Introduction
Coronary artery ectasia (CAE) is a dilation of the coronary artery lumen. The term "ectasia" refers to diffuse dilation of a coronary artery, while focal coronary dilation is called a "coronary aneurysm."[1] The definition of coronary artery ectasia is a dilatation exceeding more than one-third of the coronary artery length with the diameter of the dilated segment measuring more than 1.5 times the diameter of a normal adjacent segment. Coronary artery ectasia is well recognized, but uncommon findings are encountered during diagnostic coronary angiography (See Image. Coronary Artery Ectasia, Angiograph). The classification of coronary artery ectasia is subdivided into 4 groups:
- Type 1: Diffuse ectasia of 2 or 3 vessels
- Type 2: Diffuse ectasia in 1 vessel and localized disease in another vessel
- Type 3: Diffuse ectasia in 1 vessel only
- Type 4: ocalized or segmental involvement [2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of coronary artery ectasia can be enigmatic. Atherosclerosis lays claim to the principal etiologic cause responsible for greater than 50% of cases in adults, while Kawasaki disease is the most common cause in children and young adults.[3] The histology of atherosclerosis and ectasia is comparable. Coronary artery ectasia is rarely genetic. Acquired etiologies include atherosclerosis, Kawasaki disease, mycotic or septic emboli, Marfan syndrome, arteritis from polyarteritis nodosa, Takayasu disease, or systemic lupus erythematosus. Coronary artery ectasia secondary to iatrogenic causes includes secondary to percutaneous transluminal coronary angioplasty, stents, and directional coronary atherectomy.
Risk Factors
Some of the risk factors for coronary ectasia include:
- Hypertension
- Smoking
- Use of illicit drugs like cocaine
Epidemiology
The incidence varies between 0.3% and 4.9%. The Coronary Artery SUrgery Study registry found coronary artery ectasia in 4.9% of coronary angiograms. Coronary artery ectasia is classified as small (vessel size under 5 mm), medium (vessels size 5 to 8 mm), and giant (vessel size over 8 mm). Based on location most common location is in the right coronary artery (68%), proximal left anterior descending (60%), and left circumflex (50%).[4] Based on shape, coronary artery ectasia can be divided into "saccular," when the transverse diameter is larger than the longitudinal diameter, or "fusiform," when the longitudinal diameter is larger than the transverse diameter.
Pathophysiology
The exact pathophysiology of coronary artery ectasia is unknown. CAE is an anatomical variant or a clinical constellation of coronary artery disease because it may present with myocardial ischemia or coronary syndrome. The mechanism of luminal dilation in some atherosclerotic vessels is ambiguous; atherosclerosis typically causes vessel lumen narrowing. Due to the arterial remodeling, there is an expansion of the blood vessel's medial and external elastic membrane. This proposed methodology of arterial remodeling may be operative in the case of coronary artery ectasia. Intravascular ultrasound reveals that arterial remodeling can be bidirectional depending upon the expansion or contraction of the external elastic membrane. Coronary artery ectasia appears to be exaggerated expansive remodeling of the external elastic membrane resulting in luminal expansion.
Enzymatic degradation of the extracellular matrix by matrix metalloproteinases and other lytic enzymes and thinning of the tunica media associated with severe chronic inflammation is considered the principal pathogenesis of expansive remodeling.[5] CAE is also related to apical hypertrophic cardiomyopathy with high wall tension. In addition to that, iatrogenic mechanisms, eg, percutaneous coronary interventions, including balloon angioplasty, stent placement, and atherectomy, can lead to the formation of aneurysms or ectasias. The mechanism seems to be the injury of the media of the blood vessel.[6]
Histopathology
Histology usually shows it thickened fibrotic intima with lipid deposition. The internal elastic laminal layer usually suffers disruption, leading to reduced medial elastic tissue. This loss of elastic tissue is the primary cause along with chronic vascular inflammation leading to ectasia.
History and Physical
The symptoms of coronary artery ectasia may be associated with concomitant coronary disease, Kawasaki disease, or connective tissue disease. Most patients are asymptomatic and may present with angina post-stress tests and acute coronary syndrome. Diminished coronary flow speed or stagnancy of blood flow may cause exercise-induced angina without coexistent stenotic coronary artery disease. Formation of intracoronary thrombus or dissipation leading to distal emboli may be the trigger of acute coronary syndrome, which is hastened by stagnant flow in the ecstatic coronary segment. The hypothesis is that coronary artery ectasia is predisposed to vasospasm, which may elicit angina or acute coronary syndrome. In people younger than 50, CAE should raise concern for connective tissue disorders and vasculitides.[7][8]
Evaluation
Coronary angiography is the gold standard in diagnosing coronary artery ectasia. Intravascular ultrasound is critical for evaluating luminal characteristics and pathologies.[6] Distortions of flow and washout are common in CAE and are related to the severity of ectasia. Signs of stagnant flow include delayed antegrade contrast filling, segmental backflow, and stasis in the ectatic coronary segment.[5] Other investigative techniques include magnetic resonance angiography (MRA) and coronary computed tomography angiography. For the follow-up of patients, MRA is the preferred modality.
