Indications
Water constitutes about 60% of the average adult body weight and is responsible for many physiological processes in the human body. Thus, fluid and electrolyte homeostasis is critical for human survival, as exemplified by the potentially devastating consequences of fluid imbalance. The balance of total body fluid is an extremely well-regulated process that ensures the maintenance of a balance between fluid gain and loss through different physiological mechanisms such as neural regulation of thirst, hormonal regulation (vasopressin and natriuretic peptides), management through the skin, hemodynamic changes, and renal control of salt and water excretion. In particular, renal excretion of urine also ensures the elimination of products of metabolic activity and excess electrolytes in addition to water, thus maintaining fluid homeostasis. Fluid balance so inextricably links with electrolyte balance both in the intracellular (rich in K+ ions) and extracellular (rich in Na+ & Cl- ions) compartments, that unsurprisingly, trading of electrolytes is the core strategy of renal fluid regulation. Drugs that affect renal regulation of electrolyte excretion have the greatest effect in terms of the quantity of fluid control and thus water homeostasis.[1][2][3]
Diuretics are drugs that pharmacologically tilt the renal fluid regulation in favor of the excretion of water and electrolytes. Thus, diuretics are substances that increase the production and volume of urine. This class of drugs achieves this objective primarily by suppressing receptors that aid in the reabsorption of Na+, the most abundant extracellular cation, from the renal tubules, thereby increasing the osmolality of the renal tubules and consequently suppressing water reabsorption. Osmotic diuretics cause a direct increase in luminal hyperosmolarity in the renal tubules without affecting electrolyte balance, whereas aquaretics are substances that act directly by only affecting the excretion of water.[4][5]
This comprehensive review addresses all the relevant aspects of diuretic therapy, emphasizing the understanding of the basic pharmacophysiological mechanisms of drug action and that of adverse effects but also to more pragmatic aspects of dosing. Diuretics fall into several classes and subcategories depending on their mechanism and site of their action along the nephron. The classification is presented in Table 1, which lists all the available individual drugs in all the different classes, their peculiarities, chemical nature, their major site of action along the nephron, diuretic target molecule, and the percentage of Na+ reabsorption blocked.[6][7][8] Additionally, Table 1 also gives information (to put things in a broader perspective) about miscellaneous agents that do not have a conspicuous diuretic action and are not used for diuresis, but they do have some diuretic effect which is noticeable which must be taken into account during therapy with these agents.
Indications
Diuresis is necessary for a variety of non-edematous and edematous conditions, which require clearing out excess water when the body abnormally sequesters fluid in the third space in the form of edema. Indications for each individual drug are given below in tables 2 through 5. The quintessential of edematous conditions is heart failure (HF), where the inefficiency of the heart’s pumping ability results in:
1. Decreased renal perfusion leading to activation of the renin-angiotensin-aldosterone-system (RAAS) and
2. Long-standing venous stasis leading to extravasation of fluid into the interstitial space, both of which lead to intravascular volume expansion and result in signs of congestion such as weight gain, dyspnea, and generalized edema.[9]
Pulmonary edema, most commonly resulting from HF, is also an indication for diuretic use. Loop diuretics (due to their greater effectiveness) are the cornerstone of diuretic therapy in symptomatic HF, with furosemide being the most widely used loop diuretic (albeit Torsemide with better pharmacological properties remains underexploited and a comparison trial, TRANSFORM-HF, is currently underway) according to both New York Heart Association (NYHA) and European Society of Cardiology (ESC). These agents are started at lower doses, titrated upwards, and monitored through urine output and body weight measurements. The addition of thiazide diuretics (metolazone, hydrochlorothiazide) to loop diuretics can help relieve symptoms when loop diuretics are not sufficient in HF, as detailed below in the administration section. Aldosterone receptor antagonists (ARA) reduce the mortality and morbidity of advanced systolic HF and patients with ejection fraction less than 35% falling into NYHA-HF classification categories II-IV. This effect is because aldosterone escapes suppression on chronic use of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs), whereas the addition of ARAs can protect from the effects of aldosterone in such patients.[10][11][12]
Diuretics, along with salt restriction, are also recommended as the first-line therapy in ascites due to liver cirrhosis.[13] In cirrhotic ascites, spironolactone is the drug of choice for initial therapy (due to its antiandrogenic effect), although a loop diuretic may be added as an adjunct if the treatment fails or can be added at the outset in synergistic combination therapy.[14][15] In both HF and cirrhosis, renal dysfunction contributes to the pathophysiology through further activation of RAAS to increase fluid retention.[16][17] Fluid overload that develops in renal insufficiency or acute kidney injury patients increases mortality, and loop diuretics are the favored initial therapy in these patients though renal replacement therapy is the long-term solution.[18][19] Nephrotic syndrome (NS), characterized by hypoalbuminemia, proteinuria, and hyperlipidemia, is an edematous condition that requires diuretic therapy.[18] Activation of epithelial Na+ channels (ENaCs) in the collecting ducts is the mechanism of edema formation in NS, while RAAS activation could also play a minor role. All the diuretics are serum albumin-bound, and hence hypoalbuminemia in NS decreases the load of diuretic delivered to the renal tubules. Co-administration of albumin with furosemide or a combination of furosemide and ENaC inhibitor such as triamterene has shown some success in kidney disease patients with hypoalbuminemia.[20][21] A gain-of-function mutation in ENaC receptors clinically causes Liddle syndrome, for which ENaC inhibitor amiloride is the treatment of choice.[22]
Thiazides are the best first choice for hypertension, as concluded in a recent Cochrane review, and chlorthalidone is the best first-line agent among all the anti-hypertensive compared according to the 2017 American college of cardiology (ACC) hypertension guidelines.[23][24] Chlorthalidone, with its longer duration of action and longer half-life at lower doses, was found to significantly reduce the risk of cardiovascular (CV) events when compared to other anti-hypertensive medications. Indapamide has lower metabolic adverse effects when compared to chlorthalidone due to its non-interference in lipid or glucose metabolism and much safer for use in hypertension, making it suitable for patients with diabetes. Direct vasodilatory effects of thiazide-like diuretics also contribute to lowering blood pressure (BP) on long-term therapy. On the other hand, loop diuretics may be the preferred agent when hypertension is associated with chronic kidney disease (CKD) or glomerular filtration rate (GFR) less than or equal to 30 mL/min (though some recent reports still favor thiazides in this setting) and potassium-sparing diuretics (PSD) are used in hypertensive patients with K+ or Mg2+ loss.[25][26][27][28][29]
Thiazide-related reabsorption of calcium might be advantageous in nephrolithiasis and hypercalciuria, whereas loop diuretics cause calciuresis and therefore are suitable for use in symptomatic hypercalcemia patients.[30][31] Diabetes insipidus, a polyuric disease, results in a loss of dilute urine with low sodium levels, and paradoxically thiazide diuretics can help by increasing distal tubule Na+ excretion, which compensatively increases water and Na+ reabsorption in the proximal tubule (PT); thus impairing the maximum diluting capacity of kidneys.[32][33] Acetazolamide, the only carbonic anhydrase inhibitor available, induces metabolic acidosis by increased bicarbonate excretion and is used as a prophylaxis in high altitude sickness where it counteracts the hypoxia-induced respiratory alkalosis raising the PaO2. With similar logic, its use is warranted in reversing metabolic alkalosis.[34] Acetazolamide effectively reduces the intraocular pressure and is used for short-term therapy for open-angle glaucoma when topical therapy is not feasible.[35] There is inconclusive evidence “for” or “against” the use of diuretics in Ménière disease.[36]
Osmotherapy is the mainstay of medical therapy for raised intracranial pressure (ICP) after traumatic brain injury and cerebral edema. Hyperosmolar therapy with mannitol reduces elevated ICP rapidly in less than an hour though a rebound (an initial increase of ICP) is possible. Mannitol also promotes diuresis in acute renal failure and excretion of toxic metabolites and substances. Though hypertonic saline similarly is used to treat high ICP and sometimes has demonstrated greater efficiency than mannitol is not considered a diuretic.[37][38]
Diuretics can also be employed less commonly in the active elimination of toxic substances by forced diuresis, which increases urine volume per unit time. Clinicians employ loop diuretics along with alkalinization of the urine in forced alkaline diuresis in the treatment of salicylate, phenobarbital, and lithium poisoning.[39][40] Loop diuretics (along with salt tablets) are also used as a second-line therapy to decrease urine concentration in the syndrome of inappropriate antidiuretic hormone secretion (SIADH), where the mainstay of therapy is the restriction of water intake.[41] The loop diuretic bumetanide has shown effectiveness as an anti-seizure drug. It is used in temporal lobe epilepsy in addition to other central nervous system pathologies such as autism and schizophrenia.[6]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Almost all diuretics act by targeting ion transport receptors present on the luminal surface in the renal tubules, except for ARAs, which act on cytosolic steroid receptors. All the diuretics are bound to albumin, and as glomerular filtration excludes macromolecules such as albumin, active secretion of diuretic agents into the lumen is a prerequisite for their action. ARAs reach the distal tubule via the blood and act on the mineralocorticoid receptor (MR) in the cytoplasm of the principal cells.[42] Diuretics, which are acidic (loop, thiazides, and acetazolamide) or basic (ENaC inhibitors), are secreted respectively via the organic anion or organic cation transporters (OATs, OCTs), located on the basolateral surface of cells in the straight segment of PT.[43]
Certain general principles regarding renal physiology are critical for a thorough understanding of diuretic action and its adverse effects. The following section will explain the mechanisms of action of different diuretics, starting with a brief physiological introduction of the concerned portion of the renal tubule followed by the mechanism of action of the particular diuretic.
- Carbonic Anhydrase Inhibitors
In the Bowman’s capsule, plasma from the renal artery passes through the three-layered glomerular ultrafiltration system and delivers an ultrafiltrate that is isotonic to that of plasma. The contiguous PT reabsorbs about 60 to 70% of the filtered load, including Na+, water along with bicarbonates (HCO3+), organic solutes (glucose and amino acids), electrolytes, and other substances. Such massive reabsorptive capacity occurs with the help of the specific transport receptors in the brush border cells, which increases the surface area of the PTs yielding a fluid, in the end, that is isotonic (300 mOsm/kg) with the plasma.[44] Na+ in the filtrate gets reabsorbed and enters the cell in exchange for H+ (present inside the cells) through Na+-H+ exchanger (NHE3) present in the luminal membrane and maintains electrical neutrality across the membrane. The H+ ions that reached the lumen combine with the filtered HCO3+ ions to form carbonic acid (H2CO3) in the lumen, and this breaks down into H2O and CO2 with the help of the enzyme carbonic anhydrase present on the luminal side of the brush border cell. CO2 diffuses back into the cell, and H2O is reabsorbed via aquaporin-1 channels into the cell, both of which combine to form H2CO3 with the help of cellular carbonic anhydrase, which further catalyzes them to form HCO3+ and H+ ions inside the cells. Almost 80% of filtered HCO3+ is reabsorbed in the PT cells in this way and exits the basolateral membrane along with Na+ (that entered via NHE3 channels) through the Na+/HCO3+ co-transporter (NBCe1). Na+-K+-ATPase pump avidly depletes the excess cellular Na+ ions along the basolateral membrane while also providing the energy for NHE3 channels by creating low Na+ levels inside the cell.[45][46][47][48] The renal reabsorption of HCO3+ and secretion of H+ ions play an important role in acid-base homeostasis and the steady maintenance of pH in the body.
Acetazolamide, the only CAI, acts on this segment. Acetazolamide interferes non-competitively with both the luminal and cellular carbonic anhydrase enzymes resulting in impairment of Na+, HCO3+, and water reabsorption. Though acetazolamide targets the proximal portion of the renal tubule, where the majority of the Na+ ions undergo reabsorption, compensatory processes develop in the distal portions to reabsorb the increased distally delivered Na+ ions. These processes include the Na+ reabsorption mechanisms in the loop of Henle, the distal convoluted tubule (DCT), the activation of tubuloglomerular feedback (TGF), and in amiloride-sensitive distal nephron (ASDN) through ENaCs. Increased HCO3+ leads to alkaline diuresis, causing decreased serum HCO3+ levels which further undermines the substrate availability for carbonic anhydrase mediated Na+ reabsorption in the PTs resulting in decreased efficiency of acetazolamide.[49][50]
Acetazolamide acts on carbonic anhydrase, causing loss of HCO3+ ions in the urine leading to metabolic acidosis. The physiological response of the body to compensate for this loss of HCO3+ ions is by decreasing the levels of CO2, in other words, by causing respiratory alkalosis; this takes place by hyperventilation, which leads to increased expiration of CO2, leading to higher partial pressures of O2 in the arterial blood. As high altitude is a low O2 environment, the action of acetazolamide decreases the incidence of tissue hypoxia in high altitudes. Thus it is the drug of choice in altitude sickness.
- Loop Diuretics
The cortical proximal convoluted tubule descends into the outer medulla to continue as the thin descending limb of the loop of Henle, forms a hairpin loop in the inner medulla, and ascends back as thin and thick portions of the ascending limb of the loop and reaches back to the cortex. This structural arrangement is critical for the urinary concentrating ability of the kidney achieved by the countercurrent multiplier system of the loop of Henle. Electroneutral Na+-K+-2Cl- co-transporter 2 (NKCC2) present in the apical surface of thick ascending limb (TAL) reabsorbs 25 - 30% of the filtered Na+ into the cells. The driving force for this action is the favorable low Na+ concentration in the tubular cells achieved by the Na+-K+-ATPase antiporter pump present in the basolateral membrane. This channel pumps 3 Na+ out of the cell (into the interstitium) for every 2 K+ that comes into the cell. Excess chloride from the cells is transported via the chloride-specific channels (ClC-Ka and ClC-Kb) and the basolateral side, which requires Barttin beta-subunits for their action. Renal outer medullary K+ (ROMK) channel present in the luminal membrane, in turn, secretes and recycles back the K+ from the cell into the lumen with the help of ATP. Collectively, this not only results in creating a hyperosmolar medullary interstitial environment but also a luminal positive charge that repels luminal cations Na+, Ca2+, and Mg2+ via the paracellular pathway into the interstitium. Of note, TAL, devoid of aquaporins, is impermeable to water, and reabsorption of only the tubular solutes leads to dilution resulting in a hypotonic fluid inside the lumen (thus aka diluting segment). The thin descending segment of the loop is permeable to water, and the hyperosmolarity in the medulla draws the water out of this segment through the aquaporin-1 channels resulting in a hypertonic tubular fluid. As this tubular fluid flows continuously in the loop, repeated actions in thick and thin limbs create an osmolar gradient in the length of the medulla with concentrations in the inner medulla that can reach up to 1200 mOsm/kg of H2O.[51][52][53][54] Loop diuretics act on this segment.
