Introduction
Cryptococcus is an invasive fungus that causes cryptococcosis an infection commonly associated with immunosuppressive individuals while being rare in healthy individuals. The two species of Cryptococcus that are commonly associated with infections in humans are Cryptococcus neoformans and Cryptococcus gatti. The organism is widely prevalent in certain regions of the world. However, the most common forms of exposure include a history of exposure to soil, bird droppings.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Cryptococcal species are fungal pathogens which are encapsulated yeasts morphologically. Immune suppression is the major underlying mechanism that is involved in the causation of cryptococcal disease. Diseases like AIDS, diabetes, chronic liver disease, chronic renal disease, prolonged use of steroids and patients who undergo organ transplantation are commonly associated with the development of cryptococcal disease.[1]
Epidemiology
Globally approximately 1 million cases of cryptococcosis are reported each year resulting in 625,000 deaths approximately.[2] In the United States incidence of cryptococcosis is estimated to be about 0.4-1.3 cases per 100,000 population and 2-7 cases per 100,000 in people affected with AIDS with a case fatality ratio of about 12%. [3]The incidence of cryptococcal infections has declined drastically over the last two decades owing to advances in the anti-retroviral therapy. Cryptococcus neoformans is usually associated with infections in immunocompromised patients while Cryptococcus gatti is associated with infections in immunocompetent patients.
Pathophysiology
Cryptococcus fungi are commonly found in soil contaminated by bird droppings and in decaying wood and in tree hollows. The capsule of the fungus comprises polysaccharides glucuronoxylomannan and glucuronoxylomannogalactan which are the major factors contributing to the virulence of pathogen.[4] Infection usually occurs through inhalation of spores from the environment. The initial infection is mostly asymptomatic and is contained in healthy individuals. Spread of the disease from initial site of infection occurs through hematogenous dissemination in patients who are immune suppressed. Another mechanism through which the infection can develop is reactivation of the organism at the initial site of infection after several years when the patient becomes immunocompromised. [5]
Histopathology
They are facultative intracellular organisms. Cryptococcal fungi exist in asexual forms (yeast) and sexual forms (telomorphs). They produce white mucoid colonies when grown on a wide variety of agars. The two-predominant species of Cryptococcus are differentiated by growth features on canavanine-glycine-bromo methyl blue agar. Histological identification can be performed by methenamine silver stain for yeast forms, mucicarmine stain for yeast and capsule forms and Fontana-Masson stain for the melanin in the yeast.
History and Physical
Cryptococcus neoformans and Cryptococcus gatti both spread through inhalation and cause a similar spectrum of illness. Despite lung being the common site where the pathogen enters the body meningoencephalitis is the most common clinical manifestation of the infection. Clinical features of cryptococcal meningitis typically manifest with in 1-2 weeks and include fever, malaise, headache, neck stiffness, photophobia, nausea, and vomiting. The disease may rarely progress to coma and death. Symptoms such as a cough, dyspnea, skin rash have been reported to occur rarely in the literature.[6] Physical examination findings may sometimes reveal focal neurological deficits, and elevated diastolic pressure indicative of raised intracranial pressure.
Evaluation
Patients presenting with symptoms of central nervous system are evaluated with radiographic imaging of the brain to rule out the presence of elevated cerebrospinal fluid pressure. Cerebrospinal fluid analysis, culture, staining and immunodiagnostic tests of cerebrospinal fluid are the primary diagnostic tests that are performed to diagnose meningitis caused by Cryptococcus. Analysis of the fluid usually shows low white blood cell count, low glucose, and elevated protein but could also be normal in approximately 25-30% of the cases.[7] The culture of the infected fluid reveals cream colored colonies in about 3-7 days while staining with Indian ink helps in identifying the organism rapidly. Detection of cryptococcal antigen through immunodiagnostic tests of the serum and the cerebrospinal fluid provide a definitive diagnosis of the infection. Different techniques such as latex agglutination, enzyme-linked immunosorbent assay (ELISA) and lateral flow assay can be used to confirm the diagnosis of cryptococcal antigen.[8]
Disseminated Cryptococcus infection is defined by a positive blood culture or a positive culture from at least two different sites. Disseminated infection is commonly associated with HIV infection or several other immunocompromised states.
Treatment / Management
Pharmacological treatment for cryptococcal infections depends on the site of infection and the severity of symptoms. Per the 2010 IDSA Guidelines, non-immunosuppressive patients suspected of having a pulmonary cryptococcal infection with mild-to-moderate symptoms can be treated with fluconazole at a dose of 400mg daily for 6-12 months. This is also the treatment recommendation for non-meningeal, non-pulmonary cryptococcosis in patients where CNS disease was ruled out. In non-immunocompromised patients, a lumbar puncture should be considered ruling out asymptomatic CNS involvement, but the guidelines state that an LP can be avoided in asymptomatic, immunocompetent patients with no CNS symptoms.
