Introduction
Dengue is a mosquito-transmitted virus and is the leading cause of arthropod-borne viral disease worldwide, posing a significant global health concern. This disease is also known by various monikers, such as breakbone or 7-day fever, and is characterized by intense muscle spasms, joint pain, and high fever, reflecting both the severity and the duration of symptoms. Although most dengue fever cases are asymptomatic, severe illness and mortality can occur. Aedes mosquitoes, primarily including the female vectors Aedes aegypti and A albopictus, transmit the virus and are common in tropical and subtropical parts of the world.
The incidence of dengue fever has increased dramatically over the past few decades, and the infection is now endemic in some parts of the world, possibly due to increased global travel. Dengue fever poses a significant public health challenge, with over 100 million cases annually and 20 to 25,000 deaths, marked by epidemics across different regions globally. After infection with a subspecies known as dengue hemorrhagic fever (DHF), some individuals previously infected with one subspecies of the dengue virus (DENV) develop severe capillary permeability and bleeding.[1][2][3] Although the symptoms and signs overlap with several viral prodromes, the identifying features are discussed in the next sections.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Dengue fever is caused by any of the 4 distinct serotypes (DENV-1 to DENV-4) of single-stranded RNA viruses belonging to the genus Flavivirus. Infection by one serotype confers lifelong immunity to that serotype but not to others.[4][5][6]
Epidemiology
Dengue fever is the fastest-spreading mosquito-borne viral disease worldwide, affecting over 100 million people annually. This disease also leads to 20 to 25,000 deaths, primarily among children, and is prevalent in more than 100 countries. Epidemics occur yearly in the Americas, Asia, Africa, and Australia.
The dengue virus is maintained by the following 2 transmission cycles:
- Mosquitoes carry the virus from a nonhuman primate to another nonhuman primate
- Mosquitoes transmit the virus from human to human
The human-mosquito cycle primarily occurs in urban environments. Whether the virus transmits from affected humans to mosquitoes depends on the viral load of the mosquitoes' blood meal. The primary vectors of the disease are female mosquitoes of the species Aedes aegypti and Aedes albopictus. Although A aegypti is associated with most infections, the geographic range of A albopictus is expanding. A albopictus, being more cold-tolerant, exhibits aggressive feeding behavior but does so less frequently, which may contribute to its increasing numbers. These mosquito species typically inhabit indoor environments and are active during the day. Modes of transmission include perinatal transmission, blood transfusions, breast milk, and organ transplantation.
Between 1990 and 2010, the mean age of patients was 27.2, which has increased to 34 since 2010. The dengue viral serotype causing disease outbreaks has varied over time, along with the occurrence of severe dengue fever.[7][8] Transmission of the dengue virus generally follows 2 patterns—epidemic dengue and hyperendemic dengue.
Epidemic dengue occurs when a single strain of dengue virus (DENV) is responsible for introduction and transmission, and such epidemics were more common before World War II. During epidemics, all age groups are affected, but the incidence of DHF is relatively low. Hyperendemicity, on the other hand, refers to the co-circulation of various serotypes of DENV in a community linked to periodic outbreaks.[9] In hyperendemic areas, children are affected more than adults, and the incidence of DHF is relatively higher.
Pathophysiology
Belonging to the Flaviviridae family, the dengue virus is a 50-nm virion comprising 3 structural and 7 nonstructural proteins, a lipid envelope, and a 10.7-kb-capped positive-sense single strand of RNA. Infections are asymptomatic in up to 75% of affected individuals. The disease spectrum ranges from self-limiting dengue fever to severe hemorrhage and shock. A fraction of infections, between 0.5% and 5%, develop into severe dengue. Without proper treatment, fatality rates may exceed 20%, particularly among children. The typical incubation period for the disease is 4 to 7 days, with symptoms lasting from 3 to 10 days. Symptoms appearing more than 2 weeks after exposure are unlikely to be attributed to dengue fever.
The consequences of a mosquito bite injecting the dengue virus into the skin remain unclear. Skin macrophages and dendritic cells are believed to be the initial targets. These infected cells are thought to migrate to the lymph nodes and disseminate through the lymphatic system to other organs. Viremia, the presence of the virus in the bloodstream, may occur for 24 to 48 hours before the onset of symptoms.