Loop diuretics act principally by blocking the electroneutral NKCC2 (isoform in the kidneys) channels located on the luminal (apical) membrane of the TAL. Every loop diuretic has a distinct chemical structure, but all are anions that assist in blocking the chloride-binding site of the translocation pocket of the NKCC2 transmembrane receptor.[55] Blockage of NKCC2 action in the TAL results in inhibition of Na+, K+, and 2Cl- reabsorption and reduced interstitial tonicity, thereby thwarting the countercurrent mechanism of urinary concentration. Within the lumen, however, the dilution function of the TAL is compromised and results in excess Na+ delivery to the distal tubules by which one would expect would lead to an activation of the tubuloglomerular feedback (TGF) mechanism. TGF is a mechanism that is activated when macula densa, specialized epithelial cells in the distal tubule, senses increased NaCl levels in the lumen and causes constriction of afferent glomerular arterioles, thereby reducing the GFR. It turns out macula densa cells also contain the NKCC2 symporters, and their antagonism by loop diuretics causes decreased salt sensing ability in these cells, which results in inhibition of the TGF mechanism. Low-salt or diuretic volume depletion also induces the release of renin, activating the RAAS pathway, which helps maintain GFR by increasing BP.[56] Loop diuretics are the most potent among all the diuretics as they inhibit the largest amount of Na+ reabsorption (25% of filtered Na+). The high efficiency of loop diuretics results from profound diuretic action and therefore has acquired the tag of “high-ceiling” and “high-efficiency” diuretics.[54][57]
Acute tolerance to loop diuretics occurs within sometime after dosing and can cause a ‘braking phenomenon,’ which is rebound retention of Na+ due to increased reabsorption from the distal tubules, while chronic tolerance can occur due to distal tubular structural adaptation by the kidneys to increase Na+ retention. Acute tolerance can be overcome by choosing the correct dosage, dosing frequency, the timing of diet, and dietary salt restriction. Chronic tolerance in HF may cause diuretic resistance leading to refractory HF, and this can sometimes be overcome by increasing the dose of loop diuretics, co-administering thiazide-like diuretics along with loop diuretics to perform a sequential nephron blockade and/or dopamine can be administered to improve renal perfusion. Also, the combination of acetazolamide and loop diuretics has demonstrated effectiveness in diuretic resistance as acetazolamide can overcome the proximal tubular Na+ reabsorption.[58][59][60][61]
Mutation of NKCC2 channels causes Type I Bartter’s syndrome, which is usually present at birth and characterized by hypokalemic metabolic alkalosis, hypomagnesemia, and nephrocalcinosis.[62]
- Thiazide Diuretics
The distal convoluted tubule (DCT) starts at the macula densa and ends at the collecting duct, and 5 to 10% of the filtered Na+ load is reabsorbed here via the NaCl co-transporter (NCC). NCC channels can be activated by aldosterone, insulin, vasopressin, and angiotensin II, leading to increased NaCl reabsorption. NCC is an electroneutral Na+ and Cl- symporter, expressed throughout the DCT, and like NKCC2, derives its energy from low cellular Na+ achieved by basolateral Na+-K+-ATPase pump. As NCC channels are the predominant mechanism for Na+ reabsorption in DCT, this segment is endowed with abundant mitochondria to supply ATP for the pump. Reabsorbed Na+ exits the cell via the basolateral Na+-K+ pump into the interstitium, while Cl- is transported to the interstitium via the basolateral ClC-Kb and K+-Cl- co-transporter4 (KCC4). Tubular K+ secretion occurs through both ROMK and “maxi”-K+ channels in high-flow conditions and only through ROMK in low-flow conditions. In contrast to TAL, 10% of both Ca2+ and Mg2+ reabsorption occurs only via active transport via transient receptor potential (TRP) channel subfamilies. The early portion of DCT (with only NCC channels) has a zero potential, while the late DCT has a luminal negative voltage due to the presence of electrogenic ENaC channels here. Due to the absence of aquaporins, it is considered the terminal diluting segment of the nephron and dilutes the urine further before it reaches the next segment. Thiazide diuretics and ENaC inhibitors act on this segment.[63][64]
Thiazide diuretics are superior to any other diuretic agent for hypertension treatment and subdivide into two subcategories, i.e., thiazide-type and thiazide-like diuretics. Thiazide-like diuretics are so-called because they lack the benzothiadiazine backbone (thus the chemical properties associated with it), which is characteristic of Thiazide-type agents. Among the thiazides, thiazide-like drugs are exceptional and better than thiazide-type diuretics in handling high BP with the least adverse effects such as metabolic or electrolyte disturbances.[65]
In the DCTs, the most abundant Na+ reabsorption occurs through the NCC channels, which are the lone targets of thiazide diuretics. Thiazides exert their action by competitively binding to the chloride binding site of the NCC’s transmembrane domain and inhibiting the Na+ reabsorption. The important role of NCC channels is well-established as in patients with loss-of-mutation of this channel causes Gitelman syndrome manifesting with hypokalemic metabolic alkalosis, hypomagnesemia, hypocalciuria, and lower systemic BP. Gordon’s syndrome is the inverse of Gitelman’s phenotype in that they cause gain-of-function mutation of NCC leading to salt retention and is treatable with thiazides.[66]
TGF mechanism is not inhibited by thiazides (in contrast with loop agents) as the anatomical positioning of DCTs is after the macula densa. Increased renin secretion by thiazides is mediated only through volume depletion rather than low-salt delivery to the macula densa, as in loop diuretics.[67]
Low-dose thiazide-like agents are considered the best antihypertensive agent as it lowers BP on chronic use irrespective of volume depletion.[68] Though the exact mechanism is still unclear, it is theorized to occur through direct endothelial or vascular smooth muscle-mediated vasodilation (probably by altering Ca2+ regulation), reverse whole body regulation, and/or renal autoregulation.[69][23]
- Potassium-sparing Diuretics
Connecting tubules are short segments of renal tubules connecting the DCT with the collecting duct. Collecting duct forms the concluding segment of the nephron and receives only about 10% of the glomerular filtrate, and the Na+ reabsorptive capacity of this segment varies significantly from 1 to 5%.[70] Aquaporin-2 is the subtype of aquaporins expressed in both connecting tubules and collecting ducts, and their density is the highest in the medullary collecting duct. The antidiuretic hormone vasopressin acts only on the aquaporin-2 subtype of aquaporin channels located in the distal nephron and does not bind to the aquaporin-1 channels located in the proximal nephron.[71]
Apart from these structural segments, there is a functional segment of the distal nephron comprised of late DCT, connecting tubules, and collecting ducts (both cortical and medullary) are referred to as the aldosterone-sensitive distal nephron (ASDN). The principal cells are one of the major epithelial cell types located in ASDN and identify with the cytoplasmic MR for aldosterone and luminal membrane ENaC receptors. ENaC receptors expressed in ASDN are responsible for the final fine-tuning of the tubular fluid and accounts for the reabsorption of about 3% of the filtered Na+ load. The energy required for the function of ENaC derives from the electrochemical gradient created by the basolateral Na+-K+-ATPase pump. Increased reabsorption of Na+ through electrogenic ENaC creates a more negative luminal potential, paving the way for the cells to secrete K+ through the luminal ROMK channels, which express specifically in ENaC positive cells.[72][73] Alpha-intercalated cells, however, are responsible for H+ secretion in response to luminal negative charge causing tubular acidification via the proton pump H+-ATPase.[74] Both types of PSDs act on the ASDN segment.
As the name suggests, PSD overcomes the increased loss of K+ ions in the urine, thereby preventing hypokalemia, a predominant side effect of other diuretics. ENaC inhibitors and ARAs, two subcategories belonging to this class, are structurally different, and they target different types of receptors. ENaC inhibitors are pteridine analogs and are secreted in the PTs to reach the tubular lumen to bind to ENaC receptors located in the principal cells of ASDN, while ARAs are synthetic steroid analogs and bind to the cytoplasmic MR. Notwithstanding these differences, K+ retaining ability of both the subtypes of this class at the end is by their action on ENaC receptors, while the ENaC inhibitors achieve this by acting directly to suppress these receptors, ARAs act indirectly by suppressing the aldosterone-induced proteins, which increase production, redistribution (from the cytosol to membrane) and activation of ENaC receptors.[75][49]
These drugs account for the inhibition of only 3% of the filtered Na+ load and are thus not very potent diuretics. ENaC inhibitors, amiloride, and triamterene are primarily used in situations to correct hypokalemia induced by other diuretics without mineralocorticoid excess. They are also used to treat hypomagnesemia that can occur with diuretics, antibiotics, chemotherapeutic drugs, and immunosuppressants.[76][49] ENaC inhibitors are, therefore, both K+-sparing and Mg2+-sparing agents. Spironolactone being non-selective also mediates its effect through its anti-androgenic activity and can be used in the treatment of androgen-excess syndromes such as hirsutism.[77] Eplerenone is favored for the pharmacological treatment of primary aldosteronism due to its selective mineralocorticoid antagonism.[78].
- Osmotic Diuretics
As opposed to other agents, osmotic diuretics do not interfere with electrolyte reabsorptive mechanisms, and their main diuretic action is mediated through increasing osmolarity of the tubular fluid in PT and TAL of the loop of Henle. Mannitol is freely filtered nonmetabolized sugar, which increases the osmolality of both plasma and renal tubular fluid, causing osmotic diuresis. Mannitol raises the serum osmolality and since it does not cross the blood-brain barrier causes a positive blood-cerebrospinal fluid osmotic-gradient resulting in brain dehydration (without affecting the brain blood flow), the effect required for reducing the intracranial pressure. Mannitol is poorly reabsorbed and causes a wash-out of medullary solute gradient inhibiting the countercurrent urinary concentration function, thus drawing water along with it to the collecting ducts. This osmotic effect is similar to that of excess tubular glucose due to diabetes mellitus leading to polyuria.[37][38][79]
- Miscellaneous Diuretics
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are novel oral anti-diabetic medications that inhibit the low affinity, high capacity SGLT2 receptors in the PT. SGLT2 receptors are involved in the reabsorption of 90% of filtered glucose along with Na+ ions from the renal tubules and become overexpressed in Type-2 diabetes mellitus. By blocking these receptors, SGLT2 inhibitors increase glucose excretion in the urine, thereby increasing the tubular osmolarity, which in turn causes osmotic diuresis. These agents ending with the suffix –gliflozins can thus cause diuresis, natriuresis (due to associated Na+ loss) and reduce extracellular fluid volume. The diuretic action of these agents is only transient due to the development of compensatory adaptive mechanisms to maintain fluid volume by the kidneys.[80][81][82]
ACEIs and ARBs can cause natriuresis and diuresis primarily by blocking the production of the downstream molecules of the RAAS pathway, angiotensin II and aldosterone, which are involved in renal conservation of water and salt.[83] Though the antihypertensive action of these drugs is primarily due to the systemic effects of BP reduction, diuretic actions also play a minimal role. They are sometimes combined with other diuretics to enhance the effect.[84][85][86] Stronger alcoholic beverages (more than 13.5% alcohol), when consumed in moderation, can cause a transient diuretic effect without any electrolyte disturbances. Under conditions of hypohydration, alcohol does not induce any diuretic effect to restore fluid balance.[87][88]
Conivaptan and tolvaptan are not classified under diuretics but are called aquaretics due to their effects in increasing only the water excretion without any saluretic action of a diuretic. Conivaptan (IV route only) acts nonselectively on both V1A & V2 vasopressin receptors, whereas tolvaptan (oral agent) is a selective antagonist of V2 vasopressin receptors. Arginine vasopressin agonist action on its receptor leads to increased expression of luminal aquaporin-2 channels (thus promoting water reabsorption), whereas its antagonism by aquaretics leads to enhanced aquaresis. Aquaretics, with their electrolyte-sparing effect, are currently indicated for use only in hyponatremia.[89][90]
Administration
Diuretic administration is usually via the oral route, but when maximum potency is required, such as in cases of advanced HF, it can be given intravenously in a hospital setting. In such situations, continuous infusion over a specified period is preferable to bolus injections. Adverse effects (or complications) in a particular patient should be well-anticipated, and the choice of diuretic, the dose required, route of administration, and needed clinical improvement, should all merit consideration before administering any diuretic agent.
- Loop Diuretics
Loop diuretics are more than 95% albumin-bound and reach peak concentrations in 30 min to 2 hours as they are absorbed swiftly with an oral bioavailability that exceeds 80% for bumetanide and torsemide, while that of furosemide is the lowest at 50% on average. Loop diuretics are available in both oral and intravenous (IV) forms, and IV infusions can be for immediate effect. Furosemide is excreted unchanged in urine or through a renal metabolism, while bumetanide and torsemide undergo hepatic metabolism (hence respective organ damage will prolong their half-life). Torsemide has the longest half-life (3 to 4 hours) and the longest duration of action (12 hours) compared to both furosemide and bumetanide, with the practicability of once-daily dosing. Torsemide absorption is not affected by food intake, while that of furosemide and bumetanide decreases dramatically and essential to be taken on an empty stomach. Since furosemide is the most commonly used agent, dose conversion between different loop diuretics must be cautiously applied. In general, for oral diuresis 80 mg furosemide = 20 mg torsemide = 1 mg bumetanide are the conversion equivalents. While that for intravenous agents, 40 mg furosemide = 20 mg torsemide = 1 mg bumetanide are to be employed.[49][57][91] Loop diuretics are threshold drugs meaning that no diuretic effect will occur below the threshold drug concentration. The threshold level also depends on different clinical conditions and could be different for different patients. Hence to achieve effective diuresis, different doses might be required to achieve the threshold level. The lowest dose that is clinically effective should be chosen for HF treatment.[92] The frequency of dosing is also very important as loop diuretics with a shorter duration of action can cause post-diuretic Na+ retention (anti-natriuresis) as the diuretic effect wears off. Thus they are usually given on a twice-daily schedule.
