Introduction
Cylindromas, or cutaneous cylindromas, are rare, distinct adnexal neoplasms characterized by a dual lineage proliferation of cells nestled within the dermis.[1][2] These neoplasms are predominantly derived from likely apocrine cells in the dermis within the hair follicle bulge. Upon cross-sectional examination, cylindromas exhibit a round morphology akin to cylinders, hence their nomenclature, reflecting their cylindrical shape. Although cylindromas are typically slow-growing and manifest as diminutive entities, they are generally benign. However, exceedingly rare instances of malignant transformation and potential metastases have been reported, especially in conjunction with multiple lesions associated with Brooke-Spiegler syndrome.[3]
Cylindromas are slow-growing lesions primarily found on the scalp or face of individuals. They exhibit a marked predilection toward females, occurring approximately 9 times more frequently than males.[4] Notably, when multiple cutaneous cylindromas congregate on the scalp, they can amalgamate, creating an appearance reminiscent of headgear like a hat or turban, giving rise to the previously more common term “turban tumor,” which is no longer used due to its negative connotation.[5][6] Recognizing the intricate association between cylindromas and spiradenomas is imperative, as they share close ties and are associated with various genetic syndromes characterized by undifferentiated neoplasms stemming from apocrine lineage.[7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Cylindromas may occur either sporadically or in a familial manner, and they are generally not attributed to environmental factors. Sporadic occurrences typically involve solitary lesions.[4] Unlike in familial inherited forms, there is often an expression of MYB-NFIB fusion transcripts in sporadically occurring cylindromas. MYB, an oncogene, fuses with NFIB to form a transcription factor gene, resulting in an oncoprotein that promotes neoplastic processes.[8] MYB, when activated or overexpressed, can drive dermal cylindromas by assuming the role typically performed by the MYB-NFIB fusion oncoprotein.[8]
Familial cylindromatosis syndromes are associated with mutations in the CYLD tumor-suppressor gene, except for rare exceptions. The CYLD gene was discovered in 2000 and implicated as the causal agent in the 3 inherited cylindromatosis syndromes.[4] Of these syndromes, Brooke-Spiegler syndrome is probably the most well-known.[4] Familial cylindromatosis and multiple familial trichoepitheliomas are the other 2 inheritable cylindromatosis syndromes and involve mutations in the CYLD gene. CYLD mutations are inherited in an autosomal dominant pattern but adhere to the 2-hit hypotheses. This necessitates a second gene mutation to occur randomly due to DNA damage to induce a neoplastic change.[9]
Although the CYLD mutation follows an autosomal dominant pattern, the phenotypic expression of these mutations varies considerably. With ongoing discoveries, over 100 mutations have been identified in the CYLD gene. The most prevalent mutation occurs on chromosome 16q. However, it remains unclear which mutations will influence specific phenotypic expressions. Even within the same family, affected members often display differing phenotypes.[10][11][12][13]
Epidemiology
