
Introduction
Cervical ectropion is a benign condition that is regarded as a normal variant found in women of the reproductive age group. In this condition, the glandular cells (the columnar epithelium) that line the endocervix are present on the ectocervix, leading to exposure of the columnar cells to the vaginal milieu. It is also known as cervical ectopy or cervical eversion.[1] This condition has also been referred to as cervical erosion, which is a misleading term because there is no actual erosion of the cervix.[2]
Cervical ectropion is usually found on routine pelvic examination of women in the reproductive age group. It is an asymptomatic variant but has been correlated with chronic cervicitis. It is a common physiological condition amongst adolescents and pregnant women.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The occurrence of cervical ectropion is related to increased estrogen levels. The cervix is highly responsive to estrogen, causing the proliferation and differentiation of the cervical epithelium. Therefore cervical ectropion is usually found in the conditions of high estrogen exposure, which are as follows:
- Adolescents
- Pregnancy
- Women on hormonal contraception
- During the years of menstruation, most commonly seen in the ovulatory phase
It may be a congenital condition due to the persistence of the squamocolumnar junction at its original neonatal location. During late fetal development and the first month of life, maternal hormone exposure stimulates hyperactivity of endocervical columnar epithelium and produce cervical ectropion.
It is uncommon in postmenopausal women. In the postmenopausal phase, the estrogen levels are declining, causing the cervix to shrink and invert, thus drawing the squamous cell epithelium of the ectocervix into the endocervical canal.
Epidemiology
Cervical ectropion is one of the most commonly found gynecological conditions. The prevalence of cervical ectropion ranges between 17 percent and 50 percent. The prevalence increases with parity but decreases with age 35 and above. Cervical ectropion can be found in up to 80% of sexually active adolescents. The prevalence also depends on the type of contraception used. It is seen more commonly in women taking oral contraceptive pills and less so in women using barrier methods of contraception.[3][4]
Studies show that 54.9 percent of women in Benghazi, Libya, that use oral contraceptive pills and intra-uterine copper devices have cervical ectropion. Thus it was the most prevalent gynecological disorder in that population. 43.2 percent of women in China were reported as having cervical ectropion.[4] The prevalence of cervical ectropion is about 29 percent in premature female infants and 68 percent in the first month of life due to the transfer of maternal estrogen through the placenta.[5]
Pathophysiology
The cervix is the lower part of the uterus and is composed of two parts:
- Endocervix. It is the proximal portion of the cervix.
- Ectocervix. It is the distal portion of the cervix that projects into the vagina.
The squamocolumnar junction is the area in the cervix where the columnar and the squamous epithelium meet. The position of the squamocolumnar junction varies with age and hormone levels. The neonatal position of the squamocolumnar junction changes with hormonal influences in utero, at puberty, during pregnancy, and after menopause. At birth and menarche, it is located just within the cervical canal. During reproductive age, the columnar epithelium extends outward onto the ectocervix as the cervix events. This causes the squamocolumnar junction to move outwards as well, thus exposing it to the acidic pH of the vagina. In cervical ectropion, there is eversion of the squamous, columnar junction, as well as the columnar epithelium of the endocervix onto the ectocervix. Over time, the cells basal to the columnar cells proliferate and differentiate into squamous cells, thus replacing the overlying columnar cells.[6] The cervical ectropion is decreased over time by two processes, squamous metaplasia and epithelialization.[7][8]
- Squamous metaplasia. It is a normal and irreversible physiological process in which the columnar epithelium is replaced by squamous epithelium. Low pH, sexual activity, and cervical infections may play a role in this process as well. This process is most pronounced when the progesterone/estrogen ratio is high, like during pregnancy, hormonal contraceptive use, and late fetal life.[9] As the metaplasia progresses, the transformation zone moves downwards from its original squamocolumnar junction position towards the external os, thus decreasing the area of the ectopy (ectropion).
- Squamous epithelialization. This is an additional process of cervical remodeling. It is a reactive change due to inflammation or regeneration.
As the above two processes progress, cervical ectropion decreases with age. As a result of these processes, a new squamocolumnar junction is formed. The transformation zone is the dynamic area located on the ectocervix. The transformation zone lies between the original squamocolumnar junction and the current squamocolumnar junction, where the metaplastic squamous epithelium has replaced the columnar epithelium, which is the area of ectropion.
