Introduction
Cloacal malformations are rare congenital anomalies characterized by a confluence of the gastrointestinal, genital, and urologic systems which exits the perineum through a single orifice.[1] [Figure 1] Cloacal malformations are considered to be the most complex anorectal malformations (ARM) and represent a significant technical challenge for pediatric surgeons, pediatric urologists, and pediatric gynecologists.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of these conditions remains unknown.
Epidemiology
The incidence of cloacal anomalies is estimated to be 1 per 50000 live births, although many cloacal malformations may be misdiagnosed as a rectovaginal fistula.[2] Thus the actual incidence may be higher. They are seen exclusively in females.
Pathophysiology
Cloacal malformations result from failure of the embryonic anorectal and urogenital channels to separate during the sixth and seventh gestational weeks.[3] The current belief is that earlier arrest of normal embryologic processes results in a longer common channel which has reconstructive and functional implications later in life.
History and Physical
Prenatal diagnosis is uncommon in patients with a cloaca, although prenatal ultrasound or MRI may identify a cystic pelvic structure in the pelvis of a female patient consistent with a fluid-filled vagina (hydrocolpos).[2] Additional prenatal orthopedic or renal findings make the diagnosis of cloaca more likely.
The definitive diagnosis of cloacal malformation is made in the newborn period by physical examination with the identification of a single perineal orifice, usually posterior to the clitoris. A thorough perineal examination with adequate lighting is required, which is best accomplished by retracting the labia “up and out” to assess the relation of the urethra to the hymen. In cloacal malformations, the urethra is inside the hymen, or the anterior hymen is absent. If the urethra is distal to the hymen, then a cloaca can be ruled out. Further examination of the genitalia may demonstrate a diminutive and foreshortened labia minora and a clitoral hood. Abdominal examination may divulge the presence of a mass in the lower abdomen which likely represents a hydrocolpos which can be present in as many of 40% of patients with a cloaca.[1]
Evaluation
Initial evaluation of a patient with a cloacal malformation involves the identification and treatment of any associated life-threatening anomalies. Like other ARMs, cloacas often correlate with various anomalies in the vertebral, anorectal, cardiac, tracheoesophageal fistula, renal, and limb (VACTERL) association.[4] Early consultation with a pediatric urologist or a pediatric surgeon with experience in cloacal management is necessary upon confirmed diagnosis.
A thorough urologic assessment is mandatory in the newborn period.[5] Structural and functional urologic anomalies, including hydronephrosis, renal agenesis, renal dysplasia, horseshoe kidney, are common in patients with cloaca and are found in up to 90% of cases.[1][6][7] Urologic and renal dysfunction account for significant long-term morbidity in patients with the cloaca, and early identification of anomalies and appropriate intervention can optimize long-term renal health.
Identification of spinal anomalies is necessary as there is a high association of cloaca and tethered cord.[8] This analysis can be performed using ultrasound within the first 3 months of age, or an MRI after 3 months due to ossification of the sacrum and coccyx. The decision to de-tether a cord is a clinical one based on imaging and function effects of diagnosed with the help of urodynamics. The indications for de-tethering vary in each institution. There appear to be clear urologic benefits, although the impact on fecal continence has not been clearly shown.
An assessment of the sacrum can be performed with anteroposterior (AP) and lateral sacral x-rays to assess for sacral anomalies and determine the sacral ratio.[9] The sacral ratio is the length of the sacrum from the sacroiliac joint to the tip of the coccyx over the distance of the iliac crest to the sacroiliac joint. Dedicated lateral sacral x-rays are necessary for this calculation as films in the anterior-posterior plane can be affected by the tilt of the pelvis, yielding an inaccurate calculation. This ratio serves as a marker of development of the pelvic musculature and nerves essential to bowel and bladder function later in life and can form the basis for counseling families on their child’s functional prognosis. AP images are useful for identifying hemivertebrae or other sacral anomalies.