Cutaneous cylindromas are rare occurrences that disproportionately affect females, occurring nine times more frequently than males, and are more prevalent in Caucasian populations.[8] When present as solitary lesions, they typically belong to the sporadic type. Sporadic forms are more commonly observed in older patients. However, in some cases, they may manifest in the second or third decade of life with multiple lesions, often associated with cutaneous syndromes such as Brooke-Spiegler syndrome.[8]
In these syndromes, cylindromas are also epidemiologically associated with similar tumors, including spiradenomas, trichoepitheliomas, and salivary gland tumors, such as parotid tumors.[8] Often in these genetic syndromes, the tumors develop around puberty and can continue through adulthood, with additional lesions developing across the body, although the scalp remains the most common location.[8] Solitary lesions, usually found in older adults, are less likely to be related to a syndrome, whereas multiple lesions are more likely to be syndromic and often manifest at an earlier age.[10][11]
Pathophysiology
The pathogenesis of cylindromas is not yet well understood, and there are multiple theories regarding its origin.[14] A follicular epithelium lineage is often defended as the tumor develops exclusively in hair-covered areas.[15] The cells within the cylindroma also have exhibited expression of follicular keratin.[1] However, many experts maintain that this neoplasm's origins are eccrine or apocrine differentiation, although some cytologic studies argue against the eccrine origin.[1] Cylindromas do not develop on palmar or plantar surfaces, which contradicts an eccrine lineage hypothesis, as these areas contain numerous eccrine glands but lack hair follicles or apocrine glands. The more differentiated cells forming cylindromas exhibit morphological similarities to secretory cells, leading some to argue for the apocrine origin of these neoplasms.[16][17]
Histopathology
Cylindromas are classically described as variably sized rounded islands of basaloid cells that are arranged together in a fashion reminiscent of a jigsaw puzzle (see Image. Cylindroma).[18] These islands are mostly contained within the dermis, but also often extend into the subcutis. These islands should not connect to the overlying epidermis. The islands are composed of 2 cell populations, with a palisading peripheral lining of smaller cells with more hyperchromatic nuclei and an inner population in the islands with larger, more differentiated pale cells and nuclei and small duct-like structures.[19] These islands are surrounded by an interconnecting hyalinized sheath that looks like a thickened, dense pink lining. Within these basaloid islands, interspersed small round pink globules, or hyaline droplets, are often seen.[5][6]
History and Physical
Solitary lesions, which are usually sporadic and not familial, present as slow-growing, painless, round nodular lesions.[8] They are sometimes pedunculated. Solitary lesions usually occur in older populations and do not usually grow larger than one centimeter.[8] They are rarely painful or tender and may have a pinkish or tan coloring with a smooth surface. Small superficial blood vessels may be visualized. These lesions are most likely to occur on the scalp, and they are seen across the head and neck, with some reports showing the development of these lesions in the nasal area or along ducts, such as the parotid duct; importantly, however, there are reports of these lesions on the trunk and other areas on the body related to apocrine ductal differentiation, which is the presumed source of these neoplastic cells.[8][20][21]
