Introduction
The digastrics are a pair of muscles so named as each has an anterior and a posterior belly (see Image. Digastric Muscle, Lateral View). These muscles derive embryonically from the 1st and 2nd pharyngeal arches and thus, are supplied by different nerves and arteries. The digastrics coordinate with other muscles in performing vital actions. Neuromuscular injuries can impair digastric muscle function, which may become apparent on physical examination.
Additionally, the digastric muscles are critical surgical landmarks during neck dissections and are valuable components of neck reconstruction procedures. Digastric muscle anatomic variants can be misleading in imaging studies. Careful consideration of these variations is critical in clinical assessment and surgical planning.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The neck contains a pair of digastric muscles, each subdividing into an anterior and posterior belly. The 2 bellies connect by an intermediate tendon. The anterior digastric belly attaches superiorly near the midline of the mandibular base on the digastric fossa and runs inferiorly toward the hyoid. The posterior belly attaches superiorly to the temporal bone at the mastoid notch and slopes inferiorly to meet the intermediate tendon (see Image. Neck Muscles).
The intermediate tendon typically courses through the stylohyoid muscle, attaching to the side of the hyoid bone's body and greater cornu via a fibrous loop. However, some individuals may have the intermediate tendon attaching medially or laterally to the hyoid.[2]
The anterior belly of the digastric separates the submental from the submandibular triangle of the neck (see Image. Anterior Neck Muscles and Related Structures). The anterior and posterior digastric bellies and the inferior mandibular margin border the submandibular triangle. This region houses the submandibular gland, anterior facial vein, submental artery, mylohyoid nerve and vessels, and the external carotid. The submental triangle is bordered laterally by the anterior belly and contains lymph nodes that drain the floor of the mouth and part of the tongue.[3] The posterior digastric belly also serves as a boundary for the carotid triangle, the area where the facial artery branches from the external carotid (see Image. Superficial Neck Anatomy).[4]
The digastrics coordinate with other head and neck muscles during swallowing, chewing, and speech. The anterior belly of the digastric is 1 of 3 suprahyoid muscles stabilizing the hyoid during swallowing—an action that protects the airway while eating. The digastrics raise the tongue base and hyoid bone and depress the mandible for jaw opening, chewing, and speech.[5] Posterior digastric muscle contraction aids in head extension.
The infrahyoids are the muscles antagonistic to the digastrics.
Embryology
The embryologic period occurs during the first 8 weeks post-fertilization. During this time, neural crest cells migrate caudally to form the 5 pharyngeal arches. The 1st and 2nd pharyngeal arches give rise to the anterior and posterior bellies of the digastrics and their respective nerve supplies. The anterior digastric belly and mylohyoid nerve form from the 1st pharyngeal arch, also known as the mandibular arch. The posterior digastric belly and the facial nerve derive from the 2nd pharyngeal arch, also known as the hyoid arch.
Other muscular structures that arise from the 1st pharyngeal arch include the mylohyoid, tensor veli palatini, tensor tympani, and the mastication muscles temporalis, masseter, and medial and lateral pterygoids. Besides the posterior digastric belly, the 2nd pharyngeal arch gives rise to the stapedius, buccinator, auricular muscles, occipitofrontalis, facial muscles, platysma, and stylohyoid muscles.[6] Researchers postulate that the broad array of anatomical variants of the anterior belly of the digastric primarily results from the complex morphogenesis of the 1st pharyngeal arch.
Blood Supply and Lymphatics
The submental artery, a branch of the facial artery, supplies blood to the anterior belly of the digastric. The submental artery runs between the submandibular gland and the mylohyoid muscle. The muscular branches of the posterior auricular artery and occipital branches of the external carotid artery deliver blood to the posterior digastric belly.[6]
Nerves
The mylohyoid nerve innervates the anterior belly of the digastric. This nerve is a branch of the inferior alveolar nerve, which arises from the mandibular branch of the trigeminal nerve.[6] The mandibular branch of the trigeminal nerve branches off before the inferior alveolar nerve penetrates the mandibular foramen. The inferior alveolar nerve then courses through the mylohyoid canal before giving off motor branches to both the mylohyoid muscle and the anterior digastric belly.[7] Branches of the facial nerve innervate the posterior belly of the digastric muscle.