Treatment / Management
Initial Management
After stabilizing the child, the initial goal is to identify and drain a hydrocolpos, if present.[1] A hydrocolpos is a fluid-filled vagina that compresses the bladder anteriorly at the trigone where the ureters enter, causing hydroureternephrosis and obstructive uropathy. This condition is best investigated with an ultrasound of the abdomen and pelvis. Drainage can be performed by catheterizing the common channel; however, it is necessary to confirm that the hydrocolpos has undergone adequate emptying as the catheter may enter the bladder or a single hemivagina resulting in the drainage of fluid but not adequate decompression of the hydrocolpos. Catheterization, therefore, may not a reliable long-term strategy in all patients and definitive drainage with a vaginostomy should be a consideration in those patients with recurrent or inadequate drainage to ensure proper decompression of the urinary system. Rarely, if the bladder does not adequately empty despite adequate treatment of the hydrocolpos, urinary diversion can be performed at the time of colostomy creation with a vesicostomy or placement of a suprapubic cystostomy tube.[1](B2)
Early surgical management aims to divert the fecal stream with a descending colostomy with mucous fistula creation. Consideration should be given to the placement of the colostomy and length of the distal segment as this portion of the bowel will be used for the future pull through. A loop colostomy is not recommended as the distal limb remains in continuity with the urinary tract; thus any spillage of stool risks contamination of the urinary system and urinary tract infection.
Treatment Planning
Definitive surgical repair requires the identification and measurement of several pelvic structures, including:
- Length of the common channel
- Length of the urethra
- The presence and length of a vagina
- The presence of a hemivagina or longitudinal vaginal septum
- The presence of a cervix (or multiple cervices)
- Visualization of the height of the rectum and location of the rectal fistula relative to the pubococcygeal (PC) line.
The length of the common channel and urethra are critical for surgical planning (e.g., to decide whether to perform a urogenital separation or total urogenital mobilization). The 3 cm common channel is traditionally taught as the cutoff between simple and complex cloacas.[10] The presence and length of the patient’s native vagina are necessary to determine the likelihood of needing to perform a vaginal replacement at the time of PSARVUP. Additional details of the gynecologic anatomy are necessary as any necessary gynecologic procedures (e.g., vaginal septum excision) can be performed simultaneously. This information is also essential for long-term gynecologic counseling. Precise knowledge of the location of the rectum is necessary to correctly identify whether it is reachable from a posterior sagittal approach or if laparoscopy or laparotomy will be needed. This decision will have a significant effect on the anesthetic plan as well as the postoperative care of the patient.
No standardized imaging protocols exist at present, but endoscopy and 3D cloacagram are two useful modalities to assess the patient’s anatomy.[11] Some authors have suggested that the role of MRI will probably become more important in the future.[12](B2)
Definitive Treatment
The definitive management of cloaca is surgical, with the goal of separating the gastrointestinal, gynecologic, and urologic structures and creating a perineal opening for each of the three structures for optimization of the function of each system, and to create a catheterizable urethra.[1][13][14](B2)
The surgical management of this condition has evolved significantly over the last several decades. In 1982, Pena first described the posterior sagittal approach for the repair of a cloacal malformation; an operation termed the posterior sagittal anorectovaginourethroplasty (PSARVUP).[15] The technique described separating the vagina from the common channel using a technique called a urogenital separation. The fine dissection in the plane between the vagina and urethra often resulted in devascularization of the tissue resulting in urethrovaginal fistulae, which can be a very debilitating complication of urogenital separation.
In 1997, the total urogenital mobilization (TUM) was described as a technique to mobilize the vagina and urethra as a single unit, thereby obviating the need to mobilize the tissue between these two structures.[16] This procedure, however, risks leaving the patient with a urethra which is too short and a bladder neck which is below the urogenital diaphragm, resulting in urinary incontinence.[17] Wood, therefore, proposed an algorithm in 2016 which considers both the length of the common channel and native urethra to leave the patient with a urethra of adequate length to maximize urinary continence.[10]
Definitive repair is typically performed between 6 and 12 months of age. The specific details of the repair are beyond the scope of this manuscript; it is performed through a posterior sagittal incision, with the addition of a laparoscopic or open approach to mobilize a high rectum or vagina as dictated by the patient’s anatomy.