CKD causes a diuretic resistant state both by reducing maximal natriuresis induces a shift in the diuretic dose-response curve rightward and downward. Loop diuretics are the primary agents used in CKD, and higher starting doses are the recommendation. For furosemide, this is in the range of 40 to 80 mg is recommended for stages 4 and 5 of CKD, whereas the usual 20 to 40 mg is recommended in stages 1 through 3 of CKD. Also, continuous infusion of loop agents is recommended in hospitalized patients (to overcome anti-natriuresis), which is particularly important in CKD patients.[57][93]
Dosage for the most common indications of the individual loop diuretics appear in Table 2.[94][95][96][11][14][92]
- Thiazide Diuretics
All thiazides are sulfonamide derivatives that are readily absorbed from the gastrointestinal (GI) tract after oral administration. The oral bioavailability of thiazides ranges from 50 to 95%, and for the two most frequently used agents, hydrochlorothiazide and chlorthalidone, it is 70% and 65%, respectively. Once in the plasma, thiazides are plasma albumin-bound and do not undergo any metabolism prior to excretion, and are secreted unchanged via urine and feces.[97] The only exception is indapamide, a thiazide-like diuretic, which undergoes extensive hepatic metabolism, and less than 7% is excreted in the urine.[98]
With a half-life of approximately 42 hours, chlorthalidone has a larger volume of distribution than its thiazide-type counterpart hydrochlorothiazide because they bind to red blood cell (RBC) carbonic anhydrase and are sequestered in these cells, reaching a concentration 7 to 10 times more than that of plasma. Thus RBCs act as a reservoir, and the drug is released into the plasma gradually, which can be utilized clinically by a once-daily dosing regimen.[99] Hydrochlorothiazide, in contrast, has a shorter half-life of about 6 to 9 hours, but this increases with long-term dosing, and some studies thus recommend once-daily dosing for this drug as well. Hydrochlorothiazide is a pregnancy category B medication.[100] While loop diuretics are recommended in all stages of CKD, Thiazides are advised only in stages 1 to 3. The risk of metabolic side effects increases at higher doses of thiazides and is usually not preferred near the maximum dose range. Dosage for the most common indications of the individual thiazide diuretics appear in Table 3.[94][95][99][23][101][96][11]
- Potassium-sparing Diuretics
ENaC inhibitor amiloride does not undergo any metabolic transformation in the body, while triamterene is metabolized into a sulfate ester by extensive hepatic metabolism. Thus in patients with liver pathology, amiloride is preferred, half of which is excreted in the urine unmetabolized while the other half passes through the feces. However, amiloride must be avoided in patients with renal dysfunction as it is excreted through tubular secretion, and due to its longer half-life, the drug can accumulate in the body in such patients and predispose to life-threatening hyperkalemia. Though comfortable once-daily dosing is possible with amiloride, its peer triamterene needs twice-daily dosing, and both these drugs have an oral bioavailability of approximately 50%.[102][103] Amiloride being a pregnancy category B medication, is safer to use for the treatment of Liddle syndrome in pregnant patients.[104]
ARA spironolactone largely undergoes metabolism in the liver into its active form canrenone, which is more than 90% bound to plasma proteins. The oral bioavailability of spironolactone varies from 60 to 90%, while that of eplerenone is about 69%. Eplerenone undergoes a hepatic metabolism as well, but there are no active metabolites and is 50% bound to albumin in the serum, and about 67% is excreted in the urine while 32% passes through the feces. Food intake does not interfere with the absorption of these drugs, and taking it with food can, in effect, reduce gastric irritation and adverse symptoms associated with it.[105][106] Dosage for the most common indications of the individual PSDs appear in Table 4.[94][95][11][107][14]
- Carbonic-anhydrase Inhibitors and Osmotic Diuretics
Acetazolamide, the only diuretic CAI, is well absorbed from the GI tract, not metabolized, and is 93% protein-bound in the plasma. The onset of action of the oral form is 1 to 1.5 h with an oral bioavailability of almost 100%. It has a plasma half-life of 13 hours, and twice-daily dosing is recommended. Almost 90% of the drug is excreted in the urine by tubular secretion and is ineffective in renal insufficiency.[108][109]
Mannitol is poorly absorbed when given orally, and hence it is administered only via intravenous route as a bolus and hence has a bioavailability of 100%. Once in the plasma, mannitol, being an osmotic substance, draws fluid into the plasma, decreasing the blood viscosity and thereby the hematocrit. Mannitol is freely filtered with limited reabsorption, and it undergoes only slight metabolism in the liver to glycogen. The majority of the rest (more than 90%) is excreted unchanged in the urine, with an elimination half-life reported from 70 to 150 minutes.[79][110][111] Dosage for the most common indications of the individual CAIs and osmotic diuretics appear in Table 5.[50][11][112][113][37][114]
Adverse Effects
General Adverse Effects
The most common adverse effect for any diuretic is mild hypovolemia, which can lead to transient dehydration and increased thirst. When there is an over-treatment with a diuretic, this could lead to severe hypovolemia, causing hypotension, dizziness, and syncope. More generalized side-effects of diuretic agents include headache, urinary frequency, restlessness, weakness, fatigue, and lethargy. GI disturbances like nausea, vomiting, constipation, diarrhea, anorexia and abdominal pain can occur with loop diuretics and PSDs than any other diuretic group.
Electrolyte abnormalities are commonly associated with all the diuretic agents, and their mechanisms of such effect are well-established, and these mechanisms are explained under the respective class of diuretics below. To give a broader picture, hypokalemia, for example, is caused by all the diuretics except PSDs, which causes hyperkalemia. Acid-base disorders usually accompany the electrolyte derangement due to their close association with their reabsorption in the renal tubules. Metabolic disturbances can lead to derangement of glucose, uric acid, or lipid levels with certain diuretics and are individually discussed. Other rare adverse effects include impotence, hyperglycemic hyperosmolar non-ketotic syndrome, skin reactions, aplastic anemia, thrombocytopenia, agranulocytosis, hemolytic anemia, muscle cramps, and myalgia. In general, adverse effects are dose-dependent and are higher with loop diuretics as they have the most significant diuretic effect. With controlled low-dose formulations, adverse effects have reduced substantially, especially with thiazide diuretics.[115][116][117][118]
Loop Diuretic-specific Effects
- Hypokalemia and metabolic alkalosis can occur with both loop and thiazide diuretics but more common with loop diuretics. Loop agents increase distal Na+ delivery at macula densa and cause volume depletion, both of which indirectly activate the RAAS pathway. Aldosterone thus produced, which causes aggressive Na+ reabsorption leading to a negatively charged lumen and causing trapping of K+ and H+ ions in the lumen and eventually causing hypokalemia and metabolic alkalosis, similar to Conn syndrome. Increased distal Ca2+ delivered by loop agents may decrease the severity of hypokalemia but inhibiting K+ secretion indirectly by blocking ENaCs.[119] Contraction alkalosis can result from the rapid loss of large volumes of sodium-rich, bicarbonate-low extracellular fluid from the body; high-ceiling loop diuretics most commonly cause this.[120]
- Hypocalcemia and hypomagnesemia: Blocking NKCC2 function leads to suppression of ROMK-mediated K+ recycling into the lumen, which leaves a decreased transepithelial voltage (with a less positive luminal charge). This reduced luminal positivity reduces the driving force required for Ca2+ and Mg2+ reabsorption via the paracellular pathway, causing (see above) hypocalcemia and hypomagnesemia.[121] Despite the popular belief about hypomagnesemia caused by loop agents, a recent cohort study has concluded that thiazides but not loop diuretics are associated with the risk of hypomagnesemia.[122]
- Hyperuricemia: Both loop and thiazide diuretics are anions that are secreted in exchange for urate molecules via the OATs leading to urate reabsorption and hence hyperuricemia. Thus these diuretics are associated with an increased risk of gouty attacks.[123] Of note, probenecid, a uricosuric agent used in gout, competes with urate to bind OATs leading to urate excretion.
- Hypertriglyceridemia and Hypercholesterolemia: Loop diuretics can increase the levels of low-density lipoprotein cholesterol (LDL-C) and triglycerides (TG) levels, but the mechanism for this remains unclear.[124]
- Hypochloremia is associated with increased fractional excretion of Cl- relative to that of Na+.[125]
- Ototoxicity is a specific adverse effect of loop agents not shared by any other diuretic, and it manifests as sensory neural hearing loss, tinnitus, vertigo, or dizziness.[126] Mechanism discussed further under toxicity.
- Hypersensitivity reactions: Furosemide can cause hypersensitivity reactions such as skin rashes or acute interstitial nephritis. Reports also exist of more severe anaphylactic reactions.[127][54]
- Stevens-Johnson syndrome: Loop diuretics have implications as a rare cause of Stevens-Johnson syndrome.[128][129]
- Other less common adverse effects of loop diuretics include photosensitivity, nausea, and allergic interstitial nephritis.[130] Loop diuretics, especially furosemide and bumetanide, can displace bilirubin from albumin and cause hyperbilirubinemia leading to an increased risk of kernicterus in jaundiced neonates.[131] Furosemide, rarely, can cause aplastic anemia and agranulocytosis.[132]
Thiazide-specific Effects
Electrolyte abnormalities are the most common adverse effects associated with chronic thiazide therapy in hypertension. They occur most commonly with longer-acting agents such as chlorthalidone and metolazone, but this is mitigated to an extent with a low-dose strategy.
- Hypokalemia and metabolic alkalosis: Thiazides can cause RAAS activation only via volume depletion (see above) as they act on NCC channels located distal to the macula densa and do not influence salt-sensors located there. Aldosterone from the RAAS pathway enhances the excretion of K+ and H+ in the tubules, as explained above. Also, thiazides cause decreased distal Ca2+ delivery, which stimulates ENaCs leading to increased K+ secretion, thereby contributing to hypokalemia.[69][119] They usually respond to K+ replacement therapy very well.
- Hyponatremia: Even though loop diuretics suppresses a greater load of Na+ reabsorption than other agents, hyponatremia most often results from thiazides because thiazides lead to reduced free-water clearance and they do not interfere with urine concentrating ability (countercurrent pathway) when compared to loop agents. Furthermore, increased water intake and increased vasopressin secretion contribute to dilutional hyponatremia.[133]
- Hypercalcemia/hypocalciuria Volume depletion by thiazides causes enhanced Na+ reabsorption in the PTs, which in turn stimulates increased passive Ca2+ reabsorption via paracellular pathway there, a proximal response. As a distal response, inhibition of NCC channels by thiazides could play a role in enhancing Ca2+ reabsorption by modulating the activity of TRP vanilloid-5 channels.[134][135]
- Hypomagnesemia also correlates with the chronic use of thiazides and is mediated through thiazide-mediated inhibition of NCC channels, which indirectly inhibits Mg2+ reabsorption via downregulating TRP melastatin-6 channels.[122] Of note, a proton pump inhibitor also mediates hypomagnesemia via the same channels in both gastrointestinal (GI) and renal tubules.[136]
- Glucose intolerance: Thiazide-induced hypokalemia in pancreatic interstitium hyperpolarizes the islet cells, thereby inhibiting calcium influx and thus decreasing the calcium-dependent release of insulin resulting in hyperglycemia. Thiazides also cause an increase in the inflammatory response, abnormal lipid metabolism, RAAS activation, and oxidative stress, thus decreased insulin sensitivity that arises as a consequence is multifactorial. New-onset diabetes due to thiazides is also of concern in obese and hypertensive individuals.[137][69][138]
- Hyperuricemia: The incidence of this adverse effect increases with the number of years using thiazides for hypertensive therapy.[139]
- Hypertriglyceridemia and Hypercholesterolemia: Thiazides, while not affecting high-density lipoproteins, have been shown to increase LDL-C levels by 10%, total cholesterol by 4%, and TG levels by almost 15%. There is evidence on the dose-dependency of this side-effect and reduced occurrence with low-dose therapy.[124].
- Stevens-Johnson syndrome: Thiazides, like loop diuretics, are also implicated as a rare cause of Stevens-Johnson syndrome [128][129]
- Rarely Thiazides can increase the risk of developing acute pancreatitis owing to increased serum calcium levels.[140] Thiazides, rarely, have also been implicated in drug-induced hematological abnormalities, including thrombocytopenia and agranulocytosis.[141] Orthostatic hypotension and impotence are other side-effects of thiazide use.
Potassium-sparing Diuretic Specific Effects
More generalized and less common side-effects of K+-sparing agents include headache, fatigue, and GI disturbances like nausea, vomiting, constipation, diarrhea, anorexia, and abdominal pain.
ENaC Inhibitor Specific Effects
- Hyperkalemia and hyperchloremic metabolic acidosis are the most common side-effect of this class of diuretics due to their inhibition of ENaCs and, consequently, suppressed secretion of K+ ions and H+ ions from the ASDN.[142] This action results in hyperkalemia, and as with CAIs, the metabolic acidosis thus produced is hyperchloremic but via a different initial mechanism. Hyperkalemia produced by these K+-sparing diuretics can lead to impaired PT ammonia generation and reduced collecting duct ammonia transport resulting in impaired ammonia excretion. The HCO3+ in the blood reacts with excess ammonia to buffer the pH while getting used up in the process leading to reduced HCO3+ levels. The reduced serum HCO3+ causes lead to shifting of Cl- ions to the plasma from the cells leading to hyperchloremic metabolic acidosis.[143][144][145]
- Amiloride carries a black-box warning for hyperkalemia. Nausea, flatulence, and skin rashes can occur with amiloride or triamterene. Rarely, nephrolithiasis can result from triamterene use.[146]
Aldosterone Receptor Antagonist Specific Effects
- Side-effects of this category are attributed to spironolactone and are dose-dependent in most situations and can include menstrual irregularities, breast tenderness, and orthostatic hypotension.[147]
- Gynecomastia: Spironolactone is a non-selective ARA and is structurally similar to progesterone and results in progestogenic and anti-androgenic effects, which block both the production of androgens such as testosterone and their binding to their androgenic receptors. Such a decrease in androgens decreases the androgen to estrogen ratio, opening the way for estrogens to exert their unrestrained action causing gynecomastia.[148] Thus drugs affecting this ratio, such as tamoxifen, danazol, and letrozole, are the mainstay of medical therapy of this condition.[149] Eplerenone is more selective for MR and does not cause gynecomastia. Decreased libido and galactorrhoea are other anti-androgenic side-effects associated with spironolactone.
Carbonic Anhydrase Inhibitor Specific Effects
- Hyperchloremic metabolic acidosis: Acetazolamide most commonly cause symptomatic metabolic acidosis. The majority of HCO3+ ions are reabsorbed in the PT with the help of carbonic anhydrase enzyme, and inhibition of this enzyme by acetazolamide causes wastage of HCO3+ ions in the urine (bicarbonaturia). This activity leads to reduced serum HCO3+ levels, and intracellular Cl- ions are then released into the plasma to compensate for the loss of negative charge causing normal anion gap metabolic acidosis, aka hyperchloremic metabolic acidosis. Chronic use of acetazolamide is not warranted due to this side-effect.[150][151]
- Hypokalemia: is due to increased distal delivery of Na+ ions and their reabsorption in exchange for K+ ions.
- Fanconi syndrome: Inhibition of HCO3+ ions also cause type-2 proximal renal tubular acidosis, which can cause PT dysfunction leading to drug-induced Fanconi syndrome.[150]
- Other less common side effects include Light-headedness, circumoral paresthesias, weakness, and confusion.
Osmotic Diuretic Specific Effects
- Electrolyte abnormalities: Though mannitol does not interfere with electrolyte reabsorptive mechanisms, it can cause inhibition of water transport, and this diminishes the ability of renal tubules to reabsorb Na+ ions, which can cause hyponatremia. Increased distal delivery of Na+ ions can lead to K+ loss as described above and thus hypokalemia. As it causes increased serum osmolality, mannitol causes a shift of water from the intracellular compartment to the plasma, leading to an increase in blood volume, which can further result in dilutional hyponatremia and hypokalemia.[79]
- Mannitol-induced overt expansion of extracellular fluid volume can precipitate pulmonary edema in HF patients due to hypervolemia.[152] With frequent use, mannitol sometimes can worsen cerebral edema as it can cross the already damaged blood-brain barrier (as in intracranial hemorrhage) and draws water into the brain. Mannitol less commonly can form precipitates at low temperatures, which can cause vascular and end-organ damage. Other adverse effects include nausea, vomiting, fever, confusion, and a lethargic state.[37]
Contraindications
Severe dehydration or established anuria is a contraindication for any type of diuretic. Patients with known hypersensitivity to any of the diuretic agents are contraindicated to receive the same drug. Diuretics are contraindicated in severe electrolyte derangement and should not be administered until a detected electrolyte abnormality is corrected.
Loop and thiazide diuretics are contraindicated in patients already diagnosed with gout.[153]
Loop diuretics (except ethacrynic acid), thiazide diuretics, and CAIs are all sulfonamide derivatives and were generally regarded as contraindicated in sulfa-allergy patients. Recent evidence suggests otherwise, and several reports of instances of uneventful use of sulfa-diuretic use in documented sulfa-allergy patients exist. In conclusion, only a low risk of cross-allergenicity between sulfonamide antibiotics and sulfonamide non-antibiotics and diuretics can be prescribed with caution in sulfa-allergic patients. Notwithstanding, documented allergy to any of the sulfonamide diuretic agents themselves should be considered an absolute contraindication, and for sulfonamide non-antibiotics, it is a relative contraindication.[154][155][156][157]
Loop diuretics are contraindicated in patients with hypokalemia (only to be administered after correction), severe hyponatremia, hypotension, azotemia, oliguria/anuria, and hepatic coma. It is also contraindicated in any situation where fluid depletion is foreseen, such as surgery. Furosemide and bumetanide are pregnancy category C, while torsemide is category B and relatively safe in pregnancy.