The presentation of dengue fever, whether asymptomatic, typical, or severe, is influenced by a complex interplay of host and viral factors. Severe dengue fever, characterized by heightened microvascular permeability and shock syndrome, is often associated with infection by a second dengue virus serotype and the patient's immune response. However, severe cases of dengue fever can also arise from infection by a single serotype. Interestingly, microvascular permeability tends to escalate as viral titers decrease.
History and Physical
The 3 phases of dengue fever include febrile, critical, and recovery stages (see Image. Primary Symptoms of Dengue Fever).
The febrile phase: During the febrile phase, individuals typically experience a sudden onset of high-grade fever, reaching approximately 40 °C, which usually lasts for 2 to 7 days. Approximately 6% of cases may exhibit saddleback or biphasic fever, particularly in patients with DHF and severe dengue fever. The fever usually persists for at least 24 hours, followed by a subsequent spike lasting at least 1 more day.[10] Associated symptoms during this phase include facial flushing, skin erythema, myalgias, arthralgias, headache, sore throat, conjunctival injection, anorexia, nausea, and vomiting. Skin erythema manifests as a general blanchable macular rash within 1 to 2 days of fever onset and again on the last day. Alternatively, within 24 hours, a secondary maculopapular rash may develop.
The critical phase: During the critical phase, defervescence marks a period when the temperature typically decreases to approximately 37.5 to 38 °C or lower, occurring between days 3 and 7. This phase is associated with heightened capillary permeability and typically lasts for 1 to 2 days. Before the critical phase, there is often a rapid decline in platelet count, accompanied by increased hematocrit levels. Leukopenia may also occur up to 24 hours before the platelet count drops and warning signs emerge. If left untreated, the critical phase can progress to shock, organ dysfunction, disseminated intravascular coagulation, or hemorrhage.
The recovery phase: The recovery phase involves the gradual reabsorption of extravascular fluid over 2 to 3 days. During this period, patients often exhibit bradycardia.
Expanded dengue virus syndrome refers to unusual or atypical manifestations seen in patients with involvement of various organs such as neurological, hepatic, and renal. This syndrome can be associated with profound shock. Neurological manifestations may include febrile seizures in young children, encephalitis, aseptic meningitis, and intracranial bleeding. Gastrointestinal involvement might present as hepatitis, liver failure, pancreatitis, or acalculous cholecystitis. In addition, this syndrome can manifest as myocarditis, pericarditis, acute respiratory distress syndrome, acute kidney injury, or hemolytic uremic syndrome.
Evaluation
Common laboratory findings include thrombocytopenia, leukopenia, and elevated levels of aspartate aminotransferase. The disease is classified as either dengue or severe dengue.[11][12][13]
- Probable dengue: The patient lives in or has traveled to a Dengue-endemic area. Symptoms include fever and 2 of the following: nausea, vomiting, rash, myalgias, arthralgias, rash, positive tourniquet test, or leukopenia.
- Warning signs of dengue: Dengue symptoms include abdominal pain, persistent vomiting, clinical fluid accumulation such as ascites or pleural effusion, mucosal bleeding, lethargy, liver enlargement greater than 2 cm, increase in hematocrit, and thrombocytopenia.
- Severe dengue: Severe dengue is characterized by dengue fever accompanied by severe plasma leakage, hemorrhage, impaired consciousness, myocardial dysfunction, pulmonary dysfunction, and organ dysfunction, including transaminitis greater than 1000 IU/L.
- Dengue shock syndrome clinical warnings: Symptoms include rapidly rising hematocrit, intense abdominal pain, persistent vomiting, and narrowed or absent blood pressure.
The virus antigen can be detected using enzyme-linked immunosorbent assay (ELISA) test, polymerase chain reaction (PCR), or by isolating the virus from body fluids. Serology typically shows a significant increase in immunoglobulins. A confirmed diagnosis is established through culture, antigen detection, PCR, or serologic testing. Notably, it is crucial to evaluate pregnant patients with dengue carefully, as the symptoms can resemble those of preeclampsia.
Treatment / Management
The treatment approach for dengue fever varies depending on the patient's illness phase. Patients without warning signs can typically be treated as outpatients with acetaminophen and sufficient oral fluids. In addition, educating patients about the warning signs and advising them to seek immediate medical attention if any of these signs occur is important.