Cervical ectropion is a common finding in pregnancy. The eversion process begins early but is most marked during the second and third trimesters. Reproductive hormones play the most significant role, but in the third trimester, venous obstruction might be one factor for cervical ectropion development. Postpartum, the everted columnar epithelium reverts back into the endocervix due to a decrease in cervical volume.[10]
In postmenopausal women, the squamocolumnar junction is invisible because it recedes into the endocervix.
Cervical ectropion has been associated with infection due to Chlamydia trachomatis.[11] This can be attributed to the fact that Chlamydia trachomatis has a preference for the glandular epithelium. Also, the areas of ectropion represent an area of low cell-mediated immunity. In these areas, the subpopulation of T lymphocytes, namely, T helper cells, CD8 cells, and CD1 lymphocytes are reduced in number.[12] Therefore it is more susceptible to infections like Chlamydia. Moreover, hormonal contraceptives, mainly the depot medroxyprogesterone acetate, have correlations with both cervical ectropion and chlamydial infection, therefore further enhancing the susceptibility of women with cervical ectropion for chlamydial infection.[13]
Women with cervical ectropion also have a higher susceptibility to infection with Neisseria gonorrheae. The risk of acquiring infection by the human immunodeficiency virus (HIV) is also higher in females with cervical ectropion.[14][15] However, there is no association between cervical ectropion and syphilis, trichomoniasis, and infections caused by cytomegalovirus, yeast, and fungi.[6][16][17]
Histopathology
Microscopic exam of normal cervix shows the following:
- The endocervix is typically lined by the single-layered mucus-secreting columnar cells, both ciliated and nonciliated. The cervix does not contain true glandular units; instead, the epithelium is thrown into longitudinal folds that invaginate, forming crypts off the central canal. The nonciliated cells secrete mucin in granular form through exocytosis, and the ciliated cells propel the secreted mucin. The epithelium has undifferentiated reserve cells. Being single-layered, it is a thin epithelium that easily penetrates the stromal vascularity, thus giving it a red appearance.
- The ectocervix is typically lined by a multilayered stratified squamous, non keratinized epithelium. The epithelium is formed by four cell types, including basal cells (the deepest layer of cells), parabasal cells, intermediate cells, and superficial cells.
- The transformation zone is formed by the endocervical reserve cell layer differentiating toward the squamous cell lineage. Its appearance is similar to the parabasal cells but with relatively less cytoplasm and dense nuclei. Nonspecific inflammatory infiltrates consisting of lymphocytes, plasma cells, and even neutrophils are common and are not necessarily associated with infection.
In cervical ectropion, the glandular endocervical cells are found on the ectocervix; thus, the area around the cervical os now appears red. Also, since the endocervical cells are more fragile and now exposed to the vaginal environment, they are more vulnerable to injury, for example, during sexual intercourse.[18][19]
However, with time, the undifferentiated reserve cells of the endocervix multiply and differentiate. This is initially seen as a single (non-stratified) layer of small, round cells with darkly staining nuclei situated very close to the nuclei of columnar cells, which further proliferate to produce a reserve cell hyperplasia. With the progression of the metaplastic process, the reserve cells of the endocervix proliferate and differentiate to form a thin epithelium of immature squamous cells without stratification. This newly formed epithelium is known as the immature squamous metaplastic epithelium. Over time, the immature metaplastic squamous cells differentiate into the mature stratified metaplastic epithelium.
History and Physical
Cervical ectropion is most commonly asymptomatic. In symptomatic cases, females may present with any of the following:
- Vaginal discharge. It is the most common symptom to manifest. The vaginal discharge is non-purulent and maybe white or yellow. The surface area of the mucus-secreting columnar cells is increased; therefore, women with cervical ectropion experience excessive vaginal discharge.
- Postcoital bleeding. It is seen in 5 to 25 percent of women with cervical ectropion. The fine blood vessels in the epithelium are torn very easily during sexual intercourse, leading to postcoital bleeding.[20] Cervical ectropion is one of the common causes of vaginal bleeding in the third trimester of pregnancy.
- Intermenstrual bleeding
- Dyspareunia
- Pelvic pain
- Recurrent cervicitis
- Backache
- Micturition disturbances
The everted columnar epithelium appears reddish on speculum examination, arranged in a ring around the external os. The postcoital bleeding and reddish appearance of the cervix on the speculum exam may be confused for the early signs of cervical cancer. Cervical ectropion is not an early sign or a symptom of cervical cancer.