Management of CNS cryptococcosis and in immune-compromised hosts involves treatment targeting the fungal pathogen, reducing the intracranial pressure, and improvising the immune status of the patient. Antifungal therapy that targets Cryptococcus comprises induction, consolidation, and maintenance phase. Amphotericin B and flucytosine, for a minimum duration of 2 weeks are recommended antifungal therapies that are used for induction phase and fluconazole for a duration of eight weeks is the recommended drug for consolidation phase of the therapy. [9]The medication choices are usually similar in HIV-positive patients, patients with organ transplantation and patients suffering from other conditions that cause immune suppression. After 2 weeks of induction therapy a repeat examination of cerebrospinal fluid is recommended and the duration of induction therapy can further be extended if the cultures remain positive.[10] Maintenance therapy is recommended with fluconazole after eight weeks of induction and consolidation phases and the duration of maintenance phase is generally for a period of 1 year. Maintenance therapy can be discontinued if the patient achieves a healthy immune status clinically correlated as CD4 cell count of more than 100 cells/microL.[11](A1)
Monitoring intracranial pressure and keeping it under check plays an important role in reducing the mortality associated with cryptococcal meningitis.[12] Lumbar puncture is the recommended option for management of intracranial pressure and either a ventricular drain or ventriculo peritoneal shunt is used in patients who require frequent lumbar punctures.[13] Use of medications such as acetazolamide, mannitol and dexamethasone which normally used in bacterial meningitis for lowering intracranial pressure is not recommended in cryptococcal meningitis.[14][15] Another crucial aspect of the management of cryptococcosis includes improving the immune status of the patient. For HIV-positive patients, anti-retroviral therapy is recommended after a duration of 2-10 weeks after initiation of the anti-fungal therapy. Delayed initiation of the anti-retroviral therapy has been associated with better survival rates when compared to early initiation.[16] For patients who have organ transplantations, a reduction in the immunosuppressive therapy in a phased manner while maintaining the balance with a risk of organ rejection would be a recommended approach to enhance the immune status.[17](A1)
There has been a steep decline in the mortality rates associated with cryptococcal infections because of advancements in the anti-retroviral therapy. The prognostic predictors of the disease associated with poor outcomes include altered mental status, cerebrospinal fluid antigen titer greater than 1:1024 and cerebrospinal fluid white blood cell count less than 20/microL.[18](A1)
Differential Diagnosis
- Acanthamoeba infection
- Basal cell carcinoma
- Histoplasmosis
- Lipomas
- Molluscum contagiosum
- Pneumocystis jiroveci pneumonia (PJP)
- Syphilis
- Toxoplasmosis
- Tuberculosis
Enhancing Healthcare Team Outcomes
Prevention:
Prophylactic treatment for cryptococcal infection is recommended in HIV-positive patients with a CD4 count of fewer than 100 cells/microL. Fluconazole and Itraconazole are the recommended drugs for prophylaxis against cryptococcosis.
Current research:
Efficacy of sertraline an antidepressant as an adjunct therapy with fluconazole is being studied in preventing cryptococcal infections in asymptomatic patients who test positive for cryptococcal antigen. A long-term prospective study is being performed to have a better understanding of the immunogenetic defects that might play a role in the pathogenesis of cryptococcal infections.