Patients presenting with warning signs of the disease, severe dengue fever, or having risk factors such as age, pregnancy status, diabetes mellitus, or those who are living alone should be evaluated for hospitalization. Individuals displaying warning signs can be started on intravenous (IV) crystalloids, with the fluid rate adjusted based on the patient's response. Patients in shock and not responding to initial crystalloid boluses may require colloids.
Blood transfusion is indicated in cases of severe or suspected bleeding when the patient remains unstable despite adequate fluid resuscitation and hematocrit falls. Platelet transfusion may be necessary if the platelet count drops below 20,000 cells per microliter and there is a high risk of bleeding. Notably, it is essential to avoid administering aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), and other anticoagulants. No antiviral medications are recommended, and no laboratory tests can reliably predict the progression to severe disease.
Differential Diagnosis
The clinical diagnosis of dengue fever can be challenging as many other illnesses can present similarly early in the disease course. Other differential diagnoses include measles, influenza, and mosquito-vector diseases such as Zika virus disease, West Nile infection, chikungunya, malaria, and yellow fever (see Image. Mosquito-Borne Diseases).
Obtaining a detailed history of immunizations, travel, and exposures is crucial for the diagnosis of dengue fever. Rapid laboratory identification of the dengue virus involves NS1 antigen detection and serological tests. Serological tests are only helpful after several days of infection and may yield false positives due to other Flavivirus infections, such as yellow fever or Zika virus.
Prognosis
Untreated severe dengue fever may have a mortality rate of 10% to 20%. However, with appropriate supportive care, the mortality rate can be reduced to approximately 1%.
Complications
Complications of dengue fever may include liver injury, cardiomyopathy, pneumonia, orchitis, oophoritis, seizures, encephalopathy, and encephalitis.
Postoperative and Rehabilitation Care
Patients should be encouraged to drink plenty of fluids. The return of appetite in a patient is a sign that the infection is subsiding.
Consultations
Consulting an infectious disease specialist is recommended, as many clinicians have limited experience managing this infection. The Centers for Disease Control and Prevention (CDC) also provides a hotline offering treatment advice.
Deterrence and Patient Education
The only way to avoid contracting dengue virus is to prevent mosquito bites and avoid endemic areas.
Preventative Measures
- Using bed nets from daytime onward.
- Utilizing insecticide-treated materials such as window curtains.
- Applying mosquito-repellant creams containing DEET, IR3535, or icaridin.
- Using mosquito-repellant coils.
- Developing the habit of wearing long-sleeved shirts and pants.[14]
Biological Control
- Fish: Introducing viviparous species of fish, such as Poecilia reticulata, into confined water bodies such as large water tanks or open freshwater wells, and utilizing native larvicidal fish.
- Predatory copepods: Implementing small freshwater crustaceans as effective predators, particularly in specific container habitats.
- Endosymbiotic control: Utilizing mosquitoes infected with Wolbachia, an intracellular parasite, as they demonstrate reduced susceptibility to DENV infection compared to wild-type mosquitoes A aegypti.[15]
Chemical Control
- Using larvicidal in big breeding containers.
- Applying insecticide sprays via space sprays, which can be administered as thermal fogs or cold aerosols.
- Using oil-based formulations, as they inhibit evaporation
- Using a few common insecticides such as organophosphorus compounds (fenitrothion and malathion) and pyrethroids (bioresmethrin and cypermethrin).
Environmental Measures
- Identifying and eliminating the breeding areas of mosquitoes and pests.
- Maintaining the rooftops and sunshades properly.
- Covering stored water in buckets, pots, and other vessels appropriately.
Health Education
Educating individuals about the dengue virus is crucial for effective public health interventions. Utilizing audiovisual and mass awareness campaigns can serve as initial steps in disseminating knowledge about the virus, which can be implemented at both individual and population levels.
Vaccination
CYD-TDV, the first licensed live recombinant tetravalent dengue vaccine, is approved for use in endemic areas across 20 countries.[16]
Enhancing Healthcare Team Outcomes
Diagnosing and managing dengue fever involve a multidisciplinary team of healthcare professionals comprising an infectious disease expert, a CDC consultant, an emergency department clinician, and an internist. Treatment primarily focuses on supportive care, including fluid repletion, acetaminophen for fever management, and blood transfusion if hemorrhage occurs. A confirmed diagnosis is established through various methods such as culture, antigen detection, polymerase chain reaction, or serologic testing.