Muscles
The lateral aspect of the posterior belly is adjacent to the sternocleidomastoid muscles, longus colli, and splenius capitis. The medial aspect is related to the lateral rectus muscle of the head. The anterior belly is laterally covered by the skin planes and platysma muscle. Medially, the anterior belly rests on the mylohyoid muscle.
Physiologic Variants
The anterior belly of the digastric has more anatomical variations than the posterior belly. Anterior digastric belly variations occur in up to 65.8% of the population. Of those reported, unilateral variants are more common than bilateral variants. Many of these variants are accessory muscle bellies with different origins and insertions. Reports also exist of nerve supply variations. For example, the facial and mylohyoid nerves may innervate the anterior belly. These variants have no confirmed clinical consequences.[8]
The intermediate tendon does not always pierce the stylohyoid muscle but may lean superiorly or laterally to it. Agenesis of the anterior digastric belly is an anomaly in a few individuals.
Surgical Considerations
The digastrics serve as a significant surgical landmark in neck dissections. The posterior belly can help identify the spinal accessory and hypoglossal nerves, internal jugular veins, and carotid arteries. This portion of the digastric can also help identify the ansa cervicalis in reconstruction cases.
The anterior digastric belly is often included in submental flaps during facial reconstruction, as the submental vessels frequently course deep to the muscle. The intermediate tendon of the digastric can be attached to the tongue to help avoid stridor and the need for tracheostomy in patients who undergo anterior mandibular arch resection.
The digastrics may be used as flaps to restore a symmetrical smile to those with injury to the marginal mandibular branch of the facial nerve.[6] The digastric can be sutured to the mandible in primary tongue cancer resection with neck dissection to accomplish laryngeal suspension.[9]
Clinical Significance
Clinical considerations related to the digastric muscles include the following:
- Digastric muscle variants may be confused with neck masses. Knowledge of anatomical variations is thus critical during clinical evaluation and surgical planning.
- The digastric muscles may be implicated in post-radiation dysphagia or swallowing dysfunction.[10] Post-radiation changes leading to digastric atrophy or fibrosis is a possible sequela in patients who have undergone postoperative radiotherapy for oral cancer.[11] Exercises targeting the suprahyoid muscles, including the anterior belly of the digastric, are thought to help patients with dysphagia.[12][13]
- Styloid process neuralgia may be due to digastric muscle calcification combined with styloid ligament calcification or length alterations. This painful condition is also known as long styloid process syndrome or Eagle syndrome. Muscle calcification can manifest as throat disorders, ear pain, and pharyngeal pain. The patient may experience pain during tongue or head movements. Surgery is necessary in most cases.
- The digastric muscle is implicated as the source of pain in bruxism or the habit of clenching teeth. Myofunctional physiotherapy or speech therapy can reduce the muscle's electrical activity and reduce pain during jaw movement.
- The digastric muscle's posterior portion is occasionally the site of a Citelli abscess, a rare complication of otitis media. Management is surgical.
- Digastric muscle trigger points may cause referred pain to the teeth. The therapy is of myofunctional type.
Understanding the digastric muscle's anatomy, function, and potential involvement in various clinical conditions is crucial for healthcare professionals across different specialties.