Differential Diagnosis
The differential diagnosis of cloaca includes less severe ARM subtypes (e.g., rectovaginal fistula, rectovestibular fistula, imperforate anus with no fistula) with or without vaginal atresia. These diagnoses can be ruled out based on a thorough physical examination.
Treatment Planning
As stated above, definitive surgical repair requires the identification and measurement of several pelvic structures, including:
- Length of the common channel
- Length of the urethra
- Presence and length of a vagina
- Presence of a hemivagina or longitudinal vaginal septum
- The presence of a cervix (or multiple cervices)
- Visualization of the height of the rectum and location of the rectal fistula
The length of the common channel and urethra are critical for surgical planning (e.g., to decide whether to perform a urogenital separation or total urogenital mobilization). The 3 cm common channel is traditionally taught as the cutoff between simple and complex cloacas. The presence and length of the patient’s native vagina are necessary to determine the likelihood of needing to perform a vaginal replacement at the time of PSARVUP. Additional details of the gynecologic anatomy are necessary as any necessary gynecologic procedures (e.g., vaginal septum excision) can be performed simultaneously. This information is also necessary for long-term gynecologic counseling. Precise knowledge of the location of the rectum is necessary to correctly identify whether it is reachable from a posterior sagittal approach or if laparoscopy or laparotomy will be needed. This decision will have a significant effect on the anesthetic plan as well as the postoperative care of the patient.
No standardized imaging protocols exist at present, but endoscopy and 3D cloacagram are two useful modalities to assess the patient’s anatomy.
Prognosis
Urinary and bowel continence in patients with cloacal malformations are related primarily to the length of the common channel and the presence of other anomalies, in particular, the degree of sacral development and the presence of tethered spinal cord. Patients with a common channel of greater than 3 cm, tethered cord, and a sacral ratio of less than 0.4 tend to have worse functional outcomes.[18] However, these spinal and sacral anomalies are more commonly present in patients with more complex cloacal malformations, and a complete understanding of the individual contribution of the spine and sacrum to these functional outcomes remains unknown in patients with cloaca. Some patients with poor colorectal and urologic function may require bowel and bladder reconstruction later in childhood which can be performed simultaneously.[19]
Complications
Inability to correctly diagnose a cloaca in the newborn period may fail to identify obstructing uropathy caused by a hydrocolpos which may cause sepsis, acidosis, and in severe cases renal failure. With misdiagnosis of the cloaca in the newborn period, the surgeon may only repair the rectal component of the malformation and leave a persistent urogenital sinus. The most concerning postoperative complication is the development of a urethrovaginal fistula which requires surgical repair if proximal to the urinary sphincter.
Postoperative and Rehabilitation Care
A Foley catheter placed intraoperatively remains in place for 2 to 4 weeks. Patients should undergo an examination under anesthesia (EUA) approximately 4 weeks after PSARVUP. The Foley catheter can be removed at the time of cystoscopy to ensure that the urethra can be accessed for intermittent catheterization as needed. If long-term urinary diversion is necessary, such as in the case of a patient with a long common channel, poor sacrum, and tethered cord, a vesicostomy or suprapubic cystostomy tube may be needed.
The anus should be examined to ensure adequate healing of the perineal body and the anoplasty. If both structures well healed, the anus can undergo sizing with a Hegar dilator, and a twice-daily dilation program started with the goal to increase the size of the dilator every week to a final measurement determined by the patient’s age. Upon reaching the desired size, the colostomy can be closed.