Multiple cylindromas will usually occur in the setting of a familial syndrome and develop much earlier in life.[8] When occurring in multiples, these lesions require excisions for treatment and re-excisions later in life as they can recur or progress into malignancies.[22] Also, in syndromic patients, the cylindromas may exhibit accelerated growth and reach sizes over 20 centimeters in some cases. As they grow this large, they often will ulcerate and become painful.[23]
Ninety percent of cylindromas occur in the head and neck region.[8] They also can occur on the trunk and extremities, but the palms and soles are spared. A family history of multiple cylindromas should be helpful in aiding the diagnosis. Environmental factors have not been implicated in the development of these lesions.[16][17][24][17][25] The development of multiple lesions should be cautiously suggestive of Brooke-Spiegler syndrome, an autosomal dominant condition involving mutations in the CYLD gene causing multiple tumors.[26]
Evaluation
Tumors typically originate on the scalp and face but may also appear on the torso and sun-protected areas, such as the genital and axillary skin, necessitating further evaluation.[20][27] A minority of individuals may develop salivary gland tumors.[20] In rare instances, pulmonary cylindromas may develop in large airways, potentially compromising breathing.[28] Although these tumors are usually benign, malignant transformation is recognized.[29]
A biopsy of a lesion consistent with a diagnosis of cylindroma will show multiple circumscribed nodules in the dermis or subcutis, each of which has multiple basaloid nests that together will form the classic jigsaw puzzle appearance.[30] Usually, there can also be an eosinophilic basement membrane enveloping the jigsaw puzzle.[31]
Radiological examinations may be useful to identify the extent of the lesions as they have been known to involve underlying osseous structures, and some lesions are quite vascular. These features are important to consider when planning treatment, particularly as these lesions may also be associated with parotid neoplasms.[32] Genetic testing for mutations in the CYLD cylindromatosis gene and familial studies should be performed in patients suspected of cylindromatosis syndrome.[13][16][17]
Treatment / Management
Treatment options include excision, laser ablation, and cryotherapy. Excision is the preferred treatment and is usually curative.[33] Local recurrence has been documented but is rare.[33] Large lesions should be imaged before planning treatment to determine vascularity and involvement of surrounding tissues, including underlying osseous structures. Pretreatment embolization is vital in patients with large and multiple cylindromas to minimize intraoperative blood loss, as they can be quite vascular lesions. Topical aspirin has been utilized to prevent recurrence after excision. Excision and histopathologic examination, along with clinical correlation, should lead to the correct diagnosis.[25][34](B3)
Differential Diagnosis