The presentation of symptomatic cervical ectropion and desquamative inflammatory vaginitis may overlap. Desquamative inflammatory vaginitis is chronic vaginitis with vaginal discharge, vulvovaginal discomfort, dyspareunia, erythematous macules on the cervix, on speculum examination. No causal relationship between cervical ectropion and desquamative inflammatory vaginitis has been found.[1]
Evaluation
Being asymptomatic in most cases, cervical ectropion is diagnosed during a routine pelvic examination or at the time of pap screening.[21] Cervical ectropion is assessed and quantified by a direct and unaided speculum examination that shows a reddish area around the cervical os.
Further investigations are carried out to exclude other possibilities. They include the following:
- Nucleic acid amplification tests for chlamydia and gonorrheal cervicitis.
- Triple swab. Endocervical and high vaginal swabs are taken to rule out cervicitis. It is mainly done when vaginal discharge is purulent.
- Differentiating between cervical ectropion and cervical intraepithelial neoplasia and cervical cancer is difficult on macroscopic visualization. Though cervical ectropion is not associated with cervical cancer, in the case of cervical pain or spotting along with a red, inflamed cervix, the following tests can be done to rule out cervicitis, cervical intraepithelial neoplasia (CIN), and cervical cancer:[18][22][23]
- Pap smear
- Colposcopy
- Colposcopy with biopsy
A urine beta hCG qualitative test is carried out as the reproductive hormonal pattern during pregnancy often leads to the development of cervical ectropion.
Treatment / Management
Cervical ectropion requires no treatment unless the symptoms are affecting the patient's daily life. First-line treatment is discontinuing hormonal contraceptives like oral contraceptive pills, depot medroxyprogesterone acetate, and switching to nonhormonal contraception methods. If the symptoms persist, the following treatment can be offered:
- Cautery is an outpatient procedure carried out without general or local anesthesia. There are two types of cautery:
- Electrocautery also is known as cold coagulation. The cautery probe is held for 30 seconds against the area of ectropion, while the area is treated with heat to destroy the abnormal cells.
- Cryotherapy (freezing): The cautery probe is held for two minutes against ectropion while the area becomes frozen.[24] It has been observed that post-treatment with cryotherapy shows an improvement in the quality of the cervical mucus.[25] Therefore infertile women who also have cervical ectropion along with hostile cervical mucus can be treated with cryotherapy. It is safe in pregnancy.[24][26][27] (A1)
- Microwave tissue coagulation. Although the appearance of the cervix is better after microwave tissue coagulation, no other benefits have been found compared with either interferon-alpha suppository therapy or cryotherapy.[28] Some studies show that there is less vaginal bleeding after microwave tissue coagulation as compared with vaginal bleeding after laser therapy.
- Laser therapy. In this procedure, the carbon dioxide laser beam is used to destroy the abnormal cervical epithelium seen on magnification by a colposcope. It is an outpatient procedure and is done under no general or local anesthesia. The advantages of laser therapy are better precision, insignificant pain post-procedure, and rapid healing.
- Alpha interferon suppository. It has an immunomodulatory effect and an anti-proliferative effect. Interferon-alpha enhances the function of the T lymphocytes.
- Polydeoxyribonucleotide vaginal suppository. It leads to re-epithelialization of the area of the ectropion, therefore reducing the size of the ectropion.[26] The efficacy of this modality is explained by the excellent tolerability and compliance among the users, reduced inflammation, increased iodine-dark areas, the reestablishment of normal balance in T- and B-lymphocytes, and a reduction in the intensity of symptoms.[29][30]
- Boric acid vaginal suppositories can be used to make the pH acidic.
- Autologous platelet-rich plasma application. It is a promising therapy. The tissue healing time is short, and post-procedural bleeding is much less than laser therapy.[31][32]
- Focused ultrasound is another promising therapy for symptomatic cervical ectropion as it can be used for a wide variety of women.[33][34] (A1)
There is a cure rate of 92 percent with treatment with cautery or microwave tissue coagulation therapy. A cure rate of 79 percent has been seen with laser treatment.
Treatment success is determined by the following,
- Improved appearance of the cervix that was earlier bright red color
- Decrease in symptoms
- Improved characteristics of the cervical mucus
- Restoration of the T and the B lymphocyte populations
Ultrasound is not a reliable modality to monitor the treatment success of cervical ectropion.[35]
After appropriate treatment, the following symptoms should prompt the patient to return to the clinic for further evaluation for cervical infection or neoplasia.