Patients with cloacal malformations require long-term assessment of renal function at regular intervals, as renal impairment is common.[7] The incidence of renal failure over the lifetime of a patient with cloaca varies widely but may approach 50%.[14]
A bowel regimen should be started at the time of colostomy closure to assist colonic emptying regularly and to avoid dilation of the rectosigmoid colon which will impair normal colonic function and make potty training difficult. If the patient is unable to potty train, a formal bowel management program may be needed to determine a laxative or enema regimen that can get the child clean and in normal underwear.
Gynecologic counseling should take place before puberty with consideration of the patient’s unique gynecologic anatomy. An adequate vagina that allows menstrual egress should be ensured prior to the start of menses. Preliminary to the onset of sexual activity, the patient should be examined to ensure the vagina is adequate for penetrative vaginal intercourse. Pregnancy is possible for patients with the cloaca, although Cesarean sections are the preferred method of delivery.[20]
Enhancing Healthcare Team Outcomes
Cloacal malformations are rare, multi-system anomalies which require management by a team of an interprofessional specialists including nurses. This model allows for a collaborative approach to the myriad of preoperative, surgical, nursing and postoperative challenges often seen in these patients. Optimal functional outcomes result from an interprofessional approach beginning early in the child’s care at a high volume center dedicated to the care of these complex malformations.[21] (Level IV)
Media
(Click Image to Enlarge)

Cloacal malformation. Contributed by Marc A. Levitt, MD
(Click Image to Enlarge)
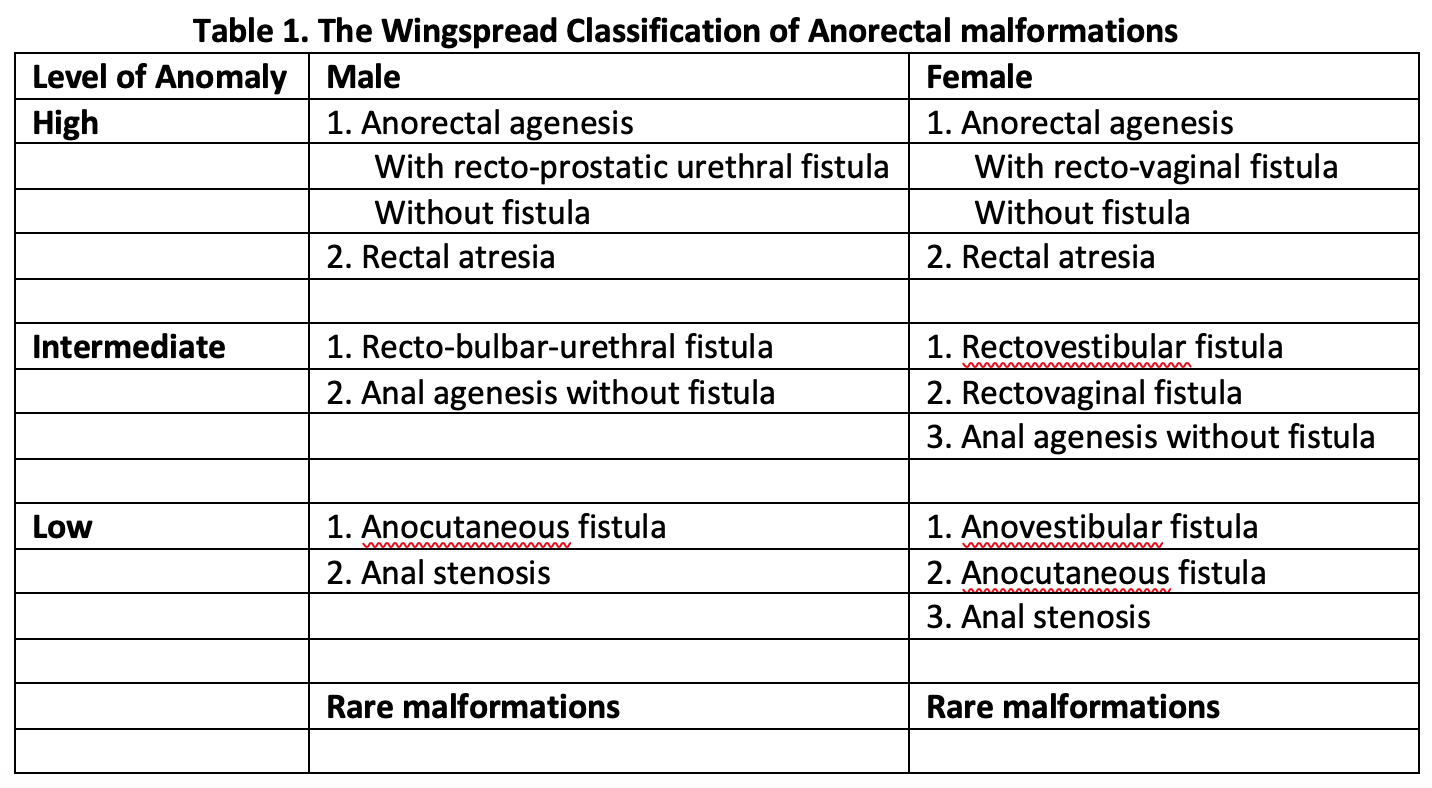
Table 1. The Wingspread Classification of Anorectal malformations "Contributed by Meenakshi Singh, MBBS"
(Click Image to Enlarge)
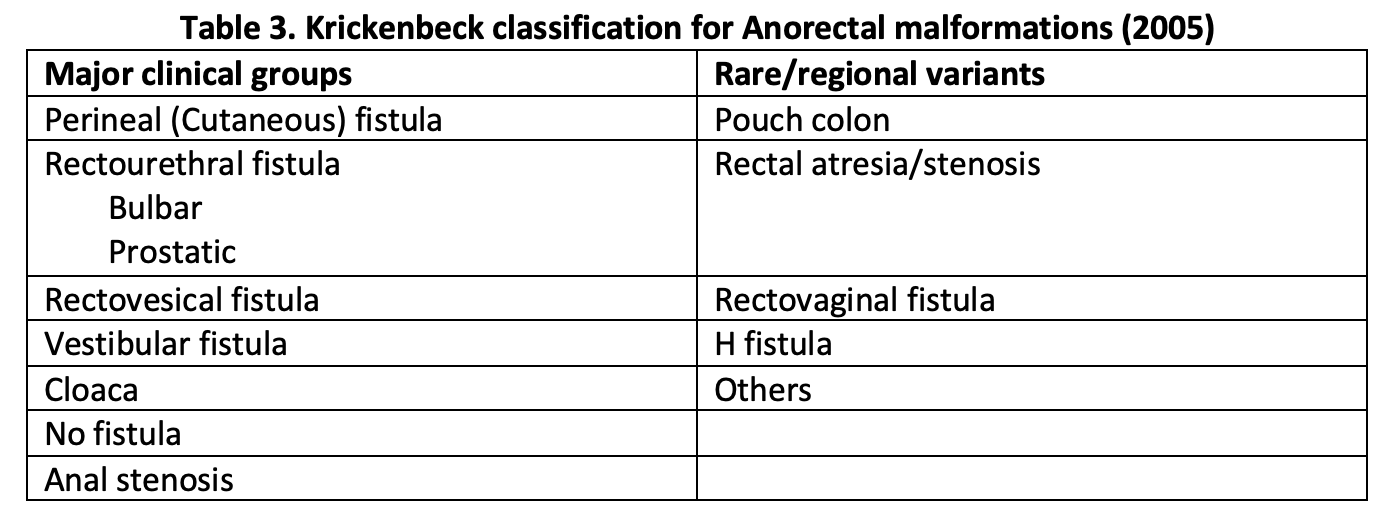