Treatment / Management
Management of coronary artery ectasia is fraught with uncertainty because the rarity of CAE prevents large randomized trials comparing different treatment approaches. When coronary artery disease coexists, intense primary and secondary risk factor modifications are mandatory. Management of isolated coronary artery ectasia in a case with angina or myocardial ischemia includes statins and anti-ischemic medications. Acute coronary syndromes associated with CAE may require thrombolysis, heparin administration, and glycoprotein IIb/IIIa receptor inhibitors. Thrombus aspiration may be necessary during primary percutaneous coronary intervention.
Percutaneous and surgical interventions are often beneficial for patients with CAE and stenotic lesions where angina persists despite maximal medical therapy. Optimal stent sizing is essential to prevent misplacement and embolization of stents. Many authors recommend chronic anticoagulation; however, no randomized trial demonstrates its benefit in CAE. The anticipated benefit must counterbalance the risk of hemorrhage.[9][10] Surgery is rarely done but is sometimes a necessity in patients who have recurring complications. The surgery involves ligation of the proximal and distal segments of the ectatic vessel and replacing it with a bypass graft. There should be no attempt to repair the ectatic vessel as the results are poor.(A1)
Differential Diagnosis
The differential diagnoses for coronary ectasia include the following:
- Atherosclerosis
- Bacterial syphilis
- Behcet disease
- Ehler-Danlos syndrome
- Fibromuscular dysplasia
- Giant cell arteritis
- Kawasaki disease
- Marfan syndrome
- Mycotic aneurysm
- Septic emboli
Prognosis
The prognosis for coronary artery ectasia is directly related to the severity of concomitant coronary artery disease. Coronary artery ectasia with underlying coronary artery disease is a dangerous combination with an increased potential for adverse cardiac events. Isolated CAE still carries the risk of myocardial ischemia and infarction. Type 1 and type CAE demonstrate a higher risk than type 3 and type 4 CAE. No reported data shows a relationship between the diameter of an artery and the outcome.[11]
Complications
The complications that can manifest with coronary ectasia are as follows:
- Thrombus leading to myocardial infarction
- Acute coronary syndromes
- Fistula formation in the cardiac chambers
- Thrombosis
- Distal embolization
- Complications after stenting include:
- Stent misplacement
- Embolization of stents
- Stent thrombosis
- Restenosis
Deterrence and Patient Education
Patients need to understand that there is no specific treatment for coronary ectasia and that the best course of action is diligent adherence to coronary artery medication regimens. In the rare instances where surgery becomes necessary, they need to understand the nature of the procedure and the requirements for postoperative recovery.[12][13]
Enhancing Healthcare Team Outcomes
In complicated cases involving multiple coronary arteries or left main artery disease, an interprofessional team approach is preferred that includes an interventional cardiologist, cardiac surgeon, cardiac intensivist, and intensive care unit and cardiovascular specialty trained nurses, radiologists, and cardiac pharmacists to devise a treatment plan to reduced complications and improve outcomes. The overall management is similar to a patient with coronary artery disease. However, because of a lack of long-term studies, the ideal management of this disorder remains unknown.
Media
(Click Image to Enlarge)
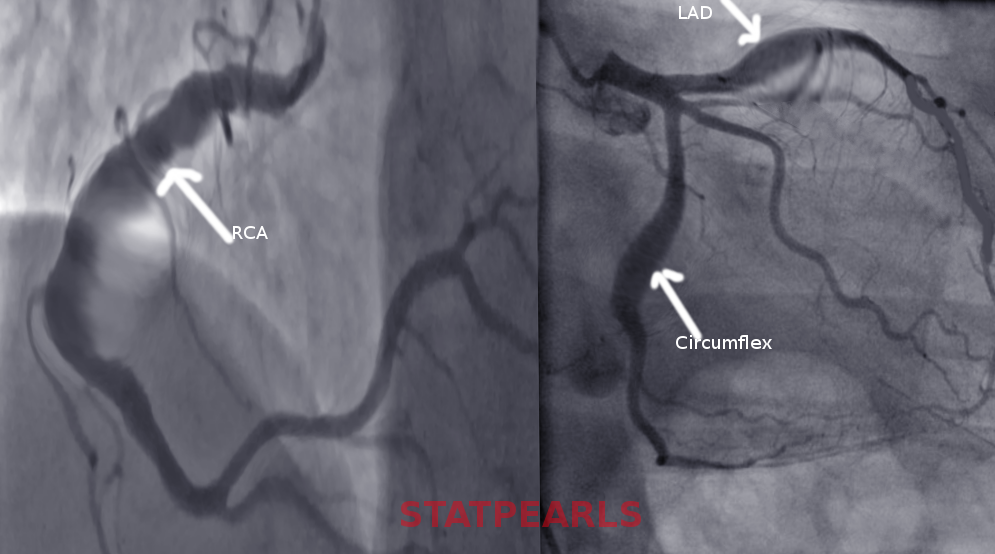
Coronary Artery Ectasia, Angiograph. The image shows coronary artery ectasia, a dilation of the coronary artery lumen.