Thiazide diuretics induce hyperglycemia, but are these agents contraindicated in hypertensive patients for the risk of new-onset diabetes or worsening of preexisting diabetes? Thiazides are of crucial importance as first-line therapy in patients with hypertension, a condition treated primarily to reduce the high risk of CV mortality. To compare the two important drugs in this class, chlorthalidone (thiazide-like diuretic) has demonstrated superiority to hydrochlorothiazide (thiazide-type diuretic) in reducing systolic BP levels and in achieving target BP values. Also, in comparison to other anti-hypertensives, chlorthalidone has been repeatedly shown in various clinical trials to greatly reduce the risk of adverse CV events. Also, chlorthalidone has been shown to cause the fewest clinical events of diabetes in contrast to any other anti-hypertensive. In a hypertensive population with preexisting diabetes, the salutary anti-hypertensive effects of low-dose (12.5 mg) chlorthalidone outweigh the risk of glucose intolerance and will particularly benefit young non-obese patients. The 2018 ESC guidelines on hypertension give the highest class I recommendation for the use of thiazide/thiazide-like diuretics along with a RAS blocker in the treatment of diabetics with hypertension.[25][23][158][159][160]
Guidelines advised against the use of thiazides in patients with severe stage 4 or stage 5 CKD (see Table 2), though recent reports are in favor of its use as anti-hypertensive (even if GFR less than 30 mL/min) as the BP-lowering mechanism of thiazides are not related to their diuretic function in the kidney. Nevertheless, thiazides are contraindicated when the diuresis is the predominant action required in patients with CKD, where loop diuretics are preferred. The only exception is metolazone, a thiazide diuretic that can be used for diuresis in CKD.[100][161]
K+-sparing diuretics are contraindicated in hyperkalemia (K+ levels more than 5 mEq/L) until the underlying pathology is corrected. PSDs are contraindicated in advanced renal failure or CKD as these patients are at risk of hyperkalemia; this is particularly true when GFR <30 mL/min/1.73 m^2 corresponding to CKD stages 4 and 5.[162][93] Spironolactone is pregnancy category C, and along with triamterene, should be avoided in pregnancy, while eplerenone is a category B medication.[163]
In hyperchloremic metabolic acidosis (see adverse effects), acetazolamide is contraindicated, and extreme caution should be exercised in severe chronic obstructive pulmonary disease when considering acetazolamide for treatment.[164]
The kidneys primarily excrete mannitol, and in patients with renal impairment, it should be used with caution as it can cause osmotic nephropathy.[111] Intravascular volume overload due to mannitol may be of concern in cardiac and renal failure patients and are hence contraindicated in such patients. Mannitol should not be used in patients with active cranial bleeding, severe dehydration, and in patients with hypersensitivity history to its use. When using mannitol in treating patients with anuria, it requires an initial test dose to verify the diuretic response.[165]
Drug-interactions
Salicylates can displace acetazolamide from plasma protein, thereby causing an increase in free acetazolamide in the plasma leading to toxicity secondary to RBC carbonic anhydrase inhibition. Acetazolamide should not be used to alkalinize urine following salicylate overdose since it may worsen metabolic acidosis.[166][167][168]
Prostaglandins are involved in the modulation of systemic and renal vasodilation, GFR, RAAS, water, and salt secretion. Their blockade by nonsteroidal anti-inflammatory drugs (NSAIDs) in a patient with hypertension could suppress the effects of antihypertensive medications, including diuretics. NSAIDs are not very influential in regulating renal functions under normal circumstances, but they can blunt the natriuretic response, reduce GFR and suppress renin production when used along with loop or thiazide diuretics and can cause acute renal failure.[169][170]
The ototoxic ability of loop diuretics can become potentiated with other ototoxic drugs such as aminoglycosides or platinum-containing chemotherapeutic compounds.[126]
Diuretic-induced hypokalemia can increase the risk of digitalis-induced arrhythmia.[163] Digoxin competes with K+ ions for its binding site on the Na+-K+-ATPase pump in the heart, and thus in diuretic-induced hypokalemia, the action of digoxin is unopposed, leading to fatal arrhythmias.[171] Although any diuretic causing hypokalemia can lead to this effect, loop diuretics carry the greatest risk when compared to other classes of diuretics, but as an individual agent, hydrochlorothiazide had the greatest risk.[172] Hence the combination of hypokalemia-inducible diuretics and digoxin can be dangerous and must be avoided. Similarly, clinicians must avoid using quinidine because thiazide-induced hypokalemia can potentiate its cardiovascular effects.[173]
Bendroflumethiazide can cause calcium retention, and care is necessary when administered along with calcium supplements or vitamin D.[174] Thiazides can cause lithium accumulation when the drugs are co-administered as they can increase lithium reabsorption in the PT.[175]
RAAS inhibiting agents like ACEIs, ARBs, beta-blockers, NSAIDs, or aliskiren can result in a small amount of potassium retention, and their concomitant use with PSDs may cause hyperkalemia and hence a relative contraindication.[115] PSDs apparently must not be administered along with another PSD to avoid the risk of dangerous hyperkalemia.
Monitoring
Diuretic treatment calls for careful assessment of extracellular fluid volume, urine output, electrolyte levels in plasma and urine, body weight, acid-base status, serum glucose, and BP regularly with particular emphasis on patients with cardiovascular, hepatic, renal, or metabolic disorders and in elderly individuals. Prerenal azotemia is of concern due to diuretic-induced hypovolemia, and blood urea nitrogen and creatinine levels require monitoring.
Ototoxicity is a risk with the use of loop diuretics, and special precautions are necessary. Baseline auditory tests are necessary (especially when planning large bolus doses at high infusion rates), which will help evaluate on a case-by-case basis the effect of loop diuretics on auditory functions after a certain length of treatment. Periodic sequential monitoring of auditory functions is also advisable, and the possibility of switching to a different diuretic therapy should be contemplated in case of any adverse outcomes.[126]
Clinical cardiac status should be assessed in patients on diuretics (especially MI, HF, or other cardiac conditions), as they are prone to develop HF due to the abrupt increase in the fluid shift between the compartments.
Failure of a diuretic agent to increase urine output should prompt cessation of the diuretic agent as it could be evidence of undiagnosed underlying renal pathology.
Frequent administration of mannitol can worsen cerebral edema and hence should be administered every 6 to 8 hours, as suggested in Table 4.
Diuretic Abuse
Diuretics are not highly controlled drugs and hence have a high probability for misuse, particularly with athletes who might abuse them for rapid weight loss or to conceal the presence of other banned drugs. The use of diuretics is prohibited in athletes. (Athletes require a prior exemption for therapeutic use in athletes) and is routinely screened for by the world anti-doping agency. If it persists chronically, such abuse can lead to detrimental effects on CV and thermoregulatory functions, which could lead to death when combined with excessive physical activity as encountered in athletes.[176] People with bulimia nervosa can misuse diuretics (when they try to purge the food), and such use can lead to pseudo-Bartter syndrome.[177] Psychotic patients also can abuse diuretics, along with laxatives [178].
Diuretics in Diagnosis
- Furosemide/Fludrocortisone test (FFT): Furosemide, combined with the mineralocorticoid fludrocortisone, has gained popularity as a diagnostic screening tool for distal renal tubular acidosis (dRTA). dRTA is a condition where there is a defect in urinary acidification due to the failure of alpha-intercalated cells to secrete H+ ions in the distal tubules (refer to the mechanism of action of PSDs). There are four different types of dRTA, usually diagnosed by ammonium chloride (NH4Cl) loading test, but due to disturbing GI symptoms after administration, the test is sometimes abandoned. NH4Cl combines with HCO3+ ions to form urea in the liver, thus decreasing the HCO3+ levels in the blood stressing the kidneys to reabsorb more HCO3+ ions in exchange for H+ ions, thus acidifying the urine. In patients with dRTA, this test can lead to systemic metabolic acidosis as kidneys cannot reabsorb HCO3+ ions due to H+ ion secretion defect. If the urine pH is greater than 5.3, then the test is considered positive for dRTA. FFT is a palatable alternative that is better tolerated. Furosemide increases the distal delivery of Na+ ions, and fludrocortisone being a mineralocorticoid, enhances the Na+ reabsorption via ENaCs and increases H+ ion secretion via the alpha-intercalated cells. This combination thus can acidify the urine without the metabolic acidosis induced by NH4Cl. In people without dRTA, the urine pH is lower than 5.3 with FFT, whereas patients with dRTA cannot lower their pH leading to its diagnosis.[179][180][181]
- Mannitol challenge test (MCT): Mannitol can be an agent in a challenge test in the diagnosis of asthma. In this test, dry powder of mannitol is inhaled, which leads to hyperosmolality of bronchial periciliary liquid inducing cell shrinkage to equilibrate the osmolality. This further results in the release of pro-inflammatory mediators from inflammatory cells (particularly mast cells), resulting in smooth muscle constriction. A 15% decrease in forced expiratory volume in the first second (FEV1) is a positive result, suggesting an easily elicited active airway inflammation, indicating airway hyperresponsiveness. Though MCT is a very safe test, it has only a moderate sensitivity to detect asthma but high specificity. In comparison, direct bronchial challenge tests such as histamine or methacholine challenge tests have less specificity when compared to MCT.[182]
Toxicity
Reversible ototoxicity (manifested as sensory neural hearing loss, tinnitus) can be caused by ischemia in stria vascularis and by inhibiting NKCC1 channels in stria vascularis by loop diuretics, which improves with discontinuation of the drug. Deafness and tinnitus from loop diuretics most frequently occur when administering large bolus doses in an acute setting, such as when using furosemide in acute kidney injury. The resulting ototoxicity is, therefore, due to the higher serum concentrations of the drug achieved. Ethacrynic acid is the most ototoxic drug in this group.[183][57][184]
There are reports of hydrochlorothiazide, furosemide, spironolactone, and triamterene, causing hepatotoxicity, but there is no suggestion of diuretic class effect.[185][186][187]
Diuretic-induced kidney injury has been reported, and it is most severe in elderly patients due to their decreased sensitivity of thirst response. Diuretics are also associated with increased risk when the renal blood flow is compromised in conditions such as congestive heart failure, hepatic cirrhosis, and nephrotic syndrome and can cause acute renal failure. Dose dependency also plays a factor as higher diuretic doses are associated with pathological injury of the glomerular basement membrane. Diuretics can lead to vacuolar degeneration of tubular epithelial cells, and hence their use with other nephrotoxic drugs should be contraindicated.[188]