- Malodorous discharge
- Persistent postcoital or intermenstrual bleeding
Differential Diagnosis
The following conditions have signs or symptoms similar to cervical ectropion and may need further evaluation.[18][36]
- Cervical cancer. Post-coital bleeding, intermenstrual bleeding, vaginal discharge, urinary complaints, red color area around the cervical os on speculum examination prompt further tests to rule out cervical cancer.
- Cervical intraepithelial neoplasia (CIN). On speculum examination, the red color area around the cervical os may be alarming and prompt further evaluation to rule out CIN.
- Infectious cervicitis. The presence of increased vaginal discharge, which may or may not be purulent, post-coital bleeding, and intermenstrual bleed, prompts further evaluation to rule out cervicitis. Other signs and symptoms such as recent unprotected sexual intercourse, and a history of infectious cervicitis, supports the diagnosis of infectious cervicitis.
- Chronic cervicitis, that is, non-gonococcal non-chlamydial cervicitis.[37]
- Vulvovaginitis.
- Pelvic inflammatory disease. Fever, dysmenorrhoea, dyschezia, itching or burning of vulvovaginal area, purulent vaginal discharge that may be blood-stained, pelvic pain, cervical motion tenderness, infertility, history of infectious cervicitis favors the diagnosis of pelvic inflammatory disease.
- Desquamative inflammatory vaginitis. It is chronic inflammatory vaginitis, most common in perimenopausal women. It is treated with vaginal clindamycin 2% cream, vaginal hydrocortisone 10% cream, or cortisone acetate 25 mg vaginal suppositories. For refractory cases, it has been noted that ablation might be beneficial.[1]
- Pregnancy
Prognosis
Cervical ectropion usually does not lead to medical complications. Studies show that there is no benefit from the routine treatment of cervical ectropion. Only symptomatic women should consider treatment. Otherwise, it usually resolves itself, overtime.[3][38]
However, cervical ectropion does increase the vulnerability of acquiring sexually transmitted infections, including chlamydia cervicitis, gonorrhea, and HIV.[21] Studies have shown that the benefit of cervical ectropion treatment is seen only in some groups, for example, high-risk women who are more likely to acquire these infections. Otherwise, treating women for cervical ectropion in the general population provides little protection against these infections, given the large number of women treated.
Though cervical ectropion may predispose HPV infection, it is not a precursor to cervical intraepithelial neoplasia and cervical cancer. Instead, it has been found that not cervical ectropion but the process of squamous metaplasia leads to increased vulnerability to HPV 16 infection, which has malignant potential. This is because the host cell replication and differentiation process during squamous metaplasia may be a favorable ground for HPV virus replication.[39]
Cervical ectropion does not lead to infertility. It has no adverse effects on pregnancy or the fetus.
Complications
Although cervical ectropion resolves itself over time, it creates a vulnerable ground for seeding various sexually transmitted infections, chlamydial cervicitis being the most common. Cervical ectropion may be debilitating for females who experience excessive vaginal discharge or frequent vaginal bleeding. However, appropriate treatment is successful in relieving these symptoms.
Mild complications may be noted after ablative treatment modalities. These complications include slight vaginal bleeding, vaginal irritation, scant vaginal discharge, or cramp-like pelvic pain. However, these do not interfere with day to day life and resolve themselves a few weeks postprocedure. The benefits of the therapy, including long term relief of symptoms, and being an outpatient procedure that is safe, simple, and inexpensive far outweigh the minor risks.
Deterrence and Patient Education
Patients with cervical ectropion might not be aware that they have it until it is diagnosed on a routine pelvic exam or a pap smears. The presence of symptoms like vaginal bleeding, dyspareunia, the excessive vaginal discharge might be alarming for patients. Patients usually worry about the possibility of cervical cancer, cervicitis, and infertility.
It is essential to educate the patient about cervical ectropion's benign nature. It has no association with pathological conditions, but carrying out other tests is required to rule out the possibility of these conditions. The patient should be fully informed about the treatment modalities available and offered treatment if the symptoms are bothersome. It will help ease the fear of unnecessary financial burden, effects on work due to frequent hospital visits, and the interference with reproductive and sexual health.
Enhancing Healthcare Team Outcomes
Cervical ectropion poses a diagnostic dilemma. These patients may present with non-specific signs and symptoms such as white to yellow vaginal discharge, post-coital or intermenstrual bleeding, pelvic pain, and dyspareunia. Such signs and symptoms lead to a myriad of differential diagnosis, including conditions that could be cervical, vaginal, or vulvar in origin. An interprofessional team that provides a holistic and integrated approach to the formulation of a management plan can help achieve the best possible outcomes.