Trichoepitheliomas and spiradenomas appear similar and often occur simultaneously. Trichoepitheliomas are differentiated from cylindromas by the presence of horn cysts.[29] Spiradenomas can prove exceedingly difficult to differentiate from cylindromas in some cases. Within a spiradenoma, populations of basaloid cells may appear indistinguishable from a cylindroma.[35] They will often appear more circumscribed and nodular than cylindromas. Spiradenomas are typically solitary lesions that often exhibit intermittent pain and are tender to palpation, as opposed to the majority of cylindromas, which are painless. A thorough histopathological examination of the entire lesion is vital under challenging cases to differentiate between cylindromas and spiradenomas.[36]
Cylindromas may transform into malignant versions in rare cases.[33] Malignant cylindromas are more frequently associated with Brooke-Spiegler Syndrome. The malignant form exhibits more rapid growth, atypical and asymmetrical architectural features, and an invasive pattern of growth.[29] Cytological features may include nuclear pleomorphism and crowding, loss of the characteristic jigsaw puzzle pattern, loss of intervening hyaline sheaths, loss of the biphasic cell population, and development of necrosis. Malignant cylindromas exhibit aggressive local infiltrative growth patterns and have been known to metastasize. Immunohistochemical stains do not help differentiate between benign or malignant lesions.[13][16]
Prognosis
Although cylindromas are generally benign lesions, a rare subset may undergo malignant transformation.[37] Additionally, there have been documented cases where cylindromas evolved into adenoid cystic carcinoma or spread to hazardous sites, such as malignant nasal cylindroma, or invasion into the lacrimal sac.[9] Malignant cylindromas are more commonly associated with Brooke-Spiegler Syndrome. The malignant variant typically demonstrates rapid growth, atypical and asymmetrical architectural features, and an invasive growth pattern.[37]
Cytological features of malignant cylindromas may include nuclear pleomorphism and crowding, loss of the characteristic jigsaw puzzle pattern, loss of intervening hyaline sheaths, loss of the biphasic cell population, and the development of necrosis.[37] Malignant cylindromas demonstrate aggressive local infiltrative growth patterns and have been known to metastasize. Immunohistochemical stains do not aid in differentiating between benign and malignant lesions.[13][16]
Complications
Complications associated with cylindromas typically arise from surgical intervention and include bleeding, scarring, recurrence, pain, and the potential necessity for further procedures. In familial cases, where lesions may be large and multiple, there could be disfigurement or pain. However, most studies suggest a low post-removal recurrence rate, indicating that the lesions tend not to recur once excised.[38]
Deterrence and Patient Education
Patients presenting with multiple cylindromas should be referred for genetic counseling and testing, as they may have Brooke-Spiegler syndrome.
Enhancing Healthcare Team Outcomes
Although cylindromas are typically benign and slow-growing, they can cause discomfort to the patient, warranting excision. Rarely, in patients with Brooke-Spiegler syndrome, they may undergo malignant transformation. Therefore, patients with multiple cylindromas should be referred for genetic counseling to assess the possibility of having Brooke-Spiegler syndrome.[13][39][40]
Media
(Click Image to Enlarge)
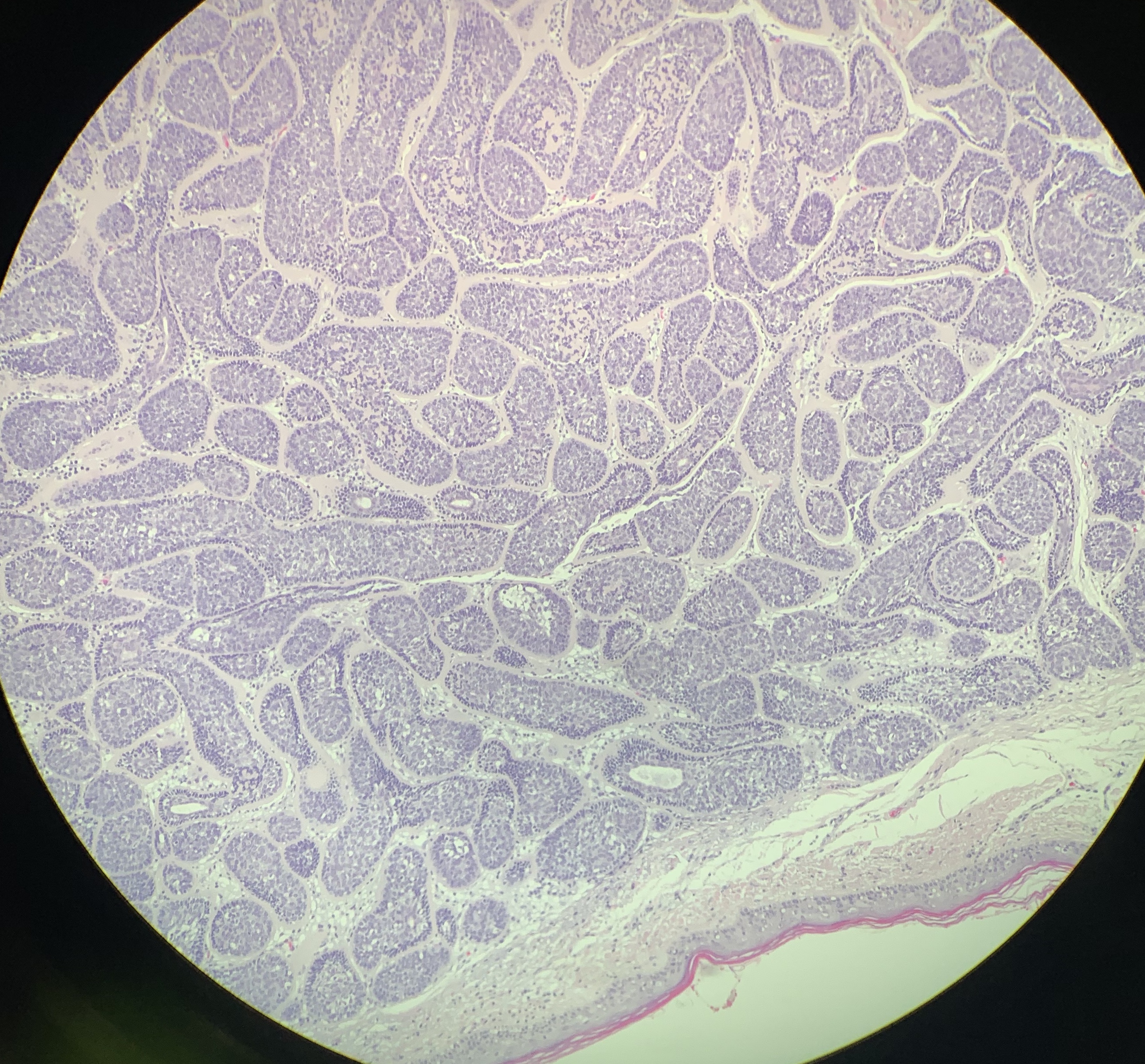
Cylindroma. A photomicrograph displays the histopathological pattern of cylindroma, characterized by variably sized, cylindrical, rounded islands of basaloid cells nestled within the dermis, forming a pattern resembling a jigsaw puzzle.