Laboratory tests cannot reliably predict the progression to severe disease. Primary care clinicians and nurse practitioners play a crucial role in educating travelers on preventing mosquito bites and adopting preventive measures such as covering their exposed skin, using bed nets, mosquito repellents, and indoor insecticides, as well as eliminating mosquito breeding grounds such as standing water. While the prognosis for untreated dengue fever is poor, most patients can survive with supportive care, although some may experience residual multisystem organ damage.[17][18]
Media
(Click Image to Enlarge)
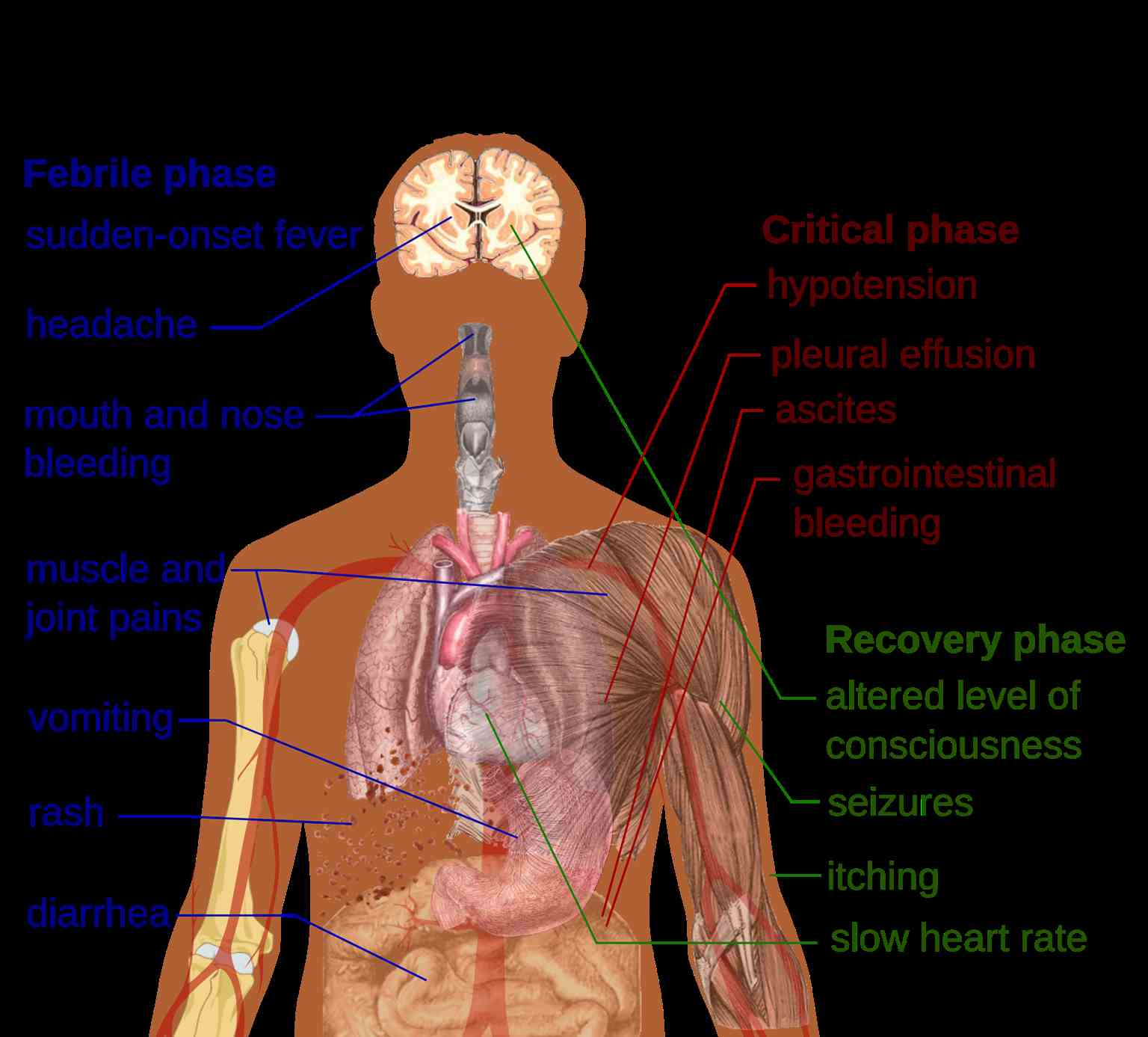
Primary Symptoms of Dengue Fever. The symptoms of dengue fever are multisystemic and encompass 3 distinct phases: febrile, critical, and recovery.