Media
(Click Image to Enlarge)
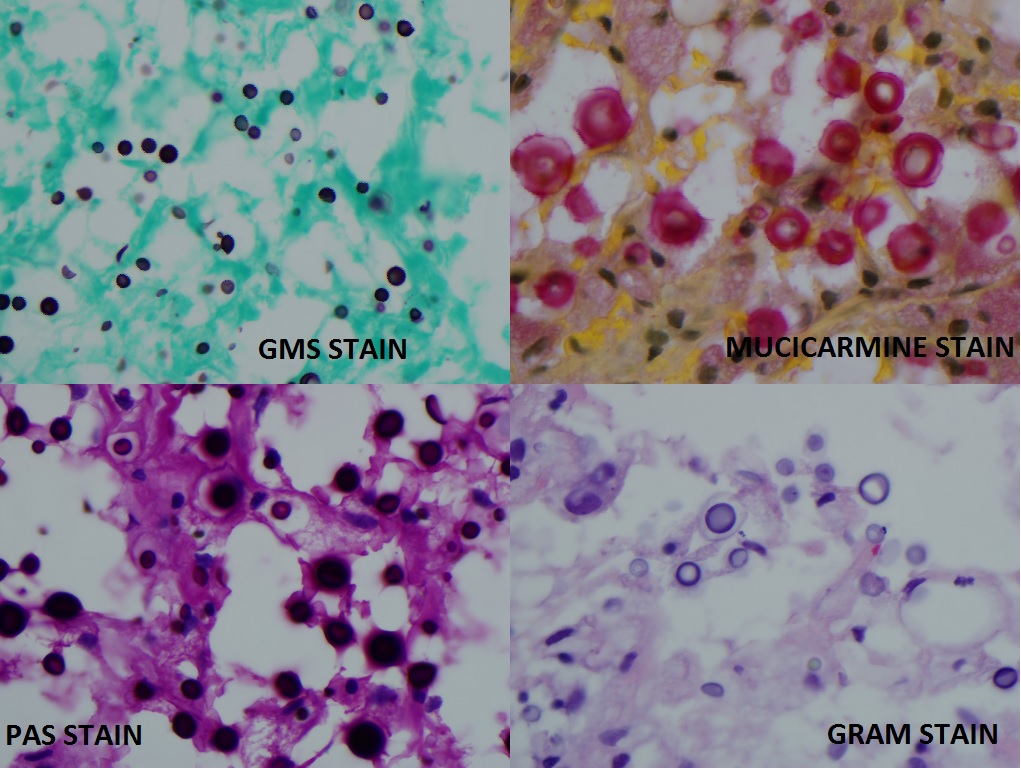
Cryptococcus showed in different fungal stains Contributed by Pradeep Kumar Mada
References
Lin YY, Shiau S, Fang CT. Risk factors for invasive Cryptococcus neoformans diseases: a case-control study. PloS one. 2015:10(3):e0119090. doi: 10.1371/journal.pone.0119090. Epub 2015 Mar 6 [PubMed PMID: 25747471]
Level 2 (mid-level) evidencePark BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS (London, England). 2009 Feb 20:23(4):525-30. doi: 10.1097/QAD.0b013e328322ffac. Epub [PubMed PMID: 19182676]
Mirza SA, Phelan M, Rimland D, Graviss E, Hamill R, Brandt ME, Gardner T, Sattah M, de Leon GP, Baughman W, Hajjeh RA. The changing epidemiology of cryptococcosis: an update from population-based active surveillance in 2 large metropolitan areas, 1992-2000. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2003 Mar 15:36(6):789-94 [PubMed PMID: 12627365]
Srikanta D, Santiago-Tirado FH, Doering TL. Cryptococcus neoformans: historical curiosity to modern pathogen. Yeast (Chichester, England). 2014 Feb:31(2):47-60. doi: 10.1002/yea.2997. Epub 2014 Jan 19 [PubMed PMID: 24375706]
Level 3 (low-level) evidenceEisenman HC, Casadevall A, McClelland EE. New insights on the pathogenesis of invasive Cryptococcus neoformans infection. Current infectious disease reports. 2007 Nov:9(6):457-64 [PubMed PMID: 17999881]
Murakawa GJ, Kerschmann R, Berger T. Cutaneous Cryptococcus infection and AIDS. Report of 12 cases and review of the literature. Archives of dermatology. 1996 May:132(5):545-8 [PubMed PMID: 8624151]
Level 3 (low-level) evidenceGarlipp CR, Rossi CL, Bottini PV. Cerebrospinal fluid profiles in acquired immunodeficiency syndrome with and without neurocryptococcosis. Revista do Instituto de Medicina Tropical de Sao Paulo. 1997 Nov-Dec:39(6):323-5 [PubMed PMID: 9674282]
Boulware DR, Rolfes MA, Rajasingham R, von Hohenberg M, Qin Z, Taseera K, Schutz C, Kwizera R, Butler EK, Meintjes G, Muzoora C, Bischof JC, Meya DB. Multisite validation of cryptococcal antigen lateral flow assay and quantification by laser thermal contrast. Emerging infectious diseases. 2014 Jan:20(1):45-53. doi: 10.3201/eid2001.130906. Epub [PubMed PMID: 24378231]
Level 2 (mid-level) evidencePerfect JR, Dismukes WE, Dromer F, Goldman DL, Graybill JR, Hamill RJ, Harrison TS, Larsen RA, Lortholary O, Nguyen MH, Pappas PG, Powderly WG, Singh N, Sobel JD, Sorrell TC. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2010 Feb 1:50(3):291-322. doi: 10.1086/649858. Epub [PubMed PMID: 20047480]
Level 1 (high-level) evidenceSloan DJ, Parris V. Cryptococcal meningitis: epidemiology and therapeutic options. Clinical epidemiology. 2014:6():169-82. doi: 10.2147/CLEP.S38850. Epub 2014 May 13 [PubMed PMID: 24872723]
Mussini C, Pezzotti P, Miró JM, Martinez E, de Quiros JC, Cinque P, Borghi V, Bedini A, Domingo P, Cahn P, Bossi P, de Luca A, d'Arminio Monforte A, Nelson M, Nwokolo N, Helou S, Negroni R, Jacchetti G, Antinori S, Lazzarin A, Cossarizza A, Esposito R, Antinori A, Aberg JA, International Working Group on Cryptococcosis. Discontinuation of maintenance therapy for cryptococcal meningitis in patients with AIDS treated with highly active antiretroviral therapy: an international observational study. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2004 Feb 15:38(4):565-71 [PubMed PMID: 14765351]