Contributed by D Myers, MD
References
Sellheyer K. Spiradenoma and cylindroma originate from the hair follicle bulge and not from the eccrine sweat gland: an immunohistochemical study with CD200 and other stem cell markers. Journal of cutaneous pathology. 2015 Feb:42(2):90-101. doi: 10.1111/cup.12406. Epub 2014 Nov 24 [PubMed PMID: 25354097]
Mahalingam M, Srivastava A, Hoang MP. Expression of stem-cell markers (cytokeratin 15 and nestin) in primary adnexal neoplasms-clues to etiopathogenesis. The American Journal of dermatopathology. 2010 Dec:32(8):774-9. doi: 10.1097/DAD.0b013e3181dafd8c. Epub [PubMed PMID: 20700038]
Jordão C, de Magalhães TC, Cuzzi T, Ramos-e-Silva M. Cylindroma: an update. International journal of dermatology. 2015 Mar:54(3):275-8. doi: 10.1111/ijd.12600. Epub 2014 Dec 16 [PubMed PMID: 25515269]
Löser C, Rütten A, Dippel E. [Cylindromas-rare but striking]. Der Hautarzt; Zeitschrift fur Dermatologie, Venerologie, und verwandte Gebiete. 2019 Sep:70(9):677-683. doi: 10.1007/s00105-019-4458-9. Epub [PubMed PMID: 31428801]
Albores-Saavedra J, Heard SC, McLaren B, Kamino H, Witkiewicz AK. Cylindroma (dermal analog tumor) of the breast: a comparison with cylindroma of the skin and adenoid cystic carcinoma of the breast. American journal of clinical pathology. 2005 Jun:123(6):866-73 [PubMed PMID: 15899777]
Chauhan DS, Guruprasad Y. Dermal cylindroma of the scalp. National journal of maxillofacial surgery. 2012 Jan:3(1):59-61. doi: 10.4103/0975-5950.102163. Epub [PubMed PMID: 23251061]
Level 3 (low-level) evidenceRevis P, Chyu J, Medenica M. Multiple eccrine spiradenoma: case report and review. Journal of cutaneous pathology. 1988 Aug:15(4):226-9 [PubMed PMID: 2846662]
Level 3 (low-level) evidenceAdam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, Dubois A, Rajan N. CYLD Cutaneous Syndrome. GeneReviews(®). 1993:(): [PubMed PMID: 32298062]
Schittkowski M, Stropahl G, Timm A, Guthoff R. [Nasolacrimal duct obstruction caused by a cylindroma. Report of an atypical tumor manifestation and review of the literature]. Klinische Monatsblatter fur Augenheilkunde. 2002 Aug:219(8):602-8 [PubMed PMID: 12353178]
Level 3 (low-level) evidenceDubois A, Hodgson K, Rajan N. Understanding Inherited Cylindromas: Clinical Implications of Gene Discovery. Dermatologic clinics. 2017 Jan:35(1):61-71. doi: 10.1016/j.det.2016.08.002. Epub [PubMed PMID: 27890238]
Level 3 (low-level) evidenceDhir G, Makkar M, Suri V, Dubey V. Familial dermal eccrine cylindromatosis with emphasis on histology and genetic mapping. Annals of medical and health sciences research. 2013 Nov:3(Suppl 1):S3-6. doi: 10.4103/2141-9248.121207. Epub [PubMed PMID: 24349843]
Level 3 (low-level) evidenceRajan N, Andersson MK, Sinclair N, Fehr A, Hodgson K, Lord CJ, Kazakov DV, Vanecek T, Ashworth A, Stenman G. Overexpression of MYB drives proliferation of CYLD-defective cylindroma cells. The Journal of pathology. 2016 Jun:239(2):197-205. doi: 10.1002/path.4717. Epub 2016 Apr 21 [PubMed PMID: 26969893]
Borik L, Heller P, Shrivastava M, Kazlouskaya V. Malignant cylindroma in a patient with Brooke-Spiegler syndrome. Dermatology practical & conceptual. 2015 Apr:5(2):61-5. doi: 10.5826/dpc.0502a09. Epub 2015 Apr 30 [PubMed PMID: 26114054]
Rajan N, Burn J, Langtry J, Sieber-Blum M, Lord CJ, Ashworth A. Transition from cylindroma to spiradenoma in CYLD-defective tumours is associated with reduced DKK2 expression. The Journal of pathology. 2011 Jul:224(3):309-21. doi: 10.1002/path.2896. Epub 2011 May 19 [PubMed PMID: 21598248]