Enhancing Healthcare Team Outcomes
Diuretic therapy, while typically well-tolerated, requires the comprehensive effort of an interprofessional medical team, including clinicians, specialists, NPs and PAs, nurses, and pharmacists. Patient education plays a crucial role and adequate knowledge of the adverse effects, dietary, and lifestyle modifications necessary while on diuretics. Patients (especially in an outpatient setting) must understand to report any changes in their compliance pattern or any adverse effect thereof. Adherence to strict treatment protocols and timely intake of the drug, and avoiding any overdosing when the patients miss their dosing will significantly improve the clinical course and the effectiveness of the diuretic agent.
Nurses, as immediate caregivers, should be cognizant of the adverse effects of diuretics and should be able to alert the treating clinician if a patient’s condition worsens. This situation is particularly true in hospitalized patients in intensive care units where updating urine output charts, daily body weight measurements, and periodic arterial blood gas analysis ensures patient safety. Pharmacists play an essential role in an outpatient setting and should be vigilant to check any drug-drug interactions or incorrect dosage in the prescriptions. Diuretics are prescription-only drugs, and any over-the-counter request of these drugs should be refused and, if needed, be reported to avoid damage to health by suspected misusers of diuretics. Several health professionals, including clinicians and specialists like cardiologists, otorhinolaryngologists, plus clinical pharmacists, nurses, and other healthcare workers, form part of the interprofessional team to operate in collaboration to avert any adverse outcome with diuretic therapy.[189] [Level 5]
Media
(Click Image to Enlarge)
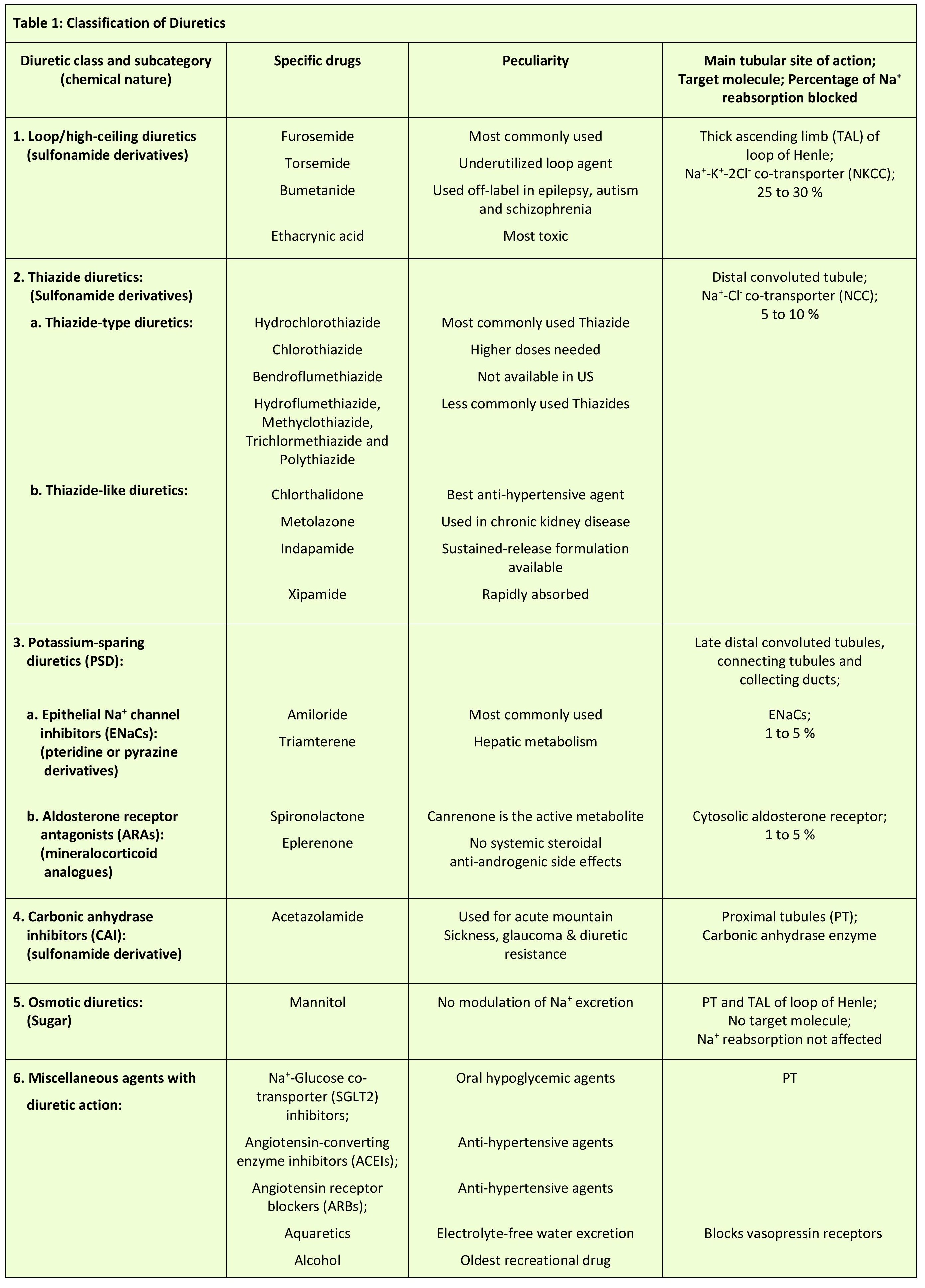
Table 1: Classification of diuretic agents Created and Contributed by Vijay Arumugham, MD, PhD
(Click Image to Enlarge)

Table 2: Dosages for specific indications of Loop diuretics Created and Contributed by Vijay Arumugham, MD, PhD
(Click Image to Enlarge)

Table 3: Dosages for specific indications of thiazide diuretics Created and Contributed by Vijay Arumugham, MD, PhD
(Click Image to Enlarge)
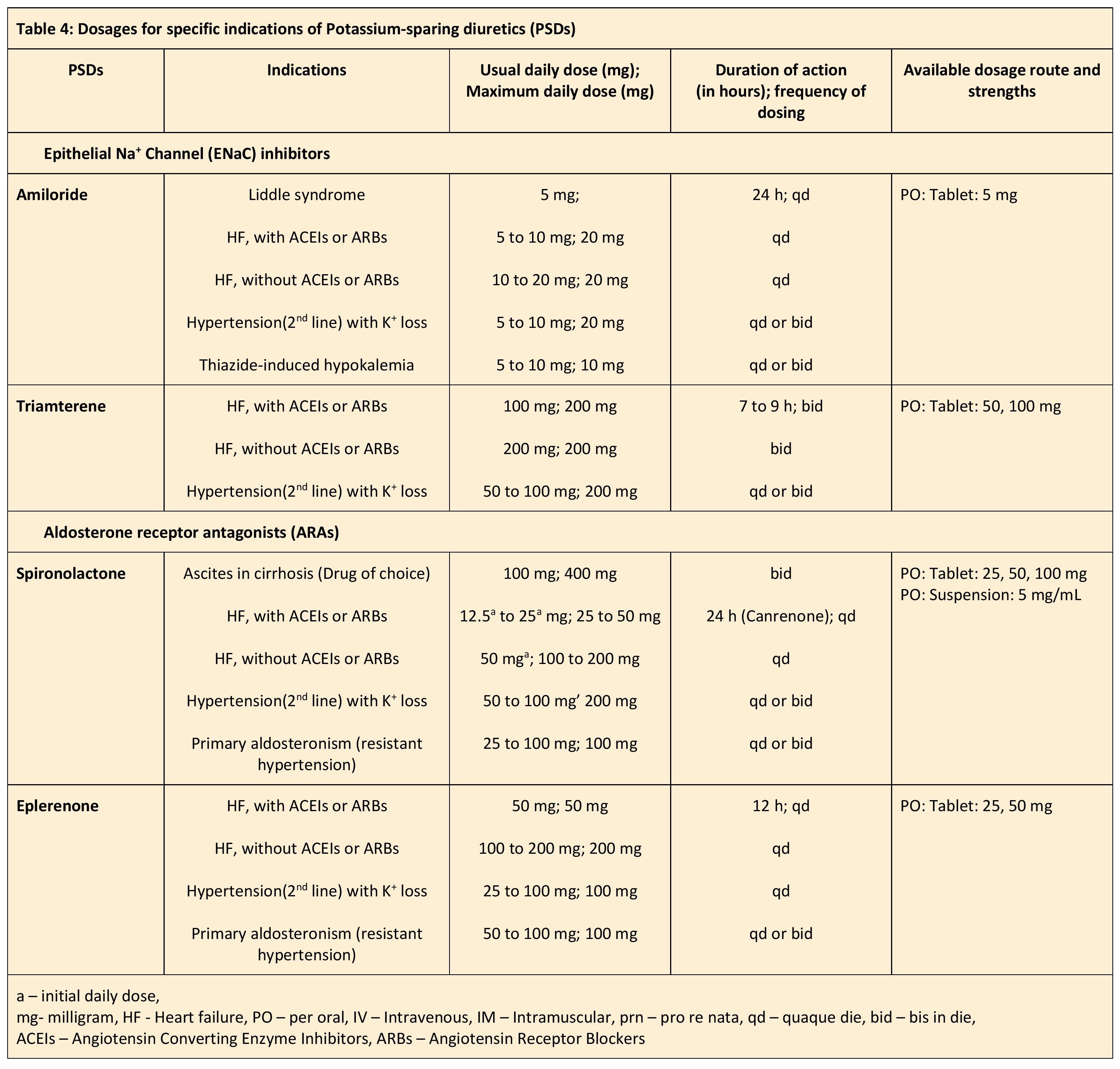
Table 4: Dosages for specific indications of potassium-sparing diuretics Created and Contributed by Vijay Arumugham, MD, PhD
(Click Image to Enlarge)
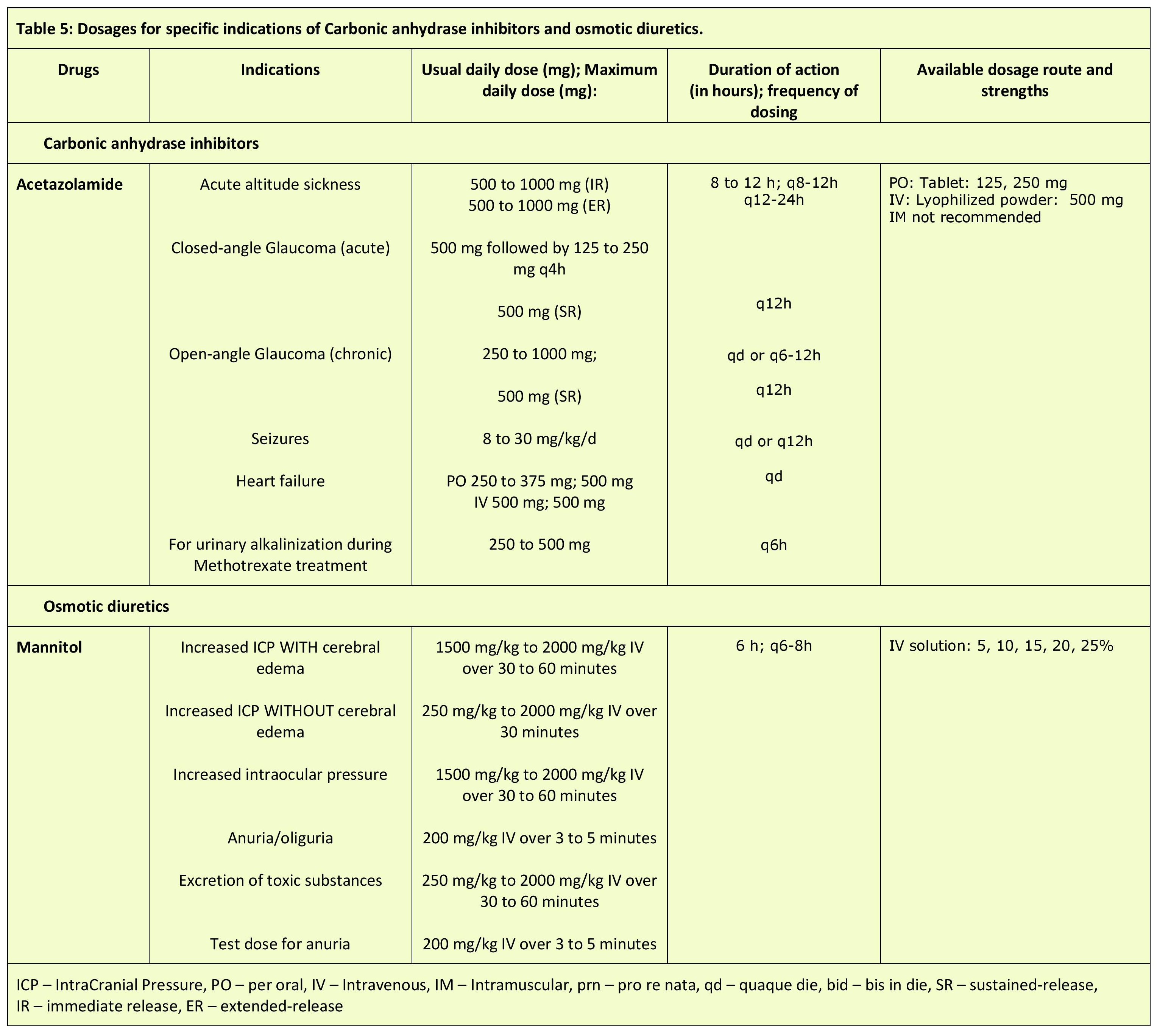
Table 5: Dosages for specific indications of carbonic anhydrase inhibitors and osmotic diuretics Created and Contributed by Vijay Arumugham, MD, PhD
References
Popkin BM, D'Anci KE, Rosenberg IH. Water, hydration, and health. Nutrition reviews. 2010 Aug:68(8):439-58. doi: 10.1111/j.1753-4887.2010.00304.x. Epub [PubMed PMID: 20646222]
Roumelioti ME, Glew RH, Khitan ZJ, Rondon-Berrios H, Argyropoulos CP, Malhotra D, Raj DS, Agaba EI, Rohrscheib M, Murata GH, Shapiro JI, Tzamaloukas AH. Fluid balance concepts in medicine: Principles and practice. World journal of nephrology. 2018 Jan 6:7(1):1-28. doi: 10.5527/wjn.v7.i1.1. Epub [PubMed PMID: 29359117]
Jéquier E, Constant F. Water as an essential nutrient: the physiological basis of hydration. European journal of clinical nutrition. 2010 Feb:64(2):115-23. doi: 10.1038/ejcn.2009.111. Epub 2009 Sep 2 [PubMed PMID: 19724292]
Wile D. Diuretics: a review. Annals of clinical biochemistry. 2012 Sep:49(Pt 5):419-31. doi: 10.1258/acb.2011.011281. Epub 2012 Jul 10 [PubMed PMID: 22783025]
Donato V, Lacquaniti A, Cernaro V, Lorenzano G, Trimboli D, Buemi A, Lupica R, Buemi M. From water to aquaretics: a legendary route. Cellular physiology and biochemistry : international journal of experimental cellular physiology, biochemistry, and pharmacology. 2014:33(5):1369-88. doi: 10.1159/000358704. Epub 2014 May 5 [PubMed PMID: 24853354]
Level 3 (low-level) evidenceKharod SC, Kang SK, Kadam SD. Off-Label Use of Bumetanide for Brain Disorders: An Overview. Frontiers in neuroscience. 2019:13():310. doi: 10.3389/fnins.2019.00310. Epub 2019 Apr 24 [PubMed PMID: 31068771]
Level 3 (low-level) evidenceHuxel C, Raja A, Ollivierre-Lawrence MD. Loop Diuretics. StatPearls. 2024 Jan:(): [PubMed PMID: 31536262]
Akbari P, Khorasani-Zadeh A. Thiazide Diuretics. StatPearls. 2024 Jan:(): [PubMed PMID: 30422513]
Miller WL. Fluid Volume Overload and Congestion in Heart Failure: Time to Reconsider Pathophysiology and How Volume Is Assessed. Circulation. Heart failure. 2016 Aug:9(8):e002922. doi: 10.1161/CIRCHEARTFAILURE.115.002922. Epub [PubMed PMID: 27436837]
Sica DA, Gehr TWB, Frishman WH. Use of Diuretics in the Treatment of Heart Failure in Older Adults. Heart failure clinics. 2017 Jul:13(3):503-512. doi: 10.1016/j.hfc.2017.02.006. Epub [PubMed PMID: 28602368]
Mullens W, Damman K, Harjola VP, Mebazaa A, Brunner-La Rocca HP, Martens P, Testani JM, Tang WHW, Orso F, Rossignol P, Metra M, Filippatos G, Seferovic PM, Ruschitzka F, Coats AJ. The use of diuretics in heart failure with congestion - a position statement from the Heart Failure Association of the European Society of Cardiology. European journal of heart failure. 2019 Feb:21(2):137-155. doi: 10.1002/ejhf.1369. Epub 2019 Jan 1 [PubMed PMID: 30600580]
Shah A, Gandhi D, Srivastava S, Shah KJ, Mansukhani R. Heart Failure: A Class Review of Pharmacotherapy. P & T : a peer-reviewed journal for formulary management. 2017 Jul:42(7):464-472 [PubMed PMID: 28674474]
Haberl J, Zollner G, Fickert P, Stadlbauer V. To salt or not to salt?-That is the question in cirrhosis. Liver international : official journal of the International Association for the Study of the Liver. 2018 Jul:38(7):1148-1159. doi: 10.1111/liv.13750. Epub 2018 May 16 [PubMed PMID: 29608812]
Moore KP, Aithal GP. Guidelines on the management of ascites in cirrhosis. Gut. 2006 Oct:55 Suppl 6(Suppl 6):vi1-12 [PubMed PMID: 16966752]
Garbuzenko DV, Arefyev NO. Current approaches to the management of patients with cirrhotic ascites. World journal of gastroenterology. 2019 Jul 28:25(28):3738-3752. doi: 10.3748/wjg.v25.i28.3738. Epub [PubMed PMID: 31391769]
Udani SM, Koyner JL. The effects of heart failure on renal function. Cardiology clinics. 2010 Aug:28(3):453-65. doi: 10.1016/j.ccl.2010.04.004. Epub [PubMed PMID: 20621250]
Level 3 (low-level) evidenceHartleb M, Gutkowski K. Kidneys in chronic liver diseases. World journal of gastroenterology. 2012 Jun 28:18(24):3035-49. doi: 10.3748/wjg.v18.i24.3035. Epub [PubMed PMID: 22791939]
Sica DA. Diuretic use in renal disease. Nature reviews. Nephrology. 2011 Dec 20:8(2):100-9. doi: 10.1038/nrneph.2011.175. Epub 2011 Dec 20 [PubMed PMID: 22183505]
Khan YH, Sarriff A, Adnan AS, Khan AH, Mallhi TH. Chronic Kidney Disease, Fluid Overload and Diuretics: A Complicated Triangle. PloS one. 2016:11(7):e0159335. doi: 10.1371/journal.pone.0159335. Epub 2016 Jul 21 [PubMed PMID: 27442587]
Gupta S, Pepper RJ, Ashman N, Walsh SB. Nephrotic Syndrome: Oedema Formation and Its Treatment With Diuretics. Frontiers in physiology. 2018:9():1868. doi: 10.3389/fphys.2018.01868. Epub 2019 Jan 15 [PubMed PMID: 30697163]
Kitsios GD, Mascari P, Ettunsi R, Gray AW. Co-administration of furosemide with albumin for overcoming diuretic resistance in patients with hypoalbuminemia: a meta-analysis. Journal of critical care. 2014 Apr:29(2):253-9. doi: 10.1016/j.jcrc.2013.10.004. Epub 2013 Oct 22 [PubMed PMID: 24268626]
Level 1 (high-level) evidenceMubarik A, Anastasopoulou C, Aeddula NR. Liddle Syndrome (Pseudohyperaldosteronism). StatPearls. 2024 Jan:(): [PubMed PMID: 30725596]
Wright JM, Musini VM, Gill R. First-line drugs for hypertension. The Cochrane database of systematic reviews. 2018 Apr 18:4(4):CD001841. doi: 10.1002/14651858.CD001841.pub3. Epub 2018 Apr 18 [PubMed PMID: 29667175]
Level 1 (high-level) evidenceWhelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2018 May 15:71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006. Epub 2017 Nov 13 [PubMed PMID: 29146535]
Level 3 (low-level) evidenceScheen AJ. Type 2 Diabetes and Thiazide Diuretics. Current diabetes reports. 2018 Feb 5:18(2):6. doi: 10.1007/s11892-018-0976-6. Epub 2018 Feb 5 [PubMed PMID: 29399724]
McNally RJ, Morselli F, Farukh B, Chowienczyk PJ, Faconti L. A review of the prescribing trend of thiazide-type and thiazide-like diuretics in hypertension: A UK perspective. British journal of clinical pharmacology. 2019 Dec:85(12):2707-2713. doi: 10.1111/bcp.14109. Epub 2019 Dec 9 [PubMed PMID: 31471972]
Level 3 (low-level) evidenceBlowey DL. Diuretics in the treatment of hypertension. Pediatric nephrology (Berlin, Germany). 2016 Dec:31(12):2223-2233 [PubMed PMID: 26983630]
Mishra S. Diuretics in primary hypertension - Reloaded. Indian heart journal. 2016 Sep-Oct:68(5):720-723. doi: 10.1016/j.ihj.2016.08.013. Epub 2016 Sep 10 [PubMed PMID: 27773415]
Roush GC, Sica DA. Diuretics for Hypertension: A Review and Update. American journal of hypertension. 2016 Oct:29(10):1130-7. doi: 10.1093/ajh/hpw030. Epub 2016 Apr 5 [PubMed PMID: 27048970]
Vigen R, Weideman RA, Reilly RF. Thiazides diuretics in the treatment of nephrolithiasis: are we using them in an evidence-based fashion? International urology and nephrology. 2011 Sep:43(3):813-9. doi: 10.1007/s11255-010-9824-6. Epub 2010 Aug 25 [PubMed PMID: 20737209]
Carroll MF, Schade DS. A practical approach to hypercalcemia. American family physician. 2003 May 1:67(9):1959-66 [PubMed PMID: 12751658]
Loffing J. Paradoxical antidiuretic effect of thiazides in diabetes insipidus: another piece in the puzzle. Journal of the American Society of Nephrology : JASN. 2004 Nov:15(11):2948-50 [PubMed PMID: 15504949]
Level 3 (low-level) evidenceCRAWFORD JD, KENNEDY GC. Chlorothiazid in diabetes insipidus. Nature. 1959 Mar 28:183(4665):891-2 [PubMed PMID: 13644230]
Burtscher M, Gatterer H, Faulhaber M, Burtscher J. Acetazolamide pre-treatment before ascending to high altitudes: when to start? International journal of clinical and experimental medicine. 2014:7(11):4378-83 [PubMed PMID: 25550957]
Schmidl D, Schmetterer L, Garhöfer G, Popa-Cherecheanu A. Pharmacotherapy of glaucoma. Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2015 Mar:31(2):63-77. doi: 10.1089/jop.2014.0067. Epub 2015 Jan 14 [PubMed PMID: 25587905]
Level 3 (low-level) evidenceRosenbaum A, Winter M. Are diuretics effective for Ménière`s disease? Medwave. 2018 Mar 28:18(2):e7188. doi: 10.5867/medwave.2018.02.7187. Epub 2018 Mar 28 [PubMed PMID: 29624570]
Tenny S, Patel R, Thorell W. Mannitol. StatPearls. 2024 Jan:(): [PubMed PMID: 29262205]
Witherspoon B, Ashby NE. The Use of Mannitol and Hypertonic Saline Therapies in Patients with Elevated Intracranial Pressure: A Review of the Evidence. The Nursing clinics of North America. 2017 Jun:52(2):249-260. doi: 10.1016/j.cnur.2017.01.002. Epub 2017 Apr 7 [PubMed PMID: 28478873]
Ghannoum M, Gosselin S. Enhanced poison elimination in critical care. Advances in chronic kidney disease. 2013 Jan:20(1):94-101. doi: 10.1053/j.ackd.2012.09.002. Epub [PubMed PMID: 23265601]
Level 3 (low-level) evidencePrescott LF, Balali-Mood M, Critchley JA, Johnstone AF, Proudfoot AT. Diuresis or urinary alkalinisation for salicylate poisoning? British medical journal (Clinical research ed.). 1982 Nov 13:285(6352):1383-6 [PubMed PMID: 6291695]