Mikael Häggström, Public Domain, via Wikimedia Commons.
{kind=link}
(Click Image to Enlarge)
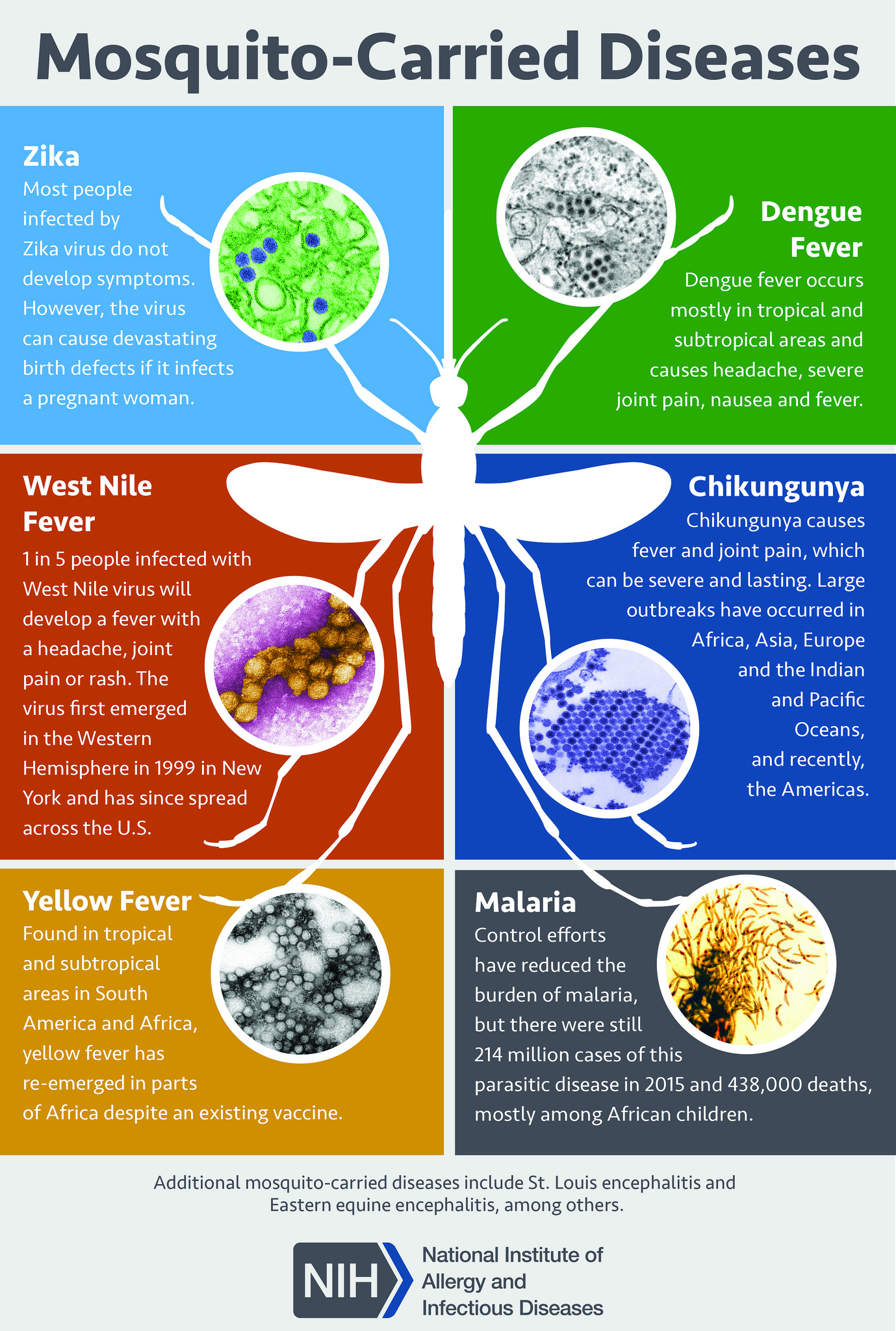
Mosquito-Borne Diseases. Mosquitoes are carriers of various diseases, including Zika, dengue fever, West Nile fever, chikungunya, yellow fever, and malaria.