While the gynecologist is always involved in the care of patients with cervical ectropion, it is essential to consult with an interprofessional team of specialists that include a radiologist, surgeon, and infectious disease. The interventions carried out to rule out more severe conditions have a detrimental effect on a women's mental, social, and sexual life. Therefore, consultation should be made with a social worker, and community nurses, as vital members of the interprofessional group, will assist with the education and support of the patient and family. The earlier that the possibilities of infections, benign growths, and malignancy are ruled out, the better the prognosis and outcome. Collaboration, shared decision making, and communication is key elements for a good outcome.
Media
(Click Image to Enlarge)
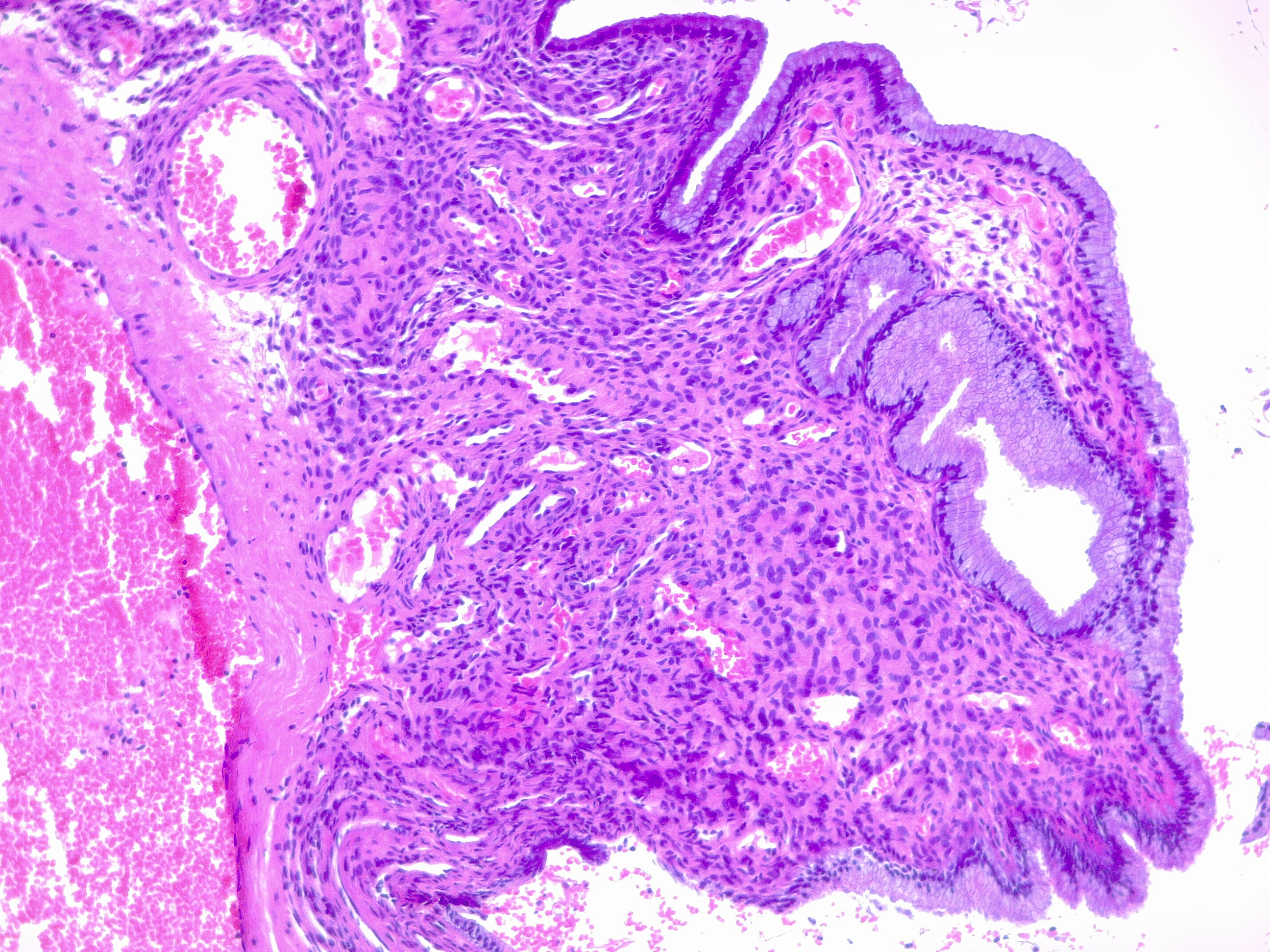
Endocervical polyp. Cervical polyps are common in reproductive years and can be found in cases of ectropion. In this image of the cervical mucosa typical endocervical glands with aedematous stroma with clear congestion. Contributed by Fabiola Farci, MD
References
Mitchell L, King M, Brillhart H, Goldstein A. Cervical Ectropion May Be a Cause of Desquamative Inflammatory Vaginitis. Sexual medicine. 2017 Sep:5(3):e212-e214. doi: 10.1016/j.esxm.2017.03.001. Epub 2017 Apr 28 [PubMed PMID: 28460993]
Chang AR. 'Erosion' of the uterine cervix; an anachronism. The Australian & New Zealand journal of obstetrics & gynaecology. 1991 Nov:31(4):358-62 [PubMed PMID: 1799353]
Goldacre MJ, Loudon N, Watt B, Grant G, Loudon JD, McPherson K, Vessey MP. Epidemiology and clinical significance of cervical erosion in women attending a family planning clinic. British medical journal. 1978 Mar 25:1(6115):748-50 [PubMed PMID: 630328]
Wright KO,Mohammed AS,Salisu-Olatunji O,Kuyinu YA, Cervical Ectropion and Intra-Uterine Contraceptive Device (IUCD): a five-year retrospective study of family planning clients of a tertiary health institution in Lagos Nigeria. BMC research notes. 2014 Dec 23; [PubMed PMID: 25539789]
Level 2 (mid-level) evidenceMadile BM. The Cervical Epithelium From Fetal Age to Adolescence. Obstetrics and gynecology. 1976 May:47(5):536-9 [PubMed PMID: 1264400]
Jacobson DL, Peralta L, Graham NM, Zenilman J. Histologic development of cervical ectopy: relationship to reproductive hormones. Sexually transmitted diseases. 2000 May:27(5):252-8 [PubMed PMID: 10821596]
Reich O, Regauer S, McCluggage WG, Bergeron C, Redman C. Defining the Cervical Transformation Zone and Squamocolumnar Junction: Can We Reach a Common Colposcopic and Histologic Definition? International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists. 2017 Nov:36(6):517-522. doi: 10.1097/PGP.0000000000000381. Epub [PubMed PMID: 28639968]