Level 2 (mid-level) evidenceRolfes MA, Hullsiek KH, Rhein J, Nabeta HW, Taseera K, Schutz C, Musubire A, Rajasingham R, Williams DA, Thienemann F, Muzoora C, Meintjes G, Meya DB, Boulware DR. The effect of therapeutic lumbar punctures on acute mortality from cryptococcal meningitis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2014 Dec 1:59(11):1607-14. doi: 10.1093/cid/ciu596. Epub 2014 Jul 23 [PubMed PMID: 25057102]
Level 2 (mid-level) evidenceGraybill JR, Sobel J, Saag M, van Der Horst C, Powderly W, Cloud G, Riser L, Hamill R, Dismukes W. Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2000 Jan:30(1):47-54 [PubMed PMID: 10619732]
Level 1 (high-level) evidenceNewton PN, Thai le H, Tip NQ, Short JM, Chierakul W, Rajanuwong A, Pitisuttithum P, Chasombat S, Phonrat B, Maek-A-Nantawat W, Teaunadi R, Lalloo DG, White NJ. A randomized, double-blind, placebo-controlled trial of acetazolamide for the treatment of elevated intracranial pressure in cryptococcal meningitis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2002 Sep 15:35(6):769-72 [PubMed PMID: 12203177]
Level 1 (high-level) evidenceBeardsley J, Wolbers M, Kibengo FM, Ggayi AB, Kamali A, Cuc NT, Binh TQ, Chau NV, Farrar J, Merson L, Phuong L, Thwaites G, Van Kinh N, Thuy PT, Chierakul W, Siriboon S, Thiansukhon E, Onsanit S, Supphamongkholchaikul W, Chan AK, Heyderman R, Mwinjiwa E, van Oosterhout JJ, Imran D, Basri H, Mayxay M, Dance D, Phimmasone P, Rattanavong S, Lalloo DG, Day JN, CryptoDex Investigators. Adjunctive Dexamethasone in HIV-Associated Cryptococcal Meningitis. The New England journal of medicine. 2016 Feb 11:374(6):542-54. doi: 10.1056/NEJMoa1509024. Epub [PubMed PMID: 26863355]
Boulware DR, Meya DB, Muzoora C, Rolfes MA, Huppler Hullsiek K, Musubire A, Taseera K, Nabeta HW, Schutz C, Williams DA, Rajasingham R, Rhein J, Thienemann F, Lo MW, Nielsen K, Bergemann TL, Kambugu A, Manabe YC, Janoff EN, Bohjanen PR, Meintjes G, COAT Trial Team. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. The New England journal of medicine. 2014 Jun 26:370(26):2487-98. doi: 10.1056/NEJMoa1312884. Epub [PubMed PMID: 24963568]
Level 1 (high-level) evidenceSingh N, Lortholary O, Alexander BD, Gupta KL, John GT, Pursell K, Munoz P, Klintmalm GB, Stosor V, del Busto R, Limaye AP, Somani J, Lyon M, Houston S, House AA, Pruett TL, Orloff S, Humar A, Dowdy L, Garcia-Diaz J, Kalil AC, Fisher RA, Husain S, Cryptococcal Collaborative Transplant Study Group. An immune reconstitution syndrome-like illness associated with Cryptococcus neoformans infection in organ transplant recipients. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2005 Jun 15:40(12):1756-61 [PubMed PMID: 15909263]
Level 3 (low-level) evidenceSaag MS, Powderly WG, Cloud GA, Robinson P, Grieco MH, Sharkey PK, Thompson SE, Sugar AM, Tuazon CU, Fisher JF. Comparison of amphotericin B with fluconazole in the treatment of acute AIDS-associated cryptococcal meningitis. The NIAID Mycoses Study Group and the AIDS Clinical Trials Group. The New England journal of medicine. 1992 Jan 9:326(2):83-9 [PubMed PMID: 1727236]
Level 1 (high-level) evidence