Corda G, Sala A. Cutaneous cylindroma: it's all about MYB. The Journal of pathology. 2016 Aug:239(4):391-3. doi: 10.1002/path.4746. Epub 2016 Jul 11 [PubMed PMID: 27185061]
Son JH, Choi YW, Cho YS, Byun YS, Chung BY, Cho HJ, Kim HO, Park CW. A Case of Eccrine Spiradenoma: A Rarely Seen Soft Tissue Tumor on the Extensor Surface of Arm. Annals of dermatology. 2017 Aug:29(4):519-522. doi: 10.5021/ad.2017.29.4.519. Epub 2017 Jun 21 [PubMed PMID: 28761313]
Level 3 (low-level) evidenceMassoumi R, Podda M, Fässler R, Paus R. Cylindroma as tumor of hair follicle origin. The Journal of investigative dermatology. 2006 May:126(5):1182-4 [PubMed PMID: 16484982]
Level 3 (low-level) evidenceGupta P, Dey P, Bal A. Fine needle aspiration cytology of dermal cylindroma. Journal of cytology. 2014 Oct-Dec:31(4):213-4. doi: 10.4103/0970-9371.151137. Epub [PubMed PMID: 25745290]
Level 3 (low-level) evidenceKaushik S, Siegel D, Niermann K, Newman N. Whole Scalp Radiation Therapy for Recurrent Benign Cylindromas. Case reports in dermatology. 2022 May-Aug:14(2):132-137. doi: 10.1159/000524012. Epub 2022 May 30 [PubMed PMID: 35813839]
Level 3 (low-level) evidenceKhoury E, Godfrey M, Yeoh CC. Gynaecological cylindroma in association with CYLD gene mutation. Oxford medical case reports. 2022 Jan:2022(1):omab139. doi: 10.1093/omcr/omab139. Epub 2022 Jan 24 [PubMed PMID: 35083054]
Level 2 (mid-level) evidenceCasale F, Elwood HR, Tchanque-Fossuo CN. Exophytic growth on nasal ala. JAAD case reports. 2022 Jan:19():48-50. doi: 10.1016/j.jdcr.2021.10.035. Epub 2021 Nov 17 [PubMed PMID: 34917724]
Level 3 (low-level) evidenceWatanabe Y, Mori T, Makino T, Yamamoto T. Giant Vascular Cylindroma in a Case of Brooke-Spiegler Syndrome. Indian dermatology online journal. 2022 Nov-Dec:13(6):792-793. doi: 10.4103/idoj.idoj_33_22. Epub 2022 Oct 12 [PubMed PMID: 36386726]
Level 3 (low-level) evidenceBargiel J, Wyszyńska-Pawelec G, Gontarz M, Gąsiorowski K, Marecik T, Szczurowski P, Zapała J. Turban Tumor Syndrome: In Search of a Gold Standard - A Case Report. Skin appendage disorders. 2021 Jun:7(4):326-328. doi: 10.1159/000514855. Epub 2021 Mar 30 [PubMed PMID: 34307484]
Level 3 (low-level) evidenceNair SP. Soft pink nodules on the scalp. Indian dermatology online journal. 2015 Sep-Oct:6(5):373-4. doi: 10.4103/2229-5178.164473. Epub [PubMed PMID: 26500882]
Manicketh I, Singh R, Ghosh PK. Eccrine cylindroma of the face and scalp. Indian dermatology online journal. 2016 May-Jun:7(3):203-5. doi: 10.4103/2229-5178.182355. Epub [PubMed PMID: 27294061]
Luo YY, Chen DG, Ji PZ, Liu B, Yang YL. [Brooke-Spiegler syndrome: report of a case]. Zhonghua bing li xue za zhi = Chinese journal of pathology. 2022 Mar 8:51(3):253-255. doi: 10.3760/cma.j.cn112151-20211228-00939. Epub [PubMed PMID: 35249296]
Level 3 (low-level) evidenceVasenina V, Cibull T, Stadlan N. Brooke-Spiegler Syndrome With Cervical Spine Lesion. Cureus. 2020 Oct 16:12(10):e10982. doi: 10.7759/cureus.10982. Epub 2020 Oct 16 [PubMed PMID: 33209538]
Davies HR, Hodgson K, Schwalbe E, Coxhead J, Sinclair N, Zou X, Cockell S, Husain A, Nik-Zainal S, Rajan N. Epigenetic modifiers DNMT3A and BCOR are recurrently mutated in CYLD cutaneous syndrome. Nature communications. 2019 Oct 17:10(1):4717. doi: 10.1038/s41467-019-12746-w. Epub 2019 Oct 17 [PubMed PMID: 31624251]