Table 3. Krickenbeck classification for Anorectal malformations (2005) "Contributed by Meenakshi Singh, MBBS"
References
Levitt MA, Peña A. Cloacal malformations: lessons learned from 490 cases. Seminars in pediatric surgery. 2010 May:19(2):128-38. doi: 10.1053/j.sempedsurg.2009.11.012. Epub [PubMed PMID: 20307849]
Level 2 (mid-level) evidenceWarne S, Chitty LS, Wilcox DT. Prenatal diagnosis of cloacal anomalies. BJU international. 2002 Jan:89(1):78-81 [PubMed PMID: 11849166]
Level 3 (low-level) evidenceKruepunga N, Hikspoors JPJM, Mekonen HK, Mommen GMC, Meemon K, Weerachatyanukul W, Asuvapongpatana S, Eleonore Köhler S, Lamers WH. The development of the cloaca in the human embryo. Journal of anatomy. 2018 Dec:233(6):724-739. doi: 10.1111/joa.12882. Epub 2018 Oct 7 [PubMed PMID: 30294789]
Minneci PC,Kabre RS,Mak GZ,Halleran DR,Cooper JN,Afrazi A,Calkins CM,Downard CD,Ehrlich P,Fraser J,Gadepalli SK,Helmrath MA,Kohler JE,Landisch R,Landman MP,Lee C,Leys CM,Lodwick DL,Mon R,McClure B,Rymeski B,Saito JM,Sato TT,St Peter SD,Wood R,Levitt MA,Deans KJ,Midwest Pediatric Surgery Consortium., Screening practices and associated anomalies in infants with anorectal malformations: Results from the Midwest Pediatric Surgery Consortium. Journal of pediatric surgery. 2018 Jun [PubMed PMID: 29602552]
VanderBrink BA, Reddy PP. Early urologic considerations in patients with persistent cloaca. Seminars in pediatric surgery. 2016 Apr:25(2):82-9. doi: 10.1053/j.sempedsurg.2015.11.005. Epub 2015 Nov 10 [PubMed PMID: 26969231]
Goossens WJ, de Blaauw I, Wijnen MH, de Gier RP, Kortmann B, Feitz WF. Urological anomalies in anorectal malformations in The Netherlands: effects of screening all patients on long-term outcome. Pediatric surgery international. 2011 Oct:27(10):1091-7. doi: 10.1007/s00383-011-2959-4. Epub [PubMed PMID: 21805172]
Level 2 (mid-level) evidenceWarne SA, Wilcox DT, Ledermann SE, Ransley PG. Renal outcome in patients with cloaca. The Journal of urology. 2002 Jun:167(6):2548-51; discussion 2551 [PubMed PMID: 11992086]