Yasir M, Mechanic OJ. Syndrome of Inappropriate Antidiuretic Hormone Secretion. StatPearls. 2024 Jan:(): [PubMed PMID: 29939554]
Cannavo A, Bencivenga L, Liccardo D, Elia A, Marzano F, Gambino G, D'Amico ML, Perna C, Ferrara N, Rengo G, Paolocci N. Aldosterone and Mineralocorticoid Receptor System in Cardiovascular Physiology and Pathophysiology. Oxidative medicine and cellular longevity. 2018:2018():1204598. doi: 10.1155/2018/1204598. Epub 2018 Sep 19 [PubMed PMID: 30327709]
Pelis RM, Wright SH. Renal transport of organic anions and cations. Comprehensive Physiology. 2011 Oct:1(4):1795-835. doi: 10.1002/cphy.c100084. Epub [PubMed PMID: 23733689]
Level 3 (low-level) evidenceZhuo JL, Li XC. Proximal nephron. Comprehensive Physiology. 2013 Jul:3(3):1079-123. doi: 10.1002/cphy.c110061. Epub [PubMed PMID: 23897681]
Level 3 (low-level) evidenceRajkumar P, Pluznick JL. Acid-base regulation in the renal proximal tubules: using novel pH sensors to maintain homeostasis. American journal of physiology. Renal physiology. 2018 Nov 1:315(5):F1187-F1190. doi: 10.1152/ajprenal.00185.2018. Epub 2018 Aug 1 [PubMed PMID: 30066586]
Skelton LA, Boron WF, Zhou Y. Acid-base transport by the renal proximal tubule. Journal of nephrology. 2010 Nov-Dec:23 Suppl 16(0 16):S4-18 [PubMed PMID: 21170887]
Level 3 (low-level) evidenceHorita S, Nakamura M, Suzuki M, Satoh N, Suzuki A, Homma Y, Nangaku M. The role of renal proximal tubule transport in the regulation of blood pressure. Kidney research and clinical practice. 2017 Mar:36(1):12-21. doi: 10.23876/j.krcp.2017.36.1.12. Epub 2017 Mar 31 [PubMed PMID: 28428931]
DuBose TD Jr. Carbonic anhydrase-dependent bicarbonate transport in the kidney. Annals of the New York Academy of Sciences. 1984:429():528-37 [PubMed PMID: 6331260]
Level 3 (low-level) evidenceSarafidis PA, Georgianos PI, Lasaridis AN. Diuretics in clinical practice. Part I: mechanisms of action, pharmacological effects and clinical indications of diuretic compounds. Expert opinion on drug safety. 2010 Mar:9(2):243-57. doi: 10.1517/14740330903499240. Epub [PubMed PMID: 20095917]
Level 3 (low-level) evidenceFarzam K, Abdullah M. Acetazolamide. StatPearls. 2023 Jan:(): [PubMed PMID: 30335315]
Sands JM, Layton HE. The physiology of urinary concentration: an update. Seminars in nephrology. 2009 May:29(3):178-95. doi: 10.1016/j.semnephrol.2009.03.008. Epub [PubMed PMID: 19523568]
Level 3 (low-level) evidencePannabecker TL. Structure and function of the thin limbs of the loop of Henle. Comprehensive Physiology. 2012 Jul:2(3):2063-86. doi: 10.1002/cphy.c110019. Epub [PubMed PMID: 23723033]
Level 3 (low-level) evidenceMount DB. Thick ascending limb of the loop of Henle. Clinical journal of the American Society of Nephrology : CJASN. 2014 Nov 7:9(11):1974-86. doi: 10.2215/CJN.04480413. Epub 2014 Oct 15 [PubMed PMID: 25318757]
Oh SW, Han SY. Loop Diuretics in Clinical Practice. Electrolyte & blood pressure : E & BP. 2015 Jun:13(1):17-21. doi: 10.5049/EBP.2015.13.1.17. Epub 2015 Jun 30 [PubMed PMID: 26240596]
Hampel P, Römermann K, MacAulay N, Löscher W. Azosemide is more potent than bumetanide and various other loop diuretics to inhibit the sodium-potassium-chloride-cotransporter human variants hNKCC1A and hNKCC1B. Scientific reports. 2018 Jun 29:8(1):9877. doi: 10.1038/s41598-018-27995-w. Epub 2018 Jun 29 [PubMed PMID: 29959396]
Peti-Peterdi J, Harris RC. Macula densa sensing and signaling mechanisms of renin release. Journal of the American Society of Nephrology : JASN. 2010 Jul:21(7):1093-6. doi: 10.1681/ASN.2009070759. Epub 2010 Apr 1 [PubMed PMID: 20360309]
Level 3 (low-level) evidenceEllison DH. Clinical Pharmacology in Diuretic Use. Clinical journal of the American Society of Nephrology : CJASN. 2019 Aug 7:14(8):1248-1257. doi: 10.2215/CJN.09630818. Epub 2019 Apr 1 [PubMed PMID: 30936153]
Shankar SS, Brater DC. Loop diuretics: from the Na-K-2Cl transporter to clinical use. American journal of physiology. Renal physiology. 2003 Jan:284(1):F11-21 [PubMed PMID: 12473535]
Level 3 (low-level) evidenceEllison DH. Diuretic resistance: physiology and therapeutics. Seminars in nephrology. 1999 Nov:19(6):581-97 [PubMed PMID: 10598546]
Level 3 (low-level) evidenceBowman BN, Nawarskas JJ, Anderson JR. Treating Diuretic Resistance: An Overview. Cardiology in review. 2016 Sep-Oct:24(5):256-60. doi: 10.1097/CRD.0000000000000116. Epub [PubMed PMID: 27465540]
Level 3 (low-level) evidenceImiela T, Budaj A. Acetazolamide as Add-on Diuretic Therapy in Exacerbations of Chronic Heart Failure: a Pilot Study. Clinical drug investigation. 2017 Dec:37(12):1175-1181. doi: 10.1007/s40261-017-0577-1. Epub [PubMed PMID: 28965280]
Level 3 (low-level) evidenceCunha TDS, Heilberg IP. Bartter syndrome: causes, diagnosis, and treatment. International journal of nephrology and renovascular disease. 2018:11():291-301. doi: 10.2147/IJNRD.S155397. Epub 2018 Nov 9 [PubMed PMID: 30519073]
McCormick JA, Ellison DH. Distal convoluted tubule. Comprehensive Physiology. 2015 Jan:5(1):45-98. doi: 10.1002/cphy.c140002. Epub [PubMed PMID: 25589264]
Level 3 (low-level) evidenceSubramanya AR, Ellison DH. Distal convoluted tubule. Clinical journal of the American Society of Nephrology : CJASN. 2014 Dec 5:9(12):2147-63. doi: 10.2215/CJN.05920613. Epub 2014 May 22 [PubMed PMID: 24855283]
Liang W, Ma H, Cao L, Yan W, Yang J. Comparison of thiazide-like diuretics versus thiazide-type diuretics: a meta-analysis. Journal of cellular and molecular medicine. 2017 Nov:21(11):2634-2642. doi: 10.1111/jcmm.13205. Epub 2017 Jun 19 [PubMed PMID: 28631393]
Level 1 (high-level) evidenceGlover M, O'Shaughnessy KM. Molecular insights from dysregulation of the thiazide-sensitive WNK/SPAK/NCC pathway in the kidney: Gordon syndrome and thiazide-induced hyponatraemia. Clinical and experimental pharmacology & physiology. 2013 Dec:40(12):876-84. doi: 10.1111/1440-1681.12115. Epub [PubMed PMID: 23683032]
Level 3 (low-level) evidenceGamba G. The thiazide-sensitive Na+-Cl- cotransporter: molecular biology, functional properties, and regulation by WNKs. American journal of physiology. Renal physiology. 2009 Oct:297(4):F838-48. doi: 10.1152/ajprenal.00159.2009. Epub 2009 May 27 [PubMed PMID: 19474192]
Level 3 (low-level) evidenceDuarte JD, Cooper-DeHoff RM. Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert review of cardiovascular therapy. 2010 Jun:8(6):793-802. doi: 10.1586/erc.10.27. Epub [PubMed PMID: 20528637]
Level 3 (low-level) evidenceEllison DH, Loffing J. Thiazide effects and adverse effects: insights from molecular genetics. Hypertension (Dallas, Tex. : 1979). 2009 Aug:54(2):196-202. doi: 10.1161/HYPERTENSIONAHA.109.129171. Epub 2009 Jun 29 [PubMed PMID: 19564550]
Level 3 (low-level) evidencePalmer LG, Schnermann J. Integrated control of Na transport along the nephron. Clinical journal of the American Society of Nephrology : CJASN. 2015 Apr 7:10(4):676-87. doi: 10.2215/CJN.12391213. Epub 2014 Aug 6 [PubMed PMID: 25098598]
Level 3 (low-level) evidenceKwon TH, Frøkiær J, Nielsen S. Regulation of aquaporin-2 in the kidney: A molecular mechanism of body-water homeostasis. Kidney research and clinical practice. 2013 Sep:32(3):96-102. doi: 10.1016/j.krcp.2013.07.005. Epub 2013 Aug 27 [PubMed PMID: 26877923]
Loffing J, Korbmacher C. Regulated sodium transport in the renal connecting tubule (CNT) via the epithelial sodium channel (ENaC). Pflugers Archiv : European journal of physiology. 2009 May:458(1):111-35. doi: 10.1007/s00424-009-0656-0. Epub 2009 Mar 11 [PubMed PMID: 19277701]
Level 3 (low-level) evidencePearce D, Soundararajan R, Trimpert C, Kashlan OB, Deen PM, Kohan DE. Collecting duct principal cell transport processes and their regulation. Clinical journal of the American Society of Nephrology : CJASN. 2015 Jan 7:10(1):135-46. doi: 10.2215/CJN.05760513. Epub 2014 May 29 [PubMed PMID: 24875192]
Level 3 (low-level) evidenceRoy A, Al-bataineh MM, Pastor-Soler NM. Collecting duct intercalated cell function and regulation. Clinical journal of the American Society of Nephrology : CJASN. 2015 Feb 6:10(2):305-24. doi: 10.2215/CJN.08880914. Epub 2015 Jan 28 [PubMed PMID: 25632105]
Level 3 (low-level) evidenceButterworth MB. Regulation of the epithelial sodium channel (ENaC) by membrane trafficking. Biochimica et biophysica acta. 2010 Dec:1802(12):1166-77. doi: 10.1016/j.bbadis.2010.03.010. Epub 2010 Mar 27 [PubMed PMID: 20347969]
Level 3 (low-level) evidenceAtsmon J, Dolev E. Drug-induced hypomagnesaemia : scope and management. Drug safety. 2005:28(9):763-88 [PubMed PMID: 16119971]
Cumming DC. Use of spironolactone in treatment of hirsutism. Cleveland Clinic journal of medicine. 1990 May:57(3):285-7 [PubMed PMID: 2357784]
Janmohamed S, Bouloux PM. The pharmacological treatment of primary aldosteronism. Expert opinion on pharmacotherapy. 2006 Apr:7(5):563-73 [PubMed PMID: 16553572]
Level 3 (low-level) evidenceRudehill A, Gordon E, Ohman G, Lindqvist C, Andersson P. Pharmacokinetics and effects of mannitol on hemodynamics, blood and cerebrospinal fluid electrolytes, and osmolality during intracranial surgery. Journal of neurosurgical anesthesiology. 1993 Jan:5(1):4-12 [PubMed PMID: 8431668]
Ansary TM, Nakano D, Nishiyama A. Diuretic Effects of Sodium Glucose Cotransporter 2 Inhibitors and Their Influence on the Renin-Angiotensin System. International journal of molecular sciences. 2019 Feb 1:20(3):. doi: 10.3390/ijms20030629. Epub 2019 Feb 1 [PubMed PMID: 30717173]
Masuda T, Muto S, Fukuda K, Watanabe M, Ohara K, Koepsell H, Vallon V, Nagata D. Osmotic diuresis by SGLT2 inhibition stimulates vasopressin-induced water reabsorption to maintain body fluid volume. Physiological reports. 2020 Jan:8(2):e14360. doi: 10.14814/phy2.14360. Epub [PubMed PMID: 31994353]
Tanaka H, Takano K, Iijima H, Kubo H, Maruyama N, Hashimoto T, Arakawa K, Togo M, Inagaki N, Kaku K. Factors Affecting Canagliflozin-Induced Transient Urine Volume Increase in Patients with Type 2 Diabetes Mellitus. Advances in therapy. 2017 Feb:34(2):436-451. doi: 10.1007/s12325-016-0457-8. Epub 2016 Dec 15 [PubMed PMID: 27981497]
Level 3 (low-level) evidenceFountain JH, Kaur J, Lappin SL. Physiology, Renin Angiotensin System. StatPearls. 2024 Jan:(): [PubMed PMID: 29261862]
Navis G, de Jong P, Donker AJ, van der Hem GK, de Zeeuw D. Diuretic effects of angiotensin-converting enzyme inhibition: comparison of low and liberal sodium diet in hypertensive patients. Journal of cardiovascular pharmacology. 1987 Jun:9(6):743-8 [PubMed PMID: 2442543]
Level 1 (high-level) evidenceHerman LL, Padala SA, Ahmed I, Bashir K. Angiotensin-Converting Enzyme Inhibitors (ACEI). StatPearls. 2024 Jan:(): [PubMed PMID: 28613705]
Thornton SN. RAAS blockade in combination with diuretic therapy increases urine excretion, which in turn increases drinking and thus reduces erythropoietin and proteinuria. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2010 Jul:25(7):2383-4; author reply 2384. doi: 10.1093/ndt/gfq237. Epub 2010 Apr 28 [PubMed PMID: 20466667]
Level 3 (low-level) evidencePolhuis KCMM, Wijnen AHC, Sierksma A, Calame W, Tieland M. The Diuretic Action of Weak and Strong Alcoholic Beverages in Elderly Men: A Randomized Diet-Controlled Crossover Trial. Nutrients. 2017 Jun 28:9(7):. doi: 10.3390/nu9070660. Epub 2017 Jun 28 [PubMed PMID: 28657601]
Level 1 (high-level) evidenceHobson RM, Maughan RJ. Hydration status and the diuretic action of a small dose of alcohol. Alcohol and alcoholism (Oxford, Oxfordshire). 2010 Jul-Aug:45(4):366-73. doi: 10.1093/alcalc/agq029. Epub 2010 May 24 [PubMed PMID: 20497950]