Other Issues
The occurrence of digastric hemangiomas has been reported in the literature. This condition may be clinically insignificant or manifest as a neck mass, pain, dysphagia, or dysphonia. Asymptomatic cases may not need treatment, but surgery is required if the tumor compromises function.[14]
Media
(Click Image to Enlarge)
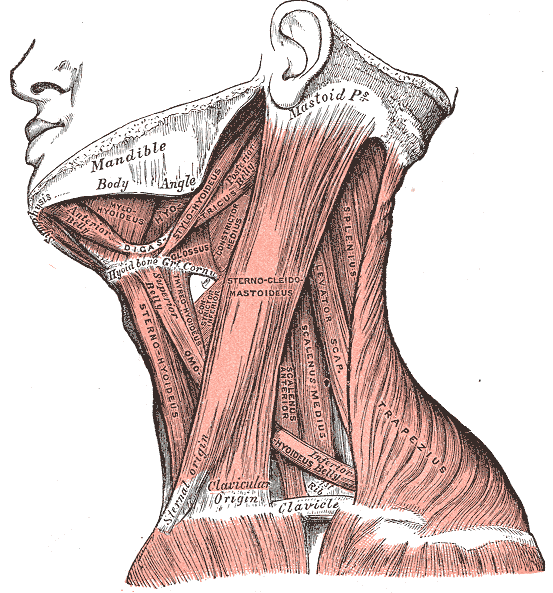
Neck Muscles. This lateral-view illustration shows the trapezius, sternocleidomastoideus, sternohyoideus, omohyoideus belly, scalenus anterior and medius, levator scapulae, splenius, mylohyoideus, thyrohyoideus, digastricus, and stylohyoideus muscles. The mandible, mastoid process, clavicle, and hyoid bone are also shown.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
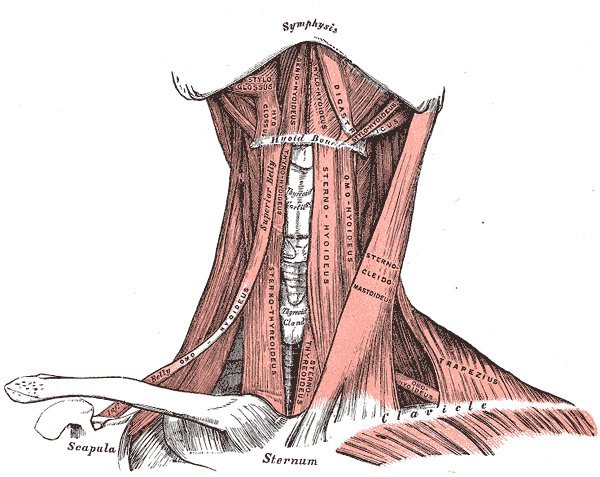
Anterior Neck Muscles and Related Structures. This illustration shows the supra- and infrahyoid, styloglossus, hyoglossus, geniohyoideus, mylohyoideus, digastricus, stylohyoideus, omohyoideus, sternothyroideus, sternohyoideus, omohyoideus, sternocleidomastoideus, trapezius, and omohyoideus muscles. The mandibular symphysis, thyroid cartilage, thyroid gland, hyoid bone, clavicles, scapula, and sternum are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
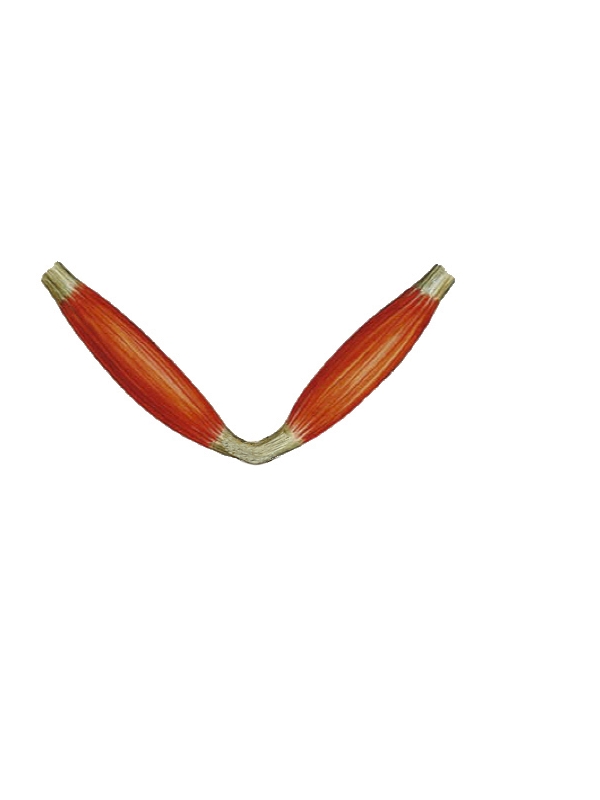
Digastric Muscle, Lateral View. This image shows the digastric muscle bellies connected by the intermediate tendon. The tendon is held in position by a fibrous loop attached to the hyoid (not shown).