Level 2 (mid-level) evidenceLevitt MA, Patel M, Rodriguez G, Gaylin DS, Pena A. The tethered spinal cord in patients with anorectal malformations. Journal of pediatric surgery. 1997 Mar:32(3):462-8 [PubMed PMID: 9094019]
Torre M, Martucciello G, Jasonni V. Sacral development in anorectal malformations and in normal population. Pediatric radiology. 2001 Dec:31(12):858-62 [PubMed PMID: 11727021]
Wood RJ, Reck-Burneo CA, Dajusta D, Ching C, Jayanthi R, Bates DG, Fuchs ME, McCracken K, Hewitt G, Levitt MA. Cloaca reconstruction: a new algorithm which considers the role of urethral length in determining surgical planning. Journal of pediatric surgery. 2017 Oct 12:():. pii: S0022-3468(17)30644-9. doi: 10.1016/j.jpedsurg.2017.10.022. Epub 2017 Oct 12 [PubMed PMID: 29132797]
Gasior AC, Reck C, Lane V, Wood RJ, Patterson J, Strouse R, Lin S, Cooper J, Gregory Bates D, Levitt MA. Transcending Dimensions: a Comparative Analysis of Cloaca Imaging in Advancing the Surgeon's Understanding of Complex Anatomy. Journal of digital imaging. 2019 Oct:32(5):761-765. doi: 10.1007/s10278-018-0139-y. Epub [PubMed PMID: 30350007]
Level 2 (mid-level) evidenceJarboe MD, Teitelbaum DH, Dillman JR. Combined 3D rotational fluoroscopic-MRI cloacagram procedure defines luminal and extraluminal pelvic anatomy prior to surgical reconstruction of cloacal and other complex pelvic malformations. Pediatric surgery international. 2012 Aug:28(8):757-63. doi: 10.1007/s00383-012-3122-6. Epub [PubMed PMID: 22810369]
Level 3 (low-level) evidenceBraga LH, Lorenzo AJ, Dave S, Del-Valle MH, Khoury AE, Pippi-Salle JL. Long-term renal function and continence status in patients with cloacal malformation. Canadian Urological Association journal = Journal de l'Association des urologues du Canada. 2007 Nov:1(4):371-6 [PubMed PMID: 18542820]
Caldwell BT, Wilcox DT. Long-term urological outcomes in cloacal anomalies. Seminars in pediatric surgery. 2016 Apr:25(2):108-11. doi: 10.1053/j.sempedsurg.2015.11.010. Epub 2015 Nov 10 [PubMed PMID: 26969235]