Level 2 (mid-level) evidenceAutier P, Coibion M, Huet F, Grivegnee AR. Transformation zone location and intraepithelial neoplasia of the cervix uteri. British journal of cancer. 1996 Aug:74(3):488-90 [PubMed PMID: 8695371]
Maqueo M, Azuela JC, Calderon JJ, Goldzieher JW. Morphology of the cervix in women treated with synthetic progestins. American journal of obstetrics and gynecology. 1966 Dec 1:96(7):994-8 [PubMed PMID: 4162849]
Ostergard DR. The effect of pregnancy on the cervical squamocolumnar junction in patients with abnormal cervical cytology. American journal of obstetrics and gynecology. 1979 Aug 1:134(7):759-60 [PubMed PMID: 463976]
Lee V, Tobin JM, Foley E. Relationship of cervical ectopy to chlamydia infection in young women. The journal of family planning and reproductive health care. 2006 Apr:32(2):104-6 [PubMed PMID: 16824301]
Level 2 (mid-level) evidenceDe Luca Brunori I, Facchini V, Filippeschi M, Battini L, Giusti G, Romani L, Scida P, Urbano M. Cell-mediated immunity in the course of cervical ectropion. Clinical and experimental obstetrics & gynecology. 1994:21(2):105-7 [PubMed PMID: 7915218]
Morrison CS, Bright P, Wong EL, Kwok C, Yacobson I, Gaydos CA, Tucker HT, Blumenthal PD. Hormonal contraceptive use, cervical ectopy, and the acquisition of cervical infections. Sexually transmitted diseases. 2004 Sep:31(9):561-7 [PubMed PMID: 15480119]
Level 2 (mid-level) evidenceVenkatesh KK, Cu-Uvin S. Assessing the relationship between cervical ectopy and HIV susceptibility: implications for HIV prevention in women. American journal of reproductive immunology (New York, N.Y. : 1989). 2013 Feb:69 Suppl 1():68-73. doi: 10.1111/aji.12029. Epub 2012 Oct 11 [PubMed PMID: 23057756]
Monroy OL, Aguilar C, Lizano M, Cruz-Talonia F, Cruz RM, Rocha-Zavaleta L. Prevalence of human papillomavirus genotypes, and mucosal IgA anti-viral responses in women with cervical ectopy. Journal of clinical virology : the official publication of the Pan American Society for Clinical Virology. 2010 Jan:47(1):43-8. doi: 10.1016/j.jcv.2009.10.008. Epub 2009 Nov 10 [PubMed PMID: 19906557]
Kleppa E, Holmen SD, Lillebø K, Kjetland EF, Gundersen SG, Taylor M, Moodley P, Onsrud M. Cervical ectopy: associations with sexually transmitted infections and HIV. A cross-sectional study of high school students in rural South Africa. Sexually transmitted infections. 2015 Mar:91(2):124-9. doi: 10.1136/sextrans-2014-051674. Epub 2014 Oct 3 [PubMed PMID: 25281761]
Level 2 (mid-level) evidenceJunior JE, Giraldo PC, Gonçalves AK, do Amaral RL, Linhares IM. Uterine cervical ectopy during reproductive age: cytological and microbiological findings. Diagnostic cytopathology. 2014 May:42(5):401-4. doi: 10.1002/dc.23053. Epub 2013 Oct 25 [PubMed PMID: 24166971]