Merlo G, Pesce M, Borra T, Orejuela I, Pasquali F, Panizza R, Ghiglione M, Grosso F. Malignant eccrine spiradenocylindroma and parotid gland involvement in Brooke Spiegler syndrome. Dermatology reports. 2022 Sep 14:14(3):9418. doi: 10.4081/dr.2022.9418. Epub 2022 Jan 26 [PubMed PMID: 36199911]
Pal S, Bose K, Sikder M, Chowdhury M. Fine needle aspiration cytology of cylindroma of scalp: A case report. Diagnostic cytopathology. 2016 Dec:44(12):1082-1084. doi: 10.1002/dc.23546. Epub 2016 Jul 26 [PubMed PMID: 27456213]
Level 3 (low-level) evidenceKacerovska D, Szepe P, Vanecek T, Nemcova J, Michal M, Mukensnabl P, Kazakov DV. Spiradenocylindroma-like basaloid carcinoma of the anus and rectum: case report, including HPV studies and analysis of the CYLD gene mutations. The American Journal of dermatopathology. 2008 Oct:30(5):472-6. doi: 10.1097/DAD.0b013e31817fb37f. Epub [PubMed PMID: 18806492]
Level 3 (low-level) evidenceKalina P, El-Azhary R. Brooke-spiegler syndrome with multiple scalp cylindromas and bilateral parotid gland adenomas. Case reports in radiology. 2012:2012():249583. doi: 10.1155/2012/249583. Epub 2012 Feb 12 [PubMed PMID: 22606564]
Level 3 (low-level) evidenceKim KE, Jeong JY, Park TJ, Kim IH. A Case of Malignant Transformation of Solitary Recurrent Cylindroma on Scalp. Annals of dermatology. 2022 Dec:34(6):478-481. doi: 10.5021/ad.20.118. Epub [PubMed PMID: 36478431]
Level 3 (low-level) evidenceNath AK, Udayashankar C. Multiple facial cylindromas: a case report. Dermatology online journal. 2012 Feb 15:18(2):8 [PubMed PMID: 22398229]
Level 3 (low-level) evidenceHerzum A, Russo R, Cozzani E, Paudice M, Guadagno A, Parodi A. Multiple rubbery nodules on the scalp. JAAD case reports. 2021 Feb:8():80-82. doi: 10.1016/j.jdcr.2020.12.023. Epub 2021 Jan 5 [PubMed PMID: 33532532]
Level 3 (low-level) evidenceThomas LW, Pham CT, Coakley B, Lee P. Treatment of Brooke-Spiegler Syndrome Trichoepitheliomas with Erbium: Yttrium-Aluminum-Garnet Laser: A Case Report and Review of the Literature. The Journal of clinical and aesthetic dermatology. 2020 Jul:13(7):41-44 [PubMed PMID: 32983336]
Level 3 (low-level) evidenceIyer PV, Leong AS. Malignant dermal cylindromas. Do they exist? A morphological and immunohistochemical study and review of the literature. Pathology. 1989 Oct:21(4):269-74 [PubMed PMID: 2483749]
Level 3 (low-level) evidenceSingh DD, Naujoks C, Depprich R, Schulte KW, Jankowiak F, Kübler NR, Handschel J. Cylindroma of head and neck: review of the literature and report of two rare cases. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2013 Sep:41(6):516-21. doi: 10.1016/j.jcms.2012.11.016. Epub 2012 Dec 21 [PubMed PMID: 23260808]
Level 3 (low-level) evidenceMogaddam MR, Maleki N. Cylindroma of the scalp. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 2015 Sep:20(9):923-4. doi: 10.4103/1735-1995.170638. Epub [PubMed PMID: 26759583]
Sicinska J, Rakowska A, Czuwara-Ladykowska J, Mroz A, Lipinski M, Nasierowska-Guttmejer A, Sikorska J, Sklinda K, Slowinska M, Kowalska-Oledzka E, Walecka I, Walecki J, Rudnicka L. Cylindroma transforming into basal cell carcinoma in a patient with Brooke-Spiegler syndrome. Journal of dermatological case reports. 2007 Dec 29:1(1):4-9. doi: 10.3315/jdcr.2007.1.1002. Epub [PubMed PMID: 21886698]
Level 3 (low-level) evidence