Peña A, Devries PA. Posterior sagittal anorectoplasty: important technical considerations and new applications. Journal of pediatric surgery. 1982 Dec:17(6):796-811 [PubMed PMID: 6761417]
Peña A. Total urogenital mobilization--an easier way to repair cloacas. Journal of pediatric surgery. 1997 Feb:32(2):263-7; discussion 267-8 [PubMed PMID: 9044134]
Halleran DR, Thompson B, Fuchs M, Vilanova-Sanchez A, Rentea RM, Bates DG, McCracken K, Hewitt G, Ching C, DaJusta D, Levitt MA, Wood RJ. Urethral length in female infants and its relevance in the repair of cloaca. Journal of pediatric surgery. 2019 Feb:54(2):303-306. doi: 10.1016/j.jpedsurg.2018.10.094. Epub 2018 Nov 7 [PubMed PMID: 30503195]
Peña A, Levitt MA, Hong A, Midulla P. Surgical management of cloacal malformations: a review of 339 patients. Journal of pediatric surgery. 2004 Mar:39(3):470-9; discussion 470-9 [PubMed PMID: 15017572]
Level 2 (mid-level) evidenceHalleran DR, Wood RJ, Vilanova-Sanchez A, Rentea RM, Brown C, Fuchs M, Jayanthi VR, Ching C, Ahmad H, Gasior AC, Michalsky MP, Levitt MA, DaJusta D. Simultaneous Robotic-Assisted Laparoscopy for Bladder and Bowel Reconstruction. Journal of laparoendoscopic & advanced surgical techniques. Part A. 2018 Dec:28(12):1513-1516. doi: 10.1089/lap.2018.0190. Epub 2018 Jun 20 [PubMed PMID: 29924670]
Vilanova-Sanchez A, McCracken K, Halleran DR, Wood RJ, Reck-Burneo CA, Levitt MA, Hewitt G. Obstetrical Outcomes in Adult Patients Born with Complex Anorectal Malformations and Cloacal Anomalies: A Literature Review. Journal of pediatric and adolescent gynecology. 2019 Feb:32(1):7-14. doi: 10.1016/j.jpag.2018.10.002. Epub 2018 Oct 24 [PubMed PMID: 30367985]
Vilanova-Sánchez A, Reck CA, Wood RJ, Garcia Mauriño C, Gasior AC, Dyckes RE, McCracken K, Weaver L, Halleran DR, Diefenbach K, Minzler D, Rentea RM, Ching CB, Jayanthi VR, Fuchs M, Dajusta D, Hewitt GD, Levitt MA. Impact on Patient Care of a Multidisciplinary Center Specializing in Colorectal and Pelvic Reconstruction. Frontiers in surgery. 2018:5():68. doi: 10.3389/fsurg.2018.00068. Epub 2018 Nov 19 [PubMed PMID: 30510931]