Level 2 (mid-level) evidenceCasey PM, Long ME, Marnach ML. Abnormal cervical appearance: what to do, when to worry? Mayo Clinic proceedings. 2011 Feb:86(2):147-50; quiz 151. doi: 10.4065/mcp.2010.0512. Epub 2011 Jan 26 [PubMed PMID: 21270291]
Level 3 (low-level) evidenceJoshi SN, Das S, Thakar M, Sahasrabuddhe V, Kumar BK, Callahan M, Mauck C. Colposcopically observed vascular changes in the cervix in relation to the hormonal levels and menstrual cycle. Journal of lower genital tract disease. 2008 Oct:12(4):293-9. doi: 10.1097/LGT.0b013e31817efbbd. Epub [PubMed PMID: 18820544]
Selo-Ojeme DO, Dayoub N, Patel A, Metha M. A clinico-pathological study of postcoital bleeding. Archives of gynecology and obstetrics. 2004 Jul:270(1):34-6 [PubMed PMID: 15224216]
Level 2 (mid-level) evidenceCritchlow CW, Wölner-Hanssen P, Eschenbach DA, Kiviat NB, Koutsky LA, Stevens CE, Holmes KK. Determinants of cervical ectopia and of cervicitis: age, oral contraception, specific cervical infection, smoking, and douching. American journal of obstetrics and gynecology. 1995 Aug:173(2):534-43 [PubMed PMID: 7645632]
Level 2 (mid-level) evidenceStillo A, Bianco V, Lorenzin MG, Franzosi N. [Colposcopic evaluation of cervical epithelium during oral contraception. A controlled clinical study]. Annali di ostetricia, ginecologia, medicina perinatale. 1989 Nov-Dec:110(6):296-304 [PubMed PMID: 2700878]
Level 1 (high-level) evidenceSlimani O, Ben Temim R, Makhlouf T, Mathlouthi N, Attia L. Cyto-colpo-histologic correlation: about an analytical study of 120 colposcopies. La Tunisie medicale. 2016 Oct:94(10):616-620 [PubMed PMID: 28972254]
Gay C, Riehl C, Ramanah R, Desmoulin G, Violaine B. [Cryotherapy in the management of symptomatic cervical ectopy]. Gynecologie, obstetrique & fertilite. 2006 Mar:34(3):214-23 [PubMed PMID: 16530444]
Level 2 (mid-level) evidenceÇekmez Y, Şanlıkan F, Göçmen A, Vural A, Türkmen SB. Is Cryotherapy Friend or Foe for Symptomatic Cervical Ectopy? Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2016:25(1):8-11. doi: 10.1159/000441433. Epub 2015 Oct 27 [PubMed PMID: 26436550]
Baram A, Paz GF, Peyser MR, Schachter A, Homonnai ZT. Treatment of cervical ectropion by cryosurgery: effect on cervical mucus characteristics. Fertility and sterility. 1985 Jan:43(1):86-9 [PubMed PMID: 3838091]
Agah J,Sharifzadeh M,Hosseinzadeh A, Cryotherapy as a Method for Relieving Symptoms of Cervical Ectopy: A Randomized Clinical Trial. Oman medical journal. 2019 Jul; [PubMed PMID: 31360321]
Level 1 (high-level) evidenceYang K, Li J, Liu Y, Ma B, Roberts H, Tan J, Tian J, Wu T, Zhang P. Microwave therapy for cervical ectropion. The Cochrane database of systematic reviews. 2007 Oct 17:2007(4):CD006227 [PubMed PMID: 17943899]
Level 1 (high-level) evidenceDe Luca Brunori I, Urbano M, Romani L, Tarani A, Felipetto R, Battini L, Amato A, Andreoni P. [Clinico-morphological changes in ectropion after treatment with polydeoxyribonucleotide (PDRN)]. Annali di ostetricia, ginecologia, medicina perinatale. 1990 Nov-Dec:111(6):379-87 [PubMed PMID: 2102065]