National Institute of Allergy and Infectious Diseases, National Institutes of Health
References
Baak-Baak CM, Cigarroa-Toledo N, Pech-May A, Cruz-Escalona GA, Cetina-Trejo RC, Tzuc-Dzul JC, Talavera-Aguilar LG, Flores-Ruiz S, Machain-Williams C, Torres-Chable OM, Blitvich BJ, Mendez-Galvan J, Garcia-Rejon JE. Entomological and virological surveillance for dengue virus in churches in Merida, Mexico. Revista do Instituto de Medicina Tropical de Sao Paulo. 2019 Feb 14:61():e9. doi: 10.1590/S1678-9946201961009. Epub 2019 Feb 14 [PubMed PMID: 30785563]
Sharma M, Glasner DR, Watkins H, Puerta-Guardo H, Kassa Y, Egan MA, Dean H, Harris E. Magnitude and Functionality of the NS1-Specific Antibody Response Elicited by a Live-Attenuated Tetravalent Dengue Vaccine Candidate. The Journal of infectious diseases. 2020 Mar 2:221(6):867-877. doi: 10.1093/infdis/jiz081. Epub [PubMed PMID: 30783676]
Oliveira LNDS, Itria A, Lima EC. Cost of illness and program of dengue: A systematic review. PloS one. 2019:14(2):e0211401. doi: 10.1371/journal.pone.0211401. Epub 2019 Feb 20 [PubMed PMID: 30785894]
Level 1 (high-level) evidenceSeixas G, Salgueiro P, Bronzato-Badial A, Gonçalves Y, Reyes-Lugo M, Gordicho V, Ribolla P, Viveiros B, Silva AC, Pinto J, Sousa CA. Origin and expansion of the mosquito Aedes aegypti in Madeira Island (Portugal). Scientific reports. 2019 Feb 19:9(1):2241. doi: 10.1038/s41598-018-38373-x. Epub 2019 Feb 19 [PubMed PMID: 30783149]
Ghani NA, Shohaimi S, Hee AK, Chee HY, Emmanuel O, Alaba Ajibola LS. Comparison of Knowledge, Attitude, and Practice among Communities Living in Hotspot and Non-Hotspot Areas of Dengue in Selangor, Malaysia. Tropical medicine and infectious disease. 2019 Feb 15:4(1):. doi: 10.3390/tropicalmed4010037. Epub 2019 Feb 15 [PubMed PMID: 30781369]
Maia LMS, Bezerra MCF, Costa MCS, Souza EM, Oliveira MEB, Ribeiro ALM, Miyazaki RD, Slhessarenko RD. Natural vertical infection by dengue virus serotype 4, Zika virus and Mayaro virus in Aedes (Stegomyia) aegypti and Aedes (Stegomyia) albopictus. Medical and veterinary entomology. 2019 Sep:33(3):437-442. doi: 10.1111/mve.12369. Epub 2019 Feb 18 [PubMed PMID: 30776139]
Prompetchara E, Ketloy C, Thomas SJ, Ruxrungtham K. Dengue vaccine: Global development update. Asian Pacific journal of allergy and immunology. 2020 Sep:38(3):178-185. doi: 10.12932/AP-100518-0309. Epub [PubMed PMID: 30660171]
Vasanthapuram R, Shahul Hameed SK, Desai A, Mani RS, Reddy V, Velayudhan A, Yadav R, Jain A, Saikia L, Borthakur AK, Mohan DG, Bandyopadhyay B, Bhattacharya N, Dhariwal AC, Sen PK, Venkatesh S, Prasad J, Laserson K, Srikantiah P. Dengue virus is an under-recognised causative agent of acute encephalitis syndrome (AES): Results from a four year AES surveillance study of Japanese encephalitis in selected states of India. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2019 Jul:84S():S19-S24. doi: 10.1016/j.ijid.2019.01.008. Epub 2019 Jan 11 [PubMed PMID: 30641206]
