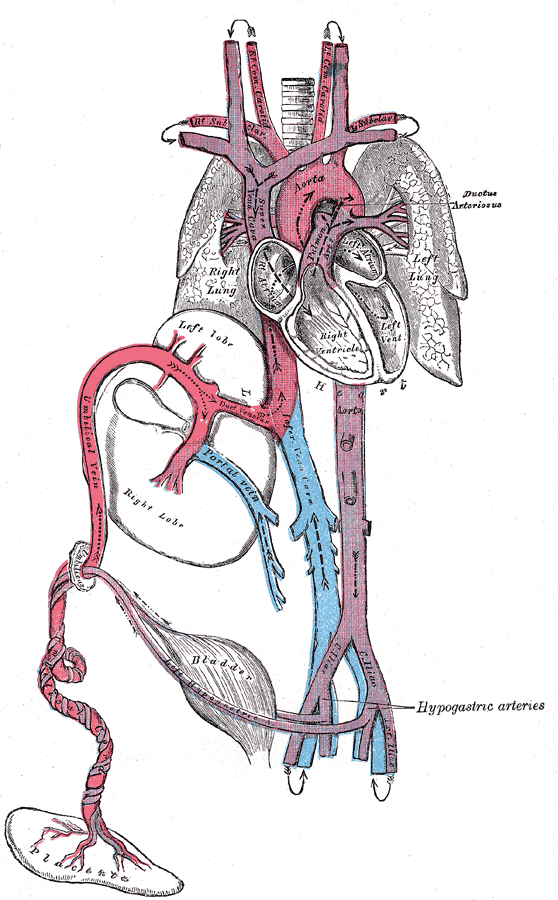
Ductus Arteriosus in fetal circulation Contributed by Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body, Public Domain, https://commons.wikimedia.org/w/index.php?curid=560282
References
Agrawal H, Waller BR 3rd, Surendan S, Sathanandam S. New Patent Ductus Arteriosus Closure Devices and Techniques. Interventional cardiology clinics. 2019 Jan:8(1):23-32. doi: 10.1016/j.iccl.2018.08.004. Epub [PubMed PMID: 30449419]
Borràs-Novell C, Riverola A, Aldecoa-Bilbao V, Izquierdo M, Domingo M. Clinical outcomes after more conservative management of patent ductus arteriosus in preterm infants. Jornal de pediatria. 2020 Mar-Apr:96(2):177-183. doi: 10.1016/j.jped.2018.10.004. Epub 2018 Nov 10 [PubMed PMID: 30423323]
Level 2 (mid-level) evidenceSathanandam S, Balduf K, Chilakala S, Washington K, Allen K, Knott-Craig C, Rush Waller B, Philip R. Role of Transcatheter patent ductus arteriosus closure in extremely low birth weight infants. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2019 Jan 1:93(1):89-96. doi: 10.1002/ccd.27808. Epub 2018 Sep 30 [PubMed PMID: 30269408]
Waleh N, Barrette AM, Dagle JM, Momany A, Jin C, Hills NK, Shelton EL, Reese J, Clyman RI. Effects of Advancing Gestation and Non-Caucasian Race on Ductus Arteriosus Gene Expression. The Journal of pediatrics. 2015 Nov:167(5):1033-41.e2. doi: 10.1016/j.jpeds.2015.07.011. Epub 2015 Aug 8 [PubMed PMID: 26265282]
Villafañe J, Lantin-Hermoso MR, Bhatt AB, Tweddell JS, Geva T, Nathan M, Elliott MJ, Vetter VL, Paridon SM, Kochilas L, Jenkins KJ, Beekman RH 3rd, Wernovsky G, Towbin JA, American College of Cardiology’s Adult Congenital and Pediatric Cardiology Council. D-transposition of the great arteries: the current era of the arterial switch operation. Journal of the American College of Cardiology. 2014 Aug 5:64(5):498-511. doi: 10.1016/j.jacc.2014.06.1150. Epub [PubMed PMID: 25082585]
van Wijk SW, Driessen MMP, Meijboom FJ, Takken T, Doevendans PA, Breur JM. Evaluation of Left Ventricular Function Long Term After Arterial Switch Operation for Transposition of the Great Arteries. Pediatric cardiology. 2019 Jan:40(1):188-193. doi: 10.1007/s00246-018-1977-6. Epub 2018 Sep 10 [PubMed PMID: 30203292]
Ashrafi AH, Levy VY. Management strategies for the preemie ductus. Current opinion in cardiology. 2019 Jan:34(1):41-45. doi: 10.1097/HCO.0000000000000580. Epub [PubMed PMID: 30394907]
Level 3 (low-level) evidenceChoi GJ, Song J, Kim YS, Lee H, Huh J, Kang IS. Outcomes of transcatheter closure of ductus arteriosus in infants less than 6 months of age: a single-center experience. Korean journal of pediatrics. 2018 Dec:61(12):397-402. doi: 10.3345/kjp.2018.06548. Epub 2018 Sep 19 [PubMed PMID: 30304903]
Khurana S, Bansal A, Saini SS, Mishra A, Kumar P. Severe Pulmonary Arteriopathy in a Neonate with Congenital Rubella Syndrome and Patent Ductus Arteriosus. Indian pediatrics. 2019 Oct 15:56(10):868-872 [PubMed PMID: 31724543]
Hung YC, Yeh JL, Hsu JH. Molecular Mechanisms for Regulating Postnatal Ductus Arteriosus Closure. International journal of molecular sciences. 2018 Jun 25:19(7):. doi: 10.3390/ijms19071861. Epub 2018 Jun 25 [PubMed PMID: 29941785]
Yokoyama U. Prostaglandin E-mediated molecular mechanisms driving remodeling of the ductus arteriosus. Pediatrics international : official journal of the Japan Pediatric Society. 2015 Oct:57(5):820-7. doi: 10.1111/ped.12769. Epub [PubMed PMID: 26228894]
Mitra S, Florez ID, Tamayo ME, Mbuagbaw L, Vanniyasingam T, Veroniki AA, Zea AM, Zhang Y, Sadeghirad B, Thabane L. Association of Placebo, Indomethacin, Ibuprofen, and Acetaminophen With Closure of Hemodynamically Significant Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-analysis. JAMA. 2018 Mar 27:319(12):1221-1238. doi: 10.1001/jama.2018.1896. Epub [PubMed PMID: 29584842]
Level 1 (high-level) evidenceSommer G,Sherifova S,Oberwalder PJ,Dapunt OE,Ursomanno PA,DeAnda A,Griffith BE,Holzapfel GA, Mechanical strength of aneurysmatic and dissected human thoracic aortas at different shear loading modes. Journal of biomechanics. 2016 Aug 16 [PubMed PMID: 26970889]