de Luca Brunori I, Battini L, Filippeschi M, Romani L, Tarani A, Urbano M. [Topical therapy with placental polydeoxyribonucleotide in cervical ectopy and ectropion]. Annali di ostetricia, ginecologia, medicina perinatale. 1989 Jan-Feb:110(1):35-41 [PubMed PMID: 2757327]
Level 1 (high-level) evidenceHua X, Zeng Y, Zhang R, Wang H, Diao J, Zhang P. Using platelet-rich plasma for the treatment of symptomatic cervical ectopy. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2012 Oct:119(1):26-9. doi: 10.1016/j.ijgo.2012.05.029. Epub 2012 Jul 24 [PubMed PMID: 22835570]
Level 1 (high-level) evidenceDawood AS, Salem HA. Current clinical applications of platelet-rich plasma in various gynecological disorders: An appraisal of theory and practice. Clinical and experimental reproductive medicine. 2018 Jun:45(2):67-74. doi: 10.5653/cerm.2018.45.2.67. Epub 2018 Jun 29 [PubMed PMID: 29984206]
Level 2 (mid-level) evidenceChen J, Zhou D, Liu Y, Peng J, Li C, Chen W, Wang Z. A comparison between ultrasound therapy and laser therapy for symptomatic cervical ectopy. Ultrasound in medicine & biology. 2008 Nov:34(11):1770-4. doi: 10.1016/j.ultrasmedbio.2008.03.013. Epub 2008 May 9 [PubMed PMID: 18471953]
Level 1 (high-level) evidenceLi C, Xiong X, Li Y, Li J, Peng B, Wang Z, Chen W. Therapeutic effects of focused ultrasound in 4014 patients with symptomatic cervical ectopy. Ultrasound in medicine & biology. 2013 Apr:39(4):604-10. doi: 10.1016/j.ultrasmedbio.2012.11.012. Epub [PubMed PMID: 23497842]
Cotarcea S,Stefanescu C,Adam G,Voicu C,Cara M,Comanescu A,Cernea N,Pană R, The Importance of Ultrasound Monitoring of the Normal and Lesional Cervical Ectropion Treatment. Current health sciences journal. 2016 Apr-Jun; [PubMed PMID: 30568831]
Mitchell H. Vaginal discharge--causes, diagnosis, and treatment. BMJ (Clinical research ed.). 2004 May 29:328(7451):1306-8 [PubMed PMID: 15166070]
Mattson SK, Polk JP, Nyirjesy P. Chronic Cervicitis: Presenting Features and Response to Therapy. Journal of lower genital tract disease. 2016 Jul:20(3):e30-3. doi: 10.1097/LGT.0000000000000225. Epub [PubMed PMID: 27243142]
Machado Junior LC, Dalmaso AS, Carvalho HB. Evidence for benefits from treating cervical ectopy: literature review. Sao Paulo medical journal = Revista paulista de medicina. 2008 Mar 6:126(2):132-9 [PubMed PMID: 18553039]
Hwang LY, Ma Y, Shiboski SC, Farhat S, Jonte J, Moscicki AB. Active squamous metaplasia of the cervical epithelium is associated with subsequent acquisition of human papillomavirus 16 infection among healthy young women. The Journal of infectious diseases. 2012 Aug 15:206(4):504-11. doi: 10.1093/infdis/jis398. Epub 2012 Jun 13 [PubMed PMID: 22696500]
Level 2 (mid-level) evidence