Level 1 (high-level) evidenceCostello-Boerrigter LC, Boerrigter G, Burnett JC Jr. Pharmacology of vasopressin antagonists. Heart failure reviews. 2009 Jun:14(2):75-82. doi: 10.1007/s10741-008-9108-8. Epub 2008 Sep 3 [PubMed PMID: 18766438]
Aditya S, Rattan A. Vaptans: A new option in the management of hyponatremia. International journal of applied & basic medical research. 2012 Jul:2(2):77-83. doi: 10.4103/2229-516X.106347. Epub [PubMed PMID: 23776817]
Testani JM, Brisco MA, Turner JM, Spatz ES, Bellumkonda L, Parikh CR, Tang WH. Loop diuretic efficiency: a metric of diuretic responsiveness with prognostic importance in acute decompensated heart failure. Circulation. Heart failure. 2014 Mar 1:7(2):261-70. doi: 10.1161/CIRCHEARTFAILURE.113.000895. Epub 2013 Dec 30 [PubMed PMID: 24379278]
Level 1 (high-level) evidencePham D, Grodin JL. Dilemmas in the Dosing of Heart Failure Drugs: Titrating Diuretics in Chronic Heart Failure. Cardiac failure review. 2017 Nov:3(2):108-112. doi: 10.15420/cfr.2017:10:1. Epub [PubMed PMID: 29387462]
Kidney Disease Outcomes Quality Initiative (K/DOQI). K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2004 May:43(5 Suppl 1):S1-290 [PubMed PMID: 15114537]
Level 1 (high-level) evidencePonikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal. 2016 Jul 14:37(27):2129-2200. doi: 10.1093/eurheartj/ehw128. Epub 2016 May 20 [PubMed PMID: 27206819]
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL, American College of Cardiology Foundation, American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2013 Oct 15:62(16):e147-239. doi: 10.1016/j.jacc.2013.05.019. Epub 2013 Jun 5 [PubMed PMID: 23747642]
Level 3 (low-level) evidenceWhelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension (Dallas, Tex. : 1979). 2018 Jun:71(6):1269-1324. doi: 10.1161/HYP.0000000000000066. Epub 2017 Nov 13 [PubMed PMID: 29133354]
Level 3 (low-level) evidenceWelling PG. Pharmacokinetics of the thiazide diuretics. Biopharmaceutics & drug disposition. 1986 Nov-Dec:7(6):501-35 [PubMed PMID: 3828483]
Caruso FS, Szabadi RR, Vukovich RA. Pharmacokinetics and clinical pharmacology of indapamide. American heart journal. 1983 Jul:106(1 Pt 2):212-20 [PubMed PMID: 6869203]
Level 3 (low-level) evidenceTamargo J, Segura J, Ruilope LM. Diuretics in the treatment of hypertension. Part 1: thiazide and thiazide-like diuretics. Expert opinion on pharmacotherapy. 2014 Mar:15(4):527-47. doi: 10.1517/14656566.2014.879118. Epub 2014 Jan 20 [PubMed PMID: 24444254]
Level 3 (low-level) evidencePourafshar N, Alshahrani S, Karimi A, Soleimani M. Thiazide Therapy in Chronic Kidney Disease: Renal and Extra Renal Targets. Current drug metabolism. 2018:19(12):1012-1020. doi: 10.2174/1389200219666180702104559. Epub [PubMed PMID: 29962339]
Burnier M, Bakris G, Williams B. Redefining diuretics use in hypertension: why select a thiazide-like diuretic? Journal of hypertension. 2019 Aug:37(8):1574-1586. doi: 10.1097/HJH.0000000000002088. Epub [PubMed PMID: 30882593]
Vidt DG. Mechanism of action, pharmacokinetics, adverse effects, and therapeutic uses of amiloride hydrochloride, a new potassium-sparing diuretic. Pharmacotherapy. 1981 Nov-Dec:1(3):179-87 [PubMed PMID: 6927605]
Mutschler E, Gilfrich HJ, Knauf H, Möhrke W, Völger KD. Pharmacokinetics of triamterene. Clinical and experimental hypertension. Part A, Theory and practice. 1983:5(2):249-69 [PubMed PMID: 6831748]
Tetti M, Monticone S, Burrello J, Matarazzo P, Veglio F, Pasini B, Jeunemaitre X, Mulatero P. Liddle Syndrome: Review of the Literature and Description of a New Case. International journal of molecular sciences. 2018 Mar 11:19(3):. doi: 10.3390/ijms19030812. Epub 2018 Mar 11 [PubMed PMID: 29534496]
Level 3 (low-level) evidenceCarone L, Oxberry SG, Twycross R, Charlesworth S, Mihalyo M, Wilcock A. Spironolactone. Journal of pain and symptom management. 2017 Feb:53(2):288-292. doi: 10.1016/j.jpainsymman.2016.12.320. Epub 2016 Dec 23 [PubMed PMID: 28024992]
Cook CS, Berry LM, Bible RH, Hribar JD, Hajdu E, Liu NW. Pharmacokinetics and metabolism of [14C]eplerenone after oral administration to humans. Drug metabolism and disposition: the biological fate of chemicals. 2003 Nov:31(11):1448-55 [PubMed PMID: 14570778]
Quinkler M, Stewart PM. Treatment of primary aldosteronism. Best practice & research. Clinical endocrinology & metabolism. 2010 Dec:24(6):923-32. doi: 10.1016/j.beem.2010.10.001. Epub [PubMed PMID: 21115161]
Level 3 (low-level) evidenceRitschel WA, Paulos C, Arancibia A, Agrawal MA, Wetzelsberger KM, Lücker PW. Pharmacokinetics of acetazolamide in healthy volunteers after short- and long-term exposure to high altitude. Journal of clinical pharmacology. 1998 Jun:38(6):533-9 [PubMed PMID: 9650543]
Kassamali R, Sica DA. Acetazolamide: a forgotten diuretic agent. Cardiology in review. 2011 Nov-Dec:19(6):276-8. doi: 10.1097/CRD.0b013e31822b4939. Epub [PubMed PMID: 21983315]
Cloyd JC, Snyder BD, Cleeremans B, Bundlie SR, Blomquist CH, Lakatua DJ. Mannitol pharmacokinetics and serum osmolality in dogs and humans. The Journal of pharmacology and experimental therapeutics. 1986 Feb:236(2):301-6 [PubMed PMID: 3080582]
Level 3 (low-level) evidenceLin SY, Tang SC, Tsai LK, Yeh SJ, Shen LJ, Wu FL, Jeng JS. Incidence and Risk Factors for Acute Kidney Injury Following Mannitol Infusion in Patients With Acute Stroke: A Retrospective Cohort Study. Medicine. 2015 Nov:94(47):e2032. doi: 10.1097/MD.0000000000002032. Epub [PubMed PMID: 26632702]
Level 2 (mid-level) evidenceMurray D. Emergency management: angle-closure glaucoma. Community eye health. 2018:31(103):64 [PubMed PMID: 30487684]
Murdoch D. Altitude sickness. BMJ clinical evidence. 2010 Mar 18:2010():. pii: 1209. Epub 2010 Mar 18 [PubMed PMID: 21718562]
Level 1 (high-level) evidenceHoward SC, McCormick J, Pui CH, Buddington RK, Harvey RD. Preventing and Managing Toxicities of High-Dose Methotrexate. The oncologist. 2016 Dec:21(12):1471-1482 [PubMed PMID: 27496039]
Prichard BN, Owens CW, Woolf AS. Adverse reactions to diuretics. European heart journal. 1992 Dec:13 Suppl G():96-103 [PubMed PMID: 1486914]
Levine SN, Sanson TH. Treatment of hyperglycaemic hyperosmolar non-ketotic syndrome. Drugs. 1989 Sep:38(3):462-72 [PubMed PMID: 2680438]
Sica DA, Carter B, Cushman W, Hamm L. Thiazide and loop diuretics. Journal of clinical hypertension (Greenwich, Conn.). 2011 Sep:13(9):639-43. doi: 10.1111/j.1751-7176.2011.00512.x. Epub 2011 Jul 27 [PubMed PMID: 21896142]
Qavi AH, Kamal R, Schrier RW. Clinical Use of Diuretics in Heart Failure, Cirrhosis, and Nephrotic Syndrome. International journal of nephrology. 2015:2015():975934. doi: 10.1155/2015/975934. Epub 2015 Jul 29 [PubMed PMID: 26294976]
Leclercq F, Leclercq B. Hypokalemic Metabolic Alkalosis. StatPearls. 2024 Jan:(): [PubMed PMID: 31424842]
Brinkman JE, Sharma S. Physiology, Metabolic Alkalosis. StatPearls. 2024 Jan:(): [PubMed PMID: 29493916]
Pham PC, Pham PA, Pham SV, Pham PT, Pham PM, Pham PT. Hypomagnesemia: a clinical perspective. International journal of nephrology and renovascular disease. 2014:7():219-30. doi: 10.2147/IJNRD.S42054. Epub 2014 Jun 9 [PubMed PMID: 24966690]
Level 3 (low-level) evidenceKieboom BCT, Zietse R, Ikram MA, Hoorn EJ, Stricker BH. Thiazide but not loop diuretics is associated with hypomagnesaemia in the general population. Pharmacoepidemiology and drug safety. 2018 Nov:27(11):1166-1173. doi: 10.1002/pds.4636. Epub 2018 Aug 10 [PubMed PMID: 30095199]
Hyndman D, Liu S, Miner JN. Urate Handling in the Human Body. Current rheumatology reports. 2016 Jun:18(6):34. doi: 10.1007/s11926-016-0587-7. Epub [PubMed PMID: 27105641]
Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, New M, Purnell J, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Herink M, Ito MK. Medication Induced Changes in Lipid and Lipoproteins. Endotext. 2000:(): [PubMed PMID: 26561699]
Hanberg JS, Rao V, Ter Maaten JM, Laur O, Brisco MA, Perry Wilson F, Grodin JL, Assefa M, Samuel Broughton J, Planavsky NJ, Ahmad T, Bellumkonda L, Tang WH, Parikh CR, Testani JM. Hypochloremia and Diuretic Resistance in Heart Failure: Mechanistic Insights. Circulation. Heart failure. 2016 Aug:9(8):. doi: 10.1161/CIRCHEARTFAILURE.116.003180. Epub [PubMed PMID: 27507113]
Ganesan P, Schmiedge J, Manchaiah V, Swapna S, Dhandayutham S, Kothandaraman PP. Ototoxicity: A Challenge in Diagnosis and Treatment. Journal of audiology & otology. 2018 Apr:22(2):59-68. doi: 10.7874/jao.2017.00360. Epub 2018 Feb 26 [PubMed PMID: 29471610]
Domínguez-Ortega J, Martínez-Alonso JC, Domínguez-Ortega C, Fuentes MJ, Frades A, Fernández-Colino T. Anaphylaxis to oral furosemide. Allergologia et immunopathologia. 2003 Nov-Dec:31(6):345-7 [PubMed PMID: 14670291]
Level 3 (low-level) evidenceWright AA, Vesta KS, Stark JE, Smith WJ. Stevens-Johnson syndrome associated with furosemide: a case report. Journal of pharmacy practice. 2010 Aug:23(4):367-70. doi: 10.1177/0897190010362260. Epub 2010 May 6 [PubMed PMID: 21507837]
Level 3 (low-level) evidenceKumar P, Chauhan A, Charaniya R, Ghosh A, Tandon V. Metolazone Associated Stevens Johnson Syndrome-Toxic Epidermal Necrolysis Overlap. Journal of clinical and diagnostic research : JCDR. 2016 Mar:10(3):FD01-2. doi: 10.7860/JCDR/2016/17768.7404. Epub 2016 Mar 1 [PubMed PMID: 27134890]
Jennings M, Shortland JR, Maddocks JL. Interstitial nephritis associated with frusemide. Journal of the Royal Society of Medicine. 1986 Apr:79(4):239-40 [PubMed PMID: 3701771]
Level 3 (low-level) evidenceTurmen T, Thom P, Louridas AT, LeMorvan P, Aranda JV. Protein binding and bilirubin displacing properties of bumetanide and furosemide. Journal of clinical pharmacology. 1982 Nov-Dec:22(11-12):551-6 [PubMed PMID: 7161408]
Kelly JP, Kaufman DW, Shapiro S. Risks of agranulocytosis and aplastic anemia in relation to the use of cardiovascular drugs: The International Agranulocytosis and Aplastic Anemia Study. Clinical pharmacology and therapeutics. 1991 Mar:49(3):330-41 [PubMed PMID: 1672513]
Level 2 (mid-level) evidenceHwang KS, Kim GH. Thiazide-induced hyponatremia. Electrolyte & blood pressure : E & BP. 2010 Jun:8(1):51-7. doi: 10.5049/EBP.2010.8.1.51. Epub 2010 Jun 30 [PubMed PMID: 21468197]
Nijenhuis T, Vallon V, van der Kemp AW, Loffing J, Hoenderop JG, Bindels RJ. Enhanced passive Ca2+ reabsorption and reduced Mg2+ channel abundance explains thiazide-induced hypocalciuria and hypomagnesemia. The Journal of clinical investigation. 2005 Jun:115(6):1651-8 [PubMed PMID: 15902302]
Level 3 (low-level) evidenceHoover RS, Tomilin V, Hanson L, Pochynyuk O, Ko B. PTH modulation of NCC activity regulates TRPV5 Ca2+ reabsorption. American journal of physiology. Renal physiology. 2016 Jan 15:310(2):F144-51. doi: 10.1152/ajprenal.00323.2015. Epub 2015 Nov 25 [PubMed PMID: 26608788]
Perazella MA. Proton pump inhibitors and hypomagnesemia: a rare but serious complication. Kidney international. 2013 Apr:83(4):553-6. doi: 10.1038/ki.2012.462. Epub [PubMed PMID: 23538697]
Whaley-Connell A, Sowers JR. Metabolic impact of adding a thiazide diuretic to captopril. Hypertension (Dallas, Tex. : 1979). 2013 Apr:61(4):765-6. doi: 10.1161/HYPERTENSIONAHA.111.00494. Epub 2013 Feb 19 [PubMed PMID: 23424231]
Carter BL, Einhorn PT, Brands M, He J, Cutler JA, Whelton PK, Bakris GL, Brancati FL, Cushman WC, Oparil S, Wright JT Jr, Working Group from the National Heart, Lung, and Blood Institute. Thiazide-induced dysglycemia: call for research from a working group from the national heart, lung, and blood institute. Hypertension (Dallas, Tex. : 1979). 2008 Jul:52(1):30-6. doi: 10.1161/HYPERTENSIONAHA.108.114389. Epub 2008 May 26 [PubMed PMID: 18504319]