Gubler DJ. The global emergence/resurgence of arboviral diseases as public health problems. Archives of medical research. 2002 Jul-Aug:33(4):330-42 [PubMed PMID: 12234522]
Level 3 (low-level) evidenceNg DH, Wong JG, Thein TL, Leo YS, Lye DC. The Significance of Prolonged and Saddleback Fever in Hospitalised Adult Dengue. PloS one. 2016:11(12):e0167025. doi: 10.1371/journal.pone.0167025. Epub 2016 Dec 9 [PubMed PMID: 27936002]
Nguyen-Tien T, Probandari A, Ahmad RA. Barriers to Engaging Communities in a Dengue Vector Control Program: An Implementation Research in an Urban Area in Hanoi City, Vietnam. The American journal of tropical medicine and hygiene. 2019 Apr:100(4):964-973. doi: 10.4269/ajtmh.18-0411. Epub [PubMed PMID: 30652660]
Wharton-Smith A, Green J, Loh EC, Gorrie A, Omar SFS, Bacchus L, Lum LCS. Using clinical practice guidelines to manage dengue: a qualitative study in a Malaysian hospital. BMC infectious diseases. 2019 Jan 11:19(1):45. doi: 10.1186/s12879-019-3680-5. Epub 2019 Jan 11 [PubMed PMID: 30634929]
Level 2 (mid-level) evidenceKellstein D, Fernandes L. Symptomatic treatment of dengue: should the NSAID contraindication be reconsidered? Postgraduate medicine. 2019 Mar:131(2):109-116. doi: 10.1080/00325481.2019.1561916. Epub 2019 Jan 16 [PubMed PMID: 30575425]
. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition. 2009:(): [PubMed PMID: 23762963]
Flores HA, Taneja de Bruyne J, O'Donnell TB, Tuyet Nhu V, Thi Giang N, Thi Xuan Trang H, Thi Thuy Van H, Thi Long V, Thi Dui L, Le Anh Huy H, Thi Le Duyen H, Thi Van Thuy N, Thanh Phong N, Van Vinh Chau N, Thi Hue Kien D, Thuy Vi T, Wills B, O'Neill SL, Simmons CP, Carrington LB. Multiple Wolbachia strains provide comparative levels of protection against dengue virus infection in Aedes aegypti. PLoS pathogens. 2020 Apr:16(4):e1008433. doi: 10.1371/journal.ppat.1008433. Epub 2020 Apr 13 [PubMed PMID: 32282862]
Level 2 (mid-level) evidenceTricou V, Sáez-Llorens X, Yu D, Rivera L, Jimeno J, Villarreal AC, Dato E, Saldaña de Suman O, Montenegro N, DeAntonio R, Mazara S, Vargas M, Mendoza D, Rauscher M, Brose M, Lefevre I, Tuboi S, Borkowski A, Wallace D. Safety and immunogenicity of a tetravalent dengue vaccine in children aged 2-17 years: a randomised, placebo-controlled, phase 2 trial. Lancet (London, England). 2020 May 2:395(10234):1434-1443. doi: 10.1016/S0140-6736(20)30556-0. Epub 2020 Mar 17 [PubMed PMID: 32197107]
Level 1 (high-level) evidenceNujum ZT, Saritha N, Prathibha Raj MR, Gayathri AV, Nirmala C, Vijayakumar K, Varghese S. Seroprevalence of dengue infection in pregnant women and placental antibody transfer. Medical journal, Armed Forces India. 2019 Jan:75(1):90-95. doi: 10.1016/j.mjafi.2018.08.009. Epub 2018 Oct 25 [PubMed PMID: 30705485]
Gordon A, Gresh L, Ojeda S, Katzelnick LC, Sanchez N, Mercado JC, Chowell G, Lopez B, Elizondo D, Coloma J, Burger-Calderon R, Kuan G, Balmaseda A, Harris E. Prior dengue virus infection and risk of Zika: A pediatric cohort in Nicaragua. PLoS medicine. 2019 Jan:16(1):e1002726. doi: 10.1371/journal.pmed.1002726. Epub 2019 Jan 22 [PubMed PMID: 30668565]