Contributed by Bruno Bordoni, PhD
(Click Image to Enlarge)
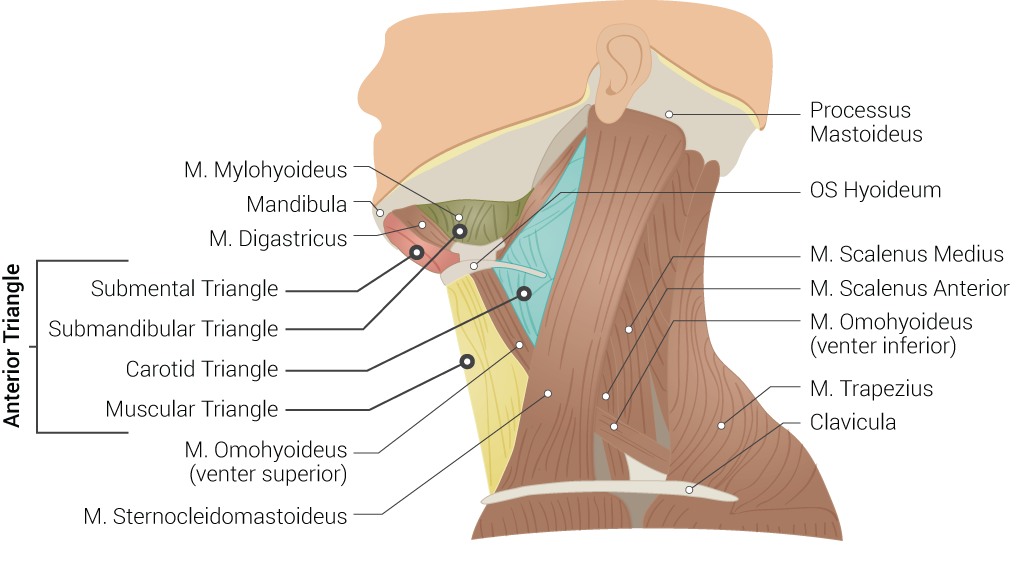
Superficial Neck Anatomy. This left lateral-view illustration shows the anterior and posterior triangles. The anterior triangle is further divided into the submental, submandibular, carotid, and muscular triangles. The muscles in this illustration include the mylohyoideus, digastricus, omohyoideus (venter superior and inferior), sternocleidomastoideus, scalenus medius and anterior, and trapezius. Bony structures include the mandible, mastoid process, left hyoid, and clavicle.