Raja R, Kavita F, Amreek F, Shah A, Sayeed KA, Sehar A. Hyperuricemia Associated with Thiazide Diuretics in Hypertensive Adults. Cureus. 2019 Aug 22:11(8):e5457. doi: 10.7759/cureus.5457. Epub 2019 Aug 22 [PubMed PMID: 31641556]
Jones MR, Hall OM, Kaye AM, Kaye AD. Drug-induced acute pancreatitis: a review. Ochsner journal. 2015 Spring:15(1):45-51 [PubMed PMID: 25829880]
Arnold DM, Nazi I, Warkentin TE, Smith JW, Toltl LJ, George JN, Kelton JG. Approach to the diagnosis and management of drug-induced immune thrombocytopenia. Transfusion medicine reviews. 2013 Jul:27(3):137-45. doi: 10.1016/j.tmrv.2013.05.005. Epub 2013 Jul 8 [PubMed PMID: 23845922]
Level 3 (low-level) evidenceSimon LV, Hashmi MF, Farrell MW. Hyperkalemia. StatPearls. 2024 Jan:(): [PubMed PMID: 29261936]
Sharma S, Hashmi MF, Aggarwal S. Hyperchloremic Acidosis. StatPearls. 2024 Jan:(): [PubMed PMID: 29493965]
Harris AN, Grimm PR, Lee HW, Delpire E, Fang L, Verlander JW, Welling PA, Weiner ID. Mechanism of Hyperkalemia-Induced Metabolic Acidosis. Journal of the American Society of Nephrology : JASN. 2018 May:29(5):1411-1425. doi: 10.1681/ASN.2017111163. Epub 2018 Feb 26 [PubMed PMID: 29483157]
DuBose TD Jr. Hyperkalemic hyperchloremic metabolic acidosis: pathophysiologic insights. Kidney international. 1997 Feb:51(2):591-602 [PubMed PMID: 9027745]
Level 3 (low-level) evidenceCarr MC, Prien EL Jr, Babayan RK. Triamterene nephrolithiasis: renewed attention is warranted. The Journal of urology. 1990 Dec:144(6):1339-40 [PubMed PMID: 2231920]
Kim GK, Del Rosso JQ. Oral Spironolactone in Post-teenage Female Patients with Acne Vulgaris: Practical Considerations for the Clinician Based on Current Data and Clinical Experience. The Journal of clinical and aesthetic dermatology. 2012 Mar:5(3):37-50 [PubMed PMID: 22468178]
Veeregowda SH, Krishnamurthy JJ, Krishnaswamy B, Narayana S. Spironolactone-Induced Unilateral Gynecomastia. International journal of applied & basic medical research. 2018 Jan-Mar:8(1):45-47. doi: 10.4103/ijabmr.IJABMR_399_16. Epub [PubMed PMID: 29552536]
Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hofland J, Kalra S, Kaltsas G, Kapoor N, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, New M, Purnell J, Sahay R, Shah AS, Singer F, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Swerdloff RS, Ng JCM. Gynecomastia: Etiology, Diagnosis, and Treatment. Endotext. 2000:(): [PubMed PMID: 25905330]
Pham AQ, Xu LH, Moe OW. Drug-Induced Metabolic Acidosis. F1000Research. 2015:4():. pii: F1000 Faculty Rev-1460. doi: 10.12688/f1000research.7006.1. Epub 2015 Dec 16 [PubMed PMID: 26918138]
Hopkins E, Sanvictores T, Sharma S. Physiology, Acid Base Balance. StatPearls. 2024 Jan:(): [PubMed PMID: 29939584]
Boone MD, Oren-Grinberg A, Robinson TM, Chen CC, Kasper EM. Mannitol or hypertonic saline in the setting of traumatic brain injury: What have we learned? Surgical neurology international. 2015:6():177. doi: 10.4103/2152-7806.170248. Epub 2015 Nov 23 [PubMed PMID: 26673517]
Pascual E,Perdiguero M, Gout, diuretics and the kidney. Annals of the rheumatic diseases. 2006 Aug; [PubMed PMID: 16837492]
Johnson KK, Green DL, Rife JP, Limon L. Sulfonamide cross-reactivity: fact or fiction? The Annals of pharmacotherapy. 2005 Feb:39(2):290-301 [PubMed PMID: 15644481]
Giles A, Foushee J, Lantz E, Gumina G. Sulfonamide Allergies. Pharmacy (Basel, Switzerland). 2019 Sep 11:7(3):. doi: 10.3390/pharmacy7030132. Epub 2019 Sep 11 [PubMed PMID: 31514363]
Wulf NR, Matuszewski KA. Sulfonamide cross-reactivity: is there evidence to support broad cross-allergenicity? American journal of health-system pharmacy : AJHP : official journal of the American Society of Health-System Pharmacists. 2013 Sep 1:70(17):1483-94. doi: 10.2146/ajhp120291. Epub [PubMed PMID: 23943179]
Level 3 (low-level) evidenceShah TJ, Moshirfar M, Hoopes PC Sr. "Doctor, I have a Sulfa Allergy": Clarifying the Myths of Cross-Reactivity. Ophthalmology and therapy. 2018 Dec:7(2):211-215. doi: 10.1007/s40123-018-0136-8. Epub 2018 Jun 29 [PubMed PMID: 29959752]
Dineva S, Uzunova K, Pavlova V, Filipova E, Kalinov K, Vekov T. Comparative efficacy and safety of chlorthalidone and hydrochlorothiazide-meta-analysis. Journal of human hypertension. 2019 Nov:33(11):766-774. doi: 10.1038/s41371-019-0255-2. Epub 2019 Oct 8 [PubMed PMID: 31595024]
Level 2 (mid-level) evidenceSilver A. What if chlorthalidone-associated hyperglycemia develops? Archives of internal medicine. 2007 Jul 9:167(13):1434; author reply 1434-5 [PubMed PMID: 17620541]
Level 3 (low-level) evidenceWilliams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I, ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European heart journal. 2018 Sep 1:39(33):3021-3104. doi: 10.1093/eurheartj/ehy339. Epub [PubMed PMID: 30165516]
Sica DA, Gehr TW. Diuretic use in stage 5 chronic kidney disease and end-stage renal disease. Current opinion in nephrology and hypertension. 2003 Sep:12(5):483-90 [PubMed PMID: 12920394]
Level 3 (low-level) evidenceBianchi S, Aucella F, De Nicola L, Genovesi S, Paoletti E, Regolisti G. Management of hyperkalemia in patients with kidney disease: a position paper endorsed by the Italian Society of Nephrology. Journal of nephrology. 2019 Aug:32(4):499-516. doi: 10.1007/s40620-019-00617-y. Epub 2019 May 22 [PubMed PMID: 31119681]
Tamargo J, Segura J, Ruilope LM. Diuretics in the treatment of hypertension. Part 2: loop diuretics and potassium-sparing agents. Expert opinion on pharmacotherapy. 2014 Apr:15(5):605-21. doi: 10.1517/14656566.2014.879117. Epub 2014 Jan 23 [PubMed PMID: 24456327]
Level 3 (low-level) evidenceAdamson R, Swenson ER. Acetazolamide Use in Severe Chronic Obstructive Pulmonary Disease. Pros and Cons. Annals of the American Thoracic Society. 2017 Jul:14(7):1086-1093. doi: 10.1513/AnnalsATS.201701-016FR. Epub [PubMed PMID: 28622013]
Mason A, Malik A, Ginglen JG. Hypertonic Fluids. StatPearls. 2024 Jan:(): [PubMed PMID: 31194351]
Sweeney KR, Chapron DJ, Kramer PA. Effect of salicylate on serum protein binding and red blood cell uptake of acetazolamide in vitro. Journal of pharmaceutical sciences. 1988 Sep:77(9):751-6 [PubMed PMID: 3225768]
Liddell NE, Maren TH. CO2 retention as a basis for increased toxicity of salicylate with acetazolamide: avoidance of increased toxicity with benzolamide. The Journal of pharmacology and experimental therapeutics. 1975 Oct:195(1):1-7 [PubMed PMID: 241836]
Level 3 (low-level) evidenceRunde TJ, Nappe TM. Salicylates Toxicity. StatPearls. 2024 Jan:(): [PubMed PMID: 29763054]
Hörl WH. Nonsteroidal Anti-Inflammatory Drugs and the Kidney. Pharmaceuticals (Basel, Switzerland). 2010 Jul 21:3(7):2291-2321 [PubMed PMID: 27713354]
Houston MC. Nonsteroidal anti-inflammatory drugs and antihypertensives. The American journal of medicine. 1991 May 17:90(5A):42S-47S [PubMed PMID: 1903902]
Zand F, Asadi S, Katibeh P. Good outcome after digoxin toxicity despite very high serum potassium level. Iranian Red Crescent medical journal. 2011 Sep:13(9):680-1. doi: 10.5812/kowsar.20741804.2238. Epub 2011 Sep 15 [PubMed PMID: 22737544]
Wang MT, Su CY, Chan AL, Lian PW, Leu HB, Hsu YJ. Risk of digoxin intoxication in heart failure patients exposed to digoxin-diuretic interactions: a population-based study. British journal of clinical pharmacology. 2010 Aug:70(2):258-67. doi: 10.1111/j.1365-2125.2010.03687.x. Epub [PubMed PMID: 20653679]
Level 2 (mid-level) evidenceJain A, SISODIA J. Quinidine. StatPearls. 2024 Jan:(): [PubMed PMID: 31194350]
Newman GH, Wade M, Hosking DJ. Effect of bendrofluazide on calcium reabsorption in hypoparathyroidism. European journal of clinical pharmacology. 1984:27(1):41-6 [PubMed PMID: 6489426]
Kirchner KA, Effect of diuretic and antidiuretic agents on lithium clearance as a marker for proximal delivery. Kidney international. Supplement. 1990 Mar; [PubMed PMID: 2182927]
Level 3 (low-level) evidenceCadwallader AB, de la Torre X, Tieri A, Botrè F. The abuse of diuretics as performance-enhancing drugs and masking agents in sport doping: pharmacology, toxicology and analysis. British journal of pharmacology. 2010 Sep:161(1):1-16. doi: 10.1111/j.1476-5381.2010.00789.x. Epub [PubMed PMID: 20718736]
Mascolo M, Chu ES, Mehler PS. Abuse and clinical value of diuretics in eating disorders therapeutic applications. The International journal of eating disorders. 2011 Apr:44(3):200-2. doi: 10.1002/eat.20814. Epub [PubMed PMID: 20186716]
Jaber D, Al Awwa I, Wazaify M. Multiple Prescription Drug Abuse and Salt Craving in a Psychotic Patient: A Case Report From a Teaching Hospital in Jordan. International journal of high risk behaviors & addiction. 2015 Sep:4(3):e22449. doi: 10.5812/ijhrba.22449v2. Epub 2015 Sep 1 [PubMed PMID: 26495254]
Level 3 (low-level) evidenceWalsh SB, Shirley DG, Wrong OM, Unwin RJ. Urinary acidification assessed by simultaneous furosemide and fludrocortisone treatment: an alternative to ammonium chloride. Kidney international. 2007 Jun:71(12):1310-6 [PubMed PMID: 17410104]
Level 1 (high-level) evidenceDhayat NA, Gradwell MW, Pathare G, Anderegg M, Schneider L, Luethi D, Mattmann C, Moe OW, Vogt B, Fuster DG. Furosemide/Fludrocortisone Test and Clinical Parameters to Diagnose Incomplete Distal Renal Tubular Acidosis in Kidney Stone Formers. Clinical journal of the American Society of Nephrology : CJASN. 2017 Sep 7:12(9):1507-1517. doi: 10.2215/CJN.01320217. Epub 2017 Aug 3 [PubMed PMID: 28775126]
Caldas A, Broyer M, Dechaux M, Kleinknecht C. Primary distal tubular acidosis in childhood: clinical study and long-term follow-up of 28 patients. The Journal of pediatrics. 1992 Aug:121(2):233-41 [PubMed PMID: 1640289]
Porsbjerg C, Sverrild A, Backer V. The usefulness of the mannitol challenge test for asthma. Expert review of respiratory medicine. 2013 Dec:7(6):655-63. doi: 10.1586/17476348.2013.847370. Epub [PubMed PMID: 24224508]
Ding D, Liu H, Qi W, Jiang H, Li Y, Wu X, Sun H, Gross K, Salvi R. Ototoxic effects and mechanisms of loop diuretics. Journal of otology. 2016 Dec:11(4):145-156. doi: 10.1016/j.joto.2016.10.001. Epub 2016 Oct 27 [PubMed PMID: 29937824]
Level 2 (mid-level) evidenceDormans TP, van Meyel JJ, Gerlag PG, Tan Y, Russel FG, Smits P. Diuretic efficacy of high dose furosemide in severe heart failure: bolus injection versus continuous infusion. Journal of the American College of Cardiology. 1996 Aug:28(2):376-82 [PubMed PMID: 8800113]
Level 1 (high-level) evidenceDiuretics 2012; [PubMed PMID: 31644115]
Taglietti F, Del Nonno F, Baiocchini A, Falasca L, Pieri S, Capone A, Grilli E, Chinello P, Petrosillo N. Acute hepatocellular and cholestatic injury during therapy with hydrochlorothiazide - clinicohistopathologic findings: a case report. Journal of medical case reports. 2010 Oct 21:4():332. doi: 10.1186/1752-1947-4-332. Epub 2010 Oct 21 [PubMed PMID: 20964809]
Level 3 (low-level) evidenceWalker RM, McElligott TF. Furosemide induced hepatotoxicity. The Journal of pathology. 1981 Dec:135(4):301-14 [PubMed PMID: 7328448]
Level 3 (low-level) evidenceWu X, Zhang W, Ren H, Chen X, Xie J, Chen N. Diuretics associated acute kidney injury: clinical and pathological analysis. Renal failure. 2014 Aug:36(7):1051-5. doi: 10.3109/0886022X.2014.917560. Epub 2014 Jun 18 [PubMed PMID: 24940940]
Level 2 (mid-level) evidenceTenny S, Varacallo M. Evidence Based Medicine. StatPearls. 2024 Jan:(): [PubMed PMID: 29262040]