Contributed by S Bhimji, MD
References
Mavrogeni S. Coronary artery ectasia: from diagnosis to treatment. Hellenic journal of cardiology : HJC = Hellenike kardiologike epitheorese. 2010 Mar-Apr:51(2):158-63 [PubMed PMID: 20378518]
Zeina AR, Sharif D, Blinder J, Rosenschein U, Barmeir E. Noninvasive assessment of coronary artery ectasia using multidetector computed tomography. Coronary artery disease. 2007 May:18(3):175-80 [PubMed PMID: 17429290]
Díaz-Zamudio M, Bacilio-Pérez U, Herrera-Zarza MC, Meave-González A, Alexanderson-Rosas E, Zambrana-Balta GF, Kimura-Hayama ET. Coronary artery aneurysms and ectasia: role of coronary CT angiography. Radiographics : a review publication of the Radiological Society of North America, Inc. 2009 Nov:29(7):1939-54. doi: 10.1148/rg.297095048. Epub [PubMed PMID: 19926755]
Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, Kemp HG, Mudd JG, Gosselin AJ. Aneurysmal coronary artery disease. Circulation. 1983 Jan:67(1):134-8 [PubMed PMID: 6847792]
Antoniadis AP, Chatzizisis YS, Giannoglou GD. Pathogenetic mechanisms of coronary ectasia. International journal of cardiology. 2008 Nov 28:130(3):335-43. doi: 10.1016/j.ijcard.2008.05.071. Epub 2008 Aug 9 [PubMed PMID: 18694609]
Manginas A, Cokkinos DV. Coronary artery ectasias: imaging, functional assessment and clinical implications. European heart journal. 2006 May:27(9):1026-31 [PubMed PMID: 16415301]
Sayin T, Döven O, Berkalp B, Akyürek O, Güleç S, Oral D. Exercise-induced myocardial ischemia in patients with coronary artery ectasia without obstructive coronary artery disease. International journal of cardiology. 2001 Apr:78(2):143-9 [PubMed PMID: 11334658]
Level 2 (mid-level) evidenceZografos TA, Korovesis S, Giazitzoglou E, Kokladi M, Venetsanakos I, Paxinos G, Fragakis N, Katritsis DG. Clinical and angiographic characteristics of patients with coronary artery ectasia. International journal of cardiology. 2013 Aug 20:167(4):1536-41. doi: 10.1016/j.ijcard.2012.04.098. Epub 2012 May 8 [PubMed PMID: 22572634]
Level 2 (mid-level) evidenceTurhan H, Yetkin E. What is the plausible strategy for the management of patients with isolated coronary artery ectasia and myocardial ischemia? International journal of cardiology. 2007 Apr 25:117(2):285-6 [PubMed PMID: 16893580]
Level 3 (low-level) evidenceLevine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011 Dec 6:124(23):e574-651. doi: 10.1161/CIR.0b013e31823ba622. Epub 2011 Nov 7 [PubMed PMID: 22064601]
Level 1 (high-level) evidenceGulec S, Atmaca Y, Kilickap M, Akyürek O, Aras O, Oral D. Angiographic assessment of myocardial perfusion in patients with isolated coronary artery ectasia. The American journal of cardiology. 2003 Apr 15:91(8):996-9, A7 [PubMed PMID: 12686347]
Ullah W, Shaukat M, Ahmad A, Ali Z, Mukhtar M, Ur Rashid M. A giant coronary artery ectasia successfully managed conservatively. Journal of community hospital internal medicine perspectives. 2020 Aug 2:10(4):343-345. doi: 10.1080/20009666.2020.1773710. Epub 2020 Aug 2 [PubMed PMID: 32850094]
Level 3 (low-level) evidenceFan CH, Hao Y, Liu YH, Li XL, Huang ZH, Luo Y, Li RL. Anti-inflammatory effects of rosuvastatin treatment on coronary artery ectasia patients of different age groups. BMC cardiovascular disorders. 2020 Jul 11:20(1):330. doi: 10.1186/s12872-020-01604-z. Epub 2020 Jul 11 [PubMed PMID: 32652935]