Contributed by B Palmer
References
Bhat NP, Sumalatha S, Shetty A, Prabhath S. A clinical perspective on the anatomical study of digastric muscle. Anatomy & cell biology. 2023 Dec 31:56(4):441-447. doi: 10.5115/acb.23.043. Epub 2023 Oct 6 [PubMed PMID: 37798015]
Level 3 (low-level) evidenceHsiao TH, Chang HP. Anatomical variations in the digastric muscle. The Kaohsiung journal of medical sciences. 2019 Feb:35(2):83-86. doi: 10.1002/kjm2.12012. Epub [PubMed PMID: 30848024]
Singh M, Vashistha A, Chaudhary M, Kaur G. Forgotten triangles of neck. Annals of maxillofacial surgery. 2016 Jan-Jun:6(1):91-3. doi: 10.4103/2231-0746.186149. Epub [PubMed PMID: 27563614]
Meegalla N, Sood G, Nessel TA, Downs BW. Anatomy, Head and Neck: Facial Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 30725617]
Sowman PF, Flavel SC, McShane CL, Sakuma S, Miles TS, Nordstrom MA. Asymmetric activation of motor cortex controlling human anterior digastric muscles during speech and target-directed jaw movements. Journal of neurophysiology. 2009 Jul:102(1):159-66. doi: 10.1152/jn.90894.2008. Epub 2009 May 6 [PubMed PMID: 19420123]
Kim SD, Loukas M. Anatomy and variations of digastric muscle. Anatomy & cell biology. 2019 Mar:52(1):1-11. doi: 10.5115/acb.2019.52.1.1. Epub 2019 Mar 29 [PubMed PMID: 30984445]
Choi P, Iwanaga J, Dupont G, Oskouian RJ, Tubbs RS. Clinical anatomy of the nerve to the mylohyoid. Anatomy & cell biology. 2019 Mar:52(1):12-16. doi: 10.5115/acb.2019.52.1.12. Epub 2019 Mar 29 [PubMed PMID: 30984446]
Kawai K, Koizumi M, Honma S, Tokiyoshi A, Kodama K. Derivation of the anterior belly of the digastric muscle receiving twigs from the mylohyoid and facial nerves. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2003 Jan:185(1):85-90 [PubMed PMID: 12597132]
Ohkoshi A, Ogawa T, Sagai S, Nakanome A, Higashi K, Ishii R, Kato K, Katori Y. Simple laryngeal suspension procedure by suturing the digastric muscle to the periosteum of the mandible in neck dissection for tongue cancer. American journal of otolaryngology. 2018 Mar-Apr:39(2):77-81. doi: 10.1016/j.amjoto.2018.01.008. Epub 2018 Jan 31 [PubMed PMID: 29395281]
Gawryszuk A, Bijl HP, Holwerda M, Halmos GB, Wedman J, Witjes MJH, van der Vliet AM, Dorgelo B, Langendijk JA. Functional Swallowing Units (FSUs) as organs-at-risk for radiotherapy. PART 1: Physiology and anatomy. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2019 Jan:130():62-67. doi: 10.1016/j.radonc.2018.10.028. Epub 2018 Nov 9 [PubMed PMID: 30420235]
Kim J, Shin ES, Kim JE, Yoon SP, Kim YS. Neck muscle atrophy and soft-tissue fibrosis after neck dissection and postoperative radiotherapy for oral cancer. Radiation oncology journal. 2015 Dec:33(4):344-9. doi: 10.3857/roj.2015.33.4.344. Epub 2015 Dec 30 [PubMed PMID: 26756035]
Shen SC, Nachalon Y, Randall DR, Nativ-Zeltzer N, Belafsky PC. High elevation training mask as a respiratory muscle strength training tool for dysphagia. Acta oto-laryngologica. 2019 Jun:139(6):536-540. doi: 10.1080/00016489.2019.1605196. Epub 2019 Apr 29 [PubMed PMID: 31035838]
Wada S, Tohara H, Iida T, Inoue M, Sato M, Ueda K. Jaw-opening exercise for insufficient opening of upper esophageal sphincter. Archives of physical medicine and rehabilitation. 2012 Nov:93(11):1995-9. doi: 10.1016/j.apmr.2012.04.025. Epub 2012 May 10 [PubMed PMID: 22579648]
Clement WA, Graham I, Ablett M, Rawlings D, Dempster JH. Intramuscular hemangioma of the posterior belly of the digastric muscle failing to highlight on magnetic resonance imaging. The Annals of otology, rhinology, and laryngology. 2002 Nov:111(11):1050-3 [PubMed PMID: 12450183]
Level 3 